
Comparative Effectiveness and Safety of Standard-Dose and Low-Dose Pembrolizumab in Patients with Non-Small-Cell Lung Cancer: A Multi-Institutional Cohort Study in Taiwan


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources
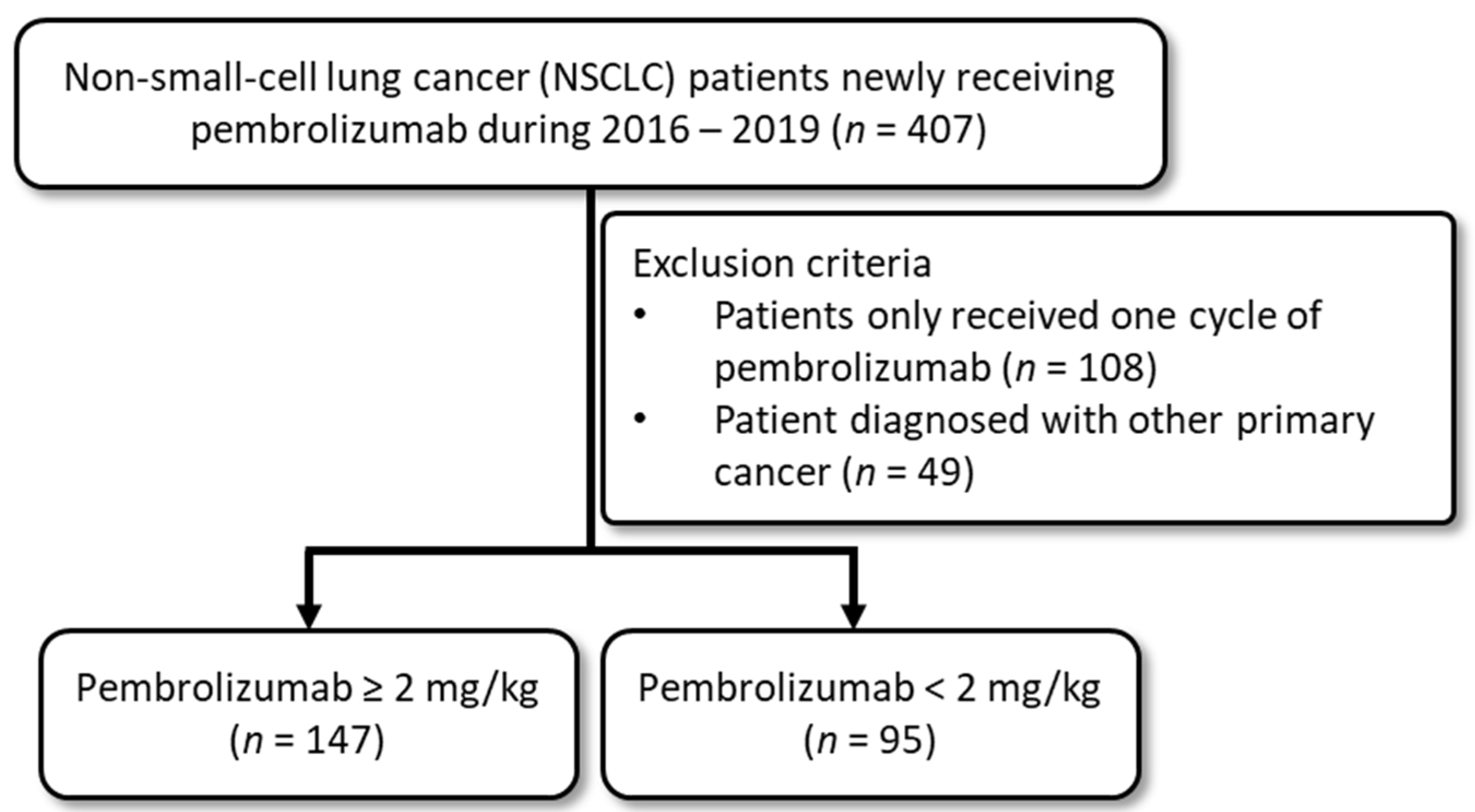
2.2. Study Population
2.3. Pembrolizumab Groups and Patients’ Demographics
2.4. Study Outcomes
2.5. Statistical Analyses
3. Results
3.1. Baseline Characteristics
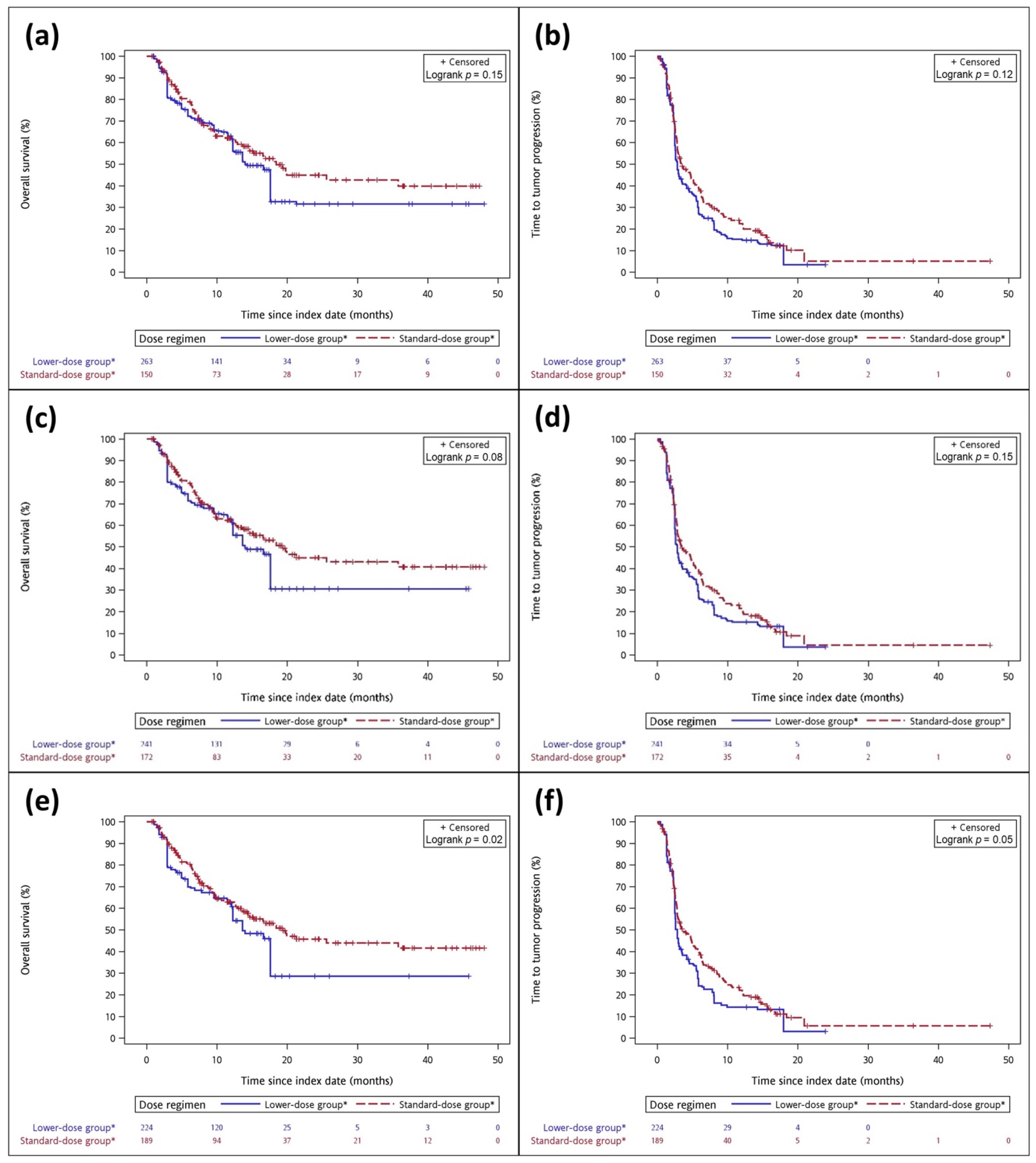
3.2. Effectiveness Outcomes in Primary and Secondary Objectives
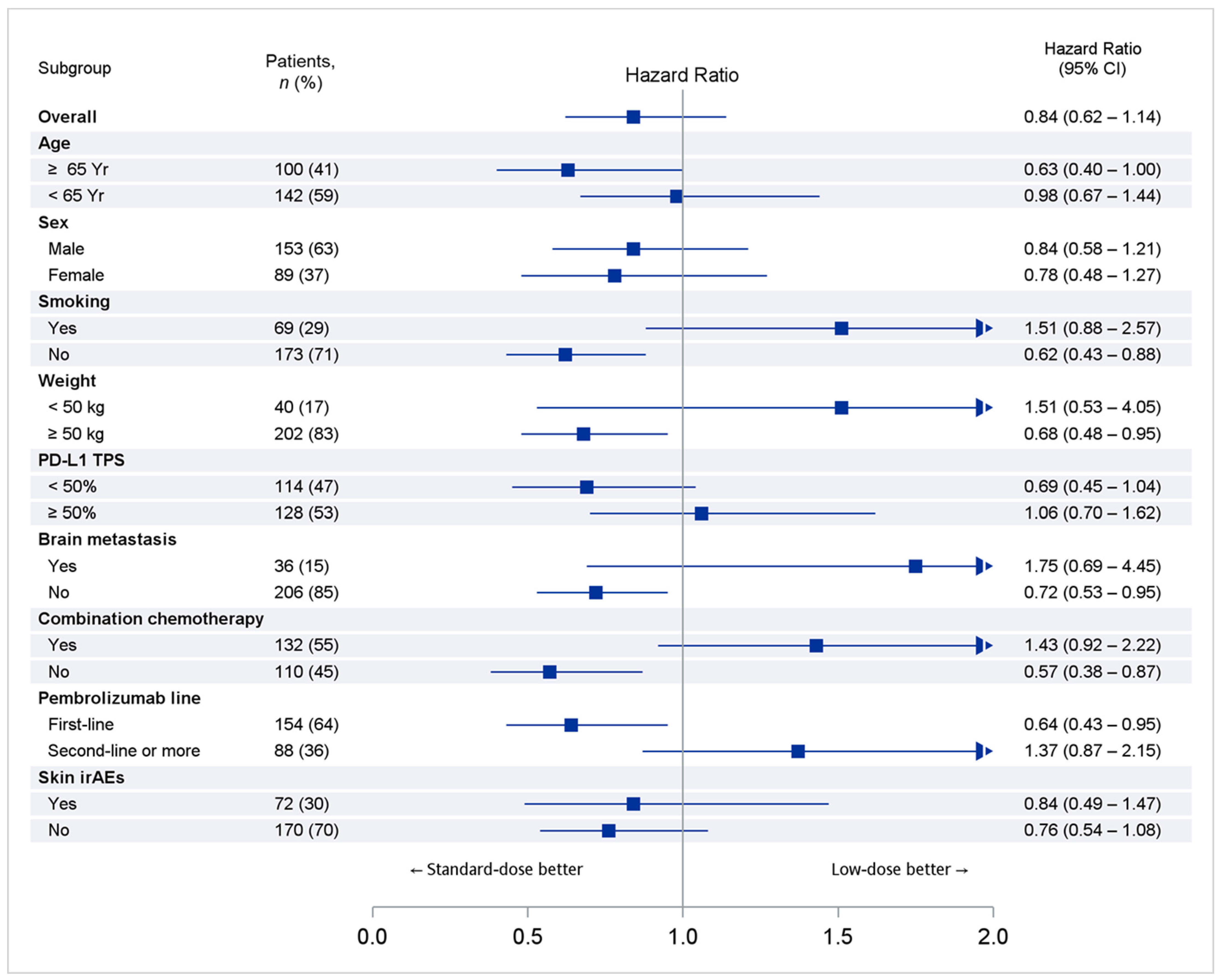
3.3. Subgroup and Sensitivity Analyses
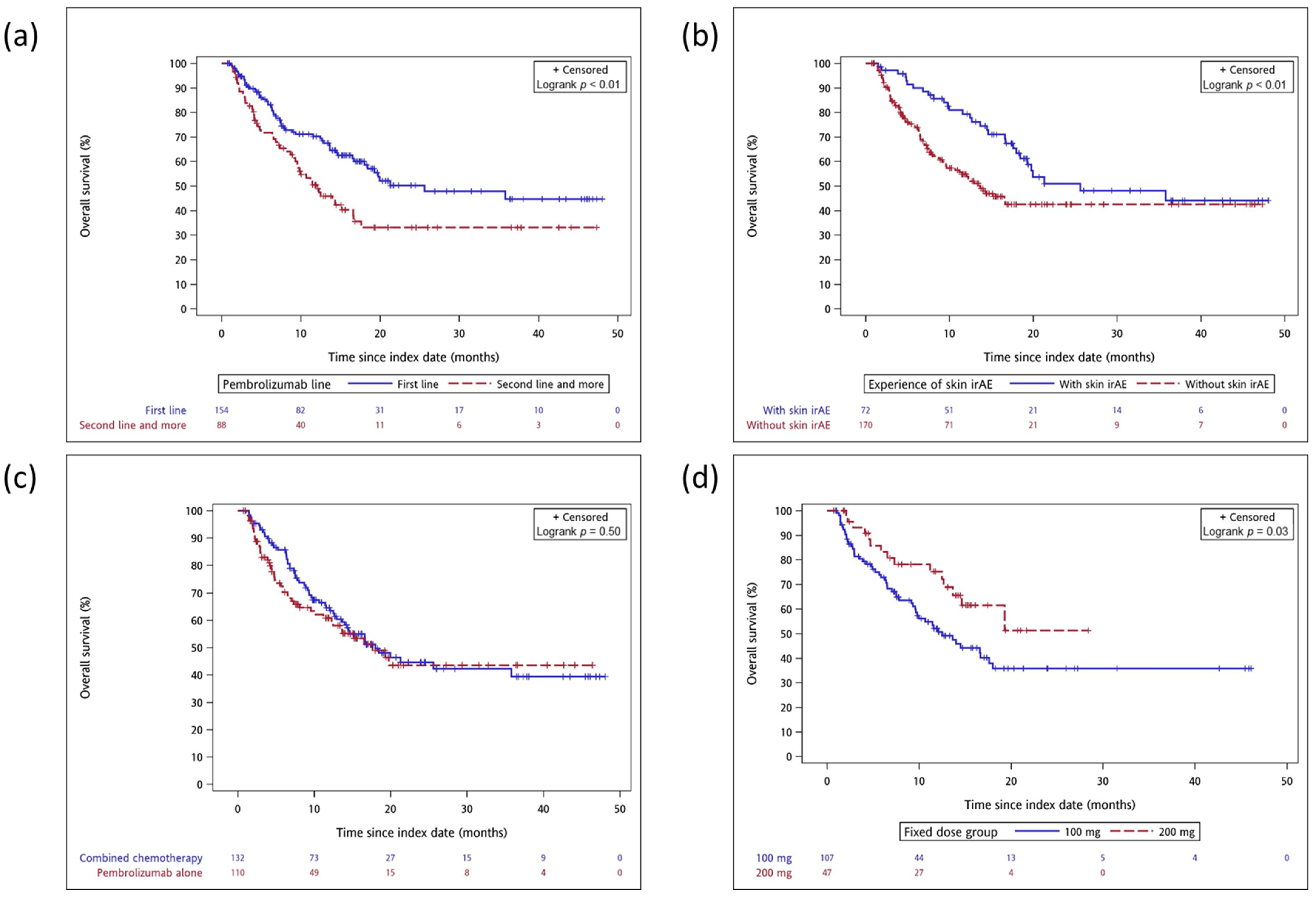
3.4. Post Hoc Subgroup Analyses of the Total Cohort
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bade, B.C.; Dela Cruz, C.S. Lung Cancer 2020: Epidemiology, Etiology, and Prevention. Clin. Chest Med. 2020, 41, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Thai, A.A.; Solomon, B.J.; Sequist, L.V.; Gainor, J.F.; Heist, R.S. Lung cancer. Lancet 2021, 398, 535–554. [Google Scholar] [CrossRef]
- Hanna, N.; Johnson, D.; Temin, S.; Baker, S., Jr.; Brahmer, J.; Ellis, P.M.; Giaccone, G.; Hesketh, P.J.; Jaiyesimi, I.; Leighl, N.B.; et al. Systemic Therapy for Stage IV Non–Small–Cell Lung Cancer: American Society of Clinical Oncology Clinical Practice Guideline Update. J. Clin. Oncol. 2017, 35, 3484–3515. [Google Scholar] [CrossRef] [PubMed]
- Zarour, H.M. Reversing T–cell Dysfunction and Exhaustion in Cancer. Clin. Cancer Res. 2016, 22, 1856–1864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Low, J.L.; Walsh, R.J.; Ang, Y.; Chan, G.; Soo, R.A. The evolving immuno–oncology landscape in advanced lung cancer: First–line treatment of non–small cell lung cancer. Ther. Adv. Med. Oncol. 2019, 11, 1758835919870360. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Rodríguez–Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus Chemotherapy for PD–L1–Positive Non–Small–Cell Lung Cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reck, M.; Rodríguez–Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Updated Analysis of KEYNOTE–024: Pembrolizumab Versus Platinum–Based Chemotherapy for Advanced Non–Small–Cell Lung Cancer With PD–L1 Tumor Proportion Score of 50% or Greater. J. Clin. Oncol. 2019, 37, 537–546. [Google Scholar] [CrossRef]
- Mok, T.S.K.; Wu, Y.L.; Kudaba, I.; Kowalski, D.M.; Cho, B.C.; Turna, H.Z.; Castro, G., Jr.; Srimuninnimit, V.; Laktionov, K.K.; Bondarenko, I.; et al. Pembrolizumab versus chemotherapy for previously untreated, PD–L1–expressing, locally advanced or metastatic non–small–cell lung cancer (KEYNOTE–042): A randomised, open–label, controlled, phase 3 trial. Lancet 2019, 393, 1819–1830. [Google Scholar] [CrossRef]
- Cho, B.C.; Wu, Y.; Lopes, G.; Kudaba, I.; Kowalski, D.M.; Turna, H.Z.; De Castro, G., Jr.; Caglevic, C.; Zhang, L.; Karaszewska, B.; et al. FP13.04 KEYNOTE–042 3–Year Survival Update: 1L Pembrolizumab vs. Platinum–Based Chemotherapy for PD–L1+ Locally Advanced/Metastatic NSCLC. J. Thorac. Oncol. 2021, 16, S225–S226. [Google Scholar] [CrossRef]
- Ahamadi, M.; Freshwater, T.; Prohn, M.; Li, C.H.; de Alwis, D.P.; de Greef, R.; Elassaiss–Schaap, J.; Kondic, A.; Stone, J.A. Model–Based Characterization of the Pharmacokinetics of Pembrolizumab: A Humanized Anti–PD–1 Monoclonal Antibody in Advanced Solid Tumors. CPT Pharmacomet. Syst. Pharmacol. 2017, 6, 49–57. [Google Scholar] [CrossRef]
- Freshwater, T.; Kondic, A.; Ahamadi, M.; Li, C.H.; de Greef, R.; de Alwis, D.; Stone, J.A. Evaluation of dosing strategy for pembrolizumab for oncology indications. J. Immunother. Cancer 2017, 5, 43. [Google Scholar] [CrossRef] [PubMed]
- Rahma, O.E.; Reuss, J.E.; Giobbie–Hurder, A.; Shoja, E.R.G.; Abu–Shawer, O.; Mehra, P.; Gupta, S.; Simon, R.; Khleif, S.N. Early 3 + 3 Trial Dose–Escalation Phase I Clinical Trial Design and Suitability for Immune Checkpoint Inhibitors. Clin. Cancer Res. 2021, 27, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Jang, A.; Nakashima, L.; Ng, T.; Fung, M.; Jiwani, S.; Schaff, K.; Suess, J.; Goncalves, R.; Jang, D.; Kuik, K.; et al. A real–world data approach to determine the optimal dosing strategy for pembrolizumab. J. Oncol Pharm Pract. 2020, 27, 635–643. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, D.A.; Gordon, N.; Davidescu, M.; Leshno, M.; Steuer, C.E.; Patel, N.; Stemmer, S.M.; Zer, A. A Phamacoeconomic Analysis of Personalized Dosing vs. Fixed Dosing of Pembrolizumab in Firstline PD–L1–Positive Non–Small Cell Lung Cancer. J. Natl. Cancer Inst. 2017, 109. [Google Scholar] [CrossRef] [PubMed]
- Bayle, A.; Besse, B.; Annereau, M.; Bonastre, J. Switch to anti–programmed cell death protein 1 (anti–PD–1) fixed–dose regimen: What is the economic impact? Eur. J. Cancer 2019, 113, 28–31. [Google Scholar] [CrossRef]
- Shao, S.C.; Chan, Y.Y.; Kao Yang, Y.H.; Lin, S.J.; Hung, M.J.; Chien, R.N.; Lai, C.C.; Lai, E.C. The Chang Gung Research Database–A multi–institutional electronic medical records database for real–world epidemiological studies in Taiwan. Pharmacoepidemiol. Drug Saf. 2019, 28, 593–600. [Google Scholar] [CrossRef]
- Shao, S.C.; Chang, K.C.; Hung, M.J.; Yang, N.I.; Chan, Y.Y.; Chen, H.Y.; Kao Yang, Y.H.; Lai, E.C. Comparative risk evaluation for cardiovascular events associated with dapagliflozin vs. empagliflozin in real–world type 2 diabetes patients: A multi–institutional cohort study. Cardiovasc. Diabetol. 2019, 18, 120. [Google Scholar] [CrossRef] [Green Version]
- Chang, S.L.; Huang, Y.L.; Lee, M.C.; Hu, S.; Hsiao, Y.C.; Chang, S.W.; Chang, C.J.; Chen, P.C. Association of Varicose Veins with Incident Venous Thromboembolism and Peripheral Artery Disease. JAMA 2018, 319, 807–817. [Google Scholar] [CrossRef]
- Liao, S.C.; Shao, S.C.; Lai, E.C.; Lin, S.J.; Huang, W.I.; Hsieh, C.Y. Positive Predictive Value of ICD-10 Codes for Cerebral Venous Sinus Thrombosis in Taiwan’s National Health Insurance Claims Database. Clin. Epidemiol. 2022, 14, 1–7. [Google Scholar] [CrossRef]
- Ogungbenro, K.; Patel, A.; Duncombe, R.; Nuttall, R.; Clark, J.; Lorigan, P. Dose Rationalization of Pembrolizumab and Nivolumab Using Pharmacokinetic Modeling and Simulation and Cost Analysis. Clin. Pharmacol. Ther. 2018, 103, 582–590. [Google Scholar] [CrossRef]
- Desai, R.J.; Franklin, J.M. Alternative approaches for confounding adjustment in observational studies using weighting based on the propensity score: A primer for practitioners. BMJ 2019, 367, l5657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Low, J.L.; Huang, Y.; Sooi, K.; Ang, Y.; Chan, Z.Y.; Spencer, K.; Jeyasekharan, A.D.; Sundar, R.; Goh, B.C.; Soo, R.; et al. Low–dose pembrolizumab in the treatment of advanced non–small cell lung cancer. Int. J. Cancer 2021, 149, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, L.; Rodríguez–Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non–Small–Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef] [PubMed]
- Gadgeel, S.; Rodríguez–Abreu, D.; Speranza, G.; Esteban, E.; Felip, E.; Dómine, M.; Hui, R.; Hochmair, M.J.; Clingan, P.; Powell, S.F.; et al. Updated Analysis From KEYNOTE–189: Pembrolizumab or Placebo Plus Pemetrexed and Platinum for Previously Untreated Metastatic Nonsquamous Non–Small–Cell Lung Cancer. J. Clin. Oncol. 2020, 38, 1505–1517. [Google Scholar] [CrossRef] [PubMed]
- Cortellini, A.; Friedlaender, A.; Banna, G.L.; Porzio, G.; Bersanelli, M.; Cappuzzo, F.; Aerts, J.; Giusti, R.; Bria, E.; Cortinovis, D.; et al. Immune–related Adverse Events of Pembrolizumab in a Large Real–world Cohort of Patients with NSCLC with a PD–L1 Expression ≥50% and Their Relationship with Clinical Outcomes. Clin. Lung Cancer 2020, 21, 498–508.e2. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Zeng, D.; Ou, Q.; Liu, S.; Li, A.; Chen, Y.; Lin, D.; Gao, Q.; Zhou, H.; Liao, W.; et al. Association of Survival and Immune–Related Biomarkers with Immunotherapy in Patients with Non–Small Cell Lung Cancer: A Meta–analysis and Individual Patient–Level Analysis. JAMA Netw. Open 2019, 2, e196879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brody, R.; Zhang, Y.; Ballas, M.; Siddiqui, M.K.; Gupta, P.; Barker, C.; Midha, A.; Walker, J. PD–L1 expression in advanced NSCLC: Insights into risk stratification and treatment selection from a systematic literature review. Lung Cancer 2017, 112, 200–215. [Google Scholar] [CrossRef] [Green Version]
- Dafni, U.; Tsourti, Z.; Vervita, K.; Peters, S. Immune checkpoint inhibitors, alone or in combination with chemotherapy, as first–line treatment for advanced non–small cell lung cancer. A systematic review and network meta–analysis. Lung Cancer 2019, 134, 127–140. [Google Scholar] [CrossRef]
- Kim, R.; Keam, B.; Hahn, S.; Ock, C.Y.; Kim, M.; Kim, T.M.; Kim, D.W.; Heo, D.S. First–line Pembrolizumab Versus Pembrolizumab Plus Chemotherapy Versus Chemotherapy Alone in Non–small–cell Lung Cancer: A Systematic Review and Network Meta–analysis. Clin. Lung Cancer 2019, 20, 331–338.e334. [Google Scholar] [CrossRef]
- Zhou, Y.; Lin, Z.; Zhang, X.; Chen, C.; Zhao, H.; Hong, S.; Zhang, L. First–line treatment for patients with advanced non–small cell lung carcinoma and high PD–L1 expression: Pembrolizumab or pembrolizumab plus chemotherapy. J. Immunother. Cancer 2019, 7, 120. [Google Scholar] [CrossRef] [Green Version]
- Raphael, J.; Batra, A.; Boldt, G.; Shah, P.S.; Blanchette, P.; Rodrigues, G.; Vincent, M.D. Predictors of Survival Benefit from Immune Checkpoint Inhibitors in Patients with Advanced Non–small–cell Lung Cancer: A Systematic Review and Meta–analysis. Clin. Lung Cancer 2020, 21, 106–113.e5. [Google Scholar] [CrossRef] [PubMed]
- Carrigan, G.; Whipple, S.; Taylor, M.D.; Torres, A.Z.; Gossai, A.; Arnieri, B.; Tucker, M.; Hofmeister, P.P.; Lambert, P.; Griffith, S.D.; et al. An evaluation of the impact of missing deaths on overall survival analyses of advanced non–small cell lung cancer patients conducted in an electronic health records database. Pharmacoepidemiol. Drug Saf. 2019, 28, 572–581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shankar, B.; Zhang, J.; Naqash, A.R.; Forde, P.M.; Feliciano, J.L.; Marrone, K.A.; Ettinger, D.S.; Hann, C.L.; Brahmer, J.R.; Ricciuti, B.; et al. Multisystem Immune–Related Adverse Events Associated with Immune Checkpoint Inhibitors for Treatment of Non–Small Cell Lung Cancer. JAMA Oncol. 2020, 6, 1952–1956. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total Patients (n = 242) | Original Cohort | IPTW Cohort * | ||||
|---|---|---|---|---|---|---|---|
| Standard-Dose (n = 147) | Low-Dose (n = 95) | p Value | Standard-Dose (n = 263) | Low-Dose (n = 150) | p Value | ||
| Age, mean years (range) | 62.0 (56.0–72.0) | 63.7 (58.0–73.0) | 62.0 (54.0–72.0) | 0.09 | 63.6 (58.0–73.0) | 63.7 (58.0–73.0) | 0.92 |
| Male (%) | 63.2% | 62.6% | 64.2% | 0.79 | 61.5% | 67.5% | 0.17 |
| Body weight, mean kg (range) | 61.5 (52.8–69.4) | 60.5 (50.0–68.8) | 63.9 (55.0–73.8) | 0.03 | 60.4 (50.0–68.8) | 65.4 (59.5–73.8) | <0.01 |
| Alcohol (%) | 17.4% | 15.6% | 20.0% | 0.38 | 16.5% | 14.0% | 0.30 |
| Smoking (%) | 28.5% | 29.9% | 26.3% | 0.50 | 29.5% | 29.8% | 0.95 |
| CCI, mean (range) | 5.4 (4.0–6.0) | 5.3 (4.0–6.0) | 5.0 (4.0–6.0) | 0.37 | 5.5 (4.0–6.0) | 5.5 (5.0–6.0) | 0.94 |
| Line of pembrolizumab (%) | |||||||
| 1 | 63.6% | 64.6% | 62.1% | 0.53 | 64.2% | 58.4% | 0.20 |
| ≥2 | 36.4% | 35.4% | 37.9% | 35.8% | 41.6% | ||
| Concomitant chemotherapy (%) | 54.5% | 50.3% | 61.0% | 0.10 | 54.0% | 51.1% | 0.52 |
| ECOG (%) | |||||||
| <2 | 86.8% | 84.4% | 90.5% | 0.16 | 85.1% | 88.8% | 0.23 |
| ≥2 | 13.2% | 15.6% | 9.5% | 14.9% | 11.2% | ||
| Stage (%) | |||||||
| 3 | 13.2% | 12.2% | 14.7% | 0.57 | 13.0% | 12.5% | 0.86 |
| 4 | 86.8% | 87.8% | 85.3% | 87.0% | 87.5% | ||
| Histologic features (%) | |||||||
| Adenocarcinoma | 67.7% | 66.7% | 69.5% | 0.76 | 67.7% | 76.1% | 0.08 |
| Squamous | 24.4% | 24.5% | 24.2% | 23.7% | 18.9% | ||
| Others | 7.9% | 8.8% | 6.3% | 8.6% | 5.0% | ||
| Metastasis status (%) | |||||||
| Brain | 14.9% | 14.9% | 14.7% | 0.96 | 14.6% | 16.5% | 0.59 |
| Bone | 31.0% | 34.6% | 25.2% | 0.12 | 33.6% | 33.6% | 0.99 |
| Liver | 12.0% | 10.8% | 13.6% | 0.51 | 12.3% | 9.8% | 0.36 |
| Others | 84.7% | 85.0% | 84.2% | 0.86 | 84.9% | 87.2% | 0.46 |
| PD-L1 tumor proportion score (%) | |||||||
| <1% | 11.6% | 11.7% | 11.6% | 0.50 | 12.1% | 9.5% | 0.86 |
| 1–49% | 21.9% | 20.4% | 24.2% | 22.4% | 21.3% | ||
| ≥50% | 47.1% | 51.0% | 41.0% | 48.0% | 51.2% | ||
| Unknown | 19.4% | 16.9% | 23.2% | 17.5% | 18.0% | ||
| Comorbidity | |||||||
| Hypertension (%) | 28.5% | 30.6% | 25.3% | 0.36 | 29.0% | 35.7% | 0.12 |
| Diabetes (%) | 14.8% | 15.6% | 13.6% | 0.67 | 14.5% | 15.7% | 0.71 |
| Dyslipidemia (%) | 11.9% | 12.2% | 11.5% | 0.87 | 13.1% | 8.4% | 0.08 |
| Ischemic heart disease (%) | 5.3% | 4.1% | 7.3% | 0.26 | 4.4% | 3.2% | 0.49 |
| Heart failure (%) | 1.6% | 0.6% | 3.1% | 0.13 | 0.5% | 0.9% | 0.57 |
| Cerebrovascular disease (%) | 4.5% | 4.7% | 4.2% | 0.84 | 5.2% | 2.5% | 0.11 |
| Hypothyroidism (%) | 0.4% | 0.6% | 0.0% | 0.42 | 0.5% | 0.0% | 0.20 |
| COPD (%) | 21.4% | 26.5% | 13.6% | 0.01 | 23.4% | 22.1% | 0.75 |
| Chronic kidney disease (%) | 7.0% | 8.8% | 4.2% | 0.16 | 8.8% | 11.7% | 0.29 |
| Biochemical data | |||||||
| eGFR (mL/min/1.73 m2) | 98.7 (71.6–118.2) | 100.7 (69.8–119.1) | 95.6 (77.4–117.8) | 0.35 | 100.8 (69.8–119.1) | 90.2 (77.4–117.8) | 0.06 |
| ALT (U/L) | 29.0(14–37) | 28.6 (13.0–36.0) | 29.7 (18.0–39.0) | 0.01 | 28.5 (13.0–36.0) | 29.4 (18.0–39.0) | 0.68 |
| AST (U/L) | 31.4(19–33) | 31.6 (18.0–31.0) | 31.0 (20.0–36.0) | 0.05 | 31.6 (18.0–31.0) | 28.3 (20.0–36.0) | 0.22 |
| Total bilirubin (mg/dL) | 0.6 (0.4–0.6) | 0.7 (0.4–0.6) | 0.6 (0.4–0.7) | 0.32 | 0.7 (0.4–0.6) | 0.7 (0.4–0.7) | 0.92 |
| Fasting glucose (mg/dL) | 126.0 (97–132) | 126.3 (98–133) | 125.6 (94–131) | 0.07 | 126.1 (98–133) | 118.8 (94–131) | 0.13 |
| HbA1c (%) | 6.2 (5.6–6.5) | 6.2 (5.6–6.5) | 6.3 (5.6–6.7) | 0.29 | 6.2 (5.6–6.5) | 6.3 (5.6–6.7) | 0.44 |
| WBC (103/uL) | 8.8 (5.9–10.9) | 9.4 (6.1–11.2) | 8.0 (5.7–9.8) | 0.02 | 9.4 (6.1–11.2) | 8.6 (5.7–9.8) | 0.06 |
| Hemoglobin (g/dL) | 11.6 (10.5–13.0) | 11.5 (10.4–13.1) | 11.7 (10.6–13.0) | 0.31 | 11.5 (10.4–13.1) | 11.6 (10.6–13.0) | 0.65 |
| Platelet (103/uL) | 273.7 (187.5–328.5) | 277.8 (196–323) | 267.3 (177–344) | 0.27 | 278.7 (196–323) | 269.0 (177–344) | 0.61 |
| Sensitivity Analyses | Overall Survival (HR, 95% CI) | Time to Tumor Progression (HR, 95% CI) |
|---|---|---|
| Pembrolizumab ≥ 2 mg/kg as standard group † | 0.84 (0.62–1.14) | 0.85 (0.68–1.05) |
| Pembrolizumab ≥ 1.9 mg/kg as standard group † | 0.78 (0.58–1.03) | 0.85 (0.69–1.06) |
| Pembrolizumab ≥ 1.8 mg/kg as standard group † | 0.73 (0.55–0.97) * | 0.81 (0.66–1.01) |
| Propensity score matching cohort (pembrolizumab ≥2 mg/kg as standard group) | 0.83 (0.52–1.34) | 0.86 (0.61–1.20) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, K.-C.; Shao, S.-C.; Chen, H.-Y.; Chan, Y.-Y.; Fang, Y.-F. Comparative Effectiveness and Safety of Standard-Dose and Low-Dose Pembrolizumab in Patients with Non-Small-Cell Lung Cancer: A Multi-Institutional Cohort Study in Taiwan. Cancers 2022, 14, 1157. https://doi.org/10.3390/cancers14051157
Chang K-C, Shao S-C, Chen H-Y, Chan Y-Y, Fang Y-F. Comparative Effectiveness and Safety of Standard-Dose and Low-Dose Pembrolizumab in Patients with Non-Small-Cell Lung Cancer: A Multi-Institutional Cohort Study in Taiwan. Cancers. 2022; 14(5):1157. https://doi.org/10.3390/cancers14051157
Chicago/Turabian StyleChang, Kai-Cheng, Shih-Chieh Shao, Hui-Yu Chen, Yuk-Ying Chan, and Yueh-Fu Fang. 2022. "Comparative Effectiveness and Safety of Standard-Dose and Low-Dose Pembrolizumab in Patients with Non-Small-Cell Lung Cancer: A Multi-Institutional Cohort Study in Taiwan" Cancers 14, no. 5: 1157. https://doi.org/10.3390/cancers14051157
APA StyleChang, K.-C., Shao, S.-C., Chen, H.-Y., Chan, Y.-Y., & Fang, Y.-F. (2022). Comparative Effectiveness and Safety of Standard-Dose and Low-Dose Pembrolizumab in Patients with Non-Small-Cell Lung Cancer: A Multi-Institutional Cohort Study in Taiwan. Cancers, 14(5), 1157. https://doi.org/10.3390/cancers14051157