
Patient Preferences for Treatment Outcomes in Oncology with a Focus on the Older Patient—A Systematic Review

 , ,
, ,  , ,
, , 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Data Synthesis and Analysis
3. Results
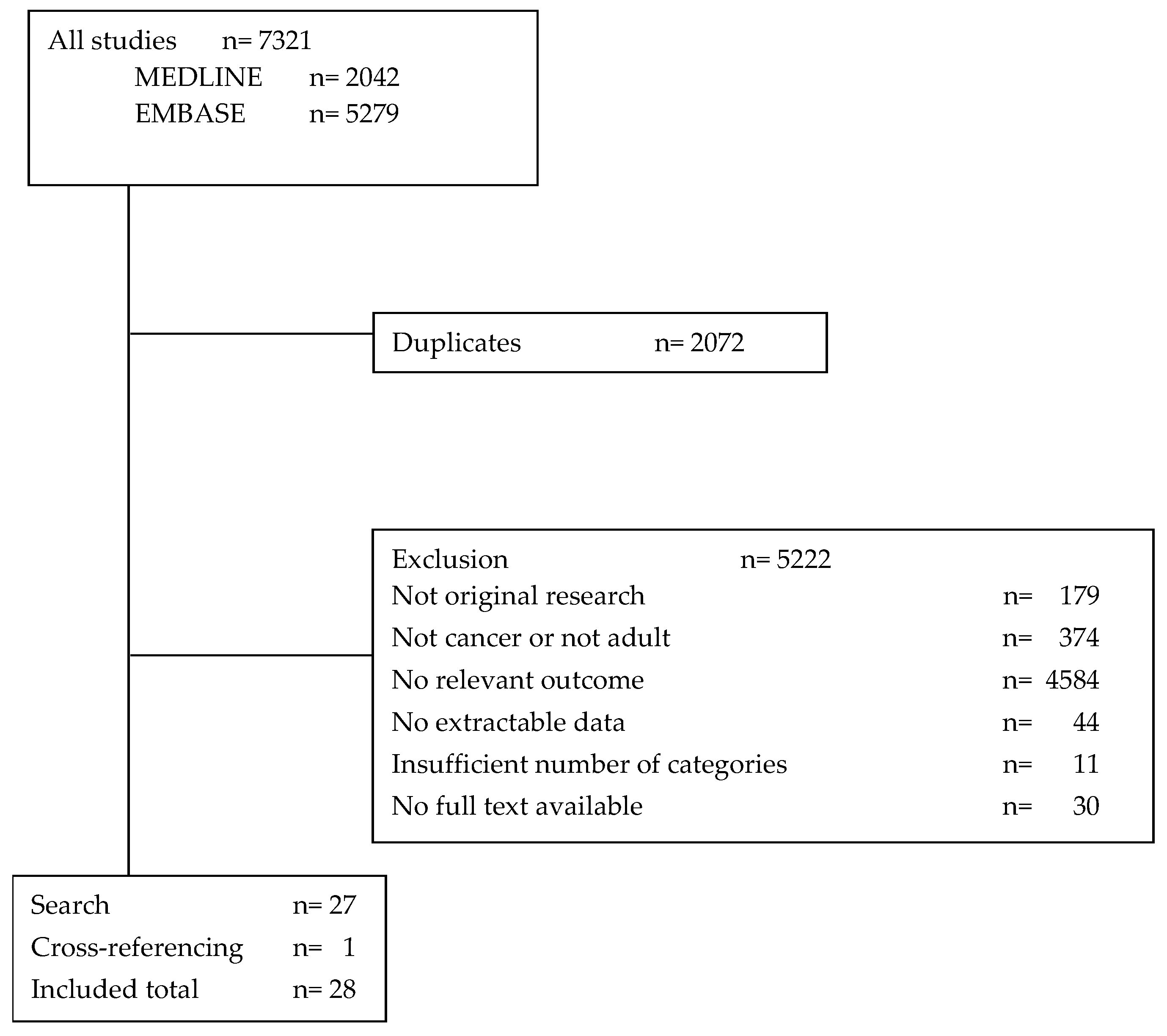
3.1. Search and Study Selection
3.2. Study Characteristics
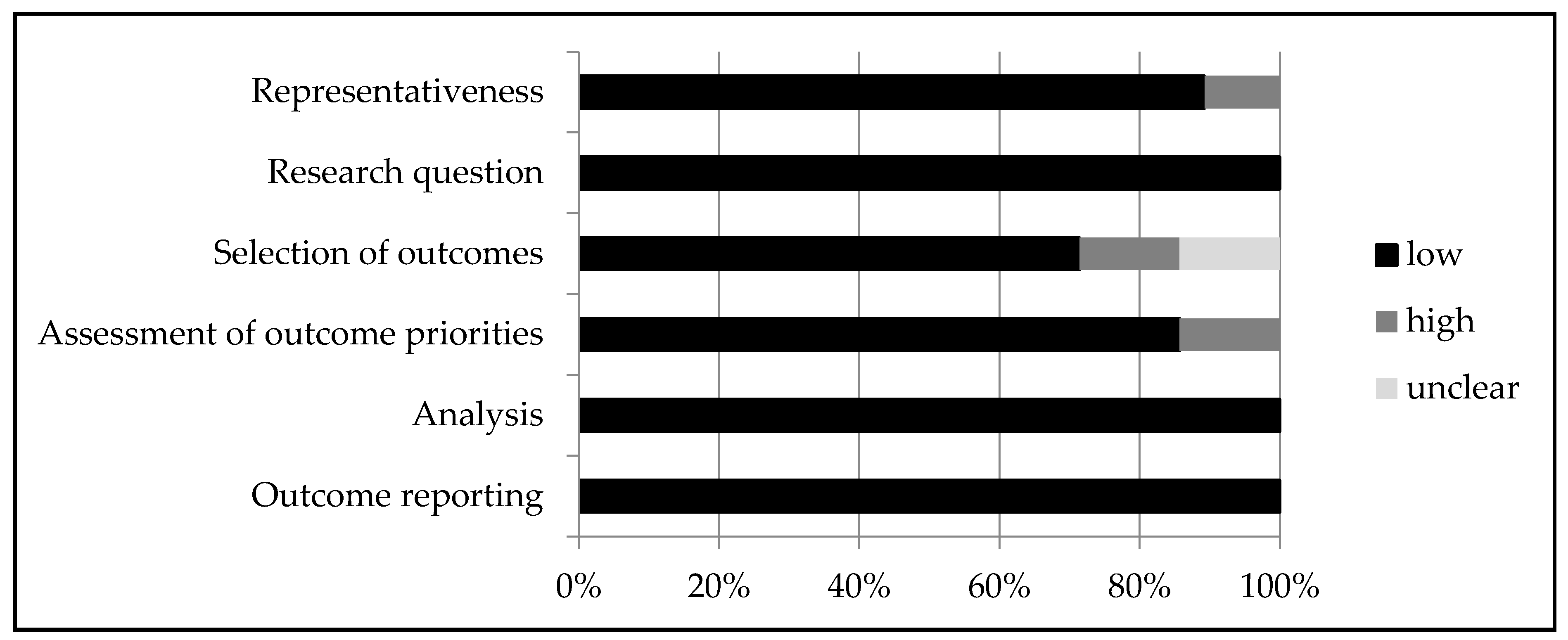
3.3. Quality Assessment
3.4. Categories
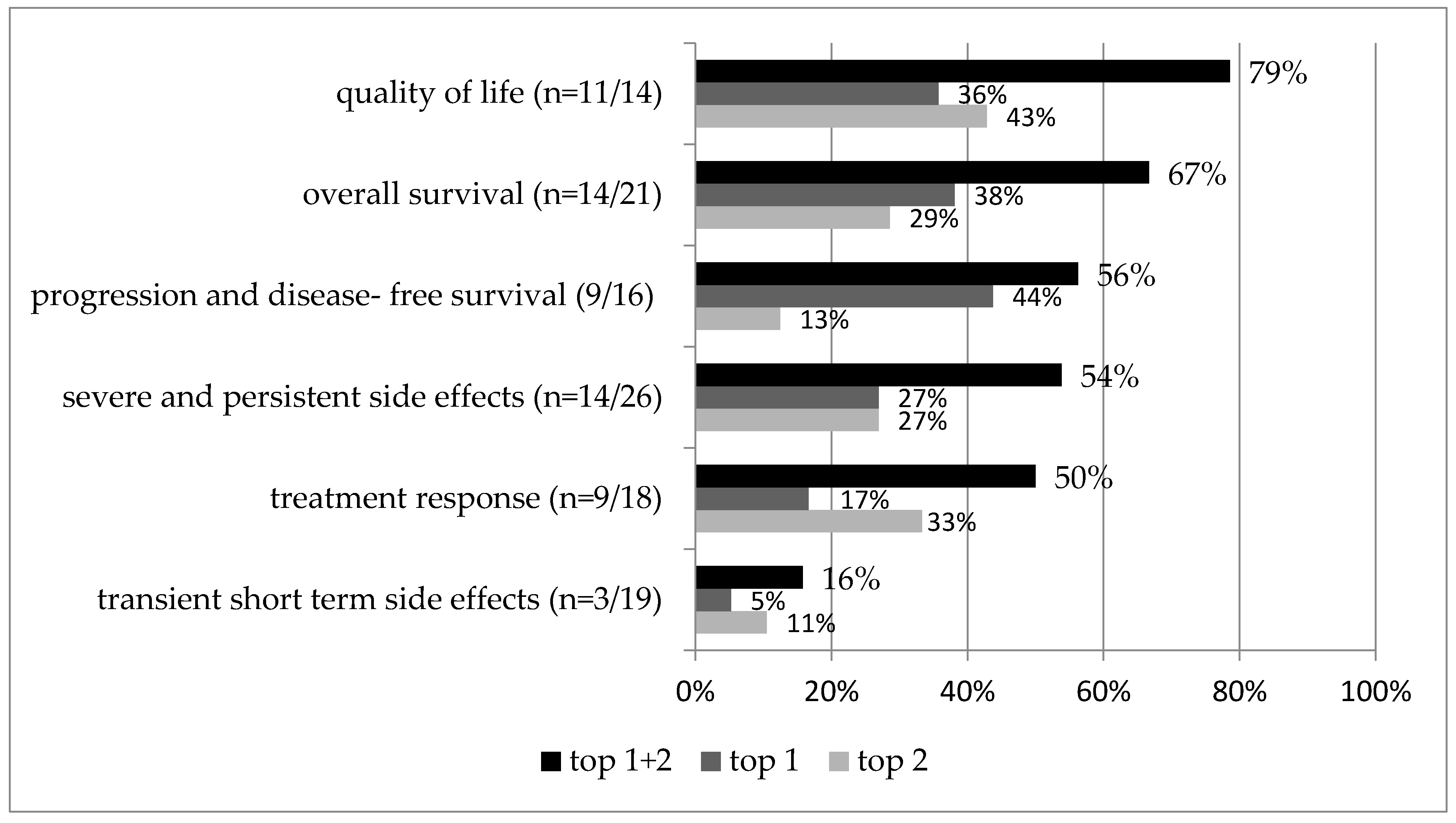
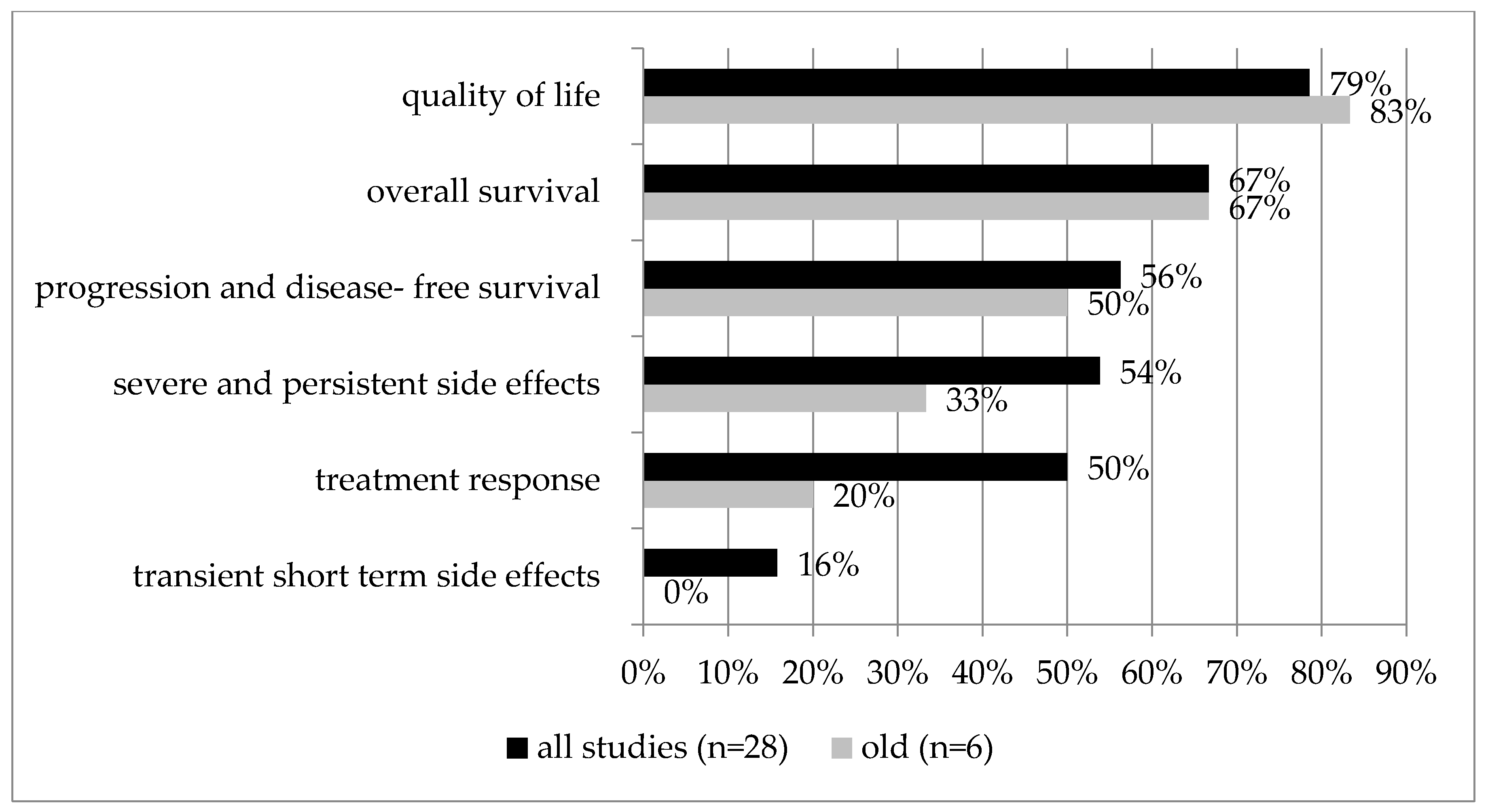
3.5. Most Important Outcome Categories
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Search
Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outcome Categories | Descriptions |
|---|---|
| Quality of life | Long-term maintenance of quality of life and functional status. Also includes other patient reported/centered measurements such as keeping one’s independence and social/role functioning. E.g., quality of life, maintaining independence of (instrumental) activities of daily living (iADL), worries, anxiety |
| Transient short-term side effects | Short-term and transient treatment-related toxicity/adverse events that terminate after cessation of treatment or that only require minimal medication. E.g., diarrhea, hair loss, nausea/vomiting, rash and skin change |
| Severe and persistent side effects | More severe adverse treatment events that require intensive treatment, hospitalization or discontinuation of treatment. Often patients will recover from these events, but it can take a long time (>6 months) and involves intensive treatment. Persistent side effects/sequelae inherent or caused by the treatment are also included here. E.g., severe bleeding, gastrointestinal perforation, heart attack, colostomy, neuropathy, fatigue, scars, permanent fecal incontinence, urinary incontinence, infertility |
| Treatment response | All treatment benefits, except for time-dependant measurements. Treatment benefits other than survival, like symptom reduction, response seen on scans, or risk reductions. E.g., symptom control, local control, complete response, partial response, recurrence risk |
| Progression- and disease-free survival | Progression-free survival or disease-free survival, but not overall survival. A time-dependent measurement that indicates how long the disease is under control or cured. Also a measurement of efficacy, but time-dependent. E.g., disease-free survival, progression-free survival, time to treatment failure |
| Overall survival | Overall survival and mortality independent of the cancer (treatment) at a certain time point during follow-up. E.g., overall survival, mortality at a certain time point, extending life |
Appendix C
| selection | 1. Representativeness of the cohort | + | Participants are patients who have cancer |
| − | Participants are asked to answer as if they have cancer or as if they have a different stage of cancer | ||
| ? | The sampling strategy leads to non-representativeness | ||
| study design | 2. Research question | + | Well-defined research question and hypothesis |
| − | Vaguely described research question | ||
| ? | No research question present | ||
| 3. Selection of outcomes included | + | Clearly described why the different outcomes (= attributes) and levels are included in the study, e.g., based on previous research, pilot study, or qualitative research | |
| − | Described vaguely, but not clear why these items or levels are selected, e.g., in a discussion with researchers | ||
| ? | No description on why these outcomes are chosen | ||
| 4. Assessment of outcome priorities | + | Clear description of the definition of the outcomes and method of assessment and clear understanding of how the outcomes are described to the patient | |
| − | Unclear description of outcomes or unclear method of assessment, e.g., quality of life is mentioned without clear description | ||
| ? | No description of definitions and unclear method of assessment | ||
| outcome | 5. Analysis | + | Clear description of method of analysis |
| − | Unclear description of method of analysis | ||
| ? | No description | ||
| 6. Outcome reporting | + | Scores for all outcomes separately reported | |
| ± | Outcomes reported, but hard to make a ranking or early stage and advanced stage of disease not separately reported | ||
| − | Not all scores reported | ||
| ? | Unclear whether all outcomes are reported |
Appendix D
| Author, Year | Representativeness | Research Question | Selection of Outcomes | Assessment of Outcome Priorities | Analysis | Outcome Reporting |
|---|---|---|---|---|---|---|
| Johnson, 2006 | + | + | + | + | + | + |
| Pieterse, 2007 | + | + | + | + | + | + |
| Thrumurthy, 2011 | + | + | + | − | + | + |
| Mohamed, 2011 | + | + | + | + | + | + |
| Park, 2012 | − | + | + | + | + | ± |
| Jorgensen, 2013 | + | + | − | + | + | + |
| Havrilesky, 2014 | + | + | + | + | + | + |
| DaCosta, 2014 | + | + | + | + | + | + |
| Molinari, 2014 | − | + | − | + | + | + |
| Muhlbacher, 2015 | + | + | + | + | + | + |
| Uemura, 2016 | + | + | + | + | + | + |
| Thill,2016 | + | + | + | + | + | ± |
| Chau, 2016 | + | + | + | + | + | + |
| Gonzalez, 2017 | + | + | + | + | + | + |
| Schmidt, 2017 | + | + | + | + | + | + |
| Bröckelmann, 2019 | + | + | + | + | + | + |
| Sun, 2019 | + | + | + | + | + | + |
| Liu, 2019 | + | + | + | − | + | + |
| Festen, 2019 | + | + | ? | + | + | + |
| van der Valk, 2020 | + | + | + | + | + | + |
| Valenti, 2020 | + | + | ? | + | + | ± |
| Wong, 2020 | − | + | + | + | + | + |
| Stegmann, 2020 | + | + | ? | + | + | ± |
| Fifer, 2020 | + | + | + | − | + | + |
| Khan, 2020 | + | + | − | + | + | + |
| Festen, 2021 | + | + | ? | + | + | + |
| Werner, 2021 | + | + | + | + | + | + |
| Weilandt, 2021 | + | + | − | − | + | + |
References
- Soto-Perez-De-Celis, E.; Li, D.; Yuan, Y.; Lau, M.; Hurria, A. Geriatric Oncology 2, Functional versus Chronological Age: Geriatric Assessments to Guide Decision Making in Older Patients with Cancer. Lancet Oncol. 2018, 19, e305–e316. [Google Scholar] [CrossRef]
- DuMontier, C.; Loh, K.P.; Soto-Perez-de-Celis, E.; Dale, W. Decision Making in Older Adults with Cancer. J. Clin. Oncol. 2021, 39, 2164–2174. [Google Scholar] [CrossRef] [PubMed]
- Kane, H.L.; Halpern, M.T.; Squiers, L.B.; Treiman, K.A.; McCormack, L.A. Implementing and Evaluating Shared Decision Making in Oncology Practice. CA Cancer J. Clin. 2014, 64, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Williams, C.P.; Miller-Sonet, E.; Nipp, R.D.; Kamal, A.H.; Love, S.; Rocque, G.B. Importance of Quality-of-Life Priorities and Preferences Surrounding Treatment Decision Making in Patients with Cancer and Oncology Clinicians. Cancer 2020, 126, 3534–3541. [Google Scholar] [CrossRef] [PubMed]
- Stiggelbout, A.M.; Pieterse, A.H.; De Haes, J.C.J.M. Shared Decision Making: Concepts, Evidence, and Practice. Patient Educ. Couns. 2015, 98, 1172–1179. [Google Scholar] [CrossRef]
- Hamaker, M.E.; van Walree, I.C.; Seghers, P.A.L.; van den Bos, F.; Soubeyran, P.; O’Hanlon, S.; Rostoft, S. Information Needs of Older Patients Newly Diagnosed with Cancer. J. Geriatr. Oncol. 2021, in press. [CrossRef]
- Extermann, M. Interaction between Comorbidity and Cancer. Cancer Control 2007, 14, 14–22. [Google Scholar] [CrossRef]
- Extermann, M.; Lee, H. Measurement and Impact of Comorbidity in Older Cancer Patients. Crit. Rev. Oncol. Hematol. 2000, 35, 181–200. [Google Scholar] [CrossRef]
- Sarfati, D.; Koczwara, B.; Jackson, C. The Impact of Comorbidity on Cancer and Its Treatment. CA Cancer J. Clin. 2016, 66, 337–350. [Google Scholar] [CrossRef]
- Wildiers, H.; Mauer, M.; Pallis, A.; Hurria, A.; Mohile, S.G.; Luciani, A.; Curigliano, G.; Extermann, M.; Lichtman, S.M.; Ballman, K.; et al. End Points and Trial Design in Geriatric Oncology Research: A Joint European Organisation for Research and Treatment of Cancer-Alliance for Clinical Trials in Oncology-International Society of Geriatric Oncology Position Article. J. Clin. Oncol. 2013, 31, 3711–3718. [Google Scholar] [CrossRef]
- Karolina, A.; Maguire, R. A Systematic Review of the Factors Associated with Regret Post-Cancer Treatment. J. Psychosoc. Oncol. 2020, 40, 1–23. [Google Scholar] [CrossRef]
- Lis, C.G.; Rodeghier, M.; Gupta, D. Patient Preference and Adherence Distribution and Determinants of Patient Satisfaction in Oncology: A Review of the Literature. Patient Prefer. Adherence 2009, 3, 287–304. [Google Scholar] [PubMed]
- Blinman, P.; King, M.; Norman, R.; Viney, R.; Stockler, M.R. Preferences for Cancer Treatments: An Overview of Methods and Applications in Oncology. Ann. Oncol. 2012, 23, 1104–1110. [Google Scholar] [CrossRef] [PubMed]
- Stegmann, M.E.; Festen, S.; Brandenbarg, D.; Schuling, J.; van Leeuwen, B.; de Graeff, P.; Berendsen, A.J. Using the Outcome Prioritization Tool (OPT) to Assess the Preferences of Older Patients in Clinical Decision-Making: A Review. Maturitas 2019, 128, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Fried, T.R.; Tinetti, M.; Agostini, J.; Iannone, L.; Towle, V. Health Outcome Prioritization to Elicit Preferences of Older Persons with Multiple Health Conditions. Patient Educ. Couns. 2011, 83, 278–282. [Google Scholar] [CrossRef]
- Thill, M.; Pisa, G.; Isbary, G. Targets for Neoadjuvant Thearpy-The Preferences of Patients with Early Breast Cancer. Geburtshilfe Frauenheilkd. 2016, 76, 551–556. [Google Scholar]
- Doolin, J.W.; Halpin, M.; Berry, J.L.; Hshieh, T.; Zerillo, J.A. Why Focus on Patient-Reported Outcome Measures in Older Colorectal Cancer Patients? Eur. J. Surg. Oncol. 2020, 46, 394–401. [Google Scholar] [CrossRef]
- LeBlanc, T.W.; Abernethy, A.P. Patient-Reported Outcomes in Cancer Care-Hearing the Patient Voice at Greater Volume. Nat. Rev. Clin. Oncol. 2017, 14, 763–772. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Center for Open Science. OSF-Open Registry. Available online: https://osf.io/ekq6u (accessed on 19 January 2022).
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analysis. 2012. Available online: https://web.archive.org/web/20210716121605id_/http://www3.med.unipmn.it/dispense_ebm/2009-2010/Corso%20Perfezionamento%20EBM_Faggiano/NOS_oxford.pdf (accessed on 22 October 2021).
- Bridges, J.F.P.; Hauber, A.B.; Marshall, D.; Lloyd, A.; Prosser, L.A.; Regier, D.A.; Johnson, F.R.; Mauskopf, J. Conjoint Analysis Applications in Health—A Checklist: A Report of the ISPOR Good Research Practices for Conjoint Analysis Task Force. Value Health 2011, 14, 403–413. [Google Scholar] [CrossRef]
- Yepes-Nuñez, J.J.; Zhang, Y.; Xie, F.; Alonso-Coello, P.; Selva, A.; Schünemann, H.; Guyatt, G. Forty-Two Systematic Reviews Generated 23 Items for Assessing the Risk of Bias in Values and Preferences’ Studies. J. Clin. Epidemiol. 2017, 85, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration (FDA). Patient Preference Information-Guidance for Industry, Food and Drug Administration Staff, and Other Stakeholders; FDA: Silver Spring, MD, USA, 2016.
- Pieterse, A.H.; Berkers, F.; Baas-Thijssen, M.C.M.; Marijnen, C.A.M.; Stiggelbout, A.M. Adaptive Conjoint Analysis as Individual Preference Assessment Tool: Feasibility through the Internet and Reliability of Preferences. Patient Educ. Couns. 2010, 78, 224–233. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, A.F.; Hauber, A.B.; Neary, M.P. Patient Benefit-Risk Preferences for Targeted Agents in the Treatment of Renal Cell Carcinoma. Pharmacoeconomics 2011, 29, 977–988. [Google Scholar] [CrossRef] [PubMed]
- Thrumurthy, S.G.; Morris, J.J.A.; Mughal, M.M.; Ward, J.B. Discrete-Choice Preference Comparison between Patients and Doctors for the Surgical Management of Oesophagogastric Cancer. Br. J. Surg. 2011, 98, 1124–1131. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, M.L.; Young, J.M.; Solomon, M.J. Adjuvant Chemotherapy for Colorectal Cancer: Age Differences in Factors Influencing Patients’ Treatment Decisions. Patient Prefer. Adherence 2013, 7, 827–834. [Google Scholar] [CrossRef]
- Molinari, M.; de Coutere, S.; Krahn, M.; Helton, S.; Urbach, D.R. Patients’ Preferences and Trade-Offs for the Treatment of Early Stage Hepatocellular Carcinoma. J. Surg. Res. 2014, 189, 57–67. [Google Scholar] [CrossRef]
- van der Valk, M.J.M.; van der Sande, M.E.; Toebes, R.E.; Breukink, S.O.; Bröker, M.E.E.; Doornebosch, P.G.; Maliko, N.; Neijenhuis, P.A.; Marinelli, A.W.K.S.; Peters, F.P.; et al. Importance of Patient Reported and Clinical Outcomes for Patients with Locally Advanced Rectal Cancer and Their Treating Physicians. Do Clinicians Know What Patients Want? Eur. J. Surg. Oncol. 2020, 46, 1634–1641. [Google Scholar] [CrossRef]
- Werner, R.N.; Gaskins, M.; Dressler, C.; Nast, A.; Schaefer, C.; Aigner, F.; Siegel, R. Measuring Importance of Outcomes to Patients: A Cross-Sectional Survey for the German Anal Cancer Guideline. J. Clin. Epidemiol. 2021, 129, 40–50. [Google Scholar] [CrossRef]
- Park, M.H.; Jo, C.; Bae, E.Y.; Lee, E.K. A Comparison of Preferences of Targeted Therapy for Metastatic Renal Cell Carcinoma between the Patient Group and Health Care Professional Group in South Korea. Value Health 2012, 15, 933–939. [Google Scholar] [CrossRef]
- Havrilesky, L.J.; Secord, A.A.; Ehrisman, J.A.; Berchuck, A.; Valea, F.A.; Lee, P.S.; Gaillard, S.L.; Samsa, G.P.; Cella, D.; Weinfurt, K.P.; et al. Patient Preferences in Advanced or Recurrent Ovarian Cancer. Cancer 2014, 120, 3651–3659. [Google Scholar] [CrossRef]
- Dacosta Dibonaventura, M.; Copher, R.; Basurto, E.; Faria, C.; Lorenzo, R. Patient Preferences and Treatment Adherence among Women Diagnosed with Metastatic Breast Cancer. Am. Health Drug Benefits 2014, 7, 386–396. [Google Scholar] [PubMed]
- Mühlbacher, A.C.; Bethge, S. Patients’ Preferences: A Discrete-Choice Experiment for Treatment of Non-Small-Cell Lung Cancer. Eur. J. Health Econ. 2015, 16, 657–670. [Google Scholar] [CrossRef] [PubMed]
- Uemura, H.; Matsubara, N.; Kimura, G.; Yamaguchi, A.; Ledesma, D.A.; DiBonaventura, M.; Mohamed, A.F.; Basurto, E.; McKinnon, I.; Wang, E.; et al. Patient Preferences for Treatment of Castration-Resistant Prostate Cancer in Japan: A Discrete-Choice Experiment. BMC Urol. 2016, 16, 63. [Google Scholar] [CrossRef] [PubMed]
- Chun-Leung Chau, D.; Wang, D.; Tedesco, A.; McGuffin, M.; di Prospero, L.; Fitch, M.; Cao, X.; Feldman-Stewart, D.; Ellis, J.; Szumachter, E. Prostate Cancer Patients’ Preferences for Intermittent vs. Continuous Androgen Deprivation—A Pilot Institutional Study. J. Med. Imaging Radiat. Sci. 2016, 47, 108–112. [Google Scholar] [CrossRef] [PubMed][Green Version]
- González, J.M.; Ogale, S.; Morlock, R.; Posner, J.; Hauber, B.; Sommer, N.; Grothey, A. Patient and Physician Preferences for Anticancer Drugs for the Treatment of Metastatic Colorectal Cancer: A Discrete-Choice Experiment. Cancer Manag. Res. 2017, 9, 149–158. [Google Scholar] [CrossRef]
- Liu, F.X.; Witt, E.A.; Ebbinghaus, S.; Dibonaventura Beyer, G.; Basurto, E.; Joseph, R.W. Patient and Oncology Nurse Preferences for the Treatment Options in Advanced Melanoma: A Discrete Choice Experiment. Cancer Nurs. 2019, 42, E52–E59. [Google Scholar] [CrossRef]
- Wong, X.Y.; Lim, A.Q.J.; Shen, Q.; Chia, J.W.K.; Chew, M.H.; Tan, W.S.; Wee, H.L. Patient Preferences and Predicted Relative Uptake for Targeted Therapies in Metastatic Colorectal Cancer: A Discrete Choice Experiment. Curr. Med. Res. Opin. 2020, 36, 1677–1686. [Google Scholar] [CrossRef] [PubMed]
- Stegmann, M.E.; Brandenbarg, D.; Berendsen, A.J.; Reyners, A.K.L.; van Geffen, W.H.; Hiltermann, T.J.N. Prioritisation of Treatment Goals among Older Patients with Non-Curable Cancer: The OPTion Randomised Controlled Trial in Dutch Primary Care. Br. J. Gen. Pract. 2020, 70, E450–E456. [Google Scholar] [CrossRef]
- Weilandt, J.; Diehl, K.; Schaarschmidt, M.L.; Kiecker, F.; Sasama, B.; Pronk, M.; Ohletz, J.; Könnecke, A.; Müller, V.; Utikal, J.; et al. Patient Preferences in Adjuvant and Palliative Treatment of Advanced Melanoma: A Discrete Choice Experiment. Acta Derm.-Venereol. 2020, 100, 1–9. [Google Scholar] [CrossRef]
- Johnson, F.R.; Hauber, A.B.; Osoba, D.; Hsu, M.A.; Coombs, J.; Copley-Merriman, C. Are Chemotherapy Patients’ HRQoL Importance Weights Consistent with Linear Scoring Rules? A Stated-Choice Approach. Qual. Life Res. 2006, 15, 285–298. [Google Scholar] [CrossRef]
- Schmidt, K.; Damm, K.; Vogel, A.; Golpon, H.; Manns, M.P.; Welte, T.; Graf von der Schulenburg, J.M. Therapy Preferences of Patients with Lung and Colon Cancer: A Discrete Choice Experiment. Patient Prefer. Adherence 2017, 11, 1647–1656. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Wang, H.; Xu, N.; Li, J.; Shi, J.; Zhou, N.; Ni, M.; Hu, X.; Chen, Y. Patient Preferences for Chemotherapy in the Treatment of Non-Small Cell Lung Cancer: A Multicenter Discrete Choice Experiment (DCE) Study in China. Patient Prefer. Adherence 2019, 13, 1701–1709. [Google Scholar] [CrossRef] [PubMed]
- Bröckelmann, P.J.; McMullen, S.; Wilson, J.B.; Mueller, K.; Goring, S.; Stamatoullas, A.; Zagadailov, E.; Gautam, A.; Huebner, D.; Dalal, M.; et al. Patient and Physician Preferences for First-Line Treatment of Classical Hodgkin Lymphoma in Germany, France and the United Kingdom. Br. J. Haematol. 2019, 184, 202–214. [Google Scholar] [CrossRef]
- Festen, S.; Kok, M.; Hopstaken, J.S.; van der Wal-Huisman, H.; van der Leest, A.; Reyners, A.K.L.; de Bock, G.H.; de Graeff, P.; van Leeuwen, B.L. How to Incorporate Geriatric Assessment in Clinical Decision-Making for Older Patients with Cancer. An Implementation Study. J. Geriatr. Oncol. 2019, 10, 951–959. [Google Scholar] [CrossRef] [PubMed]
- Valentí, V.; Ramos, J.; Pérez, C.; Capdevila, L.; Ruiz, I.; Tikhomirova, L.; Sánchez, M.; Juez, I.; Llobera, M.; Sopena, E.; et al. Increased Survival Time or Better Quality of Life? Trade-off between Benefits and Adverse Events in the Systemic Treatment of Cancer. Clin. Transl. Oncol. Off. Publ. Fed. Span. Oncol. Soc. Natl. Cancer Inst. Mex. 2020, 22, 935–942. [Google Scholar] [CrossRef] [PubMed]
- Fifer, S.; Galinsky, J.; Richard, S. Myeloma Patient Value Mapping: A Discrete Choice Experiment on Myeloma Treatment Preferences in the UK. Patient Prefer. Adherence 2020, 14, 1283–1293. [Google Scholar] [CrossRef]
- Festen, S.; Stegmann, M.E.; Prins, A.; van Munster, B.C.; van Leeuwen, B.L.; Halmos, G.B.; de Graeff, P.; Brandenbarg, D. How Well Do Healthcare Professionals Know of the Priorities of Their Older Patients Regarding Treatment Outcomes? Patient Educ. Couns. 2021, 104, 2358–2363. [Google Scholar] [CrossRef]
- Khan, N.; Feliciano, J.; Müller, K.; He, M.; Tao, R.; Korol, E.; Dalal, M.; Rebeira, M.; Matasar, M. Patient Preferences for First-Line Treatment of Classical Hodgkin Lymphoma: A US Survey and Discrete Choice Experiment. Leuk. Lymphoma 2020, 2630–2637. [Google Scholar] [CrossRef]
- Shrestha, A.; Martin, C.; Burton, M.; Walters, S.; Collins, K.; Wyld, L. Quality of Life versus Length of Life Considerations in Cancer Patients: A Systematic Literature Review. Psycho-Oncology 2019, 28, 1367–1380. [Google Scholar] [CrossRef]
- Meropol, N.J.; Egleston, B.L.; Buzaglo, J.S.; Benson, A.B.; Cegala, D.J.; Diefenbach, M.A.; Fleisher, L.; Miller, S.M.; Sulmasy, D.P.; Weinfurt, K.P.; et al. Cancer Patient Preferences for Quality and Length of Life. Cancer 2008, 113, 3459–3466. [Google Scholar] [CrossRef]
- van der Plas-Krijgsman, W.G.; de Boer, A.Z.; de Jong, P.; Bastiaannet, E.; van den Bos, F.; Mooijaart, S.P.; Liefers, G.J.; Portielje, J.E.A.; de Glas, N.A. Predicting Disease-Related and Patient-Reported Outcomes in Older Patients with Breast Cancer—A Systematic Review. J. Geriatr. Oncol. 2021, 12, 696–704. [Google Scholar] [CrossRef] [PubMed]
- Hamaker, M.E.; Schulkes, K.J.; ten Bokkel Huinink, D.; van Munster, B.C.; van Huis, L.H.; van den Bos, F. Evaluation and Reporting of Quality of Life Outcomes in Phase III Chemotherapy Trials for Poor Prognosis Malignancies. Qual. Life Res. 2017, 26, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Scheepers, E.R.M.; van Huis-Tanja, L.H.; Emmelot-Vonk, M.H.; Hamaker, M.E. Study Objectives in Clinical Trials in Older Patients with Solid Malignancies: Do We Measure What Matters? Qual. Life Res. 2021, 30, 1833–1839. [Google Scholar] [CrossRef] [PubMed]
- Bien, D.R.; Danner, M.; Vennedey, V.; Civello, D.; Evers, S.M.; Hiligsmann, M. Patients’ Preferences for Outcome, Process and Cost Attributes in Cancer Treatment: A Systematic Review of Discrete Choice Experiments. Patient 2017, 10, 553–565. [Google Scholar] [CrossRef] [PubMed]
- Guerra, R.L.; Castaneda, L.; de Albuquerque, R.D.C.R.; Ferreira, C.B.T.; Corrêa, F.D.M.; Fernandes, R.R.A.; de Almeida, L.M. Patient Preferences for Breast Cancer Treatment Interventions: A Systematic Review of Discrete Choice Experiments. Patient 2019, 12, 559–569. [Google Scholar] [CrossRef]
- Fried, T.R.; Bradley, E.H. What Matters to Seriously Ill Older Persons Making End-of-Life Treatment Decisions? A Qualitative Study. J. Palliat. Med. 2003, 6, 237–244. [Google Scholar] [CrossRef]
- Dhakal, P.; Wichman, C.S.; Pozehl, B.; Weaver, M.; Fisher, A.L.; Bociek, R.G.; Bhatt, V.R.; Vose, J. Preferences of Adults with Cancer for Systemic Cancer Treatment: Do Preferences Differ Based on Age? Future Oncol. 2021, 18, 311–321. [Google Scholar] [CrossRef]
- Hoffman, R.M.; Lo, M.; Clark, J.A.; Albertsen, P.C.; Barry, M.J.; Goodman, M.; Penson, D.F.; Stanford, J.L.; Stroup, A.M.; Hamilton, A.S. Treatment Decision Regret Among Long-Term Survivors of Localized Prostate Cancer: Results From the Prostate Cancer Outcomes Study. J. Clin. Oncol. 2017, 35, 2306–2314. [Google Scholar] [CrossRef]
- Kuijpers, M.M.T.; Veenendaal, H.; Engelen, V.; Visserman, E.; Noteboom, E.A.; Stiggelbout, A.M.; May, A.M.; Wit, N.; Wall, E.; Helsper, C.W. Shared Decision Making in Cancer Treatment: A Dutch National Survey on Patients’ Preferences and Perceptions. Eur. J. Cancer Care 2021, 31, e13534. [Google Scholar] [CrossRef]
- Rocque, G.B.; Rasool, A.; Williams, B.R.; Wallace, A.S.; Niranjan, S.J.; Halilova, K.I.; Turkman, Y.E.; Ingram, S.A.; Williams, C.P.; Forero-Torres, A.; et al. What Is Important When Making Treatment Decisions in Metastatic Breast Cancer? A Qualitative Analysis of Decision-Making in Patients and Oncologists. Oncologist 2019, 24, 1313–1321. [Google Scholar] [CrossRef]
- Festen, S.; van Twisk, Y.Z.; van Munster, B.C.; de Graeff, P. ‘What Matters to You?’ Health Outcome Prioritisation in Treatment Decision-Making for Older Patients. Age Ageing 2021, 50, 2264–2269. [Google Scholar] [CrossRef] [PubMed]
- Hazlewood, G.S. Measuring Patient Preferences: An Overview of Methods with a Focus on Discrete Choice Experiments. Rheum. Dis. Clin. N. Am. 2018, 44, 337–347. [Google Scholar] [CrossRef] [PubMed]




| Author, Year | Country | n | % Male | Me(di)an Age (SD, Range or Percentage Older) | Type of Cancer | Treatment Setting |
|---|---|---|---|---|---|---|
| Pieterse [25], 2007 | NL | 66 | 68% | 64 (±9) | Gastrointestinal | Curative |
| Mohamed [26] 2011 | USA | 138 | 49% | 57 (±9) | Renal cell | Curative |
| Thrumurthy [27] 2011 | UK | 81 | 77% | 67 (38% > 70) | Esophageal | Curative |
| * Jorgensen [28], 2013 | Australia | 68 | 100% | 64 (51% > 65) | Colorectal | Curative |
| Molinari [29], 2014 | Canada | 75 | 61% | 51 (±11) | HCC | Curative |
| Thill [16], 2016 | Germany | 41 | 100% | 50 (29–76) | Breast | Curative |
| van der Valk [30] 2020 | NL | 94 | 43% | 62 (±9) | Rectal | Curative |
| Werner [31], 2021 | Germany | 37 | 51% | 59 (±9) | Anal/colorectal | Curative |
| Park [32], 2012 | Korea | 140 | 37% | 57 | Renal cell | Palliative |
| Havrilesky [33], 2014 | USA | 95 | 0% | 60 (±10) | Ovarian | Palliative |
| DaCosta [34], 2014 | USA | 181 | 0% | 52 (±9) | Breast | Palliative |
| Muhlbacher [35], 2015 | Germany | 211 | 65% | 59 (±8) | NSCLC | Palliative |
| * Uemura [36], 2016 | Japan | 133 | 100% | 75 (±7) | Prostate | Palliative |
| * Chau [37], 2016 | Canada | 36 | 100% | 73 | Prostate | Palliative |
| Gonzalez [38], 2017 | USA | 127 | 54% | 46 (±16) | Colorectal | Palliative |
| Liu [39], 2019 | USA | 200 | 40% | 34% >50 | Melanoma | Palliative |
| Wong [40], 2020 | Singapore | 169 | 58% | 62 (±11) | Colorectal | Palliative |
| * Stegmann [41], 2020 | NL | 53 | 72% | 75 (±7) | Various types | Palliative |
| Weilandt [42], 2021 | Germany | 150 | 60% | 59 (23–85) | Melanoma | Both |
| Johnson [43], 2006 | USA | 375 | 30% | 61 (±12) | Various types | Both |
| Schmidt [44], 2017 | Germany | 310 | 62% | 63 (±11) | Various types | Both |
| Sun [45], 2019 | China | 361 | 63% | 58 (31–82) | NSCLC | Both |
| Bröckelmann [46], 2019 | EU | 289 | 64% | 36 (19–75) | Lymphoma | Both |
| * Festen [47], 2019 | NL | 197 | 56% | 78 (70–93) | Various types | Both |
| Valenti [48], 2020 | Spain | 100 | 51% | 64 (29–85) | Various types | Both |
| Fifer [49], 2020 | UK | 419 | 44% | 93% >50 | MM | Both |
| * Festen [50], 2021 | NL | 87 | 52% | 76 (IQR 72–80) | Various types | Both |
| Khan [51], 2020 | USA | 141 | 50% | 35 (19–69) | Lymphoma | Both |
| STUDY | Methods | Outcome Categories | ||||||
|---|---|---|---|---|---|---|---|---|
| Author | Year | Elicitation Method | Quality of Life | Transient Short Term Side Effects | Severe and Persistent Side Effects | Treatment Response | Progression- and Disease-Free Survival | Overall Survival |
| Curative Setting Studies | ||||||||
| Pieterse [25] | 2007 | CA | 5 | 4 | 3 | |||
| Thrumurthy [27] | 2011 | DCE | 5 | 3 | 4 | 2 | ||
| Mohamed [26] | 2011 | DCE | 3 | 4 | 5 | |||
| * Jorgensen [28] | 2013 | Rating scale | 3 | 2 | 2 | 5 | 4 | |
| Molinari [29] | 2014 | Trade-off | 2 | 5 | 4 | 3 | ||
| Thill [16] | 2016 | AHP | 2 | 3 | 5 | 4 | ||
| Bröckelmann [46] | 2019 | DCE | 2 | 4 | 5 | 3 | ||
| van der Valk [30] | 2020 | CA | 4 | 5 | 3 | 3 | ||
| Khan [51] | 2020 | DCE | 5 | 3 | 4 | |||
| Werner [31] | 2021 | Rating scale | 4 | 2 | 1 | 3 | 3 | 5 |
| Palliative Setting Studies | ||||||||
| Havrilesky [33] | 2014 | DCE | 4 | 3 | 2 | 5 | ||
| DaCosta [34] | 2014 | CA | 3 | 2 | 4 | 5 | ||
| Park [32] | 2012 | DCE | 5 | 4 | 3 | |||
| Muhlbacher [35] | 2015 | DCE | 3 | 2 | 5 | 5 | ||
| * Uemura [36] | 2016 | DCE | 4 | 1 | 5 | 2 | 3 | |
| * Chau [37] | 2016 | Rating scale | 4 | 1 | 5 | 3 | 2 | |
| Gonzalez [38] | 2017 | DCE | 3 | 5 | 4 | |||
| Liu [39] | 2019 | DCE | 4 | 3 | 2 | 5 | ||
| Bröckelmann [46] | 2019 | DCE | 2 | 3 | 5 | 4 | ||
| Wong [40] | 2020 | DCE | 4 | 5 | 3 | |||
| Khan [50] | 2020 | DCE | 4 | 3 | 5 | |||
| * Stegmann [41] | 2020 | OPT | 5 | 3 | 4 | |||
| Weilandt [42] | 2021 | DCE | 3 | 2 | 4 | 1 | 5 | |
| Both Settings Studies | ||||||||
| Johnson [43] | 2006 | CA | 5 | 3 | 4 | |||
| Schmidt [44] | 2017 | DCE | 4 | 3 | 5 | |||
| Sun [45] | 2019 | DCE | 2 | 3 | 4 | 5 | ||
| * Festen [47] | 2019 | OPT | 5 | 3 | 4 | |||
| Fifer [49] | 2020 | DCE | 3 | 3 | 4 | 5 | ||
| Valenti [48] | 2020 | CA | 4 | 3 | 3 | 5 | ||
| * Festen [50] | 2021 | OPT | 5 | 3 | 4 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seghers, P.A.L.; Wiersma, A.; Festen, S.; Stegmann, M.E.; Soubeyran, P.; Rostoft, S.; O’Hanlon, S.; Portielje, J.E.A.; Hamaker, M.E. Patient Preferences for Treatment Outcomes in Oncology with a Focus on the Older Patient—A Systematic Review. Cancers 2022, 14, 1147. https://doi.org/10.3390/cancers14051147
Seghers PAL, Wiersma A, Festen S, Stegmann ME, Soubeyran P, Rostoft S, O’Hanlon S, Portielje JEA, Hamaker ME. Patient Preferences for Treatment Outcomes in Oncology with a Focus on the Older Patient—A Systematic Review. Cancers. 2022; 14(5):1147. https://doi.org/10.3390/cancers14051147
Chicago/Turabian StyleSeghers, Petronella A. L. (Nelleke), Anke Wiersma, Suzanne Festen, Mariken E. Stegmann, Pierre Soubeyran, Siri Rostoft, Shane O’Hanlon, Johanneke E. A. Portielje, and Marije E. Hamaker. 2022. "Patient Preferences for Treatment Outcomes in Oncology with a Focus on the Older Patient—A Systematic Review" Cancers 14, no. 5: 1147. https://doi.org/10.3390/cancers14051147
APA StyleSeghers, P. A. L., Wiersma, A., Festen, S., Stegmann, M. E., Soubeyran, P., Rostoft, S., O’Hanlon, S., Portielje, J. E. A., & Hamaker, M. E. (2022). Patient Preferences for Treatment Outcomes in Oncology with a Focus on the Older Patient—A Systematic Review. Cancers, 14(5), 1147. https://doi.org/10.3390/cancers14051147