
Overall Survival and Prognostic Factors among Older Patients with Metastatic Pancreatic Cancer: A Retrospective Analysis Using a Hospital Database

 , , ,
, , , 

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Data Collection
2.3. Outcomes
2.4. Statistical Analysis
3. Results
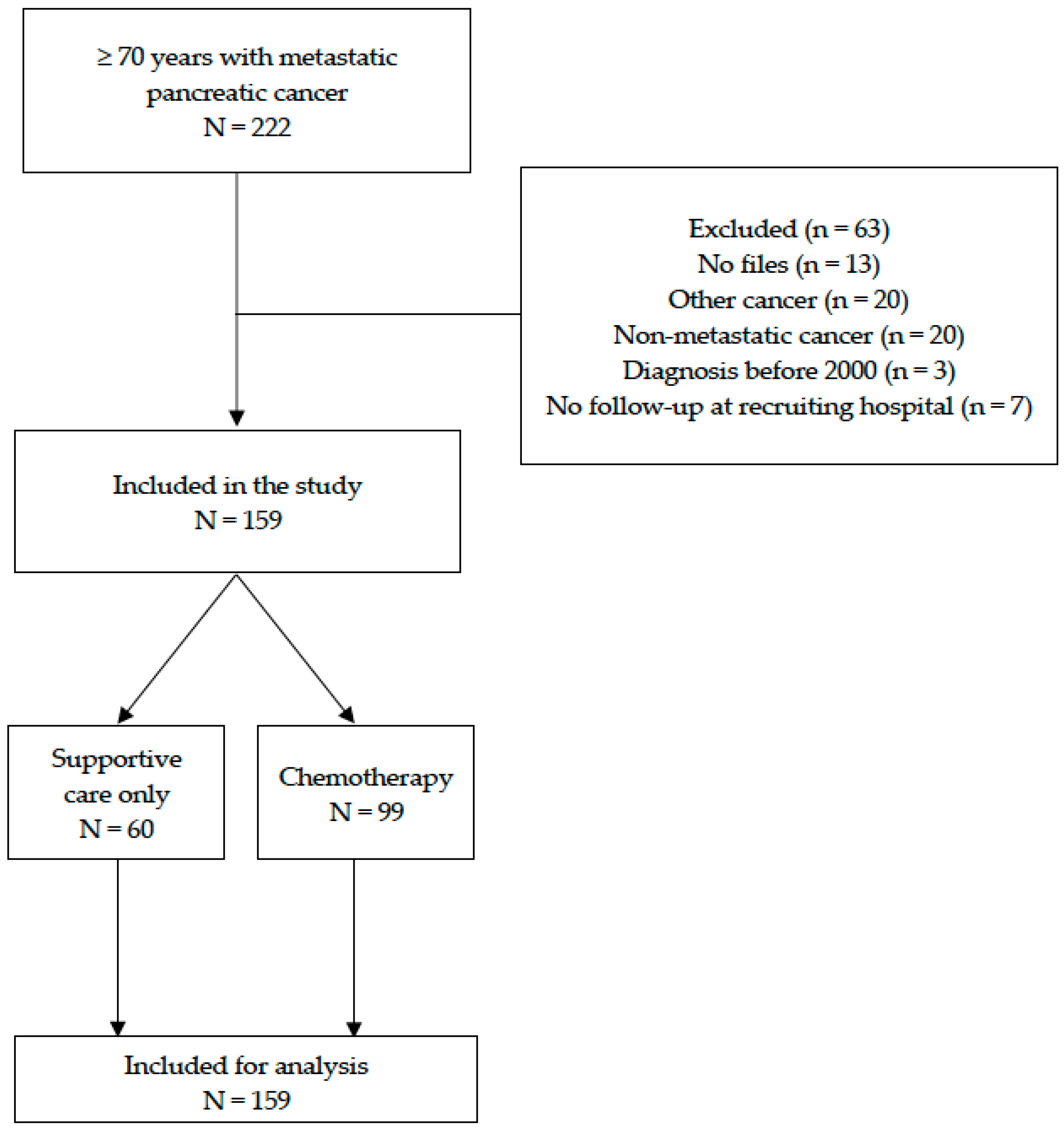
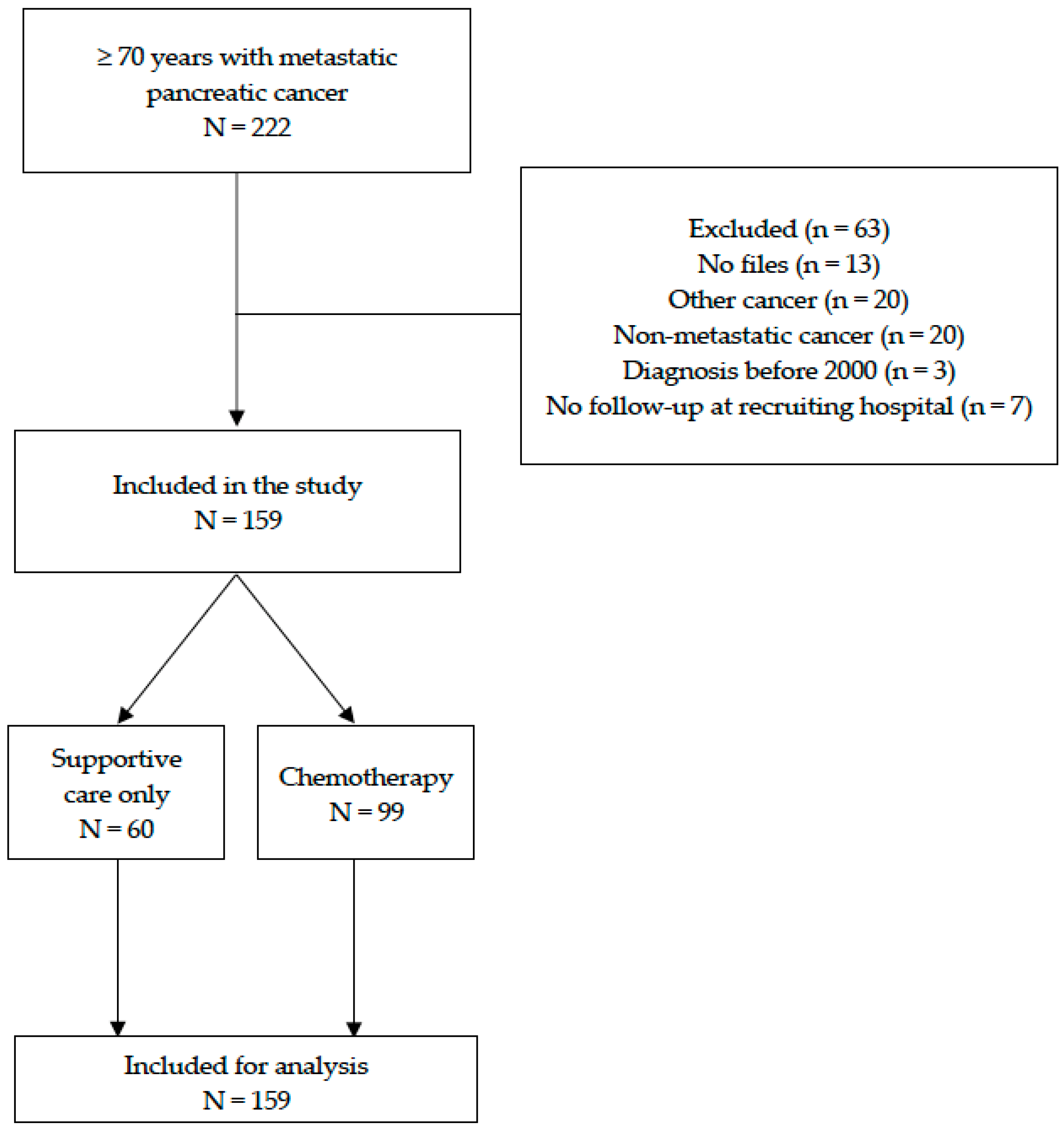
3.1. Patients
3.2. Baseline Characteristics and Comparison between Patients with and without Chemotherapy
3.3. Pre-Therapeutic Factors Associated with Overall Survival among Older Patients with Metastatic Pancreatic Cancer
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, J.; Lok, V.; Ngai, C.H.; Zhang, L.; Yuan, J.; Lao, X.Q.; Ng, K.; Chong, C.; Zheng, Z.-J.; Wong, M.C.S. Worldwide Burden of, Risk Factors for, and Trends in Pancreatic Cancer. Gastroenterology 2021, 160, 744–754. [Google Scholar] [CrossRef] [PubMed]
- Burris, H.A., III; Moore, M.J.; Andersen, J.; Green, M.R.; Rothenberg, M.L.; Modiano, M.R.; Cripps, M.C.; Portenoy, R.K.; Storniolo, A.M.; Tarassoff, P.; et al. Improvements in Survival and Clinical Benefit with Gemcitabine as First-Line Therapy for Patients with Advanced Pancreas Cancer: A Randomized Trial. J. Clin. Oncol. 1997, 15, 2403–2413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouché, O.; Guimbaud, R.; Bécouarn, Y.; Adenis, A.; Raoul, J.-L.; Gourgou-Bourgade, S.; de la Fouchardière, C.; et al. FOLFIRINOX versus Gemcitabine for Metastatic Pancreatic Cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased Survival in Pancreatic Cancer with Nab-Paclitaxel plus Gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corrigan, L.R.; Bracken-Clarke, D.M.; Horgan, A.M. The Challenge of Treating Older Patients with Pancreaticobiliary Malignancies. Curr. Probl. Cancer 2018, 42, 59–72. [Google Scholar] [CrossRef] [PubMed]
- van der Geest, L.G.M.; Haj Mohammad, N.; Besselink, M.G.H.; Lemmens, V.E.P.P.; Portielje, J.E.A.; van Laarhoven, H.W.M.; Wilmink, J.H.W. Nationwide Trends in Chemotherapy Use and Survival of Elderly Patients with Metastatic Pancreatic Cancer. Cancer Med. 2017, 6, 2840–2849. [Google Scholar] [CrossRef]
- Ferrat, E.; Paillaud, E.; Laurent, M.; Le Thuaut, A.; Caillet, P.; Tournigand, C.; Lagrange, J.-L.; Canouï-Poitrine, F.; Bastuji-Garin, S.; ELPACA Study Group. Predictors of 1-Year Mortality in a Prospective Cohort of Elderly Patients with Cancer. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 1148–1155. [Google Scholar] [CrossRef]
- Pamoukdjian, F.; Liuu, E.; Caillet, P.; Herbaud, S.; Gisselbrecht, M.; Poisson, J.; Boudou-Rouquette, P.; Zelek, L.; Paillaud, E. How to Optimize Cancer Treatment in Older Patients: An Overview of Available Geriatric Tools. Am. J. Clin. Oncol. 2019, 42, 109–116. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. PLoS Med. 2007, 4, e296. [Google Scholar] [CrossRef] [Green Version]
- Barta, A. ICD-10-CM Official Coding Guidelines. J. AHIMA 2009, 80, 70–71. [Google Scholar]
- Gnjidic, D.; Hilmer, S.N.; Blyth, F.M.; Naganathan, V.; Waite, L.; Seibel, M.J.; McLachlan, A.J.; Cumming, R.G.; Handelsman, D.J.; Le Couteur, D.G. Polypharmacy Cutoff and Outcomes: Five or More Medicines Were Used to Identify Community-Dwelling Older Men at Risk of Different Adverse Outcomes. J. Clin. Epidemiol. 2012, 65, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Katz, S.; Downs, T.D.; Cash, H.R.; Grotz, R.C. Progress in Development of the Index of ADL. Gerontologist 1970, 10, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Pamoukdjian, F.; Paillaud, E.; Zelek, L.; Laurent, M.; Lévy, V.; Landre, T.; Sebbane, G. Measurement of Gait Speed in Older Adults to Identify Complications Associated with Frailty: A Systematic Review. J. Geriatr. Oncol. 2015, 6, 484–496. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef]
- Raynaud-Simon, A.; Revel-Delhom, C.; Hébuterne, X. Clinical Practice Guidelines from the French Health High Authority: Nutritional Support Strategy in Protein-Energy Malnutrition in the Elderly. Clin. Nutr. 2011, 30, 312–319. [Google Scholar] [CrossRef]
- Ai, Y.; Xu, R.; Liu, L. The Prevalence and Risk Factors of Sarcopenia in Patients with Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Diabetol. Metab. Syndr. 2021, 13, 93. [Google Scholar] [CrossRef]
- Montvida, O.; Shaw, J.; Atherton, J.J.; Stringer, F.; Paul, S.K. Long-Term Trends in Antidiabetes Drug Usage in the U.S.: Real-World Evidence in Patients Newly Diagnosed with Type 2 Diabetes. Diabetes Care 2018, 41, 69–78. [Google Scholar] [CrossRef] [Green Version]
- Schernthaner, G.; Schernthaner, G.-H. The Right Place for Metformin Today. Diabetes Res. Clin. Pract. 2020, 159, 107946. [Google Scholar] [CrossRef] [Green Version]
- Pamoukdjian, F.; Bouillet, T.; Lévy, V.; Soussan, M.; Zelek, L.; Paillaud, E. Prevalence and Predictive Value of Pre-Therapeutic Sarcopenia in Cancer Patients: A Systematic Review. Clin. Nutr. 2018, 37, 1101–1113. [Google Scholar] [CrossRef]
- Broadhurst, P.J.; Hart, A.R. Metformin as an Adjunctive Therapy for Pancreatic Cancer: A Review of the Literature on Its Potential Therapeutic Use. Dig. Dis. Sci. 2018, 63, 2840–2852. [Google Scholar] [CrossRef] [Green Version]
- Coyle, C.; Cafferty, F.H.; Vale, C.; Langley, R.E. Metformin as an Adjuvant Treatment for Cancer: A Systematic Review and Meta-Analysis. Ann. Oncol. 2016, 27, 2184–2195. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.-Q.; Zhou, X.-C.; Du, P.; Yin, M.-Y.; Xu, L.; Chen, W.-J.; Xu, C.-F. Relationships Are between Metformin Use and Survival in Pancreatic Cancer Patients Concurrent with Diabetes: A systematic review and meta-analysis. Medicine 2020, 99, e21687. [Google Scholar] [CrossRef] [PubMed]
- Cetrone, M.; Mele, A.; Tricarico, D. Effects of the Antidiabetic Drugs on the Age-Related Atrophy and Sarcopenia Associated with Diabetes Type II. Curr. Diabetes Rev. 2014, 10, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Pamoukdjian, F.; Aparicio, T.; Zebachi, S.; Zelek, L.; Paillaud, E.; Canoui-Poitrine, F. Comparison of Mobility Indices for Predicting Early Death in Older Patients with Cancer: The Physical Frailty in Elderly Cancer Cohort Study. J. Gerontol. Ser. A 2020, 75, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Soubeyran, P.; Fonck, M.; Blanc-Bisson, C.; Blanc, J.-F.; Ceccaldi, J.; Mertens, C.; Imbert, Y.; Cany, L.; Vogt, L.; Dauba, J.; et al. Predictors of Early Death Risk in Older Patients Treated with First-Line Chemotherapy for Cancer. J. Clin. Oncol. 2012, 30, 1829–1834. [Google Scholar] [CrossRef]
- Qi, Q.; Geng, Y.; Sun, M.; Wang, P.; Chen, Z. Clinical Implications of Systemic Inflammatory Response Markers as Independent Prognostic Factors for Advanced Pancreatic Cancer. Pancreatology 2015, 15, 145–150. [Google Scholar] [CrossRef]
- Wu, L.; Zhu, L.; Xu, K.; Zhou, S.; Zhou, Y.; Zhang, T.; Hang, J.; Zee, B.C.-Y. Clinical Significance of Site-Specific Metastases in Pancreatic Cancer: A Study Based on Both Clinical Trial and Real-World Data. J. Cancer 2021, 12, 1715–1721. [Google Scholar] [CrossRef]
- Pignon, F.; Turpin, A.; Hentic, O.; Coriat, R.; Salmon, E.; Baumgaertner, I.; Bertrand, N.; Lévy, P.; Rebours, V.; Hammel, P.; et al. Efficacy and Tolerance of Gemcitabine and Nab-Paclitaxel in Elderly Patients with Advanced Pancreatic Ductal Adenocarcinoma. Pancreatology 2021, 21, 1064–1070. [Google Scholar] [CrossRef]
- Mizrahi, J.D.; Rogers, J.E.; Hess, K.R.; Wolff, R.A.; Varadhachary, G.R.; Javle, M.M.; Shroff, R.T.; Ho, L.; Fogelman, D.R.; Raghav, K.P.S.; et al. Modified FOLFIRINOX in Pancreatic Cancer Patients Age 75 or Older. Pancreatology 2020, 20, 501–504. [Google Scholar] [CrossRef]
- Berger, A.K.; Haag, G.M.; Ehmann, M.; Byl, A.; Jäger, D.; Springfeld, C. Palliative Chemotherapy for Pancreatic Adenocarcinoma: A Retrospective Cohort Analysis of Efficacy and Toxicity of the FOLFIRINOX Regimen Focusing on the Older Patient. BMC Gastroenterol. 2017, 17, 143. [Google Scholar] [CrossRef] [Green Version]
- Costa, J.G.; de Jesus, V.H.F.; Camandaroba, M.P.G.; Dettino, A.L.A. Characteristics and Survival of Older Patients with Metastatic Pancreatic Cancer: A Retrospective Analysis of the AC Camargo Cancer Center Experience. Ther. Adv. Med. Oncol. 2019, 11, 1758835919874650. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, R.; Okuwaki, K.; Kida, M.; Yamauchi, H.; Kawaguchi, Y.; Matsumoto, T.; Kaneko, T.; Miyata, E.; Uehara, K.; Iwai, T.; et al. A Clinical Trial to Assess the Feasibility and Efficacy of Nab-Paclitaxel plus Gemcitabine for Elderly Patients with Unresectable Advanced Pancreatic Cancer. Int. J. Clin. Oncol. 2019, 24, 1574–1581. [Google Scholar] [CrossRef] [PubMed]
- Paillaud, E.; Soubeyran, P.; Caillet, P.; Cudennec, T.; Brain, E.; Terret, C.; Etchepare, F.; Mourey, L.; Aparicio, T.; Pamoukdjian, F.; et al. Multidisciplinary Development of the Geriatric Core Dataset for Clinical Research in Older Patients with Cancer: A French Initiative with International Survey. Eur. J. Cancer 2018, 103, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Angeli, E.; Chouahnia, K.; Canoui-Poitrine, F.; Duchemann, B.; Aparicio, T.; Paillaud, E.; Zelek, L.; Bousquet, G.; Pamoukdjian, F. Development, Validation and Clinical Impact of a Prediction Model for 6-Month Mortality in Older Cancer Patients: The GRADE. Aging 2020, 12, 4230–4246. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Variables | Whole Cohort | Chemotherapy | Supportive Care | p * |
|---|---|---|---|---|
| n = 159 (%) | n = 99 (%) | n = 60 (%) | ||
| Age (y), median (min-max) | 80.0 (70.0–98.0) | 77.0 (70.0–93.0) | 83.0 (70.0–98.0) | <0.001 |
| Gender (female) | 83 (52) | 55 (56) | 28 (47) | 0.27 |
| Cancer site (n = 158) | ||||
| Head | 76 (48) | 53 (53.5) | 23 (38) | 0.06 |
| Body | 37 (23) | 25 (25) | 12 (20) | 0.44 |
| Tail | 41 (26) | 22 (22) | 19 (32) | 0.18 |
| Unspecified | 4 (2.5) | 1 (1) | 3 (5) | 0.15 |
| Metastases (n = 153) | ||||
| N° of metastasis sites, median (min-max) | 1.0 (1.0–4.0) | 1.0 (1.0–4.0) | 1.0 (1.0–3.0) | 0.9 |
| Lymph nodes | 20 (13) | 12 (12) | 8 (13) | 0.8 |
| Liver | 115 (72) | 66 (67) | 49 (82) | 0.04 |
| Lung | 27 (17) | 21 (21) | 6 (10) | 0.06 |
| Peritoneal carcinomatosis | 43 (27) | 30 (30) | 13 (22) | 0.2 |
| Bone | 9 (6) | 5 (5) | 4 (7) | 0.7 |
| Ascites (yes), n = 145 | 25 (17) | 13 (14) | 12 (22) | 0.22 |
| Endobiliary prosthesis (yes), n = 156 | 40 (26) | 28 (29) | 12 (20) | 0.24 |
| Ca-19.9 (KUI/L), median (min-max), n = 116 | 20.0 (0.0–71.0) | 18.0 (0.0–26.5) | 77.5 (0.0–71.0) | 0.11 |
| Marital status (single), n = 130 | 65 (50) | 34 (42) | 31 (64) | 0.01 |
| Alcohol consumption (yes), n = 123 | 12 (10) | 8 (11) | 4 (8) | 0.55 |
| Active smoker (yes), n = 123 | 37 (30) | 23 (32) | 14 (27) | 0.51 |
| ECOG-PS, median (min-max), n = 141 | 3.0 (1.0–5.0) | 3.0 (1.0–4.0) | 3.0 (1.0–5.0) | <0.0001 |
| Comorbidities (n = 158) | ||||
| Charlson’s index ≥ 1 | 80 (51) | 51 (51.5) | 29 (49) | 0.77 |
| Diabetes | 34 (21.5) | 26 (26) | 8 (14) | 0.06 |
| Heart failure | 53 (33.5) | 30 (30) | 23 (39) | 0.26 |
| Kidney failure | 2 (1) | 0 (0) | 2 (3) | 0.14 |
| Respiratory failure | 2 (1) | 0 (0) | 2 (3) | 0.14 |
| Hepatic failure | 0 (0) | - | - | - |
| Stroke | 8 (5) | 5 (5) | 3 (5) | 1 |
| Poly-medication (≥5 drugs a day), n = 155 | 58 (37) | 39 (40) | 19 (33) | 0.42 |
| ADL-dependency (≤5/6), n = 136 | 24 (18) | 2 (2) | 22 (45) | <0.0001 |
| Walking limitations (yes), n = 130 | 21 (16) | 5 (6) | 16 (33) | <0.0001 |
| Malnutrition | ||||
| Weight loss ≥ 5%, n = 119 | 79 (66) | 48 (61.5) | 31 (76) | 0.12 |
| BMI < 21 kg/m2, n = 105 | 38 (36) | 31 (40) | 7 (26) | 0.19 |
| Albumin < 35 g/L, n = 107 | 71 (66) | 43 (59) | 28 (82) | 0.01 |
| CAR, median (min-max), n = 82 | 1.02 (0.00–33.3) | 0.80 (0.00–33.3) | 2.60 (0.10–17.2) | 0.001 |
| Neutrophil cell count, median (min-max), n = 144 | 6.20 (1.50–33.3) | 5.80 (1.5–29.0) | 7.70 (2.50–33.3) | <0.0001 |
| NLR, median (min-max), n = 144 | 5.40 (0.30–88.0) | 4.40 (0.30–88.0) | 7.60 (1.50–46.5) | <0.0001 |
| Depression (yes), n = 156 | 22 (14) | 15 (15) | 7 (12) | 0.62 |
| Cognitive impairment (yes), n = 155 | 14 (9) | 6 (6) | 8 (14) | 0.09 |
| Haemoglobin < 12 g/dL, n = 145 | 76 (52) | 43 (48) | 33 (60) | 0.15 |
| Total bilirubin (μmol/L), median (min-max), n = 139 | 16.0 (0.00–545) | 14.0 (0.00–545) | 26.5 (5.00–466) | 0.004 |
| Anti-diabetic therapy, n = 34 | 0.37 | |||
| None | 5 (15) | 3 (11.5) | 2 (25) | |
| Insulin alone | 5 (15) | 3 (11.5) | 2 (25) | |
| Oral anti-diabetic drugs alone | 19 (56) | 15 (58) | 4 (50) | |
| Insulin + oral anti-diabetic drugs | 5 (15) | 5 (19) | 0 (0) | |
| Chemotherapy regimens | - | - | ||
| Gemcitabine alone | 49 (49) | |||
| GnP | 23 (23) | |||
| FOLFOX | 2 (2) | |||
| FOLFIRINOX | 12 (12) | |||
| Other ** | 13 (13) |
| Variables | Univariate Analysis | Multivariate Model 1 | Multivariate Model 2 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| HR | [95%CI] | p * | HR | [95%CI] | p * | HR | [95%CI] | p * | |
| Age | 1.04 | [1.01–1.07] | 0.009 | - | - | - | - | - | - |
| Gender (female) | 0.82 | [0.59–1.13] | 0.21 | ||||||
| Cancer site | |||||||||
| Head | 0.55 | [0.40–0.77] | <0.0001 | - | - | - | - | - | - |
| Body | 1.06 | [0.72–1.55] | 0.77 | ||||||
| Tail | 1.55 | [1.07–2.26] | 0.02 | - | - | - | - | - | - |
| Unspecified | 6.39 | [2.30–17.7] | <0.0001 | - | - | - | - | - | - |
| Metastases | |||||||||
| N° of metastasis sites | 1.62 | [1.23–2.14] | 0.001 | 1.37 | [0.90–2.07] | 0.13 | 1.44 | [0.96–2.12] | 0.07 |
| Lymph nodes | 1.05 | [0.63–1.74] | 0.85 | ||||||
| Liver | 1.52 | [1.05–2.18] | 0.02 | 1.71 | [1.06–2.77] | 0.02 | 1.61 | [1.00–2.55] | 0.04 |
| Lung | 0.81 | [0.53–1.23] | 0.32 | ||||||
| Peritoneal carcinomatosis | 1.12 | [0.78–1.61] | 0.54 | ||||||
| Bone | 1.49 | [0.75–2.93] | 0.25 | ||||||
| Other | 1.6 | [0.88–2.89] | 0.12 | 0.4 | [0.13–1.16] | 0.09 | 0.39 | [0.13–1.15] | 0.09 |
| Ascites (yes) | 1.21 | [0.77–1.91] | 0.4 | ||||||
| Endo-biliary prosthesis (yes) | 0.73 | [0.50–1.06] | 0.09 | - | - | - | - | - | - |
| Ca-19.9 (kUI/L) | 1 | [1.00–1.00] | 0.07 | - | - | - | - | - | - |
| Marital status (alone) | 1.29 | [0.90–1.84] | 0.16 | - | - | - | - | - | - |
| Alcohol consumption (yes) | 1.34 | [0.73–2.44] | 0.35 | ||||||
| Active smoker (yes) | 0.95 | [0.63–1.41] | 0.78 | ||||||
| ECOG-PS | 1.91 | [1.53–2.37] | <0.0001 | 1.47 | [1.09–1.99] | 0.01 | 1.45 | [1.08–1.93] | 0.01 |
| Comorbidities | |||||||||
| Charlson’s index | 1.03 | [0.92–1.15] | 0.59 | ||||||
| Diabetes | 0.56 | [0.37–0.85] | 0.006 | 0.43 | [0.24–0.77] | 0.004 | |||
| Heart failure | 1.03 | [0.73–1.45] | 0.86 | ||||||
| Kidney failure | 3.98 | [0.97–16.3] | 0.05 | - | - | - | - | - | - |
| Respiratory failure | 2.19 | [0.54–8.90] | 0.27 | ||||||
| Stroke | 0.82 | [0.38–1.77] | 0.62 | ||||||
| N° of medications | 0.99 | [0.94–1.05] | 0.76 | ||||||
| ADL-scale | 0.65 | [0.56–0.74] | <0.0001 | - | - | - | - | - | - |
| Walking limitations (yes) | 3.57 | [2.08–6.13] | <0.0001 | - | - | - | - | - | - |
| Malnutrition | |||||||||
| Weight loss ≥ 5% | 1.24 | [0.84–1.84] | 0.27 | ||||||
| BMI < 21 kg/m2 | 0.88 | [0.59–1.33] | 0.57 | ||||||
| CAR ≥ 1.02 | 1.48 | [0.94–2.33] | 0.09 | - | - | - | - | - | - |
| Neutrophil (G/L) | 1.1 | [1.06–1.14] | <0.0001 | 1.12 | [1.05–1.20] | 0.001 | 1.12 | [1.04–1.18] | 0.001 |
| NLR, median (min-max) | 1.02 | [1.00–1.03] | 0.02 | 0.98 | [0.96–1.01] | 0.16 | 0.98 | [0.95–1.01] | 0.16 |
| Depression (yes) | 1.19 | [0.74–1.92] | 0.47 | ||||||
| Cognitive impairment (yes) | 1.56 | [0.86–2.84] | 0.14 | - | - | - | |||
| Haemoglobin level (g/dL) | 0.97 | [0.87–1.08] | 0.52 | ||||||
| Total bilirubin (μmol/L) | 1 | [1.00–1.00] | 0.6 | ||||||
| Anti-diabetic therapy (yes) | 0.56 | [0.36–0.87] | 0.01 | 0.43 | [0.23–0.81] | 0.009 | |||
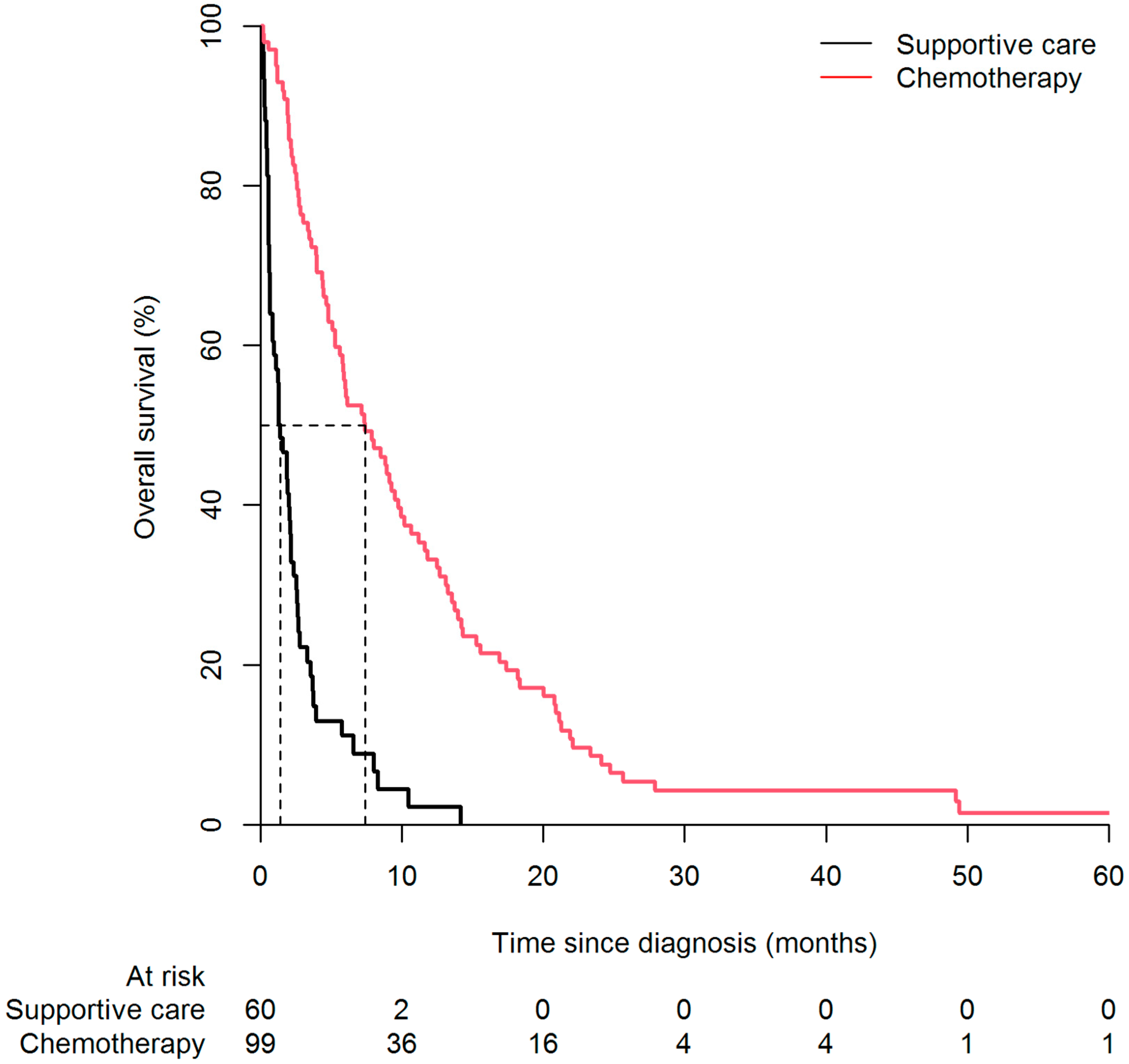
| Chemotherapy (yes) | 0.23 | [0.16–0.33] | <0.0001 | 0.22 | [0.12–0.41] | <0.0001 | 0.23 | [0.12–0.41] | <0.0001 |
| Variables | Univariate Analysis | Multivariate Model 1 | Multivariate Model 2 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| HR | [95%CI] | p * | HR | [95%CI] | p * | HR | [95%CI] | p * | |
| Age | 1.01 | [0.97–1.04] | 0.79 | ||||||
| Gender (female) | 0.86 | [0.57–1.30] | 0.48 | ||||||
| Cancer site | |||||||||
| Head | 0.59 | [0.39–0.89] | 0.01 | - | - | - | - | - | - |
| Body | 1.19 | [0.75–1.91] | 0.45 | ||||||
| Tail | 1.66 | [1.02–2.73] | 0.04 | 1.69 | [0.92–3.11] | 0.09 | 1.67 | [0.91–3.03] | 0.09 |
| Metastases | |||||||||
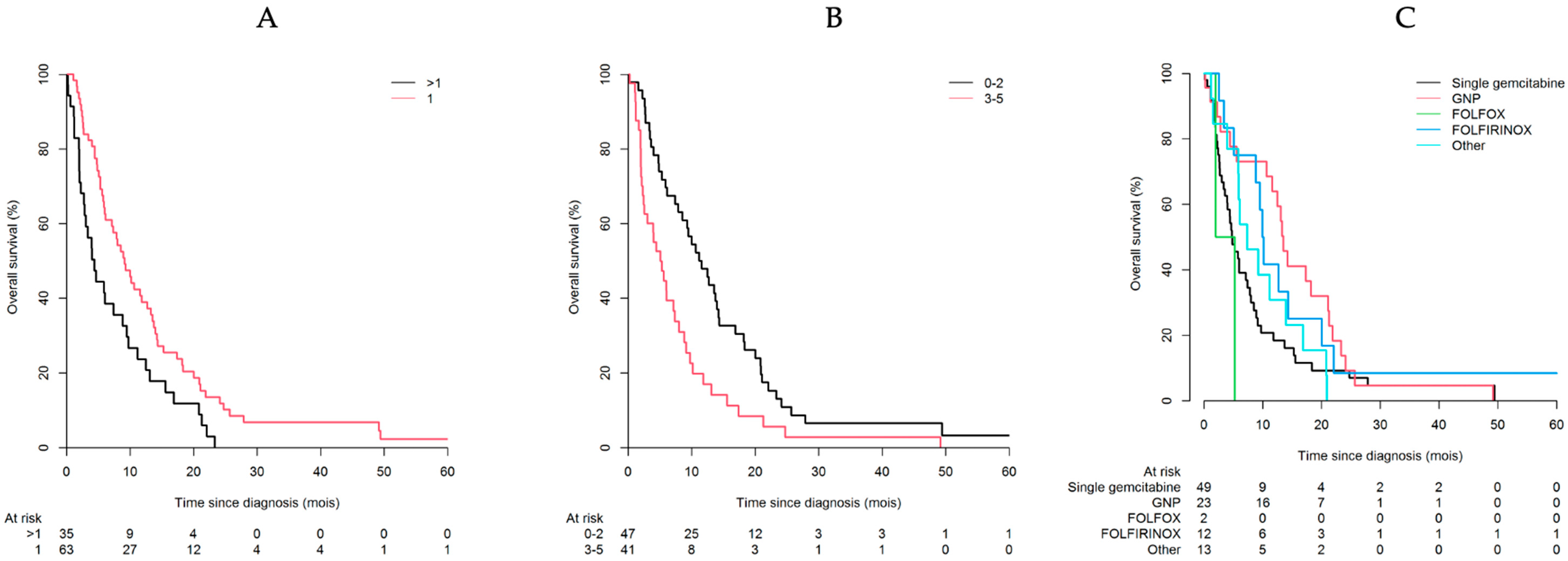
| N° of metastasis sites | 2.04 | [1.43–2.91] | <0.001 | 1.86 | [1.17–2.95] | 0.008 | 1.89 | [1.43–2.34] | 0.007 |
| Lymph nodes | 0.97 | [0.50–1.88] | 0.93 | ||||||
| Liver | 1.21 | [0.78–1.86] | 0.39 | ||||||
| Lung | 0.91 | [0.56–1.49] | 0.72 | ||||||
| Peritoneal carcinomatosis | 1.43 | [0.91–2.24] | 0.11 | - | - | - | - | - | - |
| Bone | 2 | [0.81–4.96] | 0.13 | - | - | - | - | - | - |
| Other | 2.4 | [1.15–5.01] | 0.01 | - | - | - | - | - | - |
| Ascites (yes) | 1.02 | [0.55–1.89] | 0.95 | ||||||
| Endo-biliary prosthesis (yes) | 0.89 | [0.56–1.39] | 0.6 | ||||||
| Ca-19.9 (kUI/L) | 1 | [1.00–1.00] | 0.37 | ||||||
| Marital status (single) | 0.98 | [0.62–1.56] | 0.94 | ||||||
| Alcohol consumption (yes) | 1.75 | [0.82–3.73] | 0.15 | - | - | - | - | - | - |
| Active smoker (yes) | 1.05 | [0.63–1.77] | 0.84 | ||||||
| ECOG-PS | 1.69 | [1.22–2.33] | 0.002 | 1.74 | [1.20–2.53] | 0.003 | 1.75 | [1.38–2.12] | 0.003 |
| Comorbidities | |||||||||
| Charlson’s index | 0.98 | [0.83–1.15] | 0.77 | ||||||
| Diabetes | 0.6 | [0.37–0.99] | 0.04 | 0.57 | [0.29–1.16] | 0.12 | |||
| Heart failure | 0.83 | [0.53–1.30] | 0.41 | ||||||
| Stroke | 0.69 | [0.25–1.89] | 0.47 | ||||||
| N° of medications | 0.98 | [0.92–1.06] | 0.65 | ||||||
| ADL-scale | 0.4 | [0.19–0.83] | 0.01 | - | - | - | - | - | - |
| Walking limitations (yes) | 6.07 | [2.02–18.2] | 0.001 | - | - | - | - | - | - |
| Malnutrition | |||||||||
| Weight loss ≥ 5% | 1.05 | [0.66–1.68] | 0.83 | ||||||
| BMI < 21 kg/m2 | 1 | [0.62–1.59] | 0.98 | ||||||
| CAR ≥ 1.02 | 1.41 | [0.78–2.54] | 0.25 | ||||||
| Neutrophil (G/L) | 1.07 | [1.00–1.15] | 0.05 | 1.06 | [0.99–1.13] | 0.12 | 1.05 | [0.99–1.10] | 0.1 |
| NLR, median (min-max) | 1.02 | [1.00–1.05] | 0.1 | - | - | - | - | - | - |
| Depression (yes) | 1.23 | [0.68–2.22] | 0.5 | ||||||
| Cognitive impairment (yes) | 1.17 | [0.47–2.90] | 0.73 | ||||||
| Haemoglobin level (g/dL) | 1.01 | [0.87–1.17] | 0.89 | ||||||
| Total bilirubin (μmol/L) | 1 | [1.00–1.00] | 0.95 | ||||||
| Anti-diabetic therapy (yes) | 0.49 | [0.23–1.03] | 0.06 | ||||||
| Chemotherapy regimens | |||||||||
| Single gemcitabine | 1.00 (ref) | – | - | 1.00 (ref) | - | - | 1.00 (ref) | - | - |
| GnP | 0.54 | [0.32–0.91] | 0.02 | 0.47 | [0.25–0.89] | 0.02 | 0.45 | [0.25–0.87] | 0.01 |
| FOLFOX | 2.53 | [0.60–10.6] | 0.2 | 3.45 | [0.77–15.4] | 0.1 | 3.41 | [0.77–15.0] | 0.1 |
| FOLFIRINOX | 0.55 | [0.28–1.08] | 0.08 | 0.97 | [0.44–2.15] | 0.94 | 1.01 | [0.46–2.20] | 0.96 |
| Other ** | 0.87 | [0.46–1.62] | 0.65 | 0.86 | [0.39–1.91] | 0.71 | 0.86 | [0.39–1.89] | 0.71 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conti, C.; Pamoukdjian, F.; Aparicio, T.; Mebarki, S.; Poisson, J.; Manceau, G.; Taieb, J.; Rance, B.; Katsahian, S.; Charles-Nelson, A.; et al. Overall Survival and Prognostic Factors among Older Patients with Metastatic Pancreatic Cancer: A Retrospective Analysis Using a Hospital Database. Cancers 2022, 14, 1105. https://doi.org/10.3390/cancers14051105
Conti C, Pamoukdjian F, Aparicio T, Mebarki S, Poisson J, Manceau G, Taieb J, Rance B, Katsahian S, Charles-Nelson A, et al. Overall Survival and Prognostic Factors among Older Patients with Metastatic Pancreatic Cancer: A Retrospective Analysis Using a Hospital Database. Cancers. 2022; 14(5):1105. https://doi.org/10.3390/cancers14051105
Chicago/Turabian StyleConti, Catherine, Frédéric Pamoukdjian, Thomas Aparicio, Soraya Mebarki, Johanne Poisson, Gilles Manceau, Julien Taieb, Bastien Rance, Sandrine Katsahian, Anaïs Charles-Nelson, and et al. 2022. "Overall Survival and Prognostic Factors among Older Patients with Metastatic Pancreatic Cancer: A Retrospective Analysis Using a Hospital Database" Cancers 14, no. 5: 1105. https://doi.org/10.3390/cancers14051105
APA StyleConti, C., Pamoukdjian, F., Aparicio, T., Mebarki, S., Poisson, J., Manceau, G., Taieb, J., Rance, B., Katsahian, S., Charles-Nelson, A., & Paillaud, E. (2022). Overall Survival and Prognostic Factors among Older Patients with Metastatic Pancreatic Cancer: A Retrospective Analysis Using a Hospital Database. Cancers, 14(5), 1105. https://doi.org/10.3390/cancers14051105