
Statins Reduce Hepatocellular Carcinoma Risk in Patients with Chronic Kidney Disease and End-Stage Renal Disease: A 17-Year Longitudinal Study

 , and
, and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Subjects
2.3. Outcome and Comorbidity
2.4. Statistical Analysis
3. Results
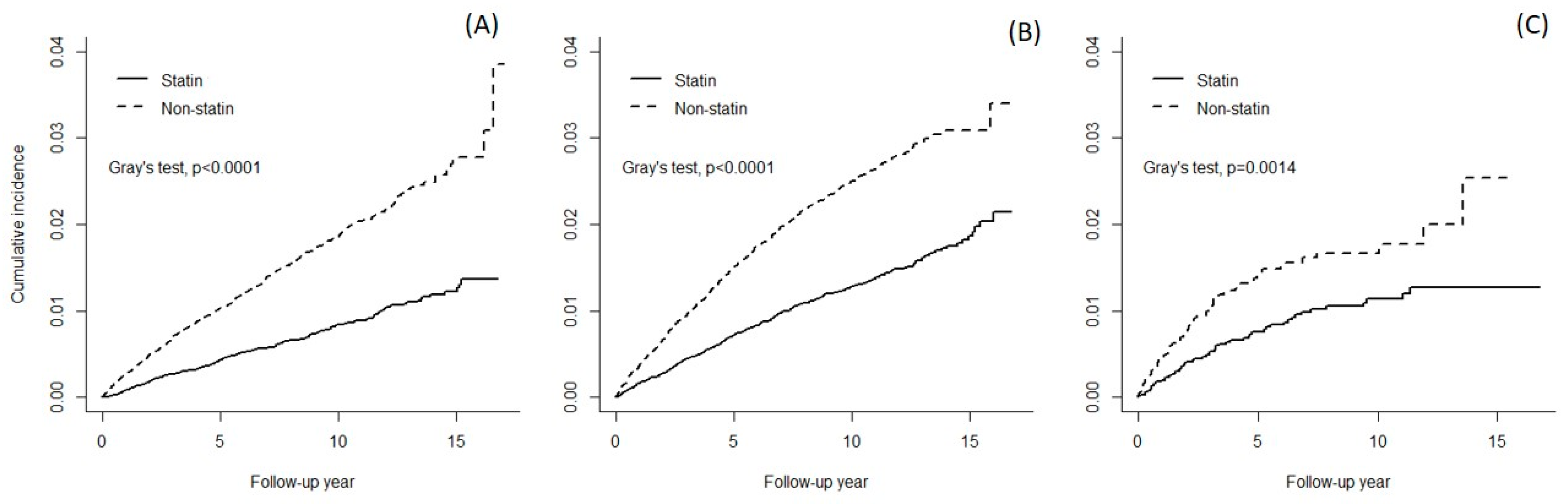
3.1. Cumulative HCC Incidence
3.2. HCC Incidence and Statin Cohort to Non-Statin Cohort HRs of HCC
3.3. Effectiveness in LS and HS Users and in SM and SECT Users
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maisonneuve, P.; Agodoa, L.; Gellert, R.; Stewart, J.H.; Buccianti, G.; Lowenfels, A.B.; Wolfe, R.A.; Jones, E.; Disney, A.P.; Briggs, D.; et al. Cancer in patients on dialysis for end-stage renal disease: An international collaborative study. Lancet 1999, 354, 93–99. [Google Scholar] [CrossRef]
- Lin, H.F.; Li, Y.H.; Wang, C.H.; Chou, C.L.; Kuo, D.J.; Fang, T.C. Increased risk of cancer in chronic dialysis patients: A population-based cohort study in Taiwan. Nephrol. Dial. Transplant. 2012, 27, 1585–1590. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.K.; Han, J.H.; Kim, H.Y.; Kang, G.; Kang, M.; Kim, Y.J.; Min, J. The Incidences and Characteristics of Various Cancers in Patients on Dialysis: A Korean Nationwide Study. J. Korean Med. Sci. 2019, 34, e176. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- U.S.R.D.S. 2020 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States; National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2020.
- Taiwan Society of Nephrology; National Health Research Institute. 2020 Kidney Disease in Taiwan, Annual Report; Hwang, S.J., Ed.; Taiwan Society of Nephrology: Taipei, Taiwan, 2021; p. 464. (In Chinese) [Google Scholar]
- Fabrizi, F.; Cerutti, R.; Alfieri, C.M.; Ridruejo, E. An Update on Hepatocellular Carcinoma in Chronic Kidney Disease. Cancers 2021, 13, 3617. [Google Scholar] [CrossRef] [PubMed]
- Tung, C.F.; Yang, D.Y.; Hu, W.H.; Peng, Y.C.; Chow, W.K.; Chen, G.H. Characteristics of hepatocellular carcinoma in hemodialysis patients in hepatitis B endemic area. Hepatogastroenterology 2003, 50, 1564–1568. [Google Scholar] [PubMed]
- Henderson, W.A.; Shankar, R.; Gill, J.M.; Kim, K.H.; Ghany, M.G.; Skanderson, M.; Butt, A.A. Hepatitis C progressing to hepatocellular carcinoma: The HCV dialysis patient in dilemma. J. Viral. Hepat. 2010, 17, 59–64. [Google Scholar] [CrossRef][Green Version]
- Younossi, Z.M.; Otgonsuren, M.; Henry, L.; Venkatesan, C.; Mishra, A.; Erario, M.; Hunt, S. Association of nonalcoholic fatty liver disease (NAFLD) with hepatocellular carcinoma (HCC) in the United States from 2004 to 2009. Hepatology 2015, 62, 1723–1730. [Google Scholar] [CrossRef]
- Garuti, F.; Neri, A.; Avanzato, F.; Gramenzi, A.; Rampoldi, D.; Rucci, P.; Farinati, F.; Giannini, E.G.; Piscaglia, F.; Rapaccini, G.L.; et al. The changing scenario of hepatocellular carcinoma in Italy: An update. Liver Int. 2021, 41, 585–597. [Google Scholar] [CrossRef] [PubMed]
- Palmer, S.C.; Navaneethan, S.D.; Craig, J.C.; Johnson, D.W.; Perkovic, V.; Hegbrant, J.; Strippoli, G.F. HMG CoA reductase inhibitors (statins) for people with chronic kidney disease not requiring dialysis. Cochrane Database Syst. Rev. 2014, CD007784. [Google Scholar] [CrossRef]
- Kuzyk, C.L.; Anderson, C.C.; Roede, J.R. Simvastatin Induces Delayed Apoptosis Through Disruption of Glycolysis and Mitochondrial Impairment in Neuroblastoma Cells. Clin. Transl. Sci. 2020, 13, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Barbalata, C.I.; Tefas, L.R.; Achim, M.; Tomuta, I.; Porfire, A.S. Statins in risk-reduction and treatment of cancer. World J. Clin. Oncol. 2020, 11, 573–588. [Google Scholar] [CrossRef] [PubMed]
- Sheikholeslami, K.; Ali Sher, A.; Lockman, S.; Kroft, D.; Ganjibakhsh, M.; Nejati-Koshki, K.; Shojaei, S.; Ghavami, S.; Rastegar, M. Simvastatin Induces Apoptosis in Medulloblastoma Brain Tumor Cells via Mevalonate Cascade Prenylation Substrates. Cancers 2019, 11, 994. [Google Scholar] [CrossRef]
- Tilija Pun, N.; Jeong, C.H. Statin as a Potential Chemotherapeutic Agent: Current Updates as a Monotherapy, Combination Therapy, and Treatment for Anti-Cancer Drug Resistance. Pharmaceuticals 2021, 14, 470. [Google Scholar] [CrossRef]
- Collins, R.; Reith, C.; Emberson, J.; Armitage, J.; Baigent, C.; Blackwell, L.; Blumenthal, R.; Danesh, J.; Smith, G.D.; DeMets, D.; et al. Interpretation of the evidence for the efficacy and safety of statin therapy. Lancet 2016, 388, 2532–2561. [Google Scholar] [CrossRef]
- Göbel, A.; Zinna, V.M.; Dell’Endice, S.; Jaschke, N.; Kuhlmann, J.D.; Wimberger, P.; Rachner, T.D. Anti-tumor effects of mevalonate pathway inhibition in ovarian cancer. BMC Cancer 2020, 20, 703. [Google Scholar] [CrossRef]
- Allott, E.H.; Ebot, E.M.; Stopsack, K.H.; Gonzalez-Feliciano, A.G.; Markt, S.C.; Wilson, K.M.; Ahearn, T.U.; Gerke, T.A.; Downer, M.K.; Rider, J.R.; et al. Statin Use Is Associated with Lower Risk of PTEN-Null and Lethal Prostate Cancer. Clin. Cancer Res. 2020, 26, 1086–1093. [Google Scholar] [CrossRef]
- Islam, M.M.; Poly, T.N.; Walther, B.A.; Yang, H.C.; Jack Li, Y.C. Statin Use and the Risk of Hepatocellular Carcinoma: A Meta-Analysis of Observational Studies. Cancers 2020, 12, 671. [Google Scholar] [CrossRef]
- Chang, Y.; Liu, Q.; Zhou, Z.; Ding, Y.; Yang, M.; Xu, W.; Chen, K.; Zhang, Q.; Wang, Z.; Li, H. Can Statin Treatment Reduce the Risk of Hepatocellular Carcinoma? A Systematic Review and Meta-Analysis. Technol Cancer Res. Treat. 2020, 19, 1533033820934881. [Google Scholar] [CrossRef]
- Facciorusso, A.; Abd El Aziz, M.A.; Singh, S.; Pusceddu, S.; Milione, M.; Giacomelli, L.; Sacco, R. Statin Use Decreases the Incidence of Hepatocellular Carcinoma: An Updated Meta-Analysis. Cancers 2020, 12, 874. [Google Scholar] [CrossRef] [PubMed]
- Pinyopornpanish, K.; Al-Yaman, W.; Butler, R.S.; Carey, W.; McCullough, A.; Romero-Marrero, C. Chemopreventive Effect of Statin on Hepatocellular Carcinoma in Patients With Nonalcoholic Steatohepatitis Cirrhosis. Am. J. Gastroenterol. 2021, 116, 2258–2269. [Google Scholar] [CrossRef] [PubMed]
- Vinogradova, Y.; Coupland, C.; Hippisley-Cox, J. Exposure to statins and risk of common cancers: A series of nested case-control studies. BMC Cancer 2011, 11, 409. [Google Scholar] [CrossRef] [PubMed]
- Chang, F.M.; Wang, Y.P.; Lang, H.C.; Tsai, C.F.; Hou, M.C.; Lee, F.Y.; Lu, C.L. Statins decrease the risk of decompensation in hepatitis B virus- and hepatitis C virus-related cirrhosis: A population-based study. Hepatology 2017, 66, 896–907. [Google Scholar] [CrossRef] [PubMed]
- Longo, J.; van Leeuwen, J.E.; Elbaz, M.; Branchard, E.; Penn, L.Z. Statins as Anticancer Agents in the Era of Precision Medicine. Clin. Cancer Res. 2020, 26, 5791–5800. [Google Scholar] [CrossRef]
- Simon, T.G.; Chan, A.T. Lifestyle and Environmental Approaches for the Primary Prevention of Hepatocellular Carcinoma. Clin. Liver Dis. 2020, 24, 549–576. [Google Scholar] [CrossRef]
- Simon, T.G.; Duberg, A.S.; Aleman, S.; Chung, R.T.; Chan, A.T.; Ludvigsson, J.F. Association of Aspirin with Hepatocellular Carcinoma and Liver-Related Mortality. N. Engl. J. Med. 2020, 382, 1018–1028. [Google Scholar] [CrossRef]
- Ielasi, L.; Tovoli, F.; Tonnini, M.; Tortora, R.; Magini, G.; Sacco, R.; Pressiani, T.; Trevisani, F.; Sansone, V.; Marasco, G.; et al. Beneficial Prognostic Effects of Aspirin in Patients Receiving Sorafenib for Hepatocellular Carcinoma: A Tale of Multiple Confounders. Cancers 2021, 13, 6376. [Google Scholar] [CrossRef]
- Khajeh, E.; Moghadam, A.D.; Eslami, P.; Ali-Hasan-Al-Saegh, S.; Ramouz, A.; Shafiei, S.; Ghamarnejad, O.; Dezfouli, S.A.; Rupp, C.; Springfeld, C.; et al. Statin use is associated with the reduction in hepatocellular carcinoma recurrence after liver surgery. BMC Cancer 2022, 22, 91. [Google Scholar] [CrossRef]
- Simon, T.G.; Duberg, A.S.; Aleman, S.; Hagstrom, H.; Nguyen, L.H.; Khalili, H.; Chung, R.T.; Ludvigsson, J.F. Lipophilic Statins and Risk for Hepatocellular Carcinoma and Death in Patients With Chronic Viral Hepatitis: Results From a Nationwide Swedish Population. Ann. Intern. Med. 2019, 171, 318–327. [Google Scholar] [CrossRef] [PubMed]
- Birmingham, B.K.; Bujac, S.R.; Elsby, R.; Azumaya, C.T.; Zalikowski, J.; Chen, Y.; Kim, K.; Ambrose, H.J. Rosuvastatin pharmacokinetics and pharmacogenetics in Caucasian and Asian subjects residing in the United States. Eur. J. Clin. Pharmacol. 2015, 71, 329–340. [Google Scholar] [CrossRef]
- Wu, H.F.; Hristeva, N.; Chang, J.; Liang, X.; Li, R.; Frassetto, L.; Benet, L.Z. Rosuvastatin Pharmacokinetics in Asian and White Subjects Wild Type for Both OATP1B1 and BCRP Under Control and Inhibited Conditions. J. Pharm. Sci. 2017, 106, 2751–2757. [Google Scholar] [CrossRef] [PubMed]
- Collaboration, C.T.T. Efficacy and safety of statin therapy in older people: A meta-analysis of individual participant data from 28 randomised controlled trials. Lancet 2019, 393, 407–415. [Google Scholar]
- Marshall, B.; Bennett, N. PURL: How old is too old for statins? J. Fam. Pract. 2020, 69, 257–259. [Google Scholar] [PubMed]
- Savarese, G.; De Ferrari, G.M.; Rosano, G.M.; Perrone-Filardi, P. Safety and efficacy of ezetimibe: A meta-analysis. Int. J. Cardiol. 2015, 201, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Battaggia, A.; Donzelli, A.; Font, M.; Molteni, D.; Galvano, A. Clinical efficacy and safety of Ezetimibe on major cardiovascular endpoints: Systematic review and meta-analysis of randomized controlled trials. PLoS ONE 2015, 10, e0124587. [Google Scholar] [CrossRef] [PubMed]
- Miura, K.; Ohnishi, H.; Morimoto, N.; Minami, S.; Ishioka, M.; Watanabe, S.; Tsukui, M.; Takaoka, Y.; Nomoto, H.; Isoda, N.; et al. Ezetimibe suppresses development of liver tumors by inhibiting angiogenesis in mice fed a high-fat diet. Cancer Sci. 2019, 110, 771–783. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Normal Renal Function | CKD without Dialysis | ESRD | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Non-Statin N = 413,867 | Statin N = 413,867 | Standardized Difference | Non-Statin N = 46,851 | Statin N = 46,851 | Standardized Difference | Non-Statin N = 6372 | Statin N = 6372 | Standardized Difference | |||||||
| Age, mean (SD) | 58.8 | (10.6) | 58.9 | (9.84) | 0.009 | 64.9 | (10.7) | 64.9 | (9.93) | 0.001 | 63.5 | (10.3) | 63.1 | (9.64) | 0.037 |
| Men, n (%) | 207,043 | 50.0 | 504,001 | 49.3 | 0.015 | 26,664 | 56.9 | 26,289 | 56.1 | 0.016 | 3244 | 50.9 | 3161 | 49.6 | 0.026 |
| Income, NTD | |||||||||||||||
| <19,200 | 88,484 | 21.4 | 88,978 | 21.5 | 0.003 | 11,699 | 25.0 | 11,677 | 24.9 | 0.001 | 1730 | 27.2 | 1737 | 27.3 | 0.002 |
| 19,200–21,900 | 128,311 | 31.0 | 128,689 | 31.1 | 0.002 | 14,859 | 31.7 | 15,031 | 32.1 | 0.008 | 2244 | 35.2 | 2253 | 35.4 | 0.003 |
| 21,901–36,300 | 78,194 | 18.9 | 77,457 | 18.7 | 0.005 | 9242 | 19.7 | 9099 | 19.4 | 0.008 | 1125 | 17.7 | 1109 | 17.4 | 0.007 |
| >36,300 | 118,878 | 28.8 | 118,743 | 28.7 | 0.005 | 11,051 | 23.6 | 11,044 | 23.6 | 0.008 | 1273 | 20.0 | 1273 | 20.0 | 0.007 |
| Living area | |||||||||||||||
| North | 191,518 | 46.3 | 192,042 | 46.4 | 0.003 | 18,104 | 38.6 | 17,885 | 38.2 | 0.010 | 2473 | 38.8 | 2502 | 39.3 | 0.009 |
| Central | 79,214 | 19.1 | 78,772 | 19.0 | 0.003 | 9811 | 20.9 | 9905 | 21.1 | 0.005 | 1320 | 20.7 | 1317 | 20.7 | 0.001 |
| South | 119,741 | 28.9 | 119,169 | 28.8 | 0.003 | 16,312 | 34.8 | 16,369 | 34.9 | 0.003 | 2216 | 34.8 | 2204 | 34.6 | 0.004 |
| East and Offshore Islands | 23,394 | 5.65 | 23,884 | 5.77 | 0.003 | 2624 | 5.60 | 2692 | 5.75 | 0.003 | 363 | 5.70 | 349 | 5.48 | 0.004 |
| Comorbidity, n (%) | |||||||||||||||
| DM | 135,188 | 32.7 | 145,069 | 35.1 | 0.050 | 20,619 | 44.0 | 21,435 | 45.8 | 0.035 | 3597 | 56.5 | 3609 | 56.6 | 0.004 |
| Hypertension | 233,360 | 56.4 | 231,858 | 56.0 | 0.007 | 35,756 | 76.3 | 36,001 | 76.8 | 0.012 | 4689 | 73.6 | 4664 | 73.2 | 0.009 |
| NAFLD | 7821 | 1.89 | 7859 | 1.90 | 0.001 | 806 | 1.72 | 829 | 1.77 | 0.004 | 26 | 0.41 | 33 | 0.52 | 0.016 |
| ALD | 2520 | 0.61 | 2387 | 0.58 | 0.004 | 289 | 0.62 | 288 | 0.61 | 0.000 | 10 | 0.16 | 10 | 0.16 | 0.000 |
| HBV | 12,265 | 2.96 | 12,146 | 2.93 | 0.002 | 1283 | 2.74 | 1263 | 2.70 | 0.003 | 266 | 3.55 | 202 | 3.17 | 0.021 |
| HCV | 4735 | 1.14 | 4512 | 1.09 | 0.005 | 862 | 1.84 | 803 | 1.71 | 0.010 | 260 | 4.08 | 237 | 3.72 | 0.019 |
| Cirrhosis | 3214 | 0.78 | 2810 | 0.68 | 0.011 | 726 | 1.55 | 624 | 1.33 | 0.018 | 140 | 2.20 | 127 | 1.99 | 0.014 |
| Metformin use | 86,387 | 20.9 | 98,503 | 23.8 | 0.070 | 11,944 | 25.5 | 12,974 | 27.7 | 0.050 | 212 | 3.33 | 2008 | 3.26 | 0.004 |
| Hemodialysis | 5843 | 91.7 | 5788 | 90.8 | 0.031 | ||||||||||
| Non-Statin | Statin | Statin to. Non-Statin Hazard Ratio (95% Confidence Interval) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Outcome | Event n | PYs | Rate, per 10,000 PYs | Event n | PYs | Rate, per 10,000 PYs | Model 1 | Model 2 | Model 3 |
| NRF | 5134 | 2,394,676 | 21.4 | 2180 | 2,807,446 | 7.77 | 0.36 (0.35–0.38) *** | 0.29 (0.22–0.39) *** | 0.46 (0.39–0.53) *** |
| 40–54 years | 1164 | 1,047,495 | 11.1 | 555 | 1,094,486 | 5.07 | 0.45 (0.41–0.50) *** | 0.33 (0.19–0.59) *** | 0.39 (0.29–0.54) *** |
| 55–64 | 1624 | 711,419 | 22.8 | 704 | 927,857 | 7.59 | 0.33 (0.30–0.36) *** | 0.28 (0.17–0.45) *** | 0.52 (0.40–0.67) *** |
| 65–80 | 2346 | 635,763 | 36.9 | 921 | 785,103 | 11.7 | 0.32 (0.30–0.35) *** | 0.28 (0.18–0.42) *** | 0.43 (0.34–0.54) *** |
| CKD | 720 | 194,009 | 37.1 | 425 | 269,655 | 15.8 | 0.42 (0.38–0.48) *** | 0.50 (0.42–0.60) *** | 0.55 (0.49–0.62) *** |
| 40–54 | 65 | 46,151 | 14.1 | 47 | 53,622 | 8.77 | 0.58 (0.40–0.85) ** | 0.85 (0.52–1.37) | 0.61 (0.42–0.90) * |
| 55–64 | 162 | 50,157 | 32.3 | 98 | 76,094 | 12.9 | 0.39 (0.30–0.50) *** | 0.55 (0.39–0.77) *** | 0.46 (0.36–0.60) *** |
| 65–80 | 493 | 97,701 | 50.5 | 280 | 139,938 | 20.0 | 0.40 (0.34–0.46) *** | 0.43 (0.34–0.54) *** | 0.56 (0.49–0.65) *** |
| ESRD | 83 | 17,356 | 47.8 | 54 | 28,240 | 19.1 | 0.41 (0.29–0.59) *** | 0.46 (0.27–0.77) ** | 0.63 (0.45–0.88) ** |
| 40–54 | 14 | 4855 | 28.8 | 12 | 7695 | 15.6 | 0.58 (0.27–1.27) | 0.64 (0.22–1.89) | 0.85 (0.39–1.85) |
| 55–64 | 24 | 5122 | 46.9 | 20 | 9391 | 21.3 | 0.45 (0.25–0.81) ** | 0.43 (0.18–1.03) | 0.65 (0.36–1.15) |
| 65–80 | 45 | 7379 | 61.0 | 22 | 11,154 | 19.7 | 0.33 (0.19–0.56) *** | 0.39 (0.18–0.86) * | 0.54 (0.32–0.91) * |
| Medication Type | N | Event n | Rate, per 10,000 PYs | aHR (95% CI) † | p | aHR (95% CI) †† | p |
|---|---|---|---|---|---|---|---|
| NRF | |||||||
| Non-statin | 413,867 | 5134 | 21.4 | Ref. | |||
| LS | 277,943 | 1617 | 8.60 | 0.40 (0.38–0.43) | <0.0001 | Ref. | |
| HS | 135,924 | 563 | 6.07 | 0.28 (0.26–0.31) | <0.0001 | 0.71 (0.64–0.78) | <0.0001 |
| CKD | |||||||
| Non-statin | 46,851 | 720 | 37.1 | Ref. | |||
| LS | 32,526 | 313 | 16.7 | 0.45 (0.39–0.52) | <0.0001 | Ref. | |
| HS | 14,325 | 112 | 13.5 | 0.36 (0.30–0.44) | <0.0001 | 0.81 (0.65–1.00) | 0.053 |
| ESRD | |||||||
| Non-statin | 6372 | 83 | 47.8 | Ref. | |||
| LS | 4851 | 42 | 19.6 | 0.42 (0.29–0.62) | <0.0001 | Ref. | |
| HS | 1521 | 12 | 17.7 | 0.38 (0.21–0.70) | 0.002 | 0.91 (0.48–1.72) | 0.760 |
| NRF | |||||||
| Non-statin | 413,867 | 5134 | 21.4 | Ref. | |||
| SM | 377,351 | 2006 | 7.88 | 0.37 (0.35–0.39) | <0.0001 | Ref. | |
| SECT | 36,516 | 174 | 6.66 | 0.31 (0.27–0.36) | <0.0001 | 0.85 (0.73–0.99) | 0.034 |
| CKD | |||||||
| Non-statin | 46,851 | 720 | 37.1 | Ref. | |||
| SM | 42,182 | 388 | 16.1 | 0.43 (0.38–0.49) | <0.0001 | Ref. | |
| SECT | 4669 | 37 | 13.2 | 0.35 (0.25–0.49) | <0.0001 | 0.82 (0.59–1.15) | 0.246 |
| ESRD | |||||||
| Non-statin | 6372 | 83 | 47.8 | Ref. | |||
| SM | 5910 | 51 | 19.5 | 0.42 (0.29–0.60) | <0.0001 | Ref. | |
| SECT | 462 | 3 | 14.4 | 0.31 (0.10–0.99) | 0.049 | 0.75 (0.23–2.39) | 0.745 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sung, F.-C.; Yeh, Y.-T.; Muo, C.-H.; Hsu, C.-C.; Tsai, W.-C.; Hsu, Y.-H. Statins Reduce Hepatocellular Carcinoma Risk in Patients with Chronic Kidney Disease and End-Stage Renal Disease: A 17-Year Longitudinal Study. Cancers 2022, 14, 825. https://doi.org/10.3390/cancers14030825
Sung F-C, Yeh Y-T, Muo C-H, Hsu C-C, Tsai W-C, Hsu Y-H. Statins Reduce Hepatocellular Carcinoma Risk in Patients with Chronic Kidney Disease and End-Stage Renal Disease: A 17-Year Longitudinal Study. Cancers. 2022; 14(3):825. https://doi.org/10.3390/cancers14030825
Chicago/Turabian StyleSung, Fung-Chang, Yi-Ting Yeh, Chih-Hsin Muo, Chih-Cheng Hsu, Wen-Chen Tsai, and Yueh-Han Hsu. 2022. "Statins Reduce Hepatocellular Carcinoma Risk in Patients with Chronic Kidney Disease and End-Stage Renal Disease: A 17-Year Longitudinal Study" Cancers 14, no. 3: 825. https://doi.org/10.3390/cancers14030825
APA StyleSung, F.-C., Yeh, Y.-T., Muo, C.-H., Hsu, C.-C., Tsai, W.-C., & Hsu, Y.-H. (2022). Statins Reduce Hepatocellular Carcinoma Risk in Patients with Chronic Kidney Disease and End-Stage Renal Disease: A 17-Year Longitudinal Study. Cancers, 14(3), 825. https://doi.org/10.3390/cancers14030825