
Long-Term Outcome in a Phase II Study of Regional Hyperthermia Added to Preoperative Radiochemotherapy in Locally Advanced and Recurrent Rectal Adenocarcinomas

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. The Inclusion Criteria
2.2. Statistics and Ethics
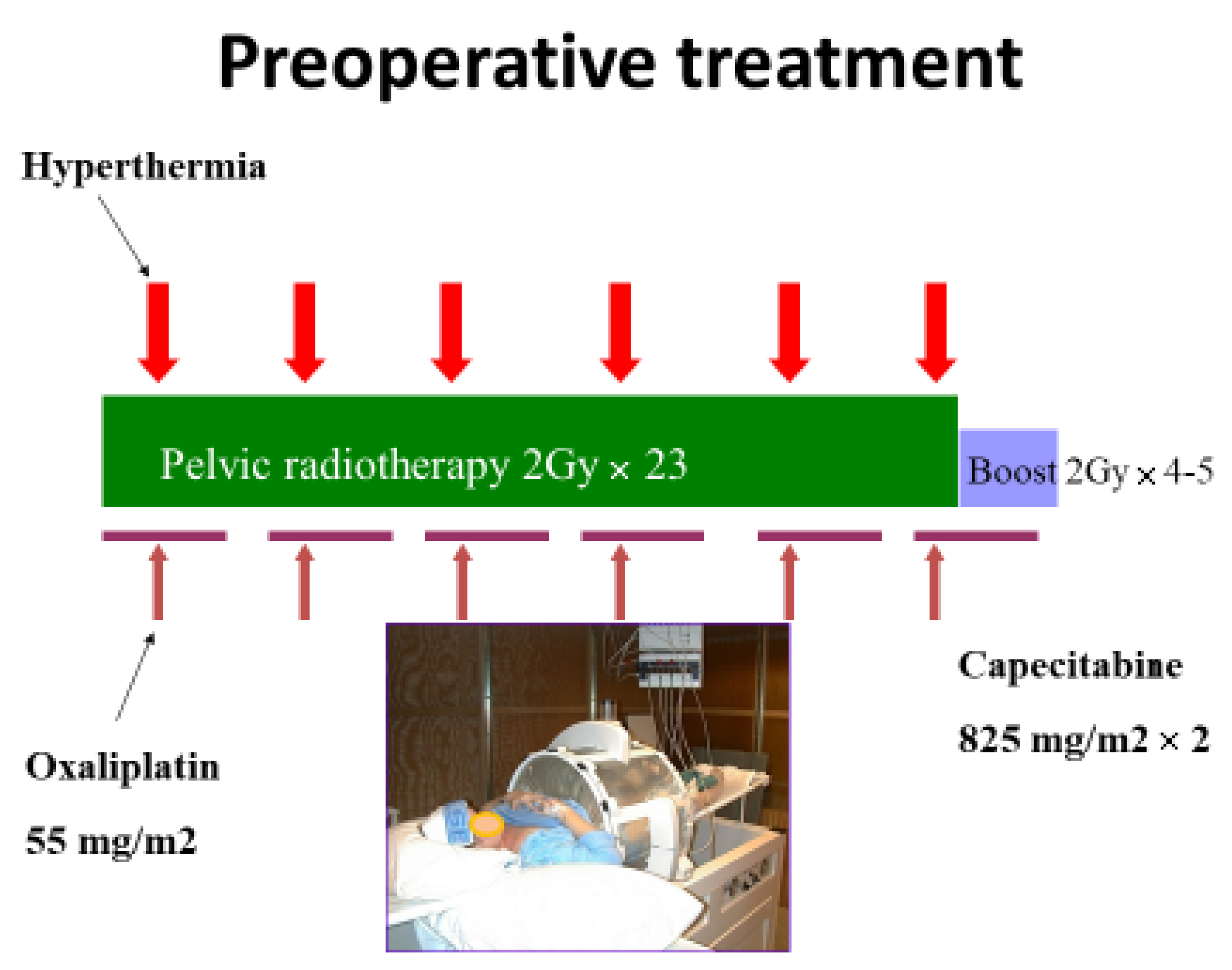
3. Treatment
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Braendengen, M.; Tveit, K.M.; Berglund, Å.; Birkemeyer, E.; Frykholm, G.; Påhlman, L.; Wiig, J.N.; Byström, P.; Bujko, K.; Glimelius, B. Randomized phase III study comparing preoperative radiotherapy with chemoradiotherapy in nonresectable rectal cancer. J. Clin. Oncol. 2008, 26, 3687–3694. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Yamaguchi, T.; Hachiya, K.; Okada, S.; Kitahara, M.; Matsuyama, K.; Matsuo, M. Radiotherapy for locally recurrent rectal cancer treated with surgery alone as the initial treatment. Radiat. Oncol. J. 2017, 35, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Temple, W.J.; Saettler, E.B. Locally recurrent rectal cancer: Role of composite resection of extensive pelvic tumors with strategies for minimizing risk of recurrence. J. Surg. Oncol. 2000, 73, 47–58. [Google Scholar] [CrossRef]
- Dahl, O.; Horn, A.; Morild, I.; Halvorsen, J.F.; Odland, G.; Reinertsen, S.; Reisæter, A.; Kavli, H.; Thunold, J. Low-dose preoperative radiation postpones recurrences in operable rectal cancer. Results of a randomized multicenter trial in western Norway. Cancer 1990, 66, 2286–2294. [Google Scholar] [CrossRef]
- Colorectal Cancer Collaborative Group. Adjuvant radiotherapy for rectal cancer: A systematic overview of 8507 patients from 22 randomized trials. Lancet 2001, 358, 1291–1304. [Google Scholar] [CrossRef]
- Krook, J.E.; Moertel, C.G.; Gunderson, L.L.; Wieand, H.S.; Collins, R.T.; Beart, R.W.; Kubista, T.P.; Poon, M.A.; Meyers, W.C.; Mailliard, J.A.; et al. Effective surgical adjuvant therapy for high-risk rectal carcinoma. N. Engl. J. Med. 1991, 324, 709–715. [Google Scholar] [CrossRef]
- Bjerkeset, T.; Dahl, O. Irradiation and surgery of primarily inoperable rectal adenocarcinoma. Dis. Colon Rectum 1980, 23, 298–303. [Google Scholar] [CrossRef]
- Mella, O.; Dahl, O.; Horn, A.; Morild, I.; Odland, G. Radiotherapy and resection for apparently inoperable rectal adenocarcinoma. Dis. Colon. Rectum 1984, 27, 663–668. [Google Scholar] [CrossRef]
- Reerink, O.; Verschueren, R.; Szabo, B.; Hospers, G.; Mulder, N. A favourable pathological stage after neoadjuvant radiochemotherapy in patients with initially irresectable rectal cancer correlates with a favourable prognosis. Eur. J. Cancer 2003, 39, 192–195. [Google Scholar] [CrossRef]
- Dahl, O.; Dalene, R.; Schem, B.C.; Mella, O. Status of clinical hyperthermia. Acta Oncol. 1999, 38, 863–873. [Google Scholar] [CrossRef]
- Harima, Y.; Nagata, K.; Harima, K.; Ostapenko, V.V.; Tanaka, Y.; Sawada, S. A randomized clinical trial of radiation therapy versus thermoradiotherapy in stage IIIB cervical carcinoma. Int. J. Hyperth. 2001, 17, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Overgaard, J.; Gonzalez Gonzalez, D.; Hulshof, M.C.; Arcangeli, G.; Dahl, O.; Mella, O.; Bentzen, S.M. Randomised trial of hyperthermia as adjuvant to radiotherapy for recurrent or metastatic malignant melanoma. European Society for Hyperthermic Oncology. Lancet 1995, 345, 540–543. [Google Scholar] [CrossRef]
- Van der Zee, J.; González, D.; van Rhoon, G.C.; van Dijk, J.D.; van Putten, W.L.; Hart, A.A. Comparison of radiotherapy alone with radiotherapy plus hyperthermia in locally advanced pelvic tumours: A prospective, randomised, multicentre trial. Dutch Deep Hyperthermia Group. Lancet 2000, 355, 1119–1125. [Google Scholar] [CrossRef]
- Schem, B.C.; Mella, O.; Dahl, O. Thermochemotherapy with cisplatin or carboplatin in the BT4 rat glioma in vitro and in vivo. Int. J. Radiat. Oncol. Biol. Phys. 1992, 23, 109–114. [Google Scholar] [CrossRef]
- Korenaga, D.; Matsushima, T.; Adachi, Y.; Mori, M.; Matsuda, H.; Kuwano, H.; Sugimachi, K. Preoperative hyperthermia combined with chemotherapy and radiotherapy for patients with rectal carcinoma may prevent early local pelvic recurrence. Int. J. Colorectal Dis. 1992, 7, 206–209. [Google Scholar] [CrossRef]
- Rau, B.; Wust, P.; Hohenberger, P.; Löffel, J.; Hünerbein, M.; Below, C.; Gellermann, J.; Speidel, A.; Vogl, T.; Riess, H.; et al. Preoperative hyperthermia combined with radiochemotherapy in locally advanced rectal cancer: A phase II clinical trial. Ann. Surg. 1998, 227, 380–389. [Google Scholar] [CrossRef]
- Wust, P.; Hildebrandt, B.; Sreenivasa, G.; Rau, B.; Gellermann, J.; Riess, H.; Felix, R.; Schlag, P.M. Hyperthermia in combined treatment of cancer. Lancet Oncol. 2002, 3, 487–497. [Google Scholar] [CrossRef]
- Dunst, J.; Reese, T.; Sutter, T.; Zühlke, H.; Hinke, A.; Kölling-Schlebusch, K.; Frings, S. Phase I trial evaluating the concurrent combination of radiotherapy and capecitabine in rectal cancer. J. Clin. Oncol. 2002, 20, 3983–3991. [Google Scholar] [CrossRef]
- Hildebrandt, B.; Wust, P.; Dräger, J.; Lüdemann, L.; Sreenivasa, G.; Tullius, S.G.; Amthauer, H.; Neuhaus, P.; Felix, R.; Riess, H. Regional pelvic hyperthermia as an adjunct to chemotherapy (oxaliplatin, folinic acid, 5-fluorouracil) in pre-irradiated patients with locally recurrent rectal cancer: A pilot study. Int. J. Hyperth. 2004, 20, 359–369. [Google Scholar] [CrossRef]
- Rietbroek, R.C.; van de Vaart, P.J.M.; Haveman, J.; Blommaert, F.A.; Geerdink, A.; Bakker, P.J.M.; Veenhof, C.H.N. Hyperthermia enhances the cytotoxicity and platinum-DNA adduct formation of lobaplatin and oxaliplatin in cultured SW 1573 cells. J. Cancer Res. Clin. Oncol. 1997, 123, 6–12. [Google Scholar] [CrossRef] [Green Version]
- Urano, M.; Ling, C.C. Thermal enhancement of melphalan and oxaliplatin cytotoxicity in vitro. Int. J. Hyperth. 2002, 18, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Hegewisch-Becker, S.; Gruber, Y.; Corovic, A.; Pichlmeier, U.; Atanackovic, D.; Nierhaus, A.; Hossfeld, D.K. Whole-body hyperthermia (41.8 degrees C) combined with bimonthly oxaliplatin, high-dose leucovorin and 5-fluorouracil 48-hour continuous infusion in pretreated metastatic colorectal cancer: A phase II study. Ann. Oncol. 2002, 13, 1197–1204. [Google Scholar] [CrossRef] [PubMed]
- Schem, B.C.; Froystein, T.; Hjertaker, B.T.; Larsen, A.; Mella, O. Trimodality treatmenet with regional hyperthermia (HT), radiotherapy (RT) and chemotherapy in primary inoperable or recurrent rectal carcinoma. In Proceedings of the International Conference of Hyperthermic Oncology—ICHO, St. Louis, MO, USA, 20–24 April 2004; pp. 88–89. [Google Scholar]
- Ohno, S.; Sumiyoshi, Y.; Mori, M.; Sugimachi, K. Hyperthermia for rectal cancer. Surgery 2002, 131, S121–S127. [Google Scholar] [CrossRef] [PubMed]
- Lagendijk, J.J.W.; Van Rhoon, G.C.; Hornsleth, S.N.; Wust, P.; De Leeuw, A.C.C.; Schneider, C.J.; Van Ddk, J.D.P.; Van Der Zee, J.; Van Heek-Romanowski, R.; Rahman, S.A.; et al. ESHO quality assurance guidelines for regional hyperthermia. Int. J. Hyperth. 1998, 14, 125–133. [Google Scholar] [CrossRef]
- Gani, C.; Schroeder, C.; Heinrich, V.; Spillner, P.; Lamprecht, U.; Berger, B.; Zips, D. Long-term local control and survival after preoperative radiochemotherapy in combination with deep regional hyperthermia in locally advanced rectal cancer. Int. J. Hyperth. 2016, 32, 187–192. [Google Scholar] [CrossRef] [Green Version]
- Peeken, J.C.; Vaupel, P.; Combs, S.E. Integrating Hyperthermia into Modern Radiation Oncology: What Evidence Is Necessary? Front. Oncol. 2017, 7, 132. [Google Scholar] [CrossRef] [Green Version]
- Hermanek, P.; Hutter, R.V.; Sobin, L.H.; Wagner, G.; Wittekind, C. TNM Atlas: Illustrated Guide to TNM/pTNM Classification of Malignant Tumours, 4th ed.; Union Internationale Contre le Cancer—UICC: Geneva, Switzerland, 1997. [Google Scholar]
- Punt, C.J.A.; Buyse, M.; Köhne, C.-H.; Hohenberger, P.; Labianca, R.; Schmoll, H.J.; Påhlman, L.; Sobrero, A.; Douillard, J.-Y. Endpoints in adjuvant treatment trials: A systematic review of the literature in colon cancer and proposed definitions for future trials. J. Natl. Cancer Inst. 2007, 99, 998–1003. [Google Scholar] [CrossRef]
- Trotti, A.; Colevas, A.; Setser, A.; Rusch, V.; Jaques, D.; Budach, V.; Langer, C.; Murphy, B.; Cumberlin, R.; Coleman, C. CTCAE v3.0: Development of a comprehensive grading system for the adverse effects of cancer treatment. Semin. Radiat. Oncol. 2003, 13, 176–181. [Google Scholar] [CrossRef]
- Hornsleth, S.N.; Frydendal, L.; Mella, O.; Dahl, O.; Raskmark, P. Quality assurance for radiofrequency regional hyperthermia. Int. J. Hyperth. 1997, 13, 169–185. [Google Scholar] [CrossRef]
- Oleson, J.R.; Samulski, T.V.; Leopold, K.A.; Clegg, S.T.; Dewhirst, M.W.; Dodge, R.K.; George, S.L. Sensitivity of hyperthermia trial outcomes to temperature and time: Implications for thermal goals of treatment. Int. J. Radiat. Oncol. Biol. Phys. 1993, 25, 289–297. [Google Scholar] [CrossRef]
- Fatehi, D.; de Bruijne, M.; van der Zee, J.; van Rhoon, G.C. RHyThM, a tool for analysis of PDOS formatted hyperthermia treatment data generated by the BSD2000/3D system. Int. J. Hyperth. 2006, 22, 173–184. [Google Scholar] [CrossRef] [PubMed]
- Dworak, O.; Keilholz, L.; Hoffmann, A. Pathological features of rectal cancer after preoperative radiochemotherapy. Int. J. Colorectal Dis. 1997, 12, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Guren, M.G.; Kørner, H.; Pfeffer, F.; Myklebust, T.Å.; Eriksen, M.T.; Edna, T.-H.; Larsen, S.G.; Knudsen, K.O.; Nesbakken, A.; Wasmuth, H.H.; et al. Nationwide improvement of rectal cancer treatment outcomes in Norway, 1993–2010. Acta Oncol. 2015, 54, 1714–1722. [Google Scholar] [CrossRef]
- Kapiteijn, E.; Marijnen, C.A.; Nagtegaal, I.D.; Putter, H.; Steup, W.H.; Wiggers, T.; Rutten, H.J.; Pahlman, L.; Glimelius, B.; Van Krieken, J.H.; et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer: 12-year follow-up of the multicentre, randomised controlled TME trial. Lancet Oncol. 2011, 12, 575–582. [Google Scholar]
- Eriksen, M.; Norwegian Gastrointestinal Cancer Group; Wibe, A.; Hestvik, U.; Haffner, J.; Wiig, J.; Norwegian Rectal Cancer Group. Surgical treatment of primary locally advanced rectal cancer in Norway. Eur. J. Surg. Oncol. 2006, 32, 174–180. [Google Scholar] [CrossRef]
- 2017 European Society of Coloproctology (ESCP) Collaborating Group; Battersby, N.; Glasbey, J.C.; Neary, P.; Negoi, I.; Kamarajah, S.; Sgro, A.; Bhangu, A.; Pinkney, T.; Frasson, M.; et al. Evaluating the incidence of pathological complete response in current international rectal cancer practice; the barriers to widespread safe deferral of surgery. Colorectal Dis. 2018, 20, 58–68. [Google Scholar]
- Hartley, A.; Ho, K.F.; McConkey, C.; Geh, J.I. Pathological complete response following pre-operative chemoradiotherapy in rectal cancer: Analysis of phase II/III trials. Br. J. Radiol. 2005, 78, 934–938. [Google Scholar] [CrossRef]
- Maas, M.; Nelemans, P.J.; Valentini, V.; Das, P.; Rödel, C.; Kuo, L.-J.; A Calvo, F.; García-Aguilar, J.; Glynne-Jones, R.; Haustermans, K.; et al. Long-term outcome in patients with a pathological complete response after chemoradiation for rectal cancer: A pooled analysis of individual patient data. Lancet Oncol. 2010, 11, 835–844. [Google Scholar] [CrossRef]
- Tan, Y.; Fu, D.; Li, D.; Kong, X.; Jiang, K.; Chen, L.; Yuan, Y.; Ding, K. Predictors and Risk Factors of Pathologic Complete Response Following Neoadjuvant Chemoradiotherapy for Rectal Cancer: A Population-Based Analysis. Front. Oncol. 2019, 9, 497. [Google Scholar] [CrossRef]
- Teo, M.T.W.; McParland, L.; Appelt, A.L.; Sebag-Montefiore, D. Phase 2 Neoadjuvant Treatment Intensification Trials in Rectal Cancer: A Systematic Review. Int. J. Radiat. Oncol. Biol. Phys. 2018, 100, 146–158. [Google Scholar] [CrossRef]
- Li, J.; Ji, J.; Cai, Y.; Li, X.-F.; Li, Y.-H.; Wu, H.; Xu, B.; Dou, F.-Y.; Li, Z.-Y.; Bu, Z.-D.; et al. Preoperative concomitant boost intensity-modulated radiotherapy with oral capecitabine in locally advanced mid-low rectal cancer: A phase II trial. Radiother. Oncol. 2012, 102, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, F.; Trevisan, F.; Cabiddu, M.; Sgroi, G.; Bruschieri, L.; Rausa, E.; Ghidini, M.; Turati, L. Total Neoadjuvant Therapy in Rectal Cancer: A Systematic Review and Meta-analysis of Treatment Outcomes. Ann. Surg. 2020, 271, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Bujko, K.; Kolodziejczyk, M.; Nasierowska-Guttmejer, A.; Michalski, W.; Kepka, L.; Chmielik, E.; Wojnar, A.; Chwalinski, M. Tumour regression grading in patients with residual rectal cancer after preoperative chemoradiation. Radiother. Oncol. 2010, 95, 298–302. [Google Scholar] [CrossRef] [PubMed]
- Kong, J.C.; Guerra, G.R.; Warrier, S.K.; Lynch, A.C.; Michael, M.; Ngan, S.Y.; Phillips, W.; Ramsay, G.; Heriot, A.G. Prognostic value of tumour regression grade in locally advanced rectal cancer: A systematic review and meta-analysis. Colorectal Dis. 2018, 20, 574–585. [Google Scholar] [CrossRef] [PubMed]
- Rödel, C.; Martus, P.; Papadoupolos, T.; Füzesi, L.; Klimpfinger, M.; Fietkau, R.; Liersch, T.; Hohenberger, W.; Raab, R.; Sauer, R.; et al. Prognostic significance of tumor regression after preoperative chemoradiotherapy for rectal cancer. J. Clin. Oncol. 2005, 23, 8688–8696. [Google Scholar] [CrossRef]
- Wiig, J.N.; Larsen, S.G.; Dueland, S.; Giercksky, K.E. Clinical outcome in patients with complete pathologic response (pT0) to preoperative irradiation/chemo-irradiation operated for locally advanced or locally recurrent rectal cancer. J. Surg. Oncol. 2005, 92, 70–75. [Google Scholar] [CrossRef]
- Braendengen, M.; Glimelius, B. Preoperative radiotherapy or chemoradiotherapy in rectal cancer—Is survival improved? An update of the “Nordic” LARC study in non-resectable cancers. Radiother. Oncol. 2018, 127, 392–395. [Google Scholar] [CrossRef]
- Zwirner, K.; Bonomo, P.; Lamprecht, U.; Zips, D.; Gani, C. External validation of a rectal cancer outcome prediction model with a cohort of patients treated with preoperative radiochemotherapy and deep regional hyperthermia. Int. J. Hyperth. 2018, 34, 455–460. [Google Scholar] [CrossRef] [Green Version]
- Ott, O.; Gani, C.; Lindner, L.; Schmidt, M.; Lamprecht, U.; Abdel-Rahman, S.; Hinke, A.; Weissmann, T.; Hartmann, A.; Issels, R.; et al. Neoadjuvant Chemoradiation Combined with Regional Hyperthermia in Locally Advanced or Recurrent Rectal Cancer. Cancers 2021, 13, 1279. [Google Scholar] [CrossRef]
- Gani, C.; Lamprecht, U.; Ziegler, A.; Moll, M.; Gellermann, J.; Heinrich, V.; Wenz, S.; Fend, F.; Königsrainer, A.; Bitzer, M.; et al. Deep regional hyperthermia with preoperative radiochemotherapy in locally advanced rectal cancer, a prospective phase II trial. Radiother. Oncol. 2021, 159, 155–160. [Google Scholar] [CrossRef]
- Datta, N.R.; Kok, H.P.; Crezee, H.; Gaipl, U.S.; Bodis, S. Integrating Loco-Regional Hyperthermia Into the Current Oncology Practice: SWOT and TOWS Analyses. Front. Oncol. 2020, 10, 819. [Google Scholar] [CrossRef] [PubMed]
- De Haas-Kock, D.F.; Buijsen, J.; Pijls-Johannesma, M.; Lutgens, L.; Lammering, G.; van Mastrigt, G.A.; De Ruysscher, D.K.; Lambin, P.; van der Zee, J. Concomitant hyperthermia and radiation therapy for treating locally advanced rectal cancer. Cochrane Database Syst. Rev. 2009, CD006269. [Google Scholar] [CrossRef] [PubMed]
- Horsman, M.R.; Overgaard, J. Hyperthermia: A potent enhancer of radiotherapy. Clin. Oncol. (R Coll. Radiol.) 2007, 19, 418–426. [Google Scholar] [CrossRef]
- Elming, P.B.; Sørensen, B.S.; Oei, A.L.; Franken, N.A.P.; Crezee, J.; Overgaard, J.; Horsman, M.R. Hyperthermia: The Optimal Treatment to Overcome Radiation Resistant Hypoxia. Cancers 2019, 11, 60. [Google Scholar] [CrossRef] [Green Version]
- Hader, M.; Frey, B.; Fietkau, R.; Hecht, M.; Gaipl, U.S. Immune biological rationales for the design of combined radio- and immunotherapies. Cancer Immunol. Immunother. 2020, 69, 293–306. [Google Scholar] [CrossRef] [Green Version]
- Hader, M.; Savcigil, D.P.; Rosin, A.; Ponfick, P.; Gekle, S.; Wadepohl, M.; Bekeschus, S.; Fietkau, R.; Frey, B.; Schlücker, E.; et al. Differences of the Immune Phenotype of Breast Cancer Cells after Ex Vivo Hyperthermia by Warm-Water or Microwave Radiation in a Closed-Loop System Alone or in Combination with Radiotherapy. Cancers 2020, 12, 1082. [Google Scholar] [CrossRef]
- Allegra, C.J.; Yothers, G.; O’Connell, M.J.; Beart, R.W.; Wozniak, T.F.; Pitot, H.C.; Shields, A.F.; Landry, J.C.; Ryan, D.P.; Arora, A.; et al. Neoadjuvant 5-FU or Capecitabine Plus Radiation With or Without Oxaliplatin in Rectal Cancer Patients: A Phase III Randomized Clinical Trial. J. Natl. Cancer Inst. 2015, 107, djv248. [Google Scholar] [CrossRef] [Green Version]
- Thavaneswaran, S.; Kok, P.S.; Price, T. Evaluating the addition of oxaliplatin to single agent fluoropyrimidine in the treatment of locally advanced rectal cancer: A systematic review and meta-analysis. Expert Rev. Anticancer. Ther. 2017, 17, 965–979. [Google Scholar] [CrossRef]
- Dueland, S.; Ree, A.; Grøholt, K.; Saelen, M.; Folkvord, S.; Hole, K.; Seierstad, T.; Larsen, S.; Giercksky, K.; Wiig, J.; et al. Oxaliplatin-containing Preoperative Therapy in Locally Advanced Rectal Cancer: Local Response, Toxicity and Long-term Outcome. Clin. Oncol. (R Coll. Radiol.) 2016, 28, 532–539. [Google Scholar] [CrossRef]
- Martijnse, I.S.; Dudink, R.L.; Kusters, M.; Vermeer, T.A.; West, N.P.; Nieuwenhuijzen, G.A.; Van Lijnschoten, I.; Martijn, H.; Creemers, G.-J.; Lemmens, V.E.; et al. T3+ and T4 rectal cancer patients seem to benefit from the addition of oxaliplatin to the neoadjuvant chemoradiation regimen. Ann. Surg. Oncol. 2012, 19, 392–401. [Google Scholar] [CrossRef]
- Rödel, C.; Graeven, U.; Fietkau, R.; Hohenberger, W.; Hothorn, T.; Arnold, D.; Hofheinz, R.-D.; Ghadimi, M.; Wolff, H.A.; Lang-Welzenbach, M.; et al. Oxaliplatin added to fluorouracil-based preoperative chemoradiotherapy and postoperative chemotherapy of locally advanced rectal cancer (the German CAO/ARO/AIO-04 study): Final results of the multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2015, 16, 979–989. [Google Scholar] [CrossRef]
- Broggi, S.; Passoni, P.; Gumina, C.; Palmisano, A.; Bresolin, A.; Burgio, V.; Di Chiara, A.; Elmore, U.; Mori, M.; Slim, N.; et al. Predicting pathological response after radio-chemotherapy for rectal cancer: Impact of late oxaliplatin administration. Radiother. Oncol. 2020, 149, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Martos, C.; Pericay, C.; Aparicio, J.; Salud, A.; Safont, M.; Massuti, B.; Vera, R.; Escudero, P.; Maurel, J.; Marcuello, E.; et al. Phase II, randomized study of concomitant chemoradiotherapy followed by surgery and adjuvant capecitabine plus oxaliplatin (CAPOX) compared with induction CAPOX followed by concomitant chemoradiotherapy and surgery in magnetic resonance imaging-defined, locally advanced rectal cancer: Grupo cancer de recto 3 study. J. Clin. Oncol. 2010, 28, 859–865. [Google Scholar] [PubMed]
- Ludmir, E.B.; Palta, M.; Willett, C.G.; Czito, B.G. Total neoadjuvant therapy for rectal cancer: An emerging option. Cancer 2017, 123, 1497–1506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masi, G.; Vivaldi, C.; Fornaro, L.; Lonardi, S.; Buccianti, P.; Sainato, A.; Marcucci, L.; Martignetti, A.; Urso, E.D.L.; Castagna, M.; et al. Total neoadjuvant approach with FOLFOXIRI plus bevacizumab followed by chemoradiotherapy plus bevacizumab in locally advanced rectal cancer: The TRUST trial. Eur. J. Cancer 2019, 110, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Schrag, D.; Weiser, M.R.; Goodman, K.A.; Gönen, M.; Hollywood, E.; Cercek, A.; Reidy-Lagunes, D.L.; Gollub, M.J.; Shia, J.; Guillem, J.G.; et al. Neoadjuvant chemotherapy without routine use of radiation therapy for patients with locally advanced rectal cancer: A pilot trial. J. Clin. Oncol. 2014, 32, 513–518. [Google Scholar] [CrossRef]
- Bahadoer, R.R.; A Dijkstra, E.; van Etten, B.; Marijnen, C.A.M.; Putter, H.; Kranenbarg, E.M.-K.; Roodvoets, A.G.H.; Nagtegaal, I.D.; Beets-Tan, R.G.H.; Blomqvist, L.K.; et al. Short-course radiotherapy followed by chemotherapy before total mesorectal excision (TME) versus preoperative chemoradiotherapy, TME, and optional adjuvant chemotherapy in locally advanced rectal cancer (RAPIDO): A randomised, open-label, phase 3 trial. Lancet. Oncol. 2021, 22, 29–42. [Google Scholar] [CrossRef]
- Cercek, A.; Roxburgh, C.S.; Strombom, P.; Smith, J.J.; Temple, L.K.; Nash, G.M.; Guillem, J.G.; Paty, P.B.; Yaeger, R.; Stadler, Z.K.; et al. Adoption of Total Neoadjuvant Therapy for Locally Advanced Rectal Cancer. JAMA Oncol. 2018, 4, e180071. [Google Scholar] [CrossRef]
- Kasi, A.; Abbasi, S.; Handa, S.; Al-Rajabi, R.; Saeed, A.; Baranda, J.; Sun, W. Total Neoadjuvant Therapy vs Standard Therapy in Locally Advanced Rectal Cancer: A Systematic Review and Meta-analysis. JAMA Netw. Open 2020, 3, e2030097. [Google Scholar] [CrossRef]
- Conroy, T.; Lamfichekh, N.; Etienne, P.L.; Rio, E.; Francois, E.; Mesgouez-Nebout, N.; Vendrely, V.; Artignan, X.; Bouché, O.; Gargot, D.; et al. Total neoadjuvant therapy with mFOLFIRINOX versus preoperative chemoradiation in patieents with locally advanced rectal cancer: Final results of PRODIGE 23 phase III trial, a UNICANCER GI trial. J. Clin. Oncol. 2020, 38, 4007. [Google Scholar] [CrossRef]
- Iversen, H.; Martling, A.; Johansson, H.; Nilsson, P.; Holm, T. Pelvic local recurrence from colorectal cancer: Surgical challenge with changing preconditions. Colorectal Dis. 2018, 20, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.J.; Sagar, P.M.; Sadadcharam, G.; Tan, K.Y. Advances in surgical management for locally recurrent rectal cancer: How far have we come? World J. Gastroenterol. 2017, 23, 4170–4180. [Google Scholar] [CrossRef] [PubMed]
- Shinoto, M.; Yamada, S.; Okamoto, M.; Shioyama, Y.; Ohno, T.; Nakano, T.; Nemoto, K.; Isozaki, Y.; Kawashiro, S.; Tsuji, H.; et al. Carbon-ion radiotherapy for locally recurrent rectal cancer: Japan Carbon-ion Radiation Oncology Study Group (J-CROS) Study 1404 Rectum. Radiother. Oncol. 2019, 132, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Yamada, S.; Kamada, T.; Ebner, D.K.; Shinoto, M.; Terashima, K.; Isozaki, Y.; Yasuda, S.; Makishima, H.; Tsuji, H.; Tsujii, H.; et al. Carbon-Ion Radiation Therapy for Pelvic Recurrence of Rectal Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Regnier, A.; Ulbrich, J.; Münch, S.; Oechsner, M.; Wilhelm, D.; Combs, S.E.; Habermehl, D. Comparative Analysis of Efficacy, Toxicity, and Patient-Reported Outcomes in Rectal Cancer Patients Undergoing Preoperative 3D Conformal Radiotherapy or VMAT. Front. Oncol. 2017, 7, 225. [Google Scholar] [CrossRef] [Green Version]
- Van der Valk, M.J.; Marijnen, C.A.; van Etten, B.; Dijkstra, E.A.; Hilling, D.E.; Kranenbarg, E.M.; Putter, H.; Roodvoets, A.G.; Bahadoer, R.R.; Fokstuen, T.; et al. Compliance and tolerability of short-course radiotherapy followed by preoperative chemotherapy and surgery for high-risk rectal cancer—Results of the international randomized RAPIDO-trial. Radiother. Oncol. 2020, 147, 75–83. [Google Scholar] [CrossRef]
- Schulze, T.; Wust, P.; Gellermann, J.; Hildebrandt, B.; Riess, H.; Felix, R.; Rau, B. Influence of neoadjuvant radiochemotherapy combined with hyperthermia on the quality of life in rectum cancer patients. Int. J. Hyperth. 2006, 22, 301–318. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Total | Male | Female |
|---|---|---|---|
| Included | 49 | 32 | 17 |
| Age (years) | 59.1 (range 21.0–75.6) | 60.3 (range 21.0–75.6) | 56.9 (range 39.4–74.7) |
| Locally advanced | 43 | 27 | 16 |
| Level 0–5 cm | 19 | 15 | 4 |
| Level 6–10 cm | 21 | 11 | 10 |
| Level 11–15 cm | 3 | 1 | 2 |
| Mean height cm | 6.7 | 6.1 | 7.4 |
| T3 | 19 | 11 | 8 |
| T4 | 24 | 16 | 8 |
| N0 | 3 | 3 | 0 |
| N1 | 17 | 11 | 1 |
| N2 | 21 | 12 | 9 |
| Nx | 2 | 1 | 1 |
| Moderate | 14 | 7 | 7 |
| High risk | 29 | 20 | 9 |
| Local recurrence | 6 | 5 | 1 |
| Grade | Maximal Acute Toxicity | Skin Toxicity | Diarrhoea | General Condition | Urinary | Nausea | Oxaliplatin Fever | Other |
|---|---|---|---|---|---|---|---|---|
| 1 | 11 | 5 | 17 | 2 | 4 | 8 | 11 | 5 |
| 2 | 16 | 4 | 13 | 7 | 3 | 4 | 1 | 9 |
| 3 | 19 | 3 | 7 | 3 | 0 | 0 | 2 | 9 |
| 4 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| No surgery | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schem, B.-C.; Pfeffer, F.; Ott, M.A.; Wiig, J.N.; Sletteskog, N.; Frøystein, T.; Myklebust, M.P.; Leh, S.; Dahl, O.; Mella, O. Long-Term Outcome in a Phase II Study of Regional Hyperthermia Added to Preoperative Radiochemotherapy in Locally Advanced and Recurrent Rectal Adenocarcinomas. Cancers 2022, 14, 705. https://doi.org/10.3390/cancers14030705
Schem B-C, Pfeffer F, Ott MA, Wiig JN, Sletteskog N, Frøystein T, Myklebust MP, Leh S, Dahl O, Mella O. Long-Term Outcome in a Phase II Study of Regional Hyperthermia Added to Preoperative Radiochemotherapy in Locally Advanced and Recurrent Rectal Adenocarcinomas. Cancers. 2022; 14(3):705. https://doi.org/10.3390/cancers14030705
Chicago/Turabian StyleSchem, Baard-Christian, Frank Pfeffer, Martin Anton Ott, Johan N. Wiig, Nils Sletteskog, Torbjørn Frøystein, Mette Pernille Myklebust, Sabine Leh, Olav Dahl, and Olav Mella. 2022. "Long-Term Outcome in a Phase II Study of Regional Hyperthermia Added to Preoperative Radiochemotherapy in Locally Advanced and Recurrent Rectal Adenocarcinomas" Cancers 14, no. 3: 705. https://doi.org/10.3390/cancers14030705
APA StyleSchem, B.-C., Pfeffer, F., Ott, M. A., Wiig, J. N., Sletteskog, N., Frøystein, T., Myklebust, M. P., Leh, S., Dahl, O., & Mella, O. (2022). Long-Term Outcome in a Phase II Study of Regional Hyperthermia Added to Preoperative Radiochemotherapy in Locally Advanced and Recurrent Rectal Adenocarcinomas. Cancers, 14(3), 705. https://doi.org/10.3390/cancers14030705