
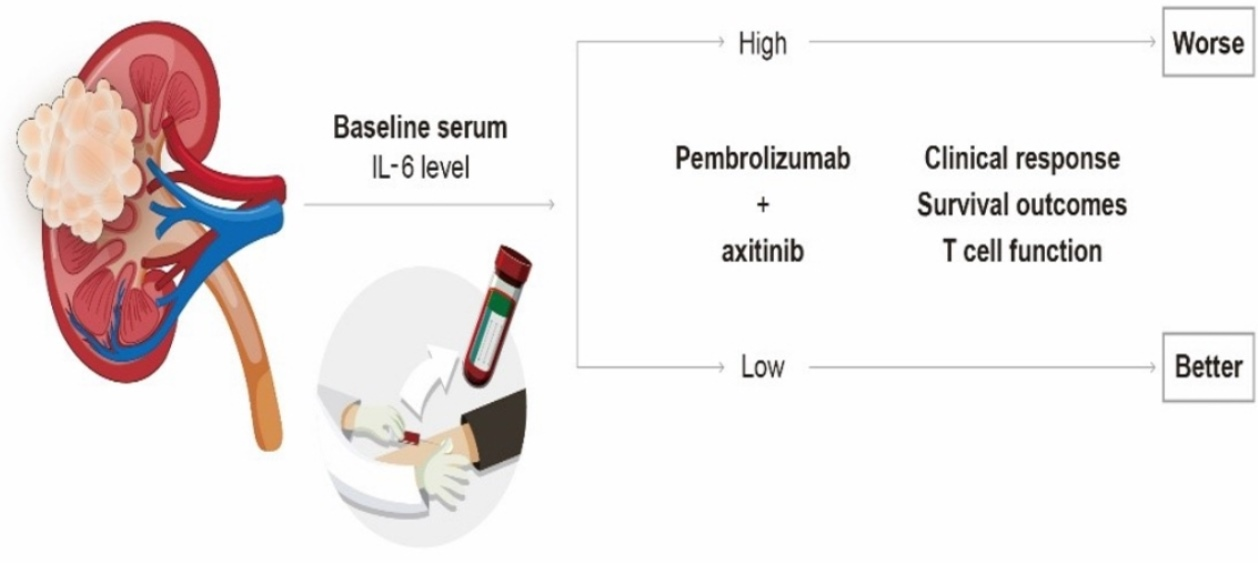
High Serum Levels of IL-6 Predict Poor Responses in Patients Treated with Pembrolizumab plus Axitinib for Advanced Renal Cell Carcinoma

 , , , and
, , , and
Abstract
Simple Summary
Abstract

1. Introduction
2. Materials and Methods
2.1. Patients and Treatments
2.2. Sample Collection and Measurement of Serum IL-6
2.3. Cytokine Secretion Assays and Flow Cytometry
2.4. Analysis of a Public Database
2.5. Statistical Analysis
3. Results
3.1. Potential Effects of IL-6 on Tumor Immunity
3.2. Patient Demography and Disease Outcome
3.3. Baseline Serum IL-6 Levels and Clinical Response to Pembrolizumab/Axitinib
3.4. Baseline Serum IL-6 Levels and Survival Outcome with Pembro/Axi Therapy
3.5. High Serum IL-6 Levels Are Associated with Reduced T-Cell Responses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Padala, S.A.; Barsouk, A.; Thandra, K.C.; Saginala, K.; Mohammed, A.; Vakiti, A.; Rawla, P.; Barsouk, A. Epidemiology of renal cell carcinoma. World J. Oncol. 2020, 11, 79. [Google Scholar] [CrossRef] [PubMed]
- Osawa, T.; Takeuchi, A.; Kojima, T.; Shinohara, N.; Eto, M.; Nishiyama, H. Overview of current and future systemic therapy for metastatic renal cell carcinoma. Jpn. J. Clin. Oncol. 2019, 49, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Hong, M.H.; Kim, H.S.; Kim, C.; Ahn, J.R.; Chon, H.J.; Shin, S.-J.; Ahn, J.-B.; Chung, H.C.; Rha, S.Y. Treatment outcomes of sunitinib treatment in advanced renal cell carcinoma patients: A single cancer center experience in Korea. Cancer Res. Treat. 2009, 41, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Rini, B.I.; Plimack, E.R.; Stus, V.; Gafanov, R.; Hawkins, R.; Nosov, D.; Pouliot, F.; Alekseev, B.; Soulières, D.; Melichar, B. Pembrolizumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N. Engl. J. Med. 2019, 380, 1116–1127. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Plimack, E.R.; Soulières, D.; Waddell, T.; Stus, V.; Gafanov, R.; Nosov, D.; Pouliot, F.; Melichar, B.; Vynnychenko, I. Pembrolizumab plus axitinib versus sunitinib monotherapy as first-line treatment of advanced renal cell carcinoma (KEYNOTE-426): Extended follow-up from a randomised, open-label, phase 3 trial. Lancet Oncol. 2020, 21, 1563–1573. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.; Stein, J.E.; Rimm, D.L.; Wang, D.W.; Bell, J.M.; Johnson, D.B.; Sosman, J.A.; Schalper, K.A.; Anders, R.A.; Wang, H. Comparison of biomarker modalities for predicting response to PD-1/PD-L1 checkpoint blockade: A systematic review and meta-analysis. JAMA Oncol. 2019, 5, 1195–1204. [Google Scholar] [CrossRef] [PubMed]
- An, H.J.; Chon, H.J.; Kim, C. Peripheral blood-based biomarkers for immune checkpoint inhibitors. Int. J. Mol. Sci. 2021, 22, 9414. [Google Scholar] [CrossRef]
- Kim, C.W.; Chon, H.J.; Kim, C. Combination Immunotherapies to Overcome Intrinsic Resistance to Checkpoint Blockade in Microsatellite Stable Colorectal Cancer. Cancers 2021, 13, 4906. [Google Scholar] [CrossRef]
- Schumacher, N.; Schmidt, S.; Schwarz, J.; Dohr, D.; Lokau, J.; Scheller, J.; Garbers, C.; Chalaris, A.; Rose-John, S.; Rabe, B. Circulating soluble IL-6R but not ADAM17 activation drives mononuclear cell migration in tissue inflammation. J. Immunol. 2016, 197, 3705–3715. [Google Scholar] [CrossRef]
- Lippitz, B.E.; Harris, R.A. Cytokine patterns in cancer patients: A review of the correlation between interleukin 6 and prognosis. Oncoimmunology 2016, 5, e1093722. [Google Scholar] [CrossRef]
- Knüpfer, H.; Preiss, R. Serum interleukin-6 levels in colorectal cancer patients—A summary of published results. Int. J. Color. Dis. 2010, 25, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Tsukamoto, H.; Fujieda, K.; Hirayama, M.; Ikeda, T.; Yuno, A.; Matsumura, K.; Fukuma, D.; Araki, K.; Mizuta, H.; Nakayama, H. Soluble IL6R Expressed by Myeloid Cells Reduces Tumor-Specific Th1 Differentiation and Drives Tumor ProgressionMyeloid Cell–Derived sIL6R Dampens Antitumor Th1 Responses. Cancer Res. 2017, 77, 2279–2291. [Google Scholar] [CrossRef] [PubMed]
- Hoejberg, L.; Bastholt, L.; Schmidt, H. Interleukin-6 and melanoma. Melanoma Res. 2012, 22, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Rossi, J.-F.; Lu, Z.-Y.; Jourdan, M.; Klein, B. Interleukin-6 as a Therapeutic TargetAnti-IL6 Therapy. Clin. Cancer Res. 2015, 21, 1248–1257. [Google Scholar] [CrossRef] [PubMed]
- Negrier, S.; Perol, D.; Menetrier-Caux, C.; Escudier, B.; Pallardy, M.; Ravaud, A.; Douillard, J.-Y.; Chevreau, C.; Lasset, C.; Blay, J.-Y. Interleukin-6, interleukin-10, and vascular endothelial growth factor in metastatic renal cell carcinoma: Prognostic value of interleukin-6—From the Groupe Francais d’Immunotherapie. J. Clin. Oncol. 2004, 22, 2371–2378. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, Y. Prognostic role of interleukin-6 in renal cell carcinoma: A meta-analysis. Clin. Transl. Oncol. 2020, 22, 835–843. [Google Scholar] [CrossRef]
- Gudbrandsdottir, G.; Aarstad, H.H.; Bostad, L.; Hjelle, K.M.; Aarstad, H.J.; Bruserud, Ø.; Tvedt, T.H.A.; Beisland, C. Serum levels of the IL-6 family of cytokines predict prognosis in renal cell carcinoma (RCC). Cancer Immunol. Immunother. 2021, 70, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Tran, H.T.; Liu, Y.; Zurita, A.J.; Lin, Y.; Baker-Neblett, K.L.; Martin, A.-M.; Figlin, R.A.; Hutson, T.E.; Sternberg, C.N.; Amado, R.G. Prognostic or predictive plasma cytokines and angiogenic factors for patients treated with pazopanib for metastatic renal-cell cancer: A retrospective analysis of phase 2 and phase 3 trials. Lancet Oncol. 2012, 13, 827–837. [Google Scholar] [CrossRef]
- Tsukamoto, H.; Fujieda, K.; Senju, S.; Ikeda, T.; Oshiumi, H.; Nishimura, Y. Immune-suppressive effects of interleukin-6 on T-cell-mediated anti-tumor immunity. Cancer Sci. 2018, 109, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Veglia, F.; Perego, M.; Gabrilovich, D. Myeloid-derived suppressor cells coming of age. Nat. Immunol. 2018, 19, 108–119. [Google Scholar] [CrossRef]
- Liu, C.; Yang, L.; Xu, H.; Zheng, S.; Wang, Z.; Wang, S.; Yang, Y.; Zhang, S.; Feng, X.; Sun, N. Systematic analysis of IL-6 as a predictive biomarker and desensitizer of immunotherapy responses in patients with non-small cell lung cancer. BMC Med. 2022, 20, 187. [Google Scholar]
- Zheng, Z.; Zheng, X.; Zhu, Y.; Yao, Z.; Zhao, W.; Zhu, Y.; Sun, F.; Mu, X.; Wang, Y.; He, W. IL-6 promotes the proliferation and immunosuppressive function of myeloid-derived suppressor cells via the MAPK signaling pathway in bladder cancer. BioMed Res. Int. 2021, 2021, 5535578. [Google Scholar] [CrossRef] [PubMed]
- Bent, E.H.; Millán-Barea, L.R.; Zhuang, I.; Goulet, D.R.; Fröse, J.; Hemann, M.T. Microenvironmental IL-6 inhibits anti-cancer immune responses generated by cytotoxic chemotherapy. Nat. Commun. 2021, 12, 6218. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Lee, W.S.; Lee, H.J.; Yang, H.; Lee, S.J.; Kong, S.J.; Je, S.; Yang, H.-J.; Jung, J.; Cheon, J. Deep learning model enables the discovery of a novel immunotherapeutic agent regulating the kynurenine pathway. Oncoimmunology 2021, 10, 2005280. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Fu, J.; Zeng, Z.; Cohen, D.; Li, J.; Chen, Q.; Li, B.; Liu, X.S. TIMER2.0 for analysis of tumor-infiltrating immune cells. Nucleic Acids Res. 2020, 48, W509–W514. [Google Scholar] [CrossRef]
- Walter, M.; Liang, S.; Ghosh, S.; Hornsby, P.; Li, R. Interleukin 6 secreted from adipose stromal cells promotes migration and invasion of breast cancer cells. Oncogene 2009, 28, 2745–2755. [Google Scholar] [CrossRef]
- Taniguchi, K.; Karin, M. IL-6 and related cytokines as the critical lynchpins between inflammation and cancer. Semin. Immunol. 2014, 26, 54–74. [Google Scholar]
- Naka, T.; Nishimoto, N.; Kishimoto, T. The paradigm of IL-6: From basic science to medicine. Arthritis Res. Ther. 2002, 4, S233–S242. [Google Scholar] [CrossRef]
- Wu, J.; Gao, F.; Wang, C.; Qin, M.; Han, F.; Xu, T.; Hu, Z.; Long, Y.; He, X.; Deng, X. IL-6 and IL-8 secreted by tumour cells impair the function of NK cells via the STAT3 pathway in oesophageal squamous cell carcinoma. J. Exp. Clin. Cancer Res. 2019, 38, 321. [Google Scholar] [CrossRef]
- Pilskog, M.; Nilsen, G.H.; Beisland, C.; Straume, O. Elevated plasma interleukin 6 predicts poor response in patients treated with sunitinib for metastatic clear cell renal cell carcinoma. Cancer Treat. Res. Commun. 2019, 19, 100127. [Google Scholar] [CrossRef]
- Mizuno, R.; Kimura, G.; Fukasawa, S.; Ueda, T.; Kondo, T.; Hara, H.; Shoji, S.; Kanao, K.; Nakazawa, H.; Tanabe, K. Angiogenic, inflammatory and immunologic markers in predicting response to sunitinib in metastatic renal cell carcinoma. Cancer Sci. 2017, 108, 1858–1863. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Number of Patients, n (% of Total) |
|---|---|
| Age | |
| ≥65 | 23 (39.7) |
| Male | 42 (72.4) |
| ECOG performance status | |
| 0 | 22 (37.9) |
| 1 | 29 (50.0) |
| 2 | 7 (12.1) |
| IMDC prognostic risk | |
| Favorable | 11 (19.0) |
| Intermediate | 29 (50.0) |
| Poor | 18 (31.0) |
| Pathology | |
| Clear cell | 41 (70.7) |
| Non-clear cell | 17 (29.3) |
| No. of organs with metastases | |
| 1 | 20 (34.5) |
| ≥2 | 38 (65.5) |
| Sites of metastasis | |
| Lung | 47 (81.0) |
| Lymph node | 17 (29.3) |
| Bone | 21 (36.2) |
| Liver | 6 (10.3) |
| Previous nephrectomy | 30 (51.7) |
| Characteristic | IL-6 Low (n = 36) | IL-6 High (n = 22) | p-Value |
|---|---|---|---|
| Age | |||
| Median (range), y | 61 (39–82) | 59 (47–83) | 0.572 |
| ≥65, n (%) | 13 (36.1) | 10 (45.5) | 0.480 |
| Male, n (%) | 28 (77.8) | 14 (63.6) | 0.242 |
| ECOG performance status | 0.316 | ||
| 0 | 16 (44.4) | 6 (27.3) | |
| 1 | 17 (47.2) | 12 (54.5) | |
| 2 | 3 (8.3) | 4 (18.2) | |
| IMDC prognostic risk, n (%) | 0.009 | ||
| Favorable | 9 (25.0) | 2 (9.1) | |
| Intermediate | 21 (58.3) | 8 (36.4) | |
| Poor | 6 (16.7) | 12 (54.5) | |
| Pathology, n (%) | 0.356 | ||
| Clear cell | 27 (75.0) | 14 (63.6) | |
| Non-clear cell | 9 (25.0) | 8 (36.4) | |
| No. of organs with metastases, n (%) | 0.366 | ||
| 0, 1 | 14 (38.9) | 6 (27.3) | |
| ≥2 | 22 (61.1) | 16 (72.7) | |
| Sites of metastasis, n (%) | |||
| Lung | 28 (77.8) | 19 (86.4) | 0.418 |
| Lymph node | 7 (19.4) | 10 (45.5) | 0.035 |
| Bone | 9 (25.0) | 12 (54.5) | 0.023 |
| Liver | 4 (11.1) | 2 (9.1) | 0.806 |
| Previous nephrectomy, n (%) | 28 (53.8) | 2 (33.3) | 0.018 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sang, Y.B.; Yang, H.; Lee, W.S.; Lee, S.J.; Kim, S.-G.; Cheon, J.; Kang, B.; Kim, C.W.; Chon, H.J.; Kim, C. High Serum Levels of IL-6 Predict Poor Responses in Patients Treated with Pembrolizumab plus Axitinib for Advanced Renal Cell Carcinoma. Cancers 2022, 14, 5985. https://doi.org/10.3390/cancers14235985
Sang YB, Yang H, Lee WS, Lee SJ, Kim S-G, Cheon J, Kang B, Kim CW, Chon HJ, Kim C. High Serum Levels of IL-6 Predict Poor Responses in Patients Treated with Pembrolizumab plus Axitinib for Advanced Renal Cell Carcinoma. Cancers. 2022; 14(23):5985. https://doi.org/10.3390/cancers14235985
Chicago/Turabian StyleSang, Yun Beom, Hannah Yang, Won Suk Lee, Seung Joon Lee, Seul-Gi Kim, Jaekyung Cheon, Beodeul Kang, Chang Woo Kim, Hong Jae Chon, and Chan Kim. 2022. "High Serum Levels of IL-6 Predict Poor Responses in Patients Treated with Pembrolizumab plus Axitinib for Advanced Renal Cell Carcinoma" Cancers 14, no. 23: 5985. https://doi.org/10.3390/cancers14235985
APA StyleSang, Y. B., Yang, H., Lee, W. S., Lee, S. J., Kim, S.-G., Cheon, J., Kang, B., Kim, C. W., Chon, H. J., & Kim, C. (2022). High Serum Levels of IL-6 Predict Poor Responses in Patients Treated with Pembrolizumab plus Axitinib for Advanced Renal Cell Carcinoma. Cancers, 14(23), 5985. https://doi.org/10.3390/cancers14235985