The Impact of Facility Surgical Caseload Volumes on Survival Outcomes in Patients Undergoing Radical Cystectomy

 ,
, 

Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Variables
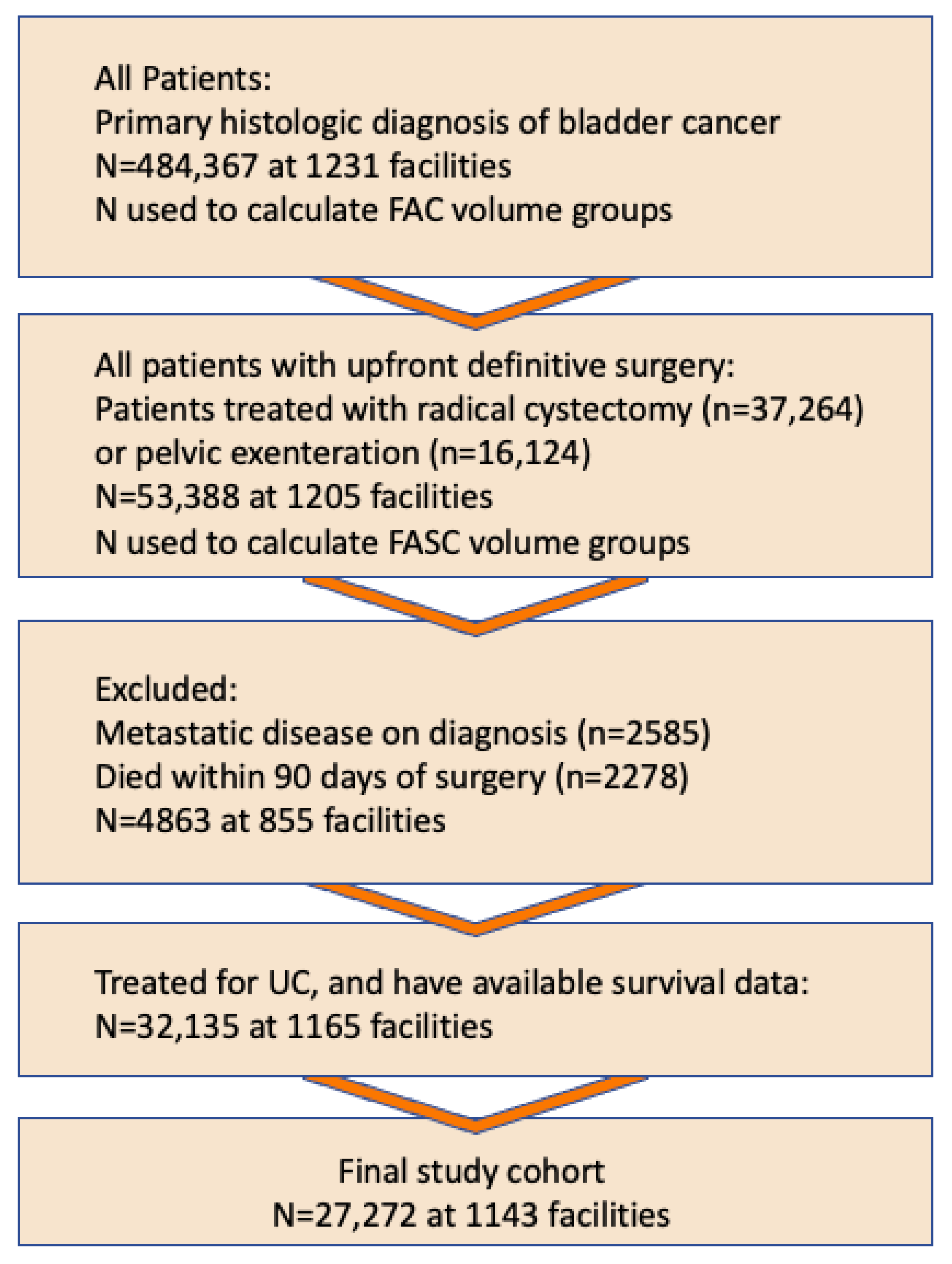
2.3. Patient Selection
2.4. Hypothesis
2.5. Statistical Analysis

3. Results
3.1. Results by Facility Volume Groups
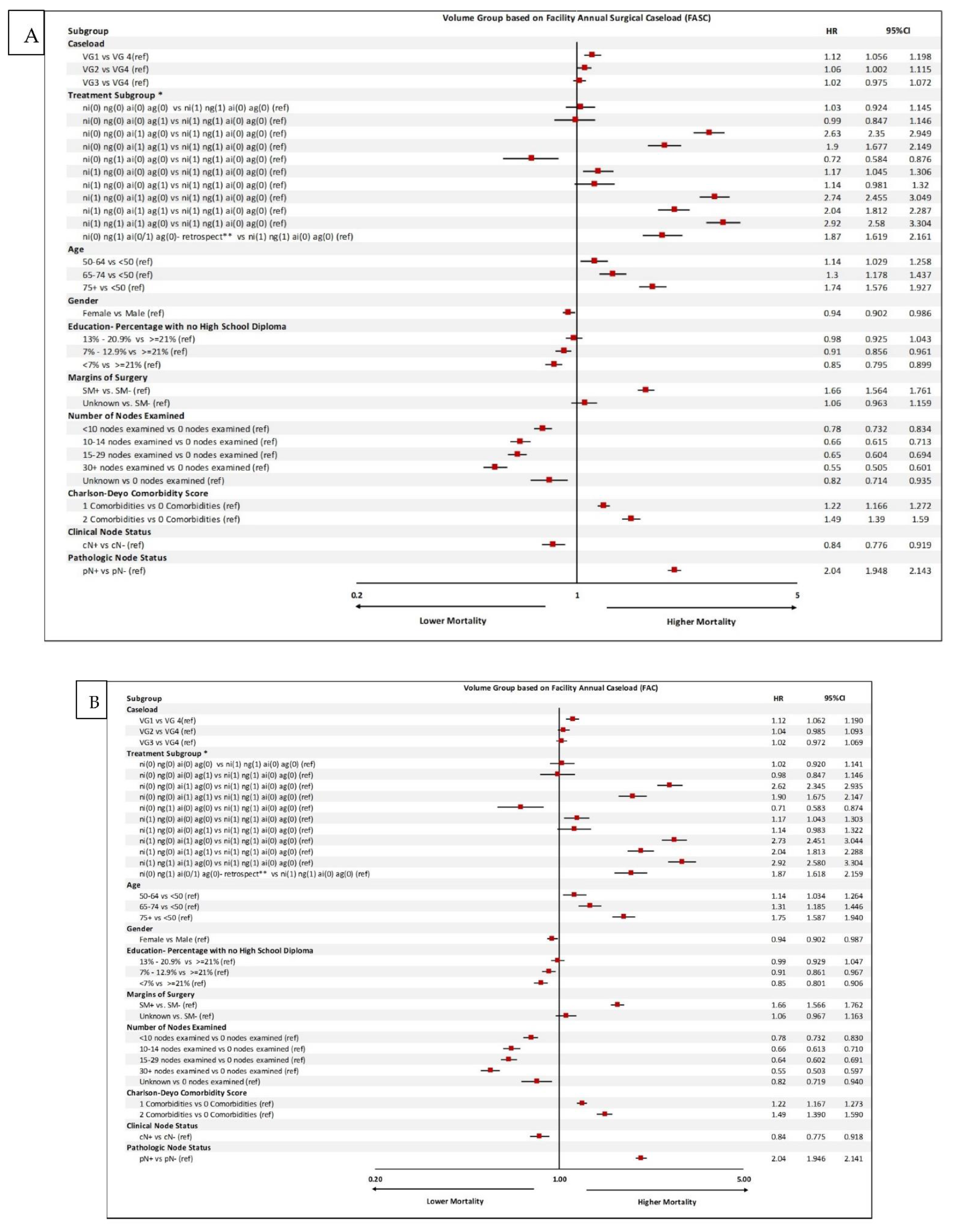
3.2. Univariable and Multivariable Survival Analyses
3.3. Overall Survival Curves

4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Joudi, F.N.; Konety, B.R. The impact of provider volume on outcomes from urological cancer therapy. J. Urol. 2005, 174, 432–438. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, G.S.; Urbach, D.R.; Austin, P.C.; Fleshner, N.E.; Laupacis, A. Higher surgeon and hospital volume improves long-term survival after radical cystectomy. Cancer 2013, 119, 3546–3554. [Google Scholar] [CrossRef] [PubMed]
- Morgan, T.M.; Barocas, D.A.; Keegan, K.A.; Cookson, M.S.; Chang, S.S.; Ni, S.; Clark, P.E.; Smith, J.A., Jr.; Penson, D.F. Volume outcomes of cystectomy--is it the surgeon or the setting? J. Urol. 2012, 188, 2139–2144. [Google Scholar] [CrossRef] [PubMed]
- Nuttall, M.; Van Der Meulen, J.; Phillips, N.; Sharpin, C.; Gillatt, D.; McIntosh, G.; Emberton, M. A systematic review and critique of the literature relating hospital or surgeon volume to health outcomes for 3 urological cancer procedures. J. Urol. 2004, 172 (6 Pt 1), 2145–2152. [Google Scholar] [CrossRef] [PubMed]
- Wilt, T.J.; Shamliyan, T.A.; Taylor, B.C.; MacDonald, R.; Kane, R.L. Association between hospital and surgeon radical prostatectomy volume and patient outcomes: A systematic review. J. Urol. 2008, 180, 820–828; discussion 8–9. [Google Scholar] [CrossRef] [PubMed]
- Afshar, M.; Goodfellow, H.; Jackson-Spence, F. Centralisation of radical cystectomies for bladder cancer in England, a decade on from the ‘Improving Outcomes Guidance’: The case for super centralization. BJU Int. 2018, 121, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Hounsome, L.S.; Verne, J.; McGrath, J.S.; Gillatt, D.A. Trends in operative caseload and mortality rates after radical cystectomy for bladder cancer in England for 1998–2010. Eur. Urol. 2015, 67, 1056–1062. [Google Scholar] [CrossRef] [PubMed]
- Fedeli, U.; De Paoli, A.; Corti, M.C.; Cacciamani, G.E.; Gill, I.S.; Zattoni, F.; Novara, G.; Porreca, A.; Artibani, W. Perioperative Mortality and Long-Term Survival after Radical Cystectomy: A Population-Based Study in a Southern European Country on 4389 Patients. Urol. Int. 2020, 104, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Scarberry, K.; Berger, N.G.; Scarberry, K.B.; Agrawal, S.; Francis, J.J.; Yih, J.M.; Gonzalez, C.M.; Abouassaly, R. Improved surgical outcomes following radical cystectomy at high-volume centers influence overall survival. Urol. Oncol. 2018, 36, 308.e11–308.e17. [Google Scholar] [CrossRef] [PubMed]
- Goossens-Laan, C.A.; Gooiker, G.A.; van Gijn, W.; Post, P.N.; Bosch, J.R.; Kil, P.J.; Wouters, M.W. A systematic review and meta-analysis of the relationship between hospital/surgeon volume and outcome for radical cystectomy: An update for the ongoing debate. Eur. Urol. 2011, 59, 775–783. [Google Scholar] [CrossRef] [PubMed]
- Vickers, A.; Savage, C.; Bianco, F.; Mulhall, J.; Sandhu, J.; Guillonneau, B.; Cronin, A.; Scardino, P. Cancer control and functional outcomes after radical prostatectomy as markers of surgical quality: Analysis of heterogeneity between surgeons at a single cancer center. Eur. Urol. 2011, 59, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Vickers, A.J.; Bianco, F.J.; Serio, A.M.; Eastham, J.A.; Schrag, D.; Klein, E.A.; Reuther, A.M.; Kattan, M.W.; Pontes, J.E.; Scardino, P.T. The surgical learning curve for prostate cancer control after radical prostatectomy. J. Natl. Cancer Inst. 2007, 99, 1171–1177. [Google Scholar] [CrossRef] [PubMed]
- Eastham, J.A. Do high-volume hospitals and surgeons provide better care in urologic oncology? Urol. Oncol. 2009, 27, 417–421. [Google Scholar] [CrossRef] [PubMed]
- Barocas, D.A.; Mitchell, R.; Chang, S.S.; Cookson, M.S. Impact of surgeon and hospital volume on outcomes of radical prostatectomy. Urol. Oncol. 2010, 28, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Lin, D.; Wei, L. The Robust Inference for the Cox Proportional Hazards Model. J. Am. Stat. Assoc. 1989, 48, 1074–1078. [Google Scholar] [CrossRef]
- Goossens-Laan, C.A.; Visser, O.; Hulshof, M.C.; Wouters, M.W.; Bosch, J.R.; Coebergh JW, W.; Kil, P.J. Survival after treatment for carcinoma invading bladder muscle: A Dutch population-based study on the impact of hospital volume. BJU Int. 2012, 110, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, M.E.; Mallin, K.; Weaver, M.A.; Palis, B.; Stewart, A.; Winchester, D.P.; Milowsky, M.I. Association of hospital volume with conditional 90-day mortality after cystectomy: An analysis of the National Cancer Data Base. BJU Int. 2014, 114, 46–55. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Variable | N | % |
|---|---|---|
| Number of Patients | 27,272 | |
| Median Age at Diagnosis | 68 | |
| Interquartile range | (61, 75) | |
| Range | (21, 90) | |
| Race/ethnicity | ||
| White | 24,883 | 91.2% |
| Black | 1508 | 5.5% |
| Other | 587 | 2% |
| Primary Payor | ||
| Not Insured | 800 | 2.9% |
| Private Insurance | 8897 | 32.6% |
| Medicaid | 1144 | 4.2% |
| Medicare | 15,642 | 57.4% |
| Other Government | 271 | 1.0% |
| Insurance Status Unknown | 518 | 1.9% |
| Charlson–Deyo Comorbidity Score | ||
| 0 | 19,263 | 70.6% |
| 1 | 6146 | 22.5% |
| 2 | 1863 | 6.8% |
| Great Circle Distance | ||
| Median | 16 | |
| Facility Type | ||
| Community Cancer Program | 1727 | 6.3% |
| Comprehensive Community Cancer Program | 8705 | 31.9% |
| Academic/Research Program | 14,139 | 51.8% |
| Integrated Network Cancer Program | 2535 | 9.3% |
| Volume Group Based on Facility Annual Surgical Caseload (FASC) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Volume Group | 1 | 2 | 3 | 4 | ||||
| Percentile [volume range] | <50th [0–2] | 50–74th [3–5] | 75–89th [6–11] | 90th+ [12+] | ||||
| Number of Facilities (total) | 903 | 100% | 748 | 100% | 464 | 100% | 251 | 100% |
| Community Cancer Program | 314 | 35% | 133 | 18% | 25 | 5% | 4 | 2% |
| Comprehensive Community Cancer Program | 462 | 51% | 417 | 56% | 235 | 51% | 54 | 22% |
| Academic/Research Program | 98 | 11% | 137 | 18% | 133 | 29% | 111 | 44% |
| Integrated Network Cancer Program | 19 | 2% | 36 | 5% | 41 | 9% | 26 | 10% |
| Unknown | 10 | 1% | 25 | 3% | 30 | 6% | 56 | 22% |
| Unique Facility Counts * | 886 | 713 | 419 | 190 | ||||
| Number of Patients Served (total) | 2804 | 100% | 4584 | 100% | 6355 | 100% | 13,529 | 100% |
| Community Cancer Program | 984 | 35% | 586 | 13% | 142 | 2% | 15 | 0% |
| Comprehensive Community Cancer Program | 1506 | 54% | 2795 | 61% | 3303 | 52% | 1101 | 8% |
| Academic/Research Program | 266 | 9% | 932 | 20% | 2175 | 34% | 10,766 | 80% |
| Integrated Network Cancer Program | 38 | 1% | 244 | 5% | 702 | 11% | 1551 | 11% |
| Unknown | 10 | 0% | 27 | 1% | 33 | 1% | 96 | 1% |
| Volume Group Based on Facility Annual Caseload (FAC) | ||||||||
| Volume Group | 1 | 2 | 3 | 4 | ||||
| Percentile [volume range] | <50th [0–28] | 50–74th [29–47] | 75–89th [48–70] | 90th+ [71+] | ||||
| Number of Facilities (total) | 717 | 100% | 633 | 100% | 423 | 100% | 257 | 100% |
| Community Cancer Program | 308 | 43% | 83 | 13% | 10 | 2% | 7 | 3% |
| Comprehensive Community Cancer Program | 293 | 41% | 394 | 62% | 241 | 57% | 77 | 30% |
| Academic/Research Program | 82 | 11% | 112 | 18% | 114 | 27% | 92 | 36% |
| Integrated Network Cancer Program | 9 | 1% | 13 | 2% | 30 | 7% | 40 | 16% |
| Unknown | 25 | 3% | 31 | 5% | 28 | 7% | 41 | 16% |
| Unique Facility Counts * | 689 | 596 | 387 | 202 | ||||
| Number of Patients Served (total) | 3828 | 100% | 5011 | 100% | 6611 | 100% | 11,822 | 100% |
| Community Cancer Program | 1321 | 35% | 323 | 6% | 48 | 1% | 35 | 0% |
| Comprehensive Community Cancer Program | 1653 | 43% | 2950 | 59% | 2613 | 40% | 1489 | 13% |
| Academic/Research Program | 794 | 21% | 1587 | 32% | 3441 | 52% | 8317 | 70% |
| Integrated Network Cancer Program | 33 | 1% | 119 | 2% | 475 | 7% | 1908 | 16% |
| Unknown | 27 | 1% | 32 | 1% | 34 | 1% | 73 | 1% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cacciamani, G.E.; Barzi, A.; Eppler, M.B.; Lara, P.N., Jr.; Pan, C.-X.; Bhanvadia, S.K.; Gill, P.; Aron, M.; Gill, I.; Sadeghi, S. The Impact of Facility Surgical Caseload Volumes on Survival Outcomes in Patients Undergoing Radical Cystectomy. Cancers 2022, 14, 5984. https://doi.org/10.3390/cancers14235984
Cacciamani GE, Barzi A, Eppler MB, Lara PN Jr., Pan C-X, Bhanvadia SK, Gill P, Aron M, Gill I, Sadeghi S. The Impact of Facility Surgical Caseload Volumes on Survival Outcomes in Patients Undergoing Radical Cystectomy. Cancers. 2022; 14(23):5984. https://doi.org/10.3390/cancers14235984
Chicago/Turabian StyleCacciamani, Giovanni E., Afsaneh Barzi, Michael B. Eppler, Primo N. Lara, Jr., Chong-Xian Pan, Sumeet K. Bhanvadia, Parkash Gill, Monish Aron, Inderbir Gill, and Sarmad Sadeghi. 2022. "The Impact of Facility Surgical Caseload Volumes on Survival Outcomes in Patients Undergoing Radical Cystectomy" Cancers 14, no. 23: 5984. https://doi.org/10.3390/cancers14235984
APA StyleCacciamani, G. E., Barzi, A., Eppler, M. B., Lara, P. N., Jr., Pan, C.-X., Bhanvadia, S. K., Gill, P., Aron, M., Gill, I., & Sadeghi, S. (2022). The Impact of Facility Surgical Caseload Volumes on Survival Outcomes in Patients Undergoing Radical Cystectomy. Cancers, 14(23), 5984. https://doi.org/10.3390/cancers14235984