


The Effect of Melatonin Intake on Survival of Patients with Breast Cancer—A Population-Based Registry Study


Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Characteristics
2.2. Statistical Analysis
3. Results
3.1. Patient and Tumor Characteristics
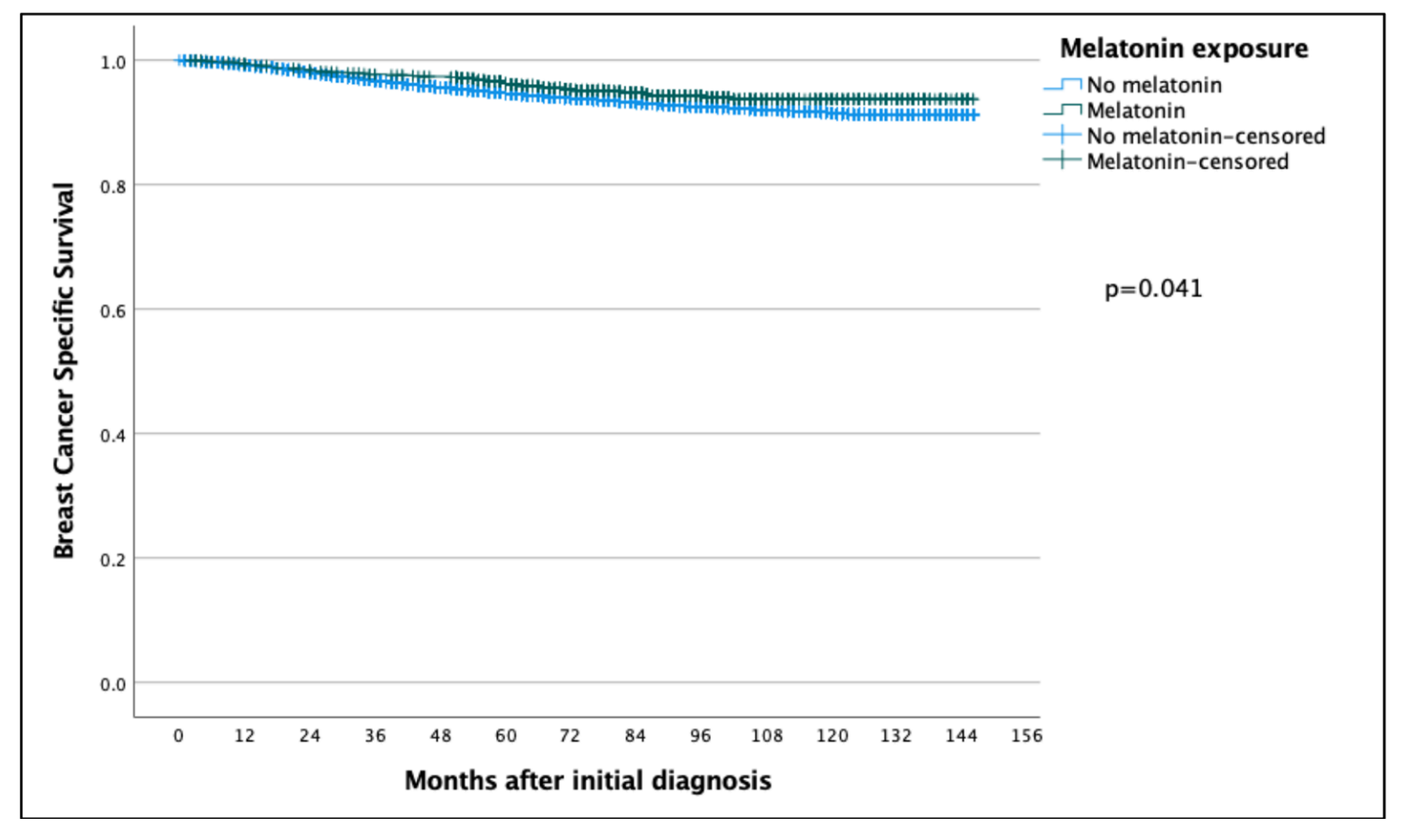
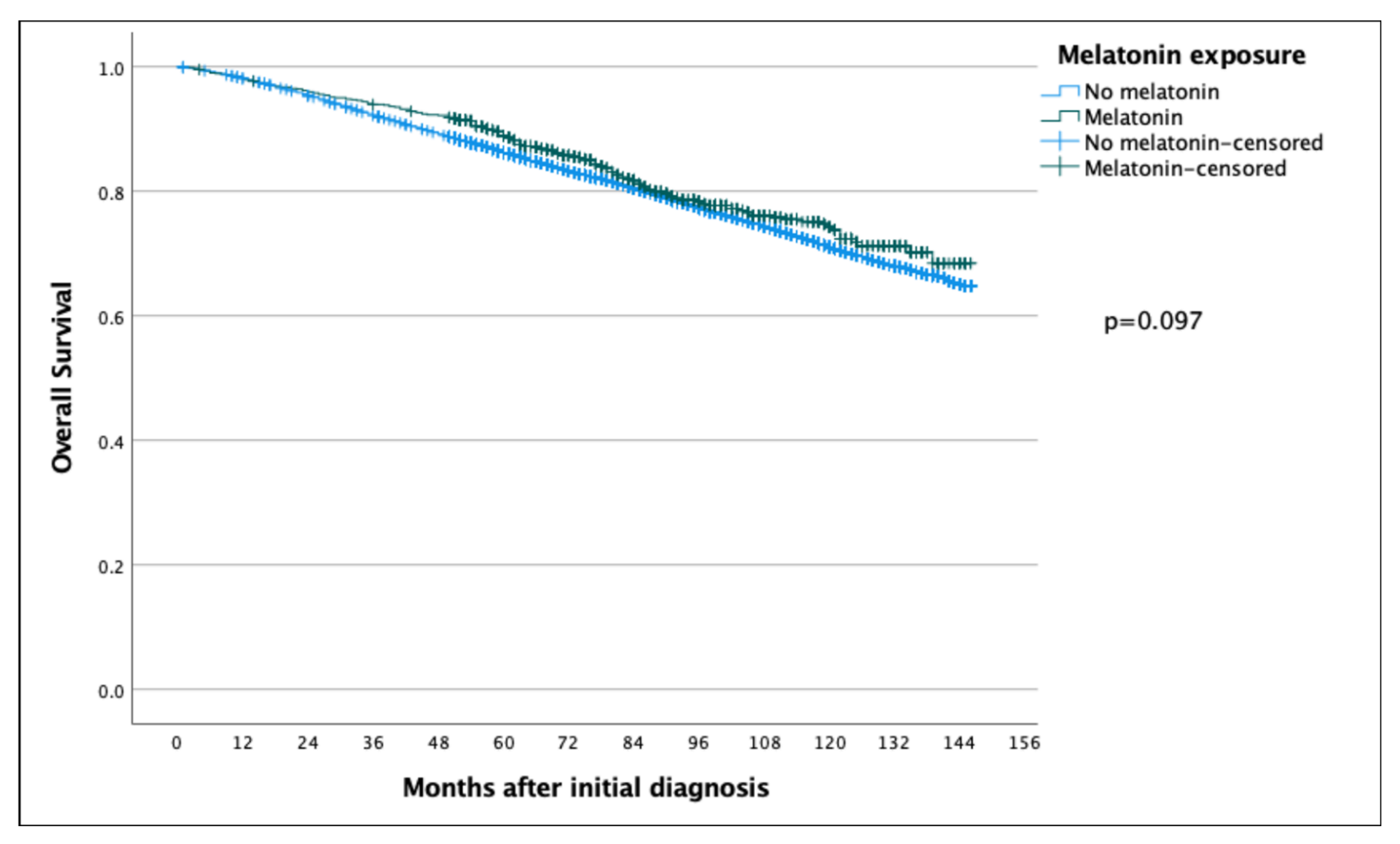
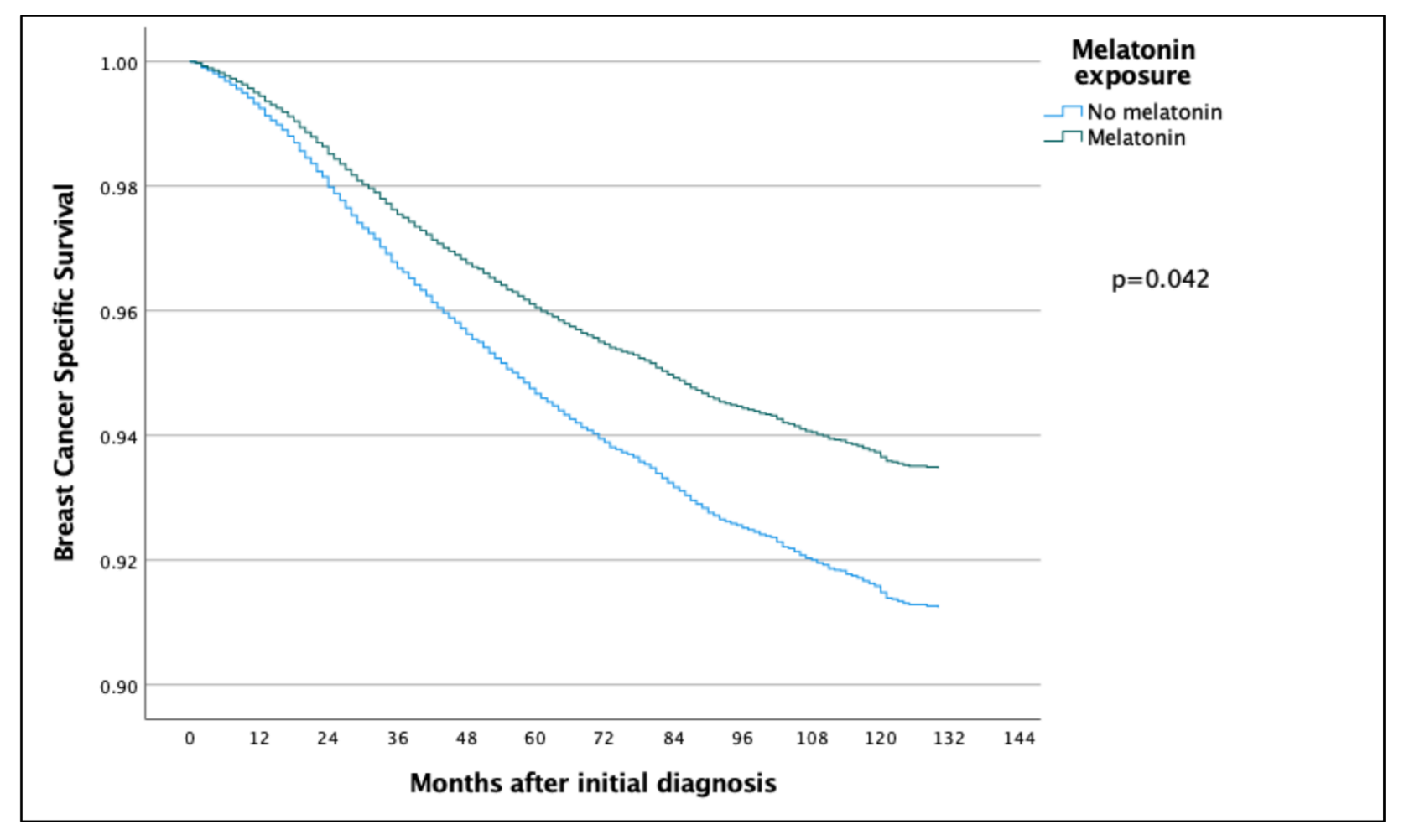
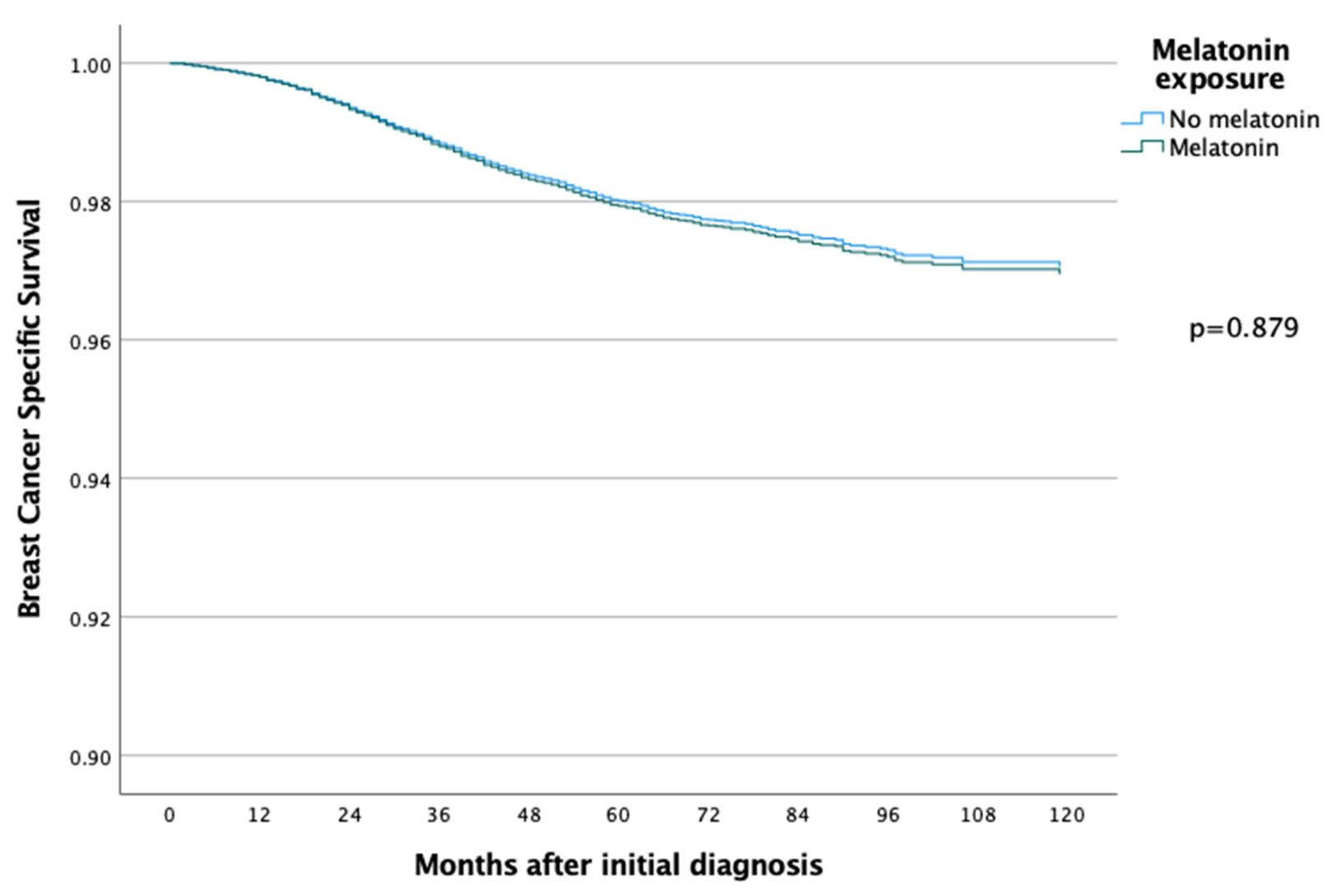
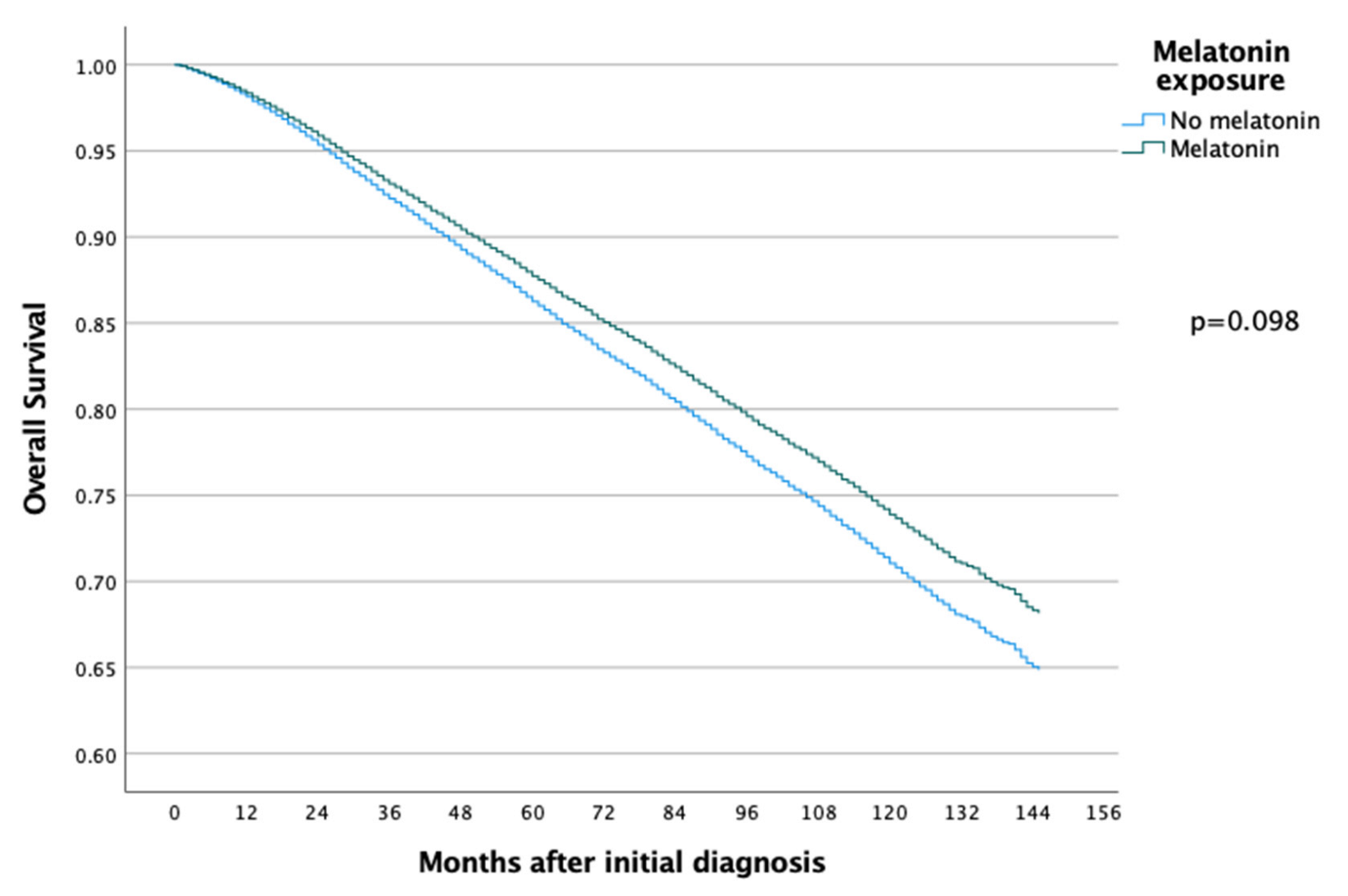
3.2. Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lerner, A.B.; Case, J.D.; Takahashi, Y. Isolation of Melatonin and 5-Methoxyindole-3-acetic Acid from Bovine Pineal Glands. J. Biol. Chem. 1960, 235, 1992–1997. [Google Scholar] [CrossRef] [PubMed]
- Tan, D.-X.; Hardeland, R.; Manchester, L.C.; Paredes, S.D.; Korkmaz, A.; Sainz, R.M.; Mayo, J.C.; Fuentes-Broto, L.; Reiter, R.J. The changing biological roles of melatonin during evolution: From an antioxidant to signals of darkness, sexual selection and fitness. Biol. Rev. 2009, 85, 607–623. [Google Scholar] [CrossRef] [PubMed]
- Hardeland, R.; Cardinali, D.P.; Srinivasan, V.; Spence, D.W.; Brown, G.M.; Pandi-Perumal, S.R. Melatonin—A pleiotropic, orchestrating regulator molecule. Prog. Neurobiol. 2011, 93, 350–384. [Google Scholar] [CrossRef] [PubMed]
- Reiter, R.J.; Tan, D.X.; Galano, A. Melatonin: Exceeding Expectations. Physiology 2014, 29, 325–333. [Google Scholar] [CrossRef]
- Cohen, M.; Lippman, M.; Chabner, B. Role of pineal gland in aetiology and treatment of breast cancer. Lancet 1978, 2, 814–816. [Google Scholar] [CrossRef]
- Cos, S.; González, A.; Güezmes, A.; Mediavilla, M.D.; Martínez-Campa, C.M.; Alonso-Gonzalez, C.; Sánchez-Barceló, E.J. Melatonin inhibits the growth of DMBA-induced mammary tumors by decreasing the local biosynthesis of estrogens through the modulation of aromatase activity. Int. J. Cancer 2005, 118, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Jardim-Perassi, B.V.; Arbab, A.S.; Ferreira, L.C.; Borin, T.F.; Varma, N.R.S.; Iskander, A.S.M.; Shankar, A.; Ali, M.M.; Zuccari, D.A.P.D.C. Effect of Melatonin on Tumor Growth and Angiogenesis in Xenograft Model of Breast Cancer. PLoS ONE 2014, 9, e85311. [Google Scholar] [CrossRef] [PubMed]
- Karadas, A.K.; Dilmac, S.; Aytac, G.; Tanriover, G. Melatonin decreases metastasis, primary tumor growth and angiogenesis in a mice model of breast cancer. Hum. Exp. Toxicol. 2021, 40, 1545–1557. [Google Scholar] [CrossRef] [PubMed]
- Lopes, J.R.; da Silva Kavagutti, M.; de Medeiros, F.A.F.; de Campos Zuccari, D.A.P. Evaluation of Melatonin Effect on Human Breast Cancer Stem Cells Using a Threedimensional Growth Method of Mammospheres. Anti-Cancer Agents Med. Chem. 2017, 17, 961–965. [Google Scholar] [CrossRef] [PubMed]
- Cucina, A.; Proietti, S.; D’Anselmi, F.; Coluccia, P.; Dinicola, S.; Frati, L.; Bizzarri, M. Evidence for a biphasic apoptotic pathway induced by melatonin in MCF-7 breast cancer cells. J. Pineal Res. 2009, 46, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Liu, B.; Guan, Y.; Gong, M.; Zhang, W.; Pan, J.; Liu, Y.; Liang, R.; Yuan, Y.; Ye, L. Melatonin inhibits the proliferation of breast cancer cells induced by bisphenol A via targeting estrogen receptor-related pathways. Thorac. Cancer 2018, 9, 368–375. [Google Scholar] [CrossRef] [PubMed]
- Mao, L.; Summers, W.; Xiang, S.; Yuan, L.; Dauchy, R.T.; Reynolds, A.; Wren-Dail, M.A.; Pointer, D.; Frasch, T.; Blask, D.E.; et al. Melatonin Represses Metastasis in Her2-Postive Human Breast Cancer Cells by Suppressing RSK2 Expression. Mol. Cancer Res. 2016, 14, 1159–1169. [Google Scholar] [CrossRef] [PubMed]
- Grant, S.G.; Melan, M.A.; Latimer, J.J.; Witt-Enderby, P.A. Melatonin and breast cancer: Cellular mechanisms, clinical studies and future perspectives. Expert Rev. Mol. Med. 2009, 11, e5. [Google Scholar] [CrossRef] [PubMed]
- Kong, X.; Gao, R.; Wang, Z.; Wang, X.; Fang, Y.; Gao, J.; Reiter, R.J.; Wang, J. Melatonin: A Potential Therapeutic Option for Breast Cancer. Trends Endocrinol. Metab. 2020, 31, 859–871. [Google Scholar] [CrossRef] [PubMed]
- Cipolla-Neto, J.; Amaral, F.G.; Soares, J.M., Jr.; Gallo, C.C.; Furtado, A.; Cavaco, J.E.; Gonçalves, I.; Santos, C.R.A.; Quintela, T. The crosstalk between melatonin and sex steroid hormones. Neuroendocrinology 2021, 112, 115–129. [Google Scholar] [CrossRef] [PubMed]
- Amin, N.; Shafabakhsh, R.; Reiter, R.J.; Asemi, Z. Melatonin is an appropriate candidate for breast cancer treatment: Based on known molecular mechanisms. J. Cell Biochem. 2019, 120, 12208–12215. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Barcelo, E.J.; Cos, S.; Mediavilla, D.; Martínez-Campa, C.M.; González, A.; Alonso-González, C. Melatonin-estrogen interactions in breast cancer. J. Pineal Res. 2005, 38, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Cos, S.; Gonzalez, A.; Martinez-Campa, C.; Mediavilla, M.; Alonso-Gonzalez, C.; Sanchez-Barcelo, E. Melatonin as a Selective Estrogen Enzyme Modulator. Curr. Cancer Drug Targets 2008, 8, 691–702. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, A.; Cos, S.; Martínez-Campa, C.M.; Alonso-Gonzalez, C.; Sanchez-Mateos, S.; Mediavilla, M.D.; Sanchez-Barcelo, E.J. Selective estrogen enzyme modulator actions of melatonin in human breast cancer cells. J. Pineal Res. 2008, 45, 86–92. [Google Scholar] [CrossRef]
- Jin, Y.; Choi, Y.; Heo, K.; Park, S.-J. Melatonin as an Oncostatic Molecule Based on Its Anti-Aromatase Role in Breast Cancer. Int. J. Mol. Sci. 2021, 22, 438. [Google Scholar] [CrossRef] [PubMed]
- Schernhammer, E.S.; Laden, F.; Speizer, F.E.; Willett, W.C.; Hunter, D.J.; Kawachi, I.; Colditz, G.A. Rotating night shifts and risk of breast cancer in women participating in the nurses’ health study. J. Natl. Cancer Inst. 2001, 93, 1563–1568. [Google Scholar] [CrossRef] [PubMed]
- Menegaux, F.; Truong, T.; Anger, A.; Cordina-Duverger, E.; Lamkarkach, F.; Arveux, P.; Kerbrat, P.; Févotte, J.; Guénel, P. Night work and breast cancer: A population-based case-control study in France (the CECILE study). Int. J. Cancer 2012, 132, 924–931. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-M.; Jin, B.-Z.; Ai, F.; Duan, C.-H.; Lü, Y.-Z.; Dong, T.-F.; Fu, Q.-L. The efficacy and safety of melatonin in concurrent chemotherapy or radiotherapy for solid tumors: A meta-analysis of randomized controlled trials. Cancer Chemother. Pharmacol. 2012, 69, 1213–1220. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, P.; Zheng, X.; Du, X. Therapeutic strategies of melatonin in cancer patients: A systematic review and meta-analysis. OncoTargets Ther. 2018, 11, 7895–7908. [Google Scholar] [CrossRef] [PubMed]
- Sedighi Pashaki, A.; Mohammadian, K.; Afshar, S.; Gholami, M.H.; Moradi, A.; Javadinia, S.A.; Keshtpour Amlashi, Z. A Randomized, Controlled, Parallel-Group, Trial on the Effects of Melatonin on Fatigue Associated with Breast Cancer and Its Adjuvant Treatments. Integr. Cancer Ther. 2021, 20, 1534735420988343. [Google Scholar] [CrossRef] [PubMed]
- Ben-David, M.A.; Elkayam, R.; Gelernter, I.; Pfeffer, R.M. Melatonin for Prevention of Breast Radiation Dermatitis: A Phase II, Prospective, Double-Blind Randomized Trial. Isr. Med. Assoc. J. 2016, 18, 188–192. [Google Scholar]
- Hansen, M.V.; Madsen, M.T.; Andersen, L.T.; Hageman, I.; Rasmussen, L.S.; Bokmand, S.; Rosenberg, J.; Gögenur, I. Effect of Melatonin on Cognitive Function and Sleep in relation to Breast Cancer Surgery: A Randomized, Double-Blind, Placebo-Controlled Trial. Int. J. Breast Cancer 2014, 2014, 416351. [Google Scholar] [CrossRef]
- Hansen, M.V.; Andersen, L.T.; Madsen, M.T.; Hageman, I.; Rasmussen, L.S.; Bokmand, S.; Rosenberg, J.; Gögenur, I. Effect of melatonin on depressive symptoms and anxiety in patients undergoing breast cancer surgery: A randomized, double-blind, placebo-controlled trial. Breast Cancer Res. Treat. 2014, 145, 683–695. [Google Scholar] [CrossRef]
- Chen, W.Y.; Giobbie-Hurder, A.; Gantman, K.; Savoie, J.; Scheib, R.; Parker, L.M.; Schernhammer, E. A randomized, placebo-controlled trial of melatonin on breast cancer survivors: Impact on sleep, mood, and hot flashes. Breast Cancer Res. Treat. 2014, 145, 381–388. [Google Scholar] [CrossRef]
- Zhao, Z.-Y.; Xie, Y.; Fu, Y.-R.; Bogdan, A.; Touitou, Y. Aging and the circadian rhythm of melatonin: A cross-sectional study of Chinese subjects 30-110 yr of age. Chronobiol. Int. 2002, 19, 1171–1182. [Google Scholar] [CrossRef]
- Wurtman, R.J. Age-related decreases in melatonin secretion--clinical consequences. J. Clin. Endocrinol. Metab. 2000, 85, 2135–2136. [Google Scholar] [PubMed]
- Lissoni, P.; Barni, S.; Meregalli, S.; Fossati, V.; Cazzaniga, M.E.; Esposti, D.; Tancini, G. Modulation of cancer endocrine therapy by melatonin: A phase II study of tamoxifen plus melatonin in metastatic breast cancer patients progressing under tamoxifen alone. Br. J. Cancer 1995, 71, 854–856. [Google Scholar] [CrossRef] [PubMed]
- Lissoni, P.; Ardizzoia, A.; Barni, S.; Paolorossi, F.; Tancini, G.; Meregalli, S.; Esposti, D.; Zubelewicz, B.; Braczowski, R. A randomized study of tamoxifen alone versus tamoxifen plus melatonin in estrogen receptor-negative heavily pretreated metastatic breast-cancer patients. Oncol. Rep. 1995, 2, 871–873. [Google Scholar] [CrossRef] [PubMed]
- Cos, S.; Martinez-Campa, C.; Mediavilla, M.D.; Sanchez-Barcelo, E.J. Melatonin modulates aromatase activity in MCF-7 human breast cancer cells. J. Pineal Res. 2005, 38, 136–142. [Google Scholar] [CrossRef]
- Li, Y.; Li, S.; Zhou, Y.; Meng, X.; Zhang, J.-J.; Xu, D.-P.; Li, H.-B. Melatonin for the prevention and treatment of cancer. Oncotarget 2017, 8, 39896–39921. [Google Scholar] [CrossRef]
- Alonso-González, C.; González, A.; Martínez-Campa, C.; Gómez-Arozamena, J.; Cos, S. Melatonin sensitizes human breast cancer cells to ionizing radiation by downregulating proteins involved in double-strand DNA break repair. J. Pineal Res. 2015, 58, 189–197. [Google Scholar] [CrossRef]
- Alonso-Gonzalez, C.; Menendez-Menendez, J.; Gonzalez-Gonzalez, A.; Gonzalez, A.; Cos, S.; Martinez-Campa, C. Melatonin enhances the apoptotic effects and modulates the changes in gene expression induced by docetaxel in MCF7 human breast cancer cells. Int. J. Oncol. 2018, 52, 560–570. [Google Scholar]
- Sabzichi, M.; Samadi, N.; Mohammadian, J.; Hamishehkar, H.; Akbarzadeh, M.; Molavi, O. Sustained release of melatonin: A novel approach in elevating efficacy of tamoxifen in breast cancer treatment. Colloids Surf. B Biointerfaces 2016, 145, 64–71. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All Patients (n = 37,075) | No Melatonin (n = 36,149, 97.5%) | Melatonin (n = 926, 2.5%) | p-Value | |
|---|---|---|---|---|---|
| Age (median, IQR) | 68 (62–74) | 68 (62–74) | 67 (62–73) | 0.019 | |
| Menstrual status (%) missing: 713 | Premenopausal | 268 (0.7) | 262 (0.7) | 6 (0.7) | 0.568 |
| Postmenopausal | 34,725 (93.7) | 33,864 (95.5) | 861 (94.9) | ||
| Uncertain | 1369 (3.7) | 1329 (3.7) | 40 (4.4) | ||
| Screening diagnosed (%) missing: 142 | No | 17,343 (46.8) | 16,874 (46.9) | 469 (50.8) | 0.019 |
| Yes | 19,590 (52.8) | 19,135 (53.1) | 455 (49.2) | ||
| Type of surgery (%) missing: 135 | Breast conservation | 21,527 (58.1) | 20,975 (58.0) | 552 (59.6) | 0.571 |
| Mastectomy | 15,474 (41.7) | 15,101 (41.8) | 373 (40.3) | ||
| No breast surgery | 65 (0.2) | 64 (0.2) | 1 (0.1) | ||
| Axillary surgery (%) missing: 135 | No axillary surgery | 1171 (3.2) | 1142 (3.2) | 29 (3.1) | 0.645 |
| Sentinel node biopsy | 24,049 (64.9) | 23,435 (65.1) | 614 (66.3) | ||
| Axillary node dissection | 4873 (13.1) | 4766 (13.2) | 107 (11.6) | ||
| SNB + ALND | 5920 (16.0) | 5770 (16) | 150 (16.2) | ||
| Axillary sampling | 927 (2.5) | 901 (2.5) | 26 (2.8) | ||
| Tumor type (%) missing: 0 | Ductal | 27,516 (74.2) | 26,840 (74.2) | 676 (73.0) | 0.080 |
| Lobular | 5324 (14.4) | 5169 (14.3) | 155 (16.7) | ||
| Other | 4235 (11.4) | 4140 (11.5) | 95 (10.3) | ||
| Tumor size in mm (median, IQR) missing: 668 | 16 (11–25) | 16 (11–25) | 16 (11–23) | 0.033 | |
| NHG (%) missing: 670 | Grade I | 8031 (21.7) | 7819 (22) | 212 (23.4) | 0.616 |
| Grade II | 18,753 (50.6) | 18,296 (51.5) | 457 (50.4) | ||
| Grade III | 9621 (26.0) | 9383 (26.4) | 238 (26.2) | ||
| ER status (%) missing: 864 | Positive | 31,804 (85.8) | 30,994 (87.8) | 810 (88.9) | 0.311 |
| Negative | 4407 (11.9) | 4306 (12.2) | 101 (11.1) | ||
| PR status (%) missing: 1076 | Positive | 26,090 (70.4) | 25,429 (72.5) | 661 (72.9) | 0.783 |
| Negative | 9909 (26.7) | 9663 (27.5) | 246 (27.1) | ||
| HER2 status (%) missing: 4827 | Positive | 3750 (10.1) | 3655 (11.6) | 95 (11.8) | 0.898 |
| Negative | 28,498 (76.9) | 27,786 (88.4) | 712 (88.2) | ||
| Ki67 (median, IQR) missing: 18,379 | 20 (10–33) | 20 (10–33) | 19 (10–34) | 0.177 | |
| T status (%) missing: 668 | T1 | 24,081 (65.0) | 23,450 (66.1) | 631 (69) | 0.076 |
| T2 | 11,013 (29.7) | 10,752 (30.3) | 261 (28.5) | ||
| T3 | 1313 (3.5) | 1290 (3.6) | 23 (2.5) | ||
| N status (%) missing: 1752 | N0 | 24,931 (67.2) | 24,299 (70.6) | 632 (71.4) | 0.090 |
| N1 | 7384 (19.9) | 7193 (20.9) | 191 (21.6) | ||
| N2 | 1984 (5.4) | 1951 (5.7) | 33 (3.7) | ||
| N3 | 1024 (2.8) | 995 (2.9) | 29 (3.3) | ||
| Chemotherapy (%) missing: 6855 | Yes | 7991 (21.6) | 7779 (26.4) | 212 (27.3) | 0.575 |
| No | 22,229 (60.0) | 21,665 (73.6) | 564 (72.7) | ||
| Radiation therapy (%) missing: 6827 | Yes | 20,092 (54.2) | 19,603 (66.5) | 489 (62.6) | 0.022 |
| No | 10,156 (27.4) | 9864 (33.5) | 292 (37.4) | ||
| Endocrine therapy (%) missing: 6850 | Yes | 22,952 (61.9) | 22,376 (76.0) | 576 (74.1) | 0.233 |
| No | 7273 (19.6) | 7072 (24.0) | 201 (25.9) | ||
| HER2 therapy (%) missing: 6863 | Yes | 2233 (6.0) | 2174 (7.4) | 59 (7.6) | 0.819 |
| No | 27,979 (75.5) | 27,262 (92.6) | 717 (92.4) | ||
| Parameter | Cox Regression—BCSS | Cox Regression–OS | ||||||
|---|---|---|---|---|---|---|---|---|
| Without Adjusting Variables | With Adjusting Variables | Without Adjusting Variables | With Adjusting Variables | |||||
| HR (95%CI) | p-Value | HR (95%CI) | p-Value | HR (95%CI) | p-Value | HR (95%CI) | p-Value | |
| Patient age | 1.069 (1.065–1.074) | <0.001 | 1.056 (1.048–1.065) | <0.001 | 1.104 (1.101–1.106) | <0.001 | 1.092 (1.087–1.097) | <0.001 |
| Tumor size | 1.017 (1.016–1.017) | <0.001 | 1.017 (1.014–1.020) | <0.001 | 1.015 (1.014–1.015) | <0.001 | 1.010 (1.008–1.012) | <0.001 |
| Tumor grade | ||||||||
| NHG 1 | Ref | Ref | Ref | Ref | ||||
| NHG 2 | 3.235 (2.691–3.888)) | <0.001 | 2.127 (1.424–3.176) | <0.001 | 1.420 (1.333–1.513) | <0.001 | 1.069 (0.946–1.210) | 0.285 |
| NHG 3 | 9.450 (7.887–11.325) | <0.001 | 3.093 (2.023–4.730) | <0.001 | 2.243 (2.100–2.395) | <0.001 | 1.333 (1.145–1.553) | <0.001 |
| ER status | ||||||||
| ER positive | Ref | Ref | Ref | Ref | ||||
| ER negative | 3.619 (3.318–3.948) | <0.001 | 2.253 (1.860–2.728) | <0.001 | 1.738 (1.642–1.838) | <0.001 | 1.294 (1.147–1.461) | <0.001 |
| HER2 status | ||||||||
| HER2 positive | 1.754 (1.573–1.957) | <0.001 | 0.831 (0.685–1.008) | 0.060 | 1.090 (1.016–1.169) | 0.016 | 0.865 (0.764–0.978) | 0.021 |
| Her2 negative | Ref | Ref | Ref | Ref | ||||
| Ki67 | 1.031 (1.029–1.034) | <0.001 | 1.014 (1.010–1.018) | <0.001 | 1.015 (1.013–1.016) | <0.001 | 1.007 (1.005–1.010) | <0.001 |
| N status | ||||||||
| N0 | Ref | Ref | Ref | Ref | ||||
| N1 | 3.043 (2.739–3.380) | <0.001 | 2.391 (1.972–2.901) | <0.001 | 1.608 (1.523–1.698) | <0.001 | 1.323 (1.203–1.456) | <0.001 |
| N2 | 8.995 (8.006–10.105) | <0.001 | 5.366 (4.332–6.647) | <0.001 | 3.150 (2.929–3.389) | <0.001 | 2.123 (1.864–2.417) | <0.001 |
| N3 | 18.346 (16.234–20.733) | <0.001 | 10.239 (8.135–12.887) | <0.001 | 5.551 (5.102–6.039) | <0.001 | 3.353 (2.873–3.913) | <0.001 |
| Melatonin exposure | ||||||||
| No melatonin | Ref | Ref | Ref | Ref | ||||
| Melatonin | 0.736 (0.548–0.989) | 0.042 | 1.037 (0.648–1.659) | 0.879 | 0.886 (0.767–1.022) | 0.098 | 0.957 (0.742–1.235) | 0.735 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pistiolis, L.; Khaki, D.; Kovács, A.; Olofsson Bagge, R. The Effect of Melatonin Intake on Survival of Patients with Breast Cancer—A Population-Based Registry Study. Cancers 2022, 14, 5884. https://doi.org/10.3390/cancers14235884
Pistiolis L, Khaki D, Kovács A, Olofsson Bagge R. The Effect of Melatonin Intake on Survival of Patients with Breast Cancer—A Population-Based Registry Study. Cancers. 2022; 14(23):5884. https://doi.org/10.3390/cancers14235884
Chicago/Turabian StylePistiolis, Leda, Djino Khaki, Anikó Kovács, and Roger Olofsson Bagge. 2022. "The Effect of Melatonin Intake on Survival of Patients with Breast Cancer—A Population-Based Registry Study" Cancers 14, no. 23: 5884. https://doi.org/10.3390/cancers14235884
APA StylePistiolis, L., Khaki, D., Kovács, A., & Olofsson Bagge, R. (2022). The Effect of Melatonin Intake on Survival of Patients with Breast Cancer—A Population-Based Registry Study. Cancers, 14(23), 5884. https://doi.org/10.3390/cancers14235884