

Oral Squamous Cell Carcinoma-Associated Thrombosis: What Evidence?
 ,
,  ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Pathogenesis of Oral Cancer-Associated Thrombosis
3. OSCC and Thrombosis: A Paradoxical Relationship?
4. Remarks on Prevention and Treatment of OSCC-Associated Thrombosis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Khorana, A.A.; Mackman, N.; Falanga, A.; Pabinger, I.; Noble, S.; Ageno, W.; Moik, F.; Lee, A.Y.Y. Cancer-associated venous thromboembolism. Nat. Rev. Dis. Prim. 2022, 8, 11. [Google Scholar] [CrossRef] [PubMed]
- Abdol Razak, N.B.; Jones, G.; Bhandari, M.; Berndt, M.C.; Metharom, P. Cancer-Associated Thrombosis: An Overview of Mechanisms, Risk Factors, and Treatment. Cancers 2018, 10, 380. [Google Scholar] [CrossRef] [PubMed]
- Falanga, A.; Brenner, B.; Khorana, A.A.; Francis, C.W. Thrombotic complications in patients with cancer: Advances in pathogenesis, prevention, and treatment-A report from ICTHIC 2021. Res. Pract. Thromb. Haemost. 2022, 6, e12744. [Google Scholar] [CrossRef] [PubMed]
- Farge, D.; Frere, C.; Connors, J.M.; Khorana, A.A.; Kakkar, A.; Ay, C.; Muñoz, A.; Brenner, B.; Prata, H.; Brilhante, D.; et al. International Initiative on Thrombosis and Cancer (ITAC) advisory panel 2022 international clinical practice guidelines for the treatment and prophylaxis of venous thromboembolism in patients with cancer, including patients with COVID-19. Lancet Oncol. 2022, 23, e334–e347. [Google Scholar] [CrossRef]
- Muller, S.; Tilakaratne, W.M. Update from the 5th Edition of the World Health Organization Classification of Head and Neck Tumors: Tumours of the Oral Cavity and Mobile Tongue. Head Neck Pathol. 2022, 16, 54–62. [Google Scholar] [CrossRef]
- Mody, M.D.; Rocco, J.W.; Yom, S.S.; Haddad, R.I.; Saba, N.F. Head and neck cancer. Lancet 2021, 398, 2289–2299. [Google Scholar] [CrossRef]
- Togni, L.; Caponio, V.C.A.; Zerman, N.; Troiano, G.; Zhurakivska, K.; Muzio, L.L.; Balercia, A.; Mascitti, M.; Santarelli, A. The Emerging Impact of Tumor Budding in Oral Squamous Cell Carcinoma: Main Issues and Clinical Relevance of a New Prognostic Marker. Cancers 2022, 14, 3571. [Google Scholar] [CrossRef]
- Goel, B.; Tiwari, A.K.; Pandey, R.K.; Singh, A.P.; Kumar, S.; Sinha, A.; Jain, S.K.; Khattri, A. Therapeutic approaches for the treatment of head and neck squamous cell carcinoma—An update on clinical trials. Transl. Oncol. 2022, 21, 101426. [Google Scholar] [CrossRef]
- Li, H.; Zhang, Y.; Xu, M.; Yang, D. Current trends of targeted therapy for oral squamous cell carcinoma. J. Cancer Res. Clin. Oncol. 2022, 148, 2169–2186. [Google Scholar] [CrossRef]
- Haen, P.; Mege, D.; Crescence, L.; Dignat-George, F.; Dubois, C.; Panicot-Dubois, L. Thrombosis Risk Associated with Head and Neck Cancer: A Review. Int. J. Mol. Sci. 2019, 20, 2838. [Google Scholar] [CrossRef]
- Sanfilippo, K.M.; Moik, F.; Candeloro, M.; Ay, C.; Di Nisio, M.; Lee, A.Y.Y. Unanswered questions in cancer—Associated thrombosis. Br. J. Haematol. 2022, 198, 812–825. [Google Scholar] [CrossRef] [PubMed]
- Canonico, M.E.; Santoro, C.; Avvedimento, M.; Giugliano, G.; Mandoli, G.E.; Prastaro, M.; Franzone, A.; Piccolo, R.; Ilardi, F.; Cameli, M.; et al. Venous Thromboembolism and Cancer: A Comprehensive Review from Pathophysiology to Novel Treatment. Biomolecules 2022, 12, 259. [Google Scholar] [CrossRef] [PubMed]
- Christensen, A.; Kiss, K.; Lelkaitis, G.; Juhl, K.; Persson, M.; Charabi, B.W.; Mortensen, J.; Forman, J.L.; Sørensen, A.L.; Jensen, D.H.; et al. Urokinase-type plasminogen activator receptor (uPAR), tissue factor (TF) and epidermal growth factor receptor (EGFR): Tumor expression patterns and prognostic value in oral cancer. BMC Cancer 2017, 17, 572. [Google Scholar] [CrossRef] [PubMed]
- Ruf, W.; Edgington, T.S. Structural biology of tissue factor, the initiator of thrombogenesis in vivo. FASEB J. 1994, 8, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Adesanya, M.A.; Maraveyas, A.; Madden, L.A. Cancer microvesicles induce tissue factor-related procoagulant activity in endothelial cells in vitro. Blood Coagul. Fibrinolysis Int. J. Lab. Hematol. 2017, 28, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Thomas, G.M.; Panicot-Dubois, L.; Lacroix, R.; Dignat-George, F.; Lombardo, D.; Dubois, C. Cancer cell–derived microparticles bearing P-selectin glycoprotein ligand 1 accelerate thrombus formation in vivo. J. Exp. Med. 2009, 206, 1913–1927. [Google Scholar] [CrossRef]
- Ren, J.G.; Man, Q.W.; Zhang, W.; Li, C.; Xiong, X.P.; Zhu, J.Y.; Wang, W.M.; Sun, Z.J.; Jia, J.; Zhang, W.F.; et al. Elevated Level of Circulating Platelet-derived Microparticles in Oral Cancer. J. Dent. Res. 2016, 95, 87–93. [Google Scholar] [CrossRef]
- Lipets, E.N. Ataullakhanov FI. Global assays of hemostasis in the diagnostics of hypercoagulation and evaluation of thrombosis risk. Thromb, J. 2015, 13, 4. [Google Scholar] [CrossRef]
- Palacios-Acedo, A.L.; Langiu, M.; Crescence, L.; Mège, D.; Dubois, C.; Panicot-Dubois, L. Platelet and Cancer-Cell Interactions Modulate Cancer-Associated Thrombosis Risk in Different Cancer Types. Cancers 2022, 14, 730. [Google Scholar] [CrossRef]
- Gallo, O.; Pinto, S.; Boccuzzi, S.; Dilaghi, M.; Gallina, E.; Attanasio, M.; Gori, A.M.; Martini, F.; Abbate, R. Monocyte tumor necrosis factor production in head and neck squamous cell carcinoma. Laryngoscope 1992, 102, 447–450. [Google Scholar] [CrossRef]
- Johnstone, S.; Logan, R.M. Expression of vascular endothelial growth factor (VEGF) in normal oral mucosa, oral dysplasia and oral squamous cell carcinoma. Int. J. Oral Maxillofac. Surg. 2007, 36, 263–266. [Google Scholar] [CrossRef] [PubMed]
- Eisma, R.J.; Spiro, J.D.; Kreutzer, D.L. Vascular endothelial growth factor expression in head and neck squamous cell carcinoma. Am. J. Surg. 1997, 174, 513–517. [Google Scholar] [CrossRef]
- Slotman, G.J. Plasma thromboxane A2 and prostacyclin concentrations in squamous cell carcinoma of the head and neck. J. Surg. Oncol. 1988, 38, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, J.D.; Killion, K.M.; Pruet, C.F.; Spaulding, M.B. Von Willebrand factor in head and neck cancer. Cancer 1990, 66, 2387–2389. [Google Scholar] [CrossRef]
- Tabata, M.; Sugihara, K.; Yonezawa, S.; Yamashita, S.; Maruyama, I. An immunohistochemical study of thrombomodulin in oral squamous cell carcinoma and its association with invasive and metastatic potential. J. Oral Pathol. Med. Off. Publ. Int. Assoc. Oral Pathol. Am. Acad. Oral Pathol. 1997, 26, 258–264. [Google Scholar] [CrossRef]
- Haen, P.; Crescence, L.; Mege, D.; Altié, A.; Dubois, C.; Panicot-Dubois, L. Oral Squamous Cell Carcinoma Is Associated with a Low Thrombosis Risk Due to Storage Pool Deficiency in Platelets. Biomedicines 2021, 9, 228. [Google Scholar] [CrossRef]
- Lee, H.-Y.; Yu, N.-Y.; Lee, S.-H.; Tsai, H.-J.; Wu, C.-C.; Cheng, J.-C.; Chen, D.-P.; Wang, Y.-R.; Tseng, C.-P. Podoplanin promotes cancer-associated thrombosis and contributes to the unfavorable overall survival in an ectopic xenograft mouse model of oral cancer. Biomed. J. 2019, 43, 146–162. [Google Scholar] [CrossRef]
- Tsai, A.W.; Cushman, M.; Rosamond, W.D.; Heckbert, S.R.; Polak, J.F.; Folsom, A.R. Cardiovascular risk factors and venous thromboembolism incidence: The longitudinal investigation of thromboembolism etiology. Arch. Intern. Med. 2002, 162, 1182–1189. [Google Scholar] [CrossRef]
- Khorana, A.A.; Francis, C.W.; Culakova, E.; Lyman, G.H. Risk factors for chemotherapy-associated venous thromboembolism in a prospective observational study. Cancer. 2005, 104, 2822–2829. [Google Scholar] [CrossRef]
- Thai, L.; McCarn, K.; Stott, W.; Watts, T.; Andersen, P.E.; Gross, N.D. Venous thromboembolism in patients with head and neck cancer after surgery. Head Neck 2013, 35, 4. [Google Scholar] [CrossRef]
- Kakei, Y.; Akashi, M.; Hasegawa, T.; Minamikawa, T.; Usami, S.; Komori, T.J. Incidence of Venous Thromboembolism After Oral Oncologic Surgery with Simultaneous Reconstruction. Oral Maxillofac. Surg. 2016, 74, 212–217. [Google Scholar] [CrossRef] [PubMed]
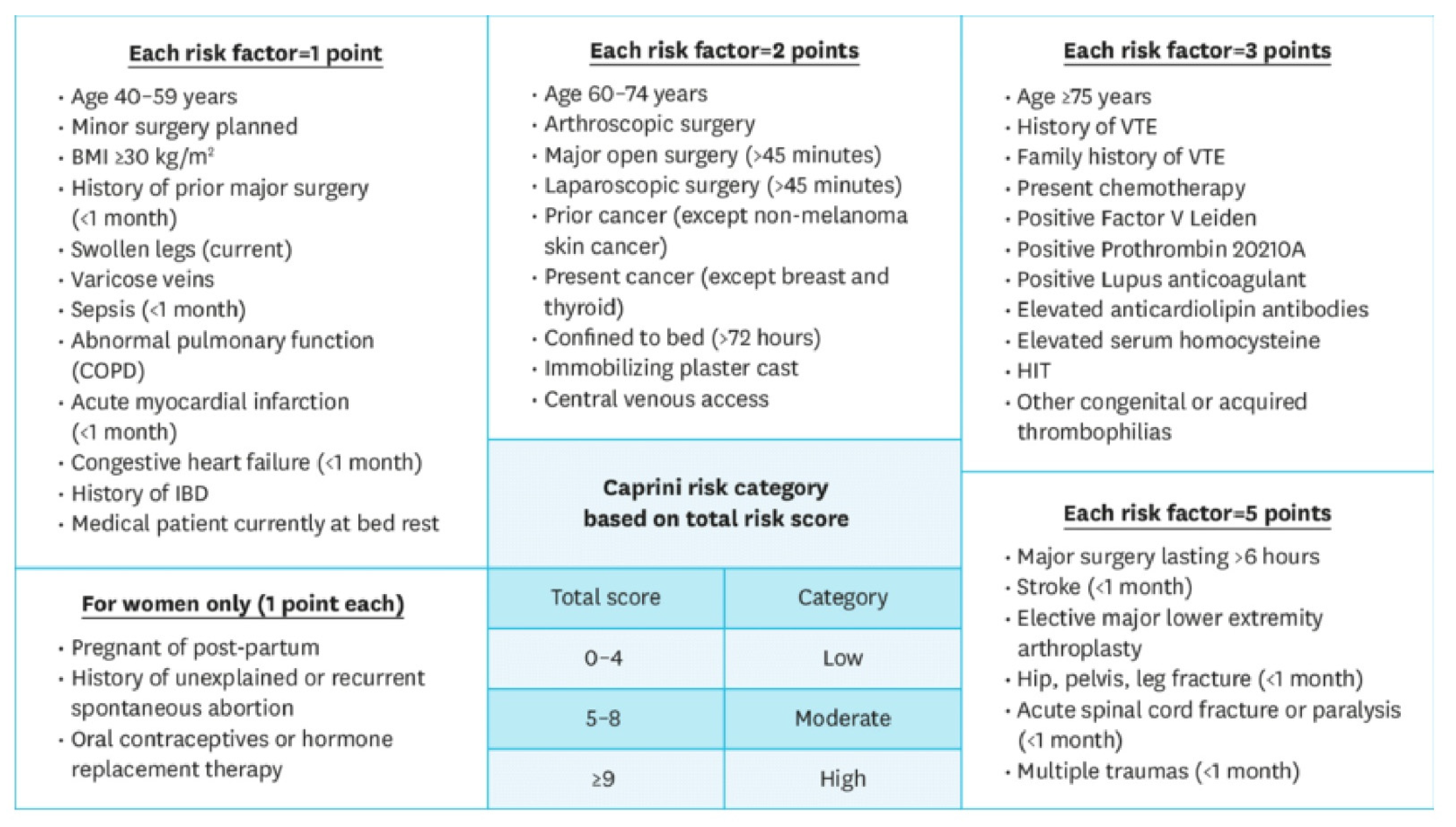
- Grant, P.J.; Greene, M.T.; Chopra, V.; Bernstein, S.J.; Hofer, T.P.; Flanders, S.A. Assessing the Caprini Score for risk assessment of venous thromboembolism in hospitalized medical patients. Am. J. Med. 2015, 129, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Khorana, A.A.; Dalal, M.; Lin, J.; Connolly, G.C. Incidence and predictors of venous thromboembolism (VTE) among ambulatory high-risk cancer patients undergoing chemotherapy in the United States. Cancer 2013, 119, 648–655. [Google Scholar] [CrossRef]
- Khorana, A.A.; Kuderer, N.M.; Culakova, E.; Lyman, G.H.; Francis, C.W. Development and validation of a predictive model for chemotherapy-associated thrombosis. Blood 2008, 111, 4902–4907. [Google Scholar] [CrossRef]
- Khorana, A.A.; Francis, C.W.; Culakova, E.; Kuderer, N.M.; Lyman, G.H. Thromboembolism is a leading cause of death in cancer patients receiving outpatient chemotherapy. J. Thromb. Haemost. 2007, 5, 632–634. [Google Scholar] [CrossRef] [PubMed]
- Oppelt, P.; Betbadal, A.; Nayak, L. Approach to chemotherapy-associated thrombosis. Vasc. Med. 2015, 20, 153–161. [Google Scholar] [CrossRef]
- Ikeda, A.; Yamachika, E.; Mizutani, M.; Moritani, N.; Nakatsuji, K.; Iida, S. Rapid occurrence of left ventricular thrombus associated with platinum-based chemotherapy plus cetuximab for the treatment of metastatic squamous cell carcinoma of the head and neck: A case report. Mol. Clin. Oncol. 2017, 7, 833–836. [Google Scholar] [CrossRef]
- Ando, Y.; Hayashi, T.; Sugimoto, R.; Nishibe, S.; Ito, K.; Kawada, K.; Ikeda, Y.; Yamada, S.; Imaizumi, K. Risk factors for cancer-associated thrombosis in patients undergoing treatment with immune checkpoint inhibitors. Investig. New Drugs 2019, 38, 1200–1206. [Google Scholar] [CrossRef]
- Vermorken, J.B.; Mesia, R.; Rivera, F.; Remenar, E.; Kawecki, A.; Rottey, S.; Erfan, J.; Zabolotnyy, D.; Kienzer, H.-R.; Cupissolet, D.; et al. Platinum-based chemotherapy plus cetuximab in head and neck cancer. N. Engl. J. Med. 2008, 359, 1116–1127. [Google Scholar] [CrossRef]
- Jiang, D.; Lee, A.I. Thrombotic Risk from Chemotherapy and Other Cancer Therapies. Cancer Treat Res. 2019, 179, 87–101. [Google Scholar]
- Burgy, M.; Barthélémy, P.; Lefevre, F.; Dupret-Bories, A.; Truntzer, P.; Korenbaum, C.; Flesch, H.; Bronner, G.; Borel, C. Cetuximab-Carboplatin-5-Fluorouracil Regimen in Elderly Patients with Recurrent or Metastatic Head and Neck Squamous-Cell Carcinoma: A French Retrospective Survey. Oncology 2017, 93, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Buxó, E.; Sosa, A.; Reig, O.; Victoria, I.; Caballero, M.; Grau, J.J.; Garcia-Morillo, M. Intravenous 5-Fluorouracil in Patients with Advanced Squamous Cell Carcinoma: A Retrospective Study. Ann. Otol. Rhinol. Laryngol. 2018, 127, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Key, N.S.; Khorana, A.A.; Kuderer, N.M.; Bohlke, K.; Lee, A.Y.Y.; Arcelus, J.I.; Wong, S.L.; Balaban, E.P.; Flowers, C.W.; Francis, C.W.; et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: ASCO clinical practice guideline update. J. Clin. Oncol. 2020, 38, 496–520. [Google Scholar] [CrossRef] [PubMed]
- Lyman, G.H.; Carrier, M.; Ay, C.; Nisio, M.D.; Hicks, L.K.; Khorana, A.A.; Leavitt, A.D.; Lee, A.Y.Y.; Macbeth, F.; Morgan, R.L.; et al. American Society of Hematology 2021 guidelines for management of venous thromboembolism: Prevention and treatment in patients with cancer. Blood Adv. 2021, 5, 927–974. [Google Scholar] [CrossRef] [PubMed]
- Cramer, J.D.; Shuman, A.G.; Brenner, M.J. Antithrombotic Therapy for Venous Thromboembolism and Prevention of Thrombosis in Otolaryngology-Head and Neck Surgery: State of the Art Review. Otolaryngol. Head Neck Surg. Off. J. Am. Acad. Otolaryngol. Head Neck Surg. 2018, 158, 627–636. [Google Scholar] [CrossRef]
- Robson, A.; Sturman, J.; Williamson, P.; Conboy, P.; Penney, S.; Wood, H. Pre-treatment clinical assessment in head and neck cancer: United Kingdom National Multidisciplinary Guidelines. J. Laryngol. Otol. 2016, 130, S13–S22. [Google Scholar] [CrossRef]
- Raskob, G.E.; van Es, N.; Verhamme, P.; Carrier, M.; Di Nisio, M.; Garcia, D.; Grosso, M.A.; Kakkar, A.K.; Michael, J.; Kovacs, B.S.; et al. Edoxaban for the treatment of cancer-associated venous thromboembolism. N. Engl. J. Med. 2018, 378, 615–624. [Google Scholar] [CrossRef]
- Young, A.M.; Marshall, A.; Thirlwall, J.; Chapman, O.; Lokare, A.; Hill, C.; Hale, D.; Dunn, J.A.; Lyman, G.H.; Hutchinson, C.; et al. Comparison of an Oral Factor Xa Inhibitor with Low Molecular Weight Heparin in Patients with Cancer with Venous Thromboembolism: Results of a Randomized Trial (SELECT-D). J. Clin. Oncol. 2018, 36, 2017–2023. [Google Scholar] [CrossRef]
- McBane, R.D.; Wysokinski, W.E.; Le-Rademacher, J.G.; Zemla, T.; Ashrani, A.; Tafur, A.; Perepu, U.; Anderson, D.; Gundabolu, K.; Kuzma, C.; et al. Apixaban and dalteparin in active malignancy—Associated venous thromboembolism: The ADAM VTE trial. J. Thromb. Haemost. 2019, 18, 411–421. [Google Scholar] [CrossRef]
- Agnelli, G.; Becattini, C.; Bauersachs, R.; Brenner, B.; Campanini, M.; Cohen, A.; Connors, J.M.; Fontanella, A.; Gussoni, G.; Huisman, M.V.; et al. Apixaban versus Dalteparin for the Treatment of Acute Venous Thromboembolism in Patients with Cancer: The Caravaggio Study. Thromb. Haemost. 2018, 118, 1668–1678. [Google Scholar] [CrossRef]
- Khorana, A.A.; Noble, S.; Lee, A.Y.Y.; Soff, G.; Meyer, G.; O’Connell, C.; Carrier, M. Role of direct oral anticoagulants in the treatment of cancer-associated venous thromboembolism: Guidance from the SSC of the ISTH. J. Thromb. Haemost. 2018, 16, 1891–1894. [Google Scholar] [CrossRef] [PubMed]
- Farge, D.; Frere, C.; Connors, J.M.; Ay, C.; Khorana, A.A.; Munoz, A.; Brenner, B.; Kakkar, A.; Rafii, H.; Solymoss, S.; et al. 2019 international clinical practice guidelines for the treatment and prophylaxis of venous thromboembolism in patients with cancer. Lancet Oncol. 2019, 20, e566–e581. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Risk Factor | Points |
|---|---|
| Site of primary tumour | |
| Very high risk (stomach, pancreas) | 2 |
| High risk (lung, lymphoma, gynaecologic, bladder, testicular) | 1 |
| All other sites | 0 |
| Pre-chemotherapy platelet count ≥ 350,000/microL | 1 |
| Haemoglobin level < 10 g/dL or use of ESAs | 1 |
| Pre-chemotherapy WBC > 11,000/microL | 1 |
| BMI ≥ 35 kg/m2 | 1 |
| Agent | VTE | ATE | |
|---|---|---|---|
| Platinum-based agents | Cisplatin | ++ | − |
| Carboplatin | ++ | − | |
| Oxaliplatin | + | − | |
| Anthracyclines | Doxorubicin | + | NR |
| Daunorubicin | NR | NR | |
| Epirubicin | NR | NR | |
| Pyrimidine antagonists | 5-fluorouracil | − | − |
| Gemcitabine | − | − | |
| L-asparaginase | NR | NR | |
| Tamoxifen | + | + | |
| Immunomodulatory agents | Thalidomide | ++ | NR |
| Lenalidomide | ++ | NR | |
| Pomalidomide | + | NR | |
| Anti-EGFR antibodies | Cetuximab | + | − |
| Panitumumab | + | − | |
| Necitumumab | + | − | |
| VEGF-targeted molecules | Bevacizumab | − | ++ |
| Aflibercept | − | NR | |
| VEGFR RTKI | Sunitinib | − | ++ |
| Sorafenib | − | ++ | |
| Axitinib | − | ++ | |
| Pazopanib | − | + | |
| Vandetanib | − | + | |
| Lenvatinib | NR | NR | |
| Cabozantinib | NR | NR | |
| BCR-ABL RTKI | Imatinib | − | − |
| Dasatinib | ++ | ++ | |
| Nilotinib | ++ | ++ | |
| Ponatinib | ++ | ++ | |
| Bosutinib | NR | NR | |
| CDK inhibitors | Palbociclib | + | NR |
| Abemaciclib | ++ | NR | |
| Ribociclib | + | NR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Gennaro, L.; De Cristofaro, R.; Ferretti, A.; Basso, M.; Riccio, C.; Cordaro, M.; Lajolo, C. Oral Squamous Cell Carcinoma-Associated Thrombosis: What Evidence? Cancers 2022, 14, 5616. https://doi.org/10.3390/cancers14225616
Di Gennaro L, De Cristofaro R, Ferretti A, Basso M, Riccio C, Cordaro M, Lajolo C. Oral Squamous Cell Carcinoma-Associated Thrombosis: What Evidence? Cancers. 2022; 14(22):5616. https://doi.org/10.3390/cancers14225616
Chicago/Turabian StyleDi Gennaro, Leonardo, Raimondo De Cristofaro, Antonietta Ferretti, Maria Basso, Claudia Riccio, Massimo Cordaro, and Carlo Lajolo. 2022. "Oral Squamous Cell Carcinoma-Associated Thrombosis: What Evidence?" Cancers 14, no. 22: 5616. https://doi.org/10.3390/cancers14225616
APA StyleDi Gennaro, L., De Cristofaro, R., Ferretti, A., Basso, M., Riccio, C., Cordaro, M., & Lajolo, C. (2022). Oral Squamous Cell Carcinoma-Associated Thrombosis: What Evidence? Cancers, 14(22), 5616. https://doi.org/10.3390/cancers14225616