
A Risk Model for Patients with PSA-Only Recurrence (Biochemical Recurrence) Based on PSA and PSMA PET/CT: An Individual Patient Data Meta-Analysis

 , , , , and
, , , , and
Abstract
Simple Summary
Abstract
1. Introduction
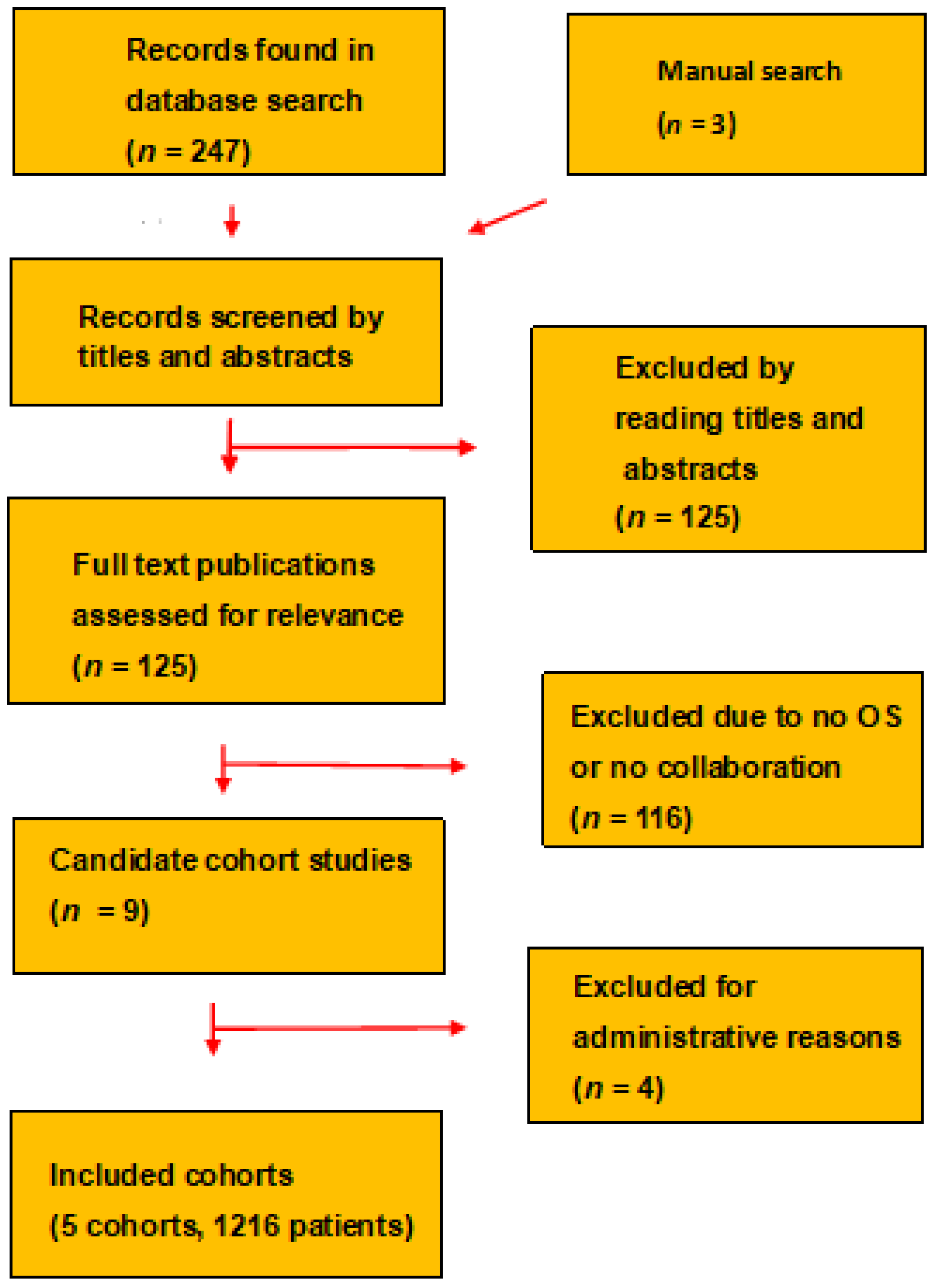
2. Evidence Acquisition
2.1. Selection of Patient Cohorts and Synthesis of Clinical Data
2.2. PSA
2.3. PSMA PET/CT
2.4. Definitions
2.5. Statistical Analysis
3. Results
3.1. Patients
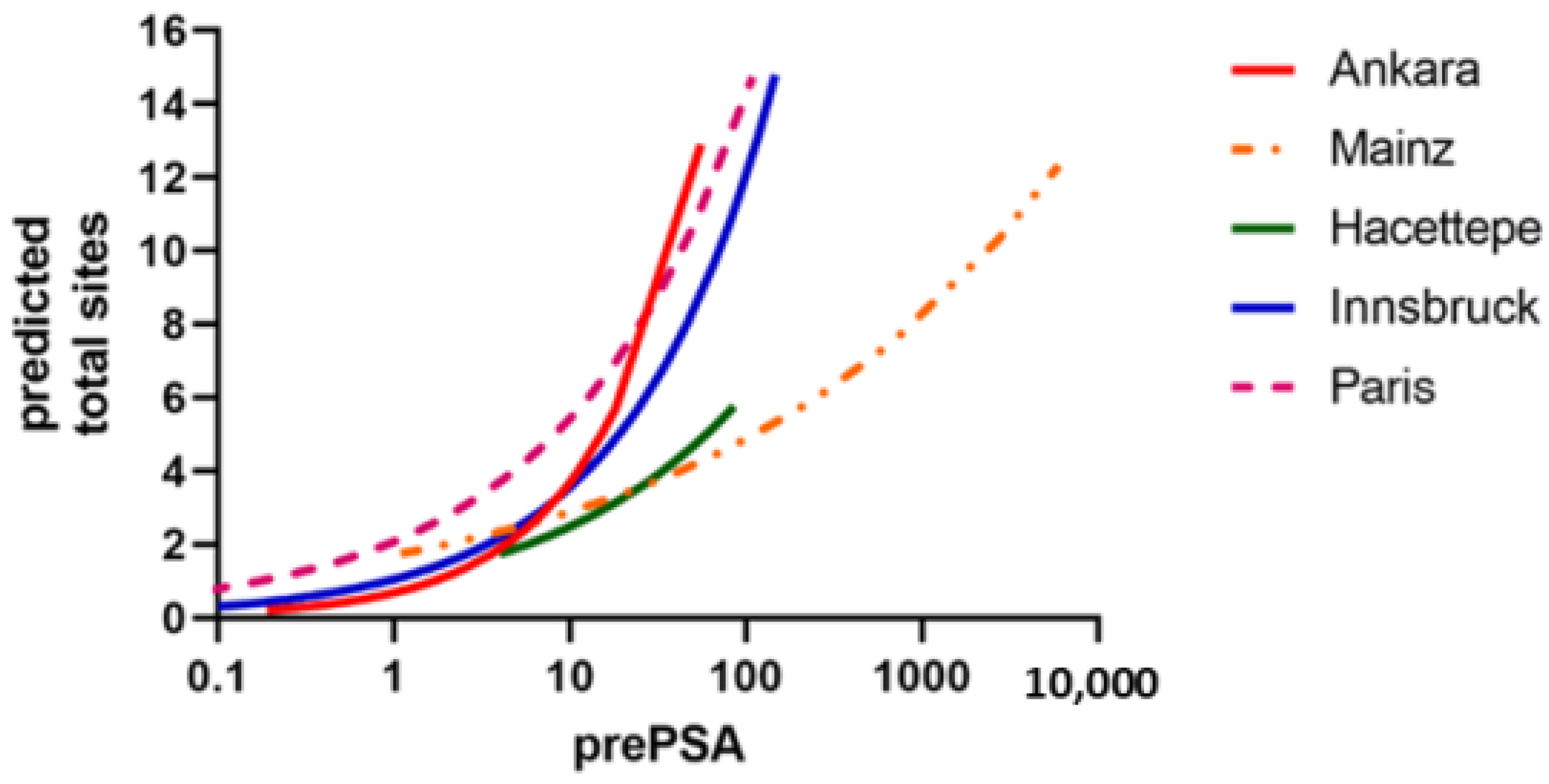
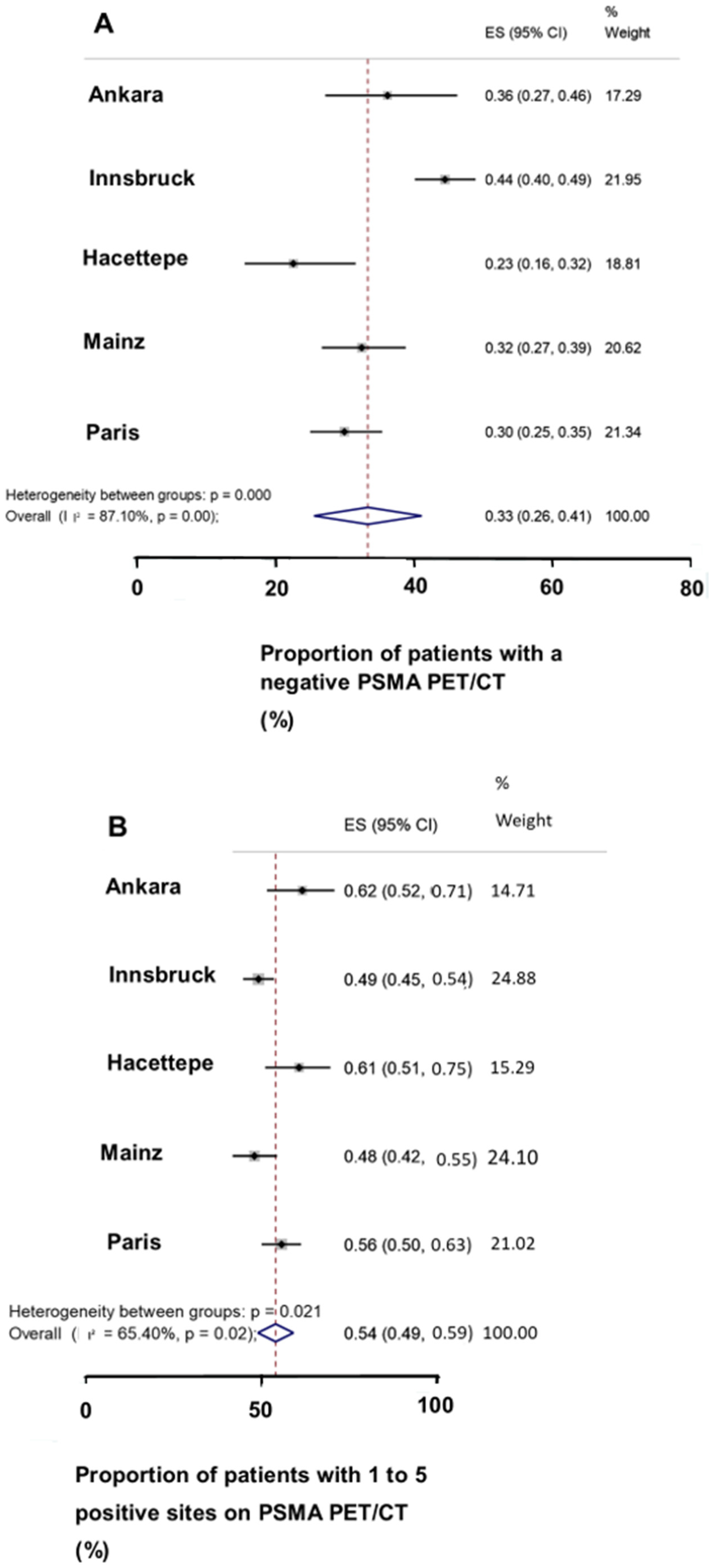
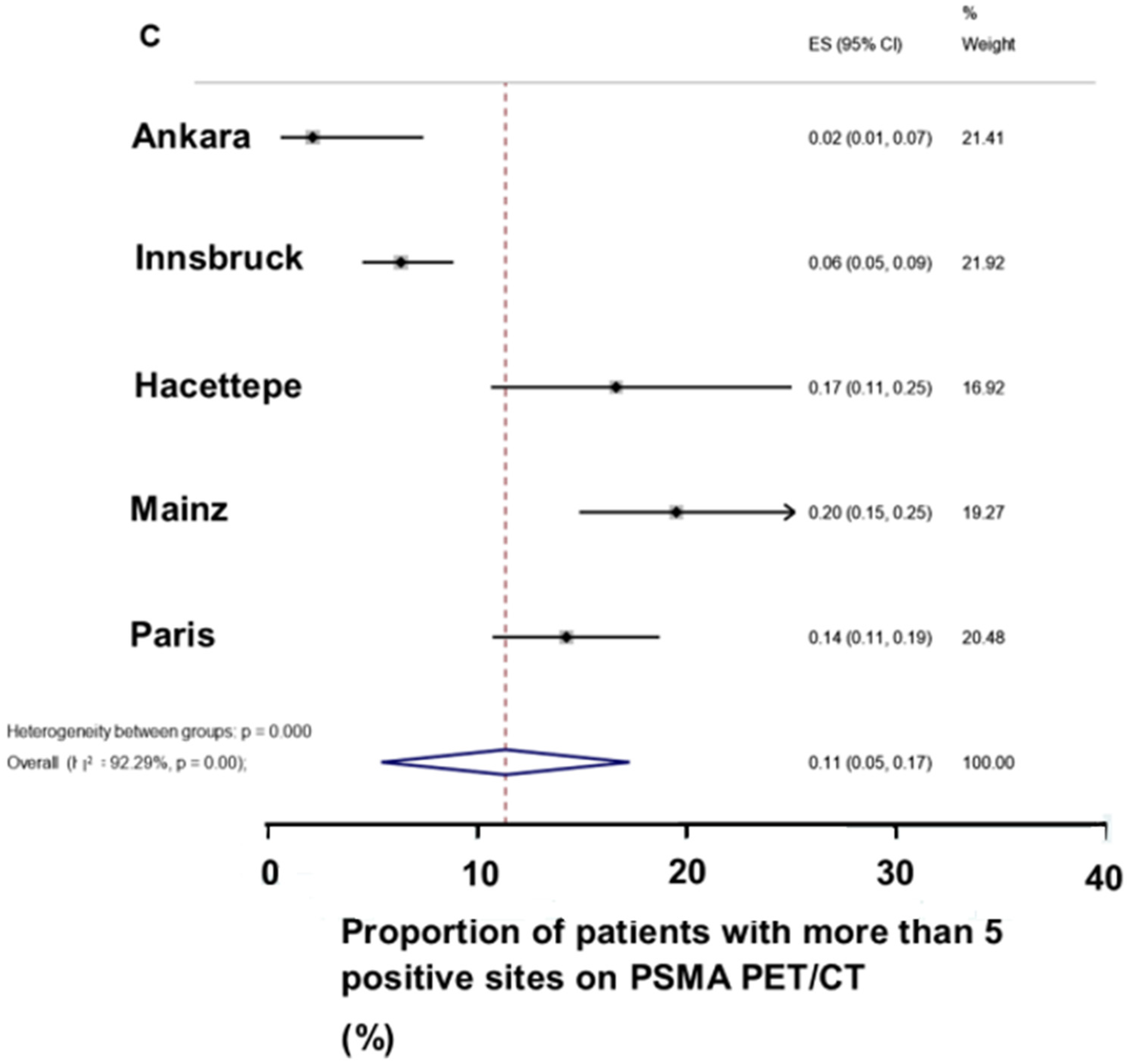
3.2. PSA and PSMA PET/CT
3.3. Cohorts and Restaging PSMA PET/CT
3.4. Treatment after the Restaging PSMA PET/CT
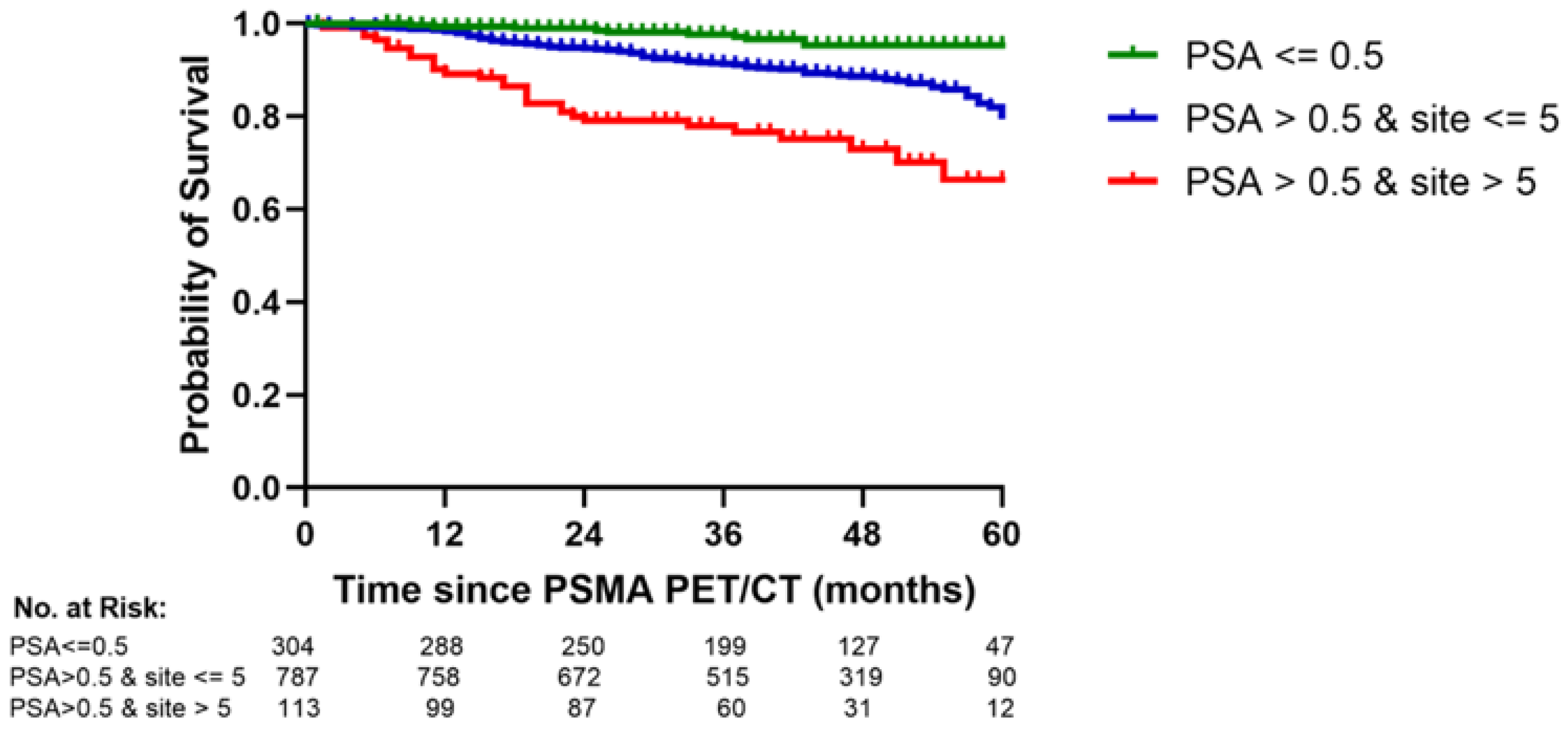
3.5. Restaging PSMA PET/CT and OS
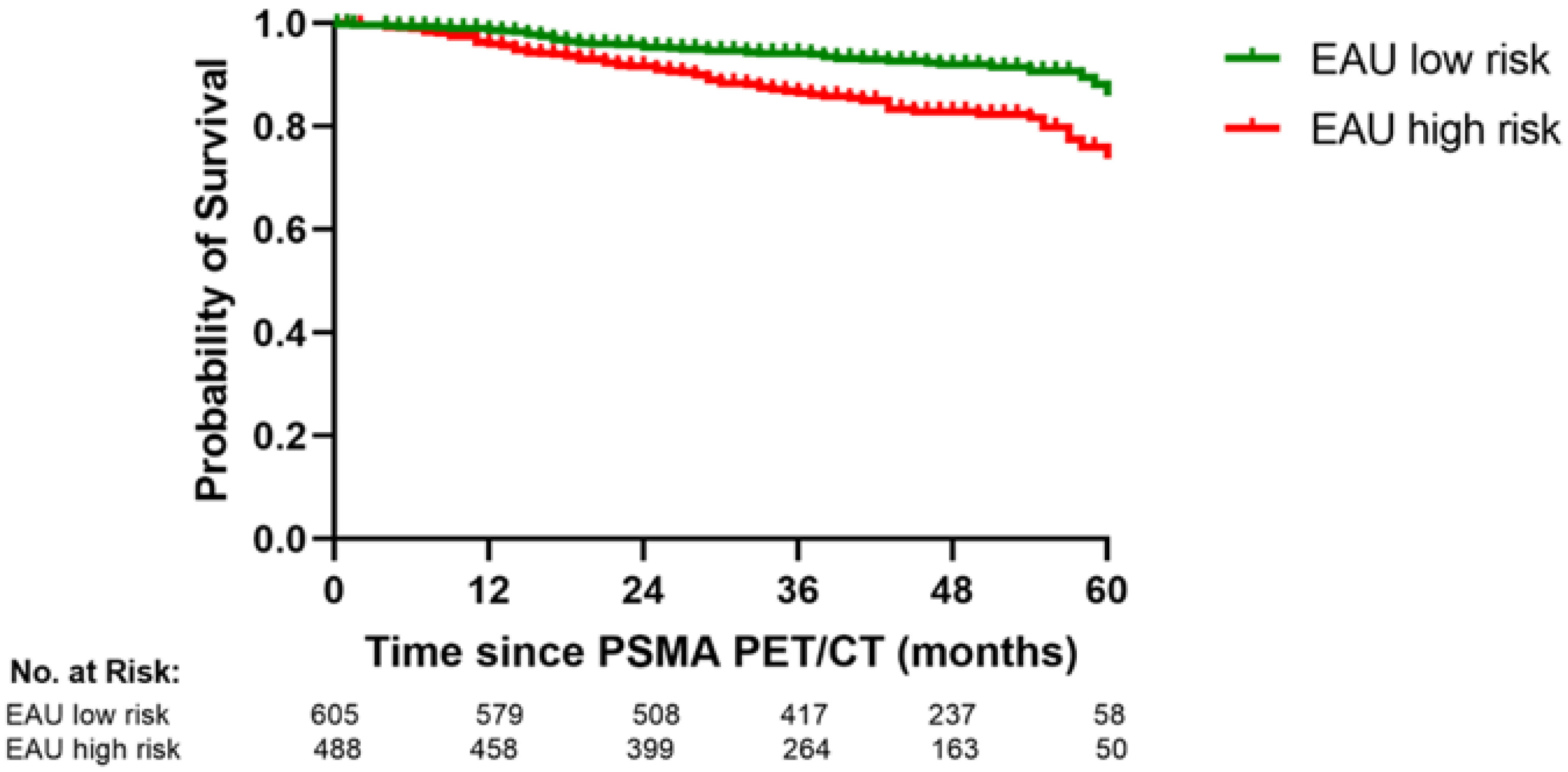
3.6. The PSA/PSMA PET Risk Model and the EAU BCR Risk Classsification
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Cornford, P.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-ISUP-SIOG guidelines on prostate cancer. Part II-2020 Update. Eur. Urol. 2021, 79, 263–282. [Google Scholar] [CrossRef] [PubMed]
- Broeck, T.V.D.; Bergh, R.C.V.D.; Arfi, N.; Gross, T.; Moris, L.; Briers, E.; Cumberbatch, M.; De Santis, M.; Tilki, D.; Fanti, S.; et al. Prognostic Value of Biochemical Recurrence Following Treatment with Curative Intent for Prostate Cancer: A Systematic Review. Eur. Urol. 2018, 75, 967–987. [Google Scholar] [CrossRef] [PubMed]
- von Eyben, F.E.; Soydal, C.; von Eyben, R. 68Ga-PSMA PET/CT for patients with PSA relapse after radical prostatectomy or external beam radiotherapy. Diagnostics 2021, 11, 622. [Google Scholar] [CrossRef]
- von Eyben, R.; Hoffmann, M.A.; Kapp, D.S.; Soydal, C.; Uprimny, C.; Virgolini, I.; Tuncel, M.; Gauthe, M.; von Eyben, F.E. Quality goals for salvage treatment of patients with prostate cancer at PSA relapse. Eur. Urol. Oncol. 2022, 13, e3492. [Google Scholar] [CrossRef]
- Akdemir, E.N.; Tuncel, M.; Akyol, F.; Bilen, C.Y.; Baydar, D.E.; Karabulut, E.; Ozen, H.; Caglar, M. 68Ga-labelled PSMA ligand HBED-CC PET/CT imaging in patients with recurrent prostate cancer. World J. Urol. 2018, 37, 813–821. [Google Scholar] [CrossRef]
- Uprimny, C.; Bayerschmidt, S.; Kroiss, A.S.; Fritz, J.; Nilica, B.; Svirydenka, A.; Decristoforo, C.; Di Santo, G.; von Guggenberg, E.; Horninger, W.; et al. Impact of forced diuresis with furosemide and hydration on the halo artefact and intensity of tracer accumulation in the urinary bladder and kidneys on [68Ga]Ga-PSMA-11-PET/CT in the evaluation of prostate cancer patients. Eur. J. Nusl. Med. Mol. Imaging 2021, 48, 123–133. [Google Scholar] [CrossRef]
- Uprimny, C.; Bayerschmidt, S.; Kroiss, A.S.; Fritz, J.; Nilica, B.; Svirydenka, H.; Decristoforo, C.; von Guggenberg, E.; Horninger, W.; Virgolini, I.J. Early Injection of Furosemide Increases Detection Rate of Local Recurrence in Prostate Cancer Patients with Biochemical Recurrence Referred for 68Ga-PSMA-11 PET/CT. J. Nucl. Med. 2021, 62, 1550–1557. [Google Scholar] [CrossRef]
- Hoffmann, M.A.; Buchholz, H.-G.; Wieler, H.J.; Miederer, M.; Rosar, F.; Fischer, N.; Müller-Hübenthal, J.; Trampert, L.; Pektor, S.; Schreckenberger, M. PSA and PSA Kinetics Thresholds for the Presence of 68Ga-PSMA-11 PET/CT-Detectable Lesions in Patients with Biochemical Recurrent Prostate Cancer. Cancers 2020, 12, 398. [Google Scholar] [CrossRef]
- Fourquet, A.; Lahmi, L.; Rusu, T.; Belkacemi, Y.; Créhange, G.; de la Taille, A.; Fournier, G.; Cussenot, O.; Gauthé, M. Restaging the Biochemical Recurrence of Prostate Cancer with [68Ga]Ga-PSMA-11 PET/CT: Diagnostic Performance and Impact on Patient Disease Management. Cancers 2021, 13, 1594. [Google Scholar] [CrossRef]
- Fendler, W.P.; Eiber, M.; Beheshti, M.; Bomanji, J.; Ceci, F.; Cho, S.; Giesel, F.; Haberkorn, U.; Hope, T.A.; Kopka, K.; et al. 68Ga-PSMA PET/CT: Joint EANM and SNMMI procedure guideline for prostate cancer imaging: Version 1.0. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1014–1024. [Google Scholar] [CrossRef] [PubMed]
- Ceci, F.; Oprea-Lager, D.E.; Emmett, L.; Adam, J.A.; Bomanji, J.; Czernin, J.; Eiber, M.; Haberkorn, U.; Hofman, M.S.; Hope, T.A.; et al. E-PSMA: The EANM standardized reporting guidelines v1.0 for PSMA-PET. Eur. J. Pediatr. 2021, 48, 1626–1638. [Google Scholar] [CrossRef]
- Eiber, M.; Herrmann, K.; Calais, J.; Hadaschik, B.; Giesel, F.L.; Hartenbach, M.; Hope, T.A.; Reiter, R.; Maurer, T.; Weber, W.A.; et al. Prostate Cancer Molecular Imaging Standardized Evaluation (PROMISE): Proposed miTNM Classification for the Interpretation of PSMA-Ligand PET/CT. J. Nucl. Med. 2018, 59, 469–478. [Google Scholar] [CrossRef] [PubMed]
- von Eyben, F.E. Ga-PSMA PET/CT for Patients with Prostate Cancer with PSA Relapse. In The Evolution of Radionanotargeting towards Clinical Precision Oncology: A Festschrift in Honor of Kalevi Kairemo; Jekunen, A., Ed.; Bentham Science Publishers: Sharjah, United Arab Emirates, 2022; pp. 164–178. ISBN 978-1-68108-866-2. eISBN 978-1-6808-865-5. [Google Scholar]
- Abdel-Rahman, O. Assessment of the prognostic value of the 8th AJCC staging system for patients with clinically staged prostate cancer, A time to sub-classify stage IV? PLoS ONE 2017, 12, e0188450. [Google Scholar] [CrossRef]
- Raveenthiran, S.; Yaxley, J.; Gianduzzo, T.; Kua, B.; McEwan, L.; Wong, D.; Tsang, G.; MacKean, J. The use of 68Ga-PET/CT PSMA to determine patterns of disease for biochemically recurrent prostate cancer following primary radiotherapy. Prostate Cancer Prostatic Dis. 2019, 22, 385–390. [Google Scholar] [CrossRef]
- Roach, M., III; Hanks, G.; Thames, H., Jr.; Schellhammer, P.; Shipley, W.U.; Sokol, G.H.; Sandler, H. Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: Recommendations of the RTOG-ASTRO Phoenix consensusc conference. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 965–974. [Google Scholar] [CrossRef] [PubMed]
- Abghari-Gerst, M.; Armstrong, W.R.; Nguyen, K.; Calais, J.; Czernin, J.; Lin, D.; Jariwala, N.; Rodnick, M.; Hope, T.A.; Hearn, J.; et al. A Comprehensive Assessment of 68Ga-PSMA-11 PET in Biochemically Recurrent Prostate Cancer: Results from a Prospective Multicenter Study on 2,005 Patients. J. Nucl. Med. 2021, 63, 567–572. [Google Scholar] [CrossRef]
- Metser, U.; Zukotynski, K.; Mak, V.; Langer, D.; MacCrostie, P.; Finelli, A.; Kapoor, A.; Chin, J.; Lavallee, L.; Klotz, L.H.; et al. Effect of (18)F-DCFPyL PET/CT on the management of patients with recurrent prostate cancer: Results of a prospective multicenter registry trial. Radiology 2022, 303, 414–420. [Google Scholar] [CrossRef]
- Afshar-Oromieh, A.; da Cunha, M.L.; Wagner, J.; Haberkorn, U.; Debus, N.; Weber, W.; Eiber, M.; Holland-Letz, T.; Rauscher, I. Performance of [68Ga]Ga-PSMA-11 PET/CT in patients with recurrent prostate cancer after prostatectomy—A multi-centre evaluation of 2533 patients. Eur. J. Nucl. Med. Mol. Imaging 2021, 8, 2925–2934. [Google Scholar] [CrossRef]
- Artigas, C.; Diamand, R.; Shagera, Q.A.; Plouznikoff, N.; Fokoue, F.; Otte, F.-X.; Gil, T.; Peltier, A.; Van Gestel, D.; Flamen, P. Oligometastatic Disease Detection with 68Ga-PSMA-11 PET/CT in Hormone-Sensitive Prostate Cancer Patients (HSPC) with Biochemical Recurrence after Radical Prostatectomy: Predictive Factors and Clinical Impact. Cancers 2021, 13, 4982. [Google Scholar] [CrossRef]
- Zamboglou, C.; Strouthos, I.; Sahlmann, J.; Farolfi, A.; Serani, F.; Medici, F.; Cavallini, L.; Morganti, A.G.; Trapp, C.; Koerber, S.A.; et al. Metastasis-free survival and patterns of distant metastatic disease after PSMA-PET-guided salvage radiotherapy in recurrent or persistent prostate cancer after prostatectomy. Int. J. Radiat. Oncol. Biol. Phys. 2022, 113, 1015–1024. [Google Scholar] [CrossRef] [PubMed]
- Ceci, F.; Rovera, G.; Iorio, G.C.; Guarneri, A.; Chiofalo, V.; Passera, R.; Oderda, M.; Dall’Armellina, S.; Liberini, V.; Grimaldi, S.; et al. Event-free survival after 68 Ga-PSMA-11 PET/CT in recurrent hormone-sensitive prostate cancer (HSPC) patients eligible for salvage therapy. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 3257–3268. [Google Scholar] [CrossRef] [PubMed]
- Wenzel, M.; Hussein, R.; Maurer, T.; Karakiewicz, P.I.; Tilki, D.; Graefen, M.; Würnschimmel, C. PSMA PET predicts metastasis-free survival in the setting of salvage radiotherapy after radical prostatectomy. Urol. Oncol. Semin. Orig. Investig. 2021, 40, 7.e1–7.e8. [Google Scholar] [CrossRef]
- Kirste, S.; Kroeze, S.G.C.; Henkenberens, C.; Schmidt-Hegemann, N.S.; Vogel, M.M.E.; Becker, J.; Zamboglou, C.; Burger, I.; Derlin, T.; Bartenstein, P.; et al. Combining (68)Ga-PSMA-PET/CT-directed and elective radiation therapy improves outcome in oligorecurrent prostate cancer: A retrospective multicenter study. Front. Oncol. 2021, 11, 640467. [Google Scholar] [CrossRef]
- Emmett, L.; Buteau, J.; Papa, N.; Moon, D.; Thompson, J.; Roberts, M.J.; Rasiah, K.; Pattison, D.A.; Yaxley, J.; Thomas, P.; et al. The additive diagnostic value of prostate-specific membrane antigen positron emission tomography computed tomography to multiparametric magnetic resonance imaging triage in the diagnosis of prostate cancer (PRIMARY): A prospective multicentre study. Eur. Urol. 2021, 80, 682–689. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.A.; von Eyben, F.E.; Fischer, N.; Rosar, F.; Muller-Hubenthal, J.; Buchholz, H.G.; Wieler, H.J.; Schreckenberger, M. Comparison of [(18)F]PSMA-1007 with [(68)Ga]Ga-PSMA-11 PET/CT in restaging of prostate cancer patients with PSA relapse. Cancers 2022, 14, 1479. [Google Scholar] [CrossRef]
- Staal, F.H.E.; Janssen, J.; Brouwer, C.L.; Langendijk, J.A.; Siang, K.N.W.; Schuit, E.; de Jong, I.J.; Verzijlbergen, J.F.; Smeenk, R.J.; Aluwini, S. Phase III randomised controlled trial on PSMA PET/CT guided hypofractionated salvage prostate bed radiotherapy of biochemical failure after radical prostatectomy for prostate cancer (PERYTON-trial): Study protocol. BMC Cancer 2022, 22, 416. [Google Scholar] [CrossRef]
- Janssen, J.; Staal, F.H.E.; Brouwer, C.L.; Langendijk, J.A.; de Jong, I.J.; van Moorselaar, R.J.A.; Schuit, E.; Verzijlbergen, J.F.; Smeenk, R.J.; Aluwini, S. Androgen Deprivation therapy for Oligo-recurrent Prostate cancer in addition to radioTherapy (ADOPT): Study protocol for a randomised phase III trial. BMC Cancer 2022, 22, 482. [Google Scholar] [CrossRef]
- Meijer, D.; Eppinga, W.S.; Mohede, R.M.; Vanneste, B.G.; Meijnen, P.; Meijer, O.W.; Daniels, L.A.; Bergh, R.C.V.D.; Lont, A.P.; Ettema, R.H.; et al. Prostate-specific Membrane Antigen Positron Emission Tomography/Computed Tomography Is Associated with Improved Oncological Outcome in Men Treated with Salvage Radiation Therapy for Biochemically Recurrent Prostate Cancer. Eur. Urol. Oncol. 2022, 5, 146–152. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Results | |
|---|---|---|
| (Median, IQR, percentage) | Whole range | |
| Age, yrs | 68 (62, 73) | 41–88 |
| Unknown | 118 (10%) | |
| Time to relapse, months | 58 (25, 105) | 1–292 |
| Unknown | 103 (8%) | |
| ISUP | ||
| 1 | 123 (10%) | |
| 2 | 356 (29%) | |
| 3 | 253 (21%) | |
| 4 | 158 (13%) | |
| 5 | 245 (20%) | |
| Unknown | 81 (7%) | |
| T stage | ||
| 1 | 35 (3%) | |
| 2 | 389 (32%) | |
| 3 | 567 (47%) | |
| Unknown | 225 (19%) | |
| Initial treatment | ||
| RP only | 754 (62%) | |
| RP and RT | 145 (12%) | |
| RT only | 304 (25%) | |
| Unknown | 13 (1%) | |
| Unknown | 44 (4%) | |
| EAU BCR risk score | ||
| Low risk | 501 (41%) | |
| High risk | 474 (39%) | |
| Unknown | 241 (20%) | |
| Follow up time, months | 42 (29, 53) | 0.2–86 |
| Prescan PSA (ng/mL) | 1.4 (0.2, 3.4) | 0.1–308.2 |
| Prescan PSA ≤ 0.5 ng/mL | 285 | |
| Prescan PSA > 0.5 ng/mL | 900 | |
| Unknown | 31 |
| Variable | Results (Median, IQR, Percentage) |
|---|---|
| Total number of regional sites, count | 1 (0, 2) |
| Regional location of positive sites | |
| No positive sites | 369 (30%) |
| Local sites | 187 (15%) |
| Regional sites | 290 (24%) |
| Distant sites | 357 (29%) |
| Unknown | 13 (1%) |
| EAU BCR risk score | |
| Insignificant risk | 501 (41%) |
| High risk | 474 (39%) |
| Unknown | 241 (20%) |
| Groupings by no of sites on PSMA PET/CT | |
| No site | 369 (30%) |
| Oligosites | 711 (58%) |
| Polysites | 123 (10%) |
| Unknown | 13 (1%) |
| Predictor | HR | 95% CI | p-Value for the HR | Overall p-Value | |
|---|---|---|---|---|---|
| Age (years) | 1 | 0.98 | 1.03 | 0.8263 | |
| Time to relapse (months) | 0.99 | 0.97 | 0.997 | 0.0129 | |
| ISUP | 0.0146 | ||||
| 1 (reference) | |||||
| 2 | 1 | 0.5 | 2 | 0.9695 | |
| 3 | 1.2 | 0.6 | 2.6 | 0.6272 | |
| 4 | 1.6 | 0.8 | 3.4 | 0.2028 | |
| 5 | 2.1 | 1.1 | 4.2 | 0.0347 | |
| T stage (1/2 vs. 3) | 1.31 | 0.86 | 1.99 | 0.2162 | |
| Initial treatment | 0.4739 | ||||
| RP only (reference) | |||||
| RP and RT | 1.28 | 0.76 | 2.15 | 0.3541 | |
| RT only | 1.26 | 0.82 | 1.93 | 0.2994 | |
| Total sites | 1.12 | 1.09 | 1.15 | <0.0001 | |
| Prescan PSA ≤ 0.5 ng/mL (reference) | |||||
| Prescan PSA > 0.5 ng/mL | 3.706 | 1.591 | 8.633 | 0.0024 | |
| Regional location of positive sites | <0.0001 | ||||
| No sites (reference) | |||||
| Oligosites | 2.8 | 1.7 | 4.6 | <0.0001 | |
| Polysites | 8.2 | 4.5 | 14.8 | <0.0001 | |
| No positive sites | |||||
| Local sites | 3.4 | 1.8 | 6.5 | <0.0001 | |
| Regional sites | 3.5 | 2 | 6.3 | <0.0001 | |
| Distant sites | 4.7 | 2.7 | 8.4 | <0.0001 | |
| EAU BCR risk score (low vs. high risk) | 1.42 | 0.99 | 2.06 | 0.0597 | |
| Groupings by no of sites on PSMA PET/CT | <0.0001 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
von Eyben, R.; Kapp, D.S.; Hoffmann, M.A.; Soydal, C.; Uprimny, C.; Virgolini, I.; Tuncel, M.; Gauthé, M.; von Eyben, F.E. A Risk Model for Patients with PSA-Only Recurrence (Biochemical Recurrence) Based on PSA and PSMA PET/CT: An Individual Patient Data Meta-Analysis. Cancers 2022, 14, 5461. https://doi.org/10.3390/cancers14215461
von Eyben R, Kapp DS, Hoffmann MA, Soydal C, Uprimny C, Virgolini I, Tuncel M, Gauthé M, von Eyben FE. A Risk Model for Patients with PSA-Only Recurrence (Biochemical Recurrence) Based on PSA and PSMA PET/CT: An Individual Patient Data Meta-Analysis. Cancers. 2022; 14(21):5461. https://doi.org/10.3390/cancers14215461
Chicago/Turabian Stylevon Eyben, Rie, Daniel S. Kapp, Manuela Andrea Hoffmann, Cigdem Soydal, Christian Uprimny, Irene Virgolini, Murat Tuncel, Mathieu Gauthé, and Finn E. von Eyben. 2022. "A Risk Model for Patients with PSA-Only Recurrence (Biochemical Recurrence) Based on PSA and PSMA PET/CT: An Individual Patient Data Meta-Analysis" Cancers 14, no. 21: 5461. https://doi.org/10.3390/cancers14215461
APA Stylevon Eyben, R., Kapp, D. S., Hoffmann, M. A., Soydal, C., Uprimny, C., Virgolini, I., Tuncel, M., Gauthé, M., & von Eyben, F. E. (2022). A Risk Model for Patients with PSA-Only Recurrence (Biochemical Recurrence) Based on PSA and PSMA PET/CT: An Individual Patient Data Meta-Analysis. Cancers, 14(21), 5461. https://doi.org/10.3390/cancers14215461