Utilization Trend and Comparison of Different Radiotherapy Modes for Patients with Early-Stage High-Intermediate-Risk Endometrial Cancer: A Real-World, Multi-Institutional Study

 ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
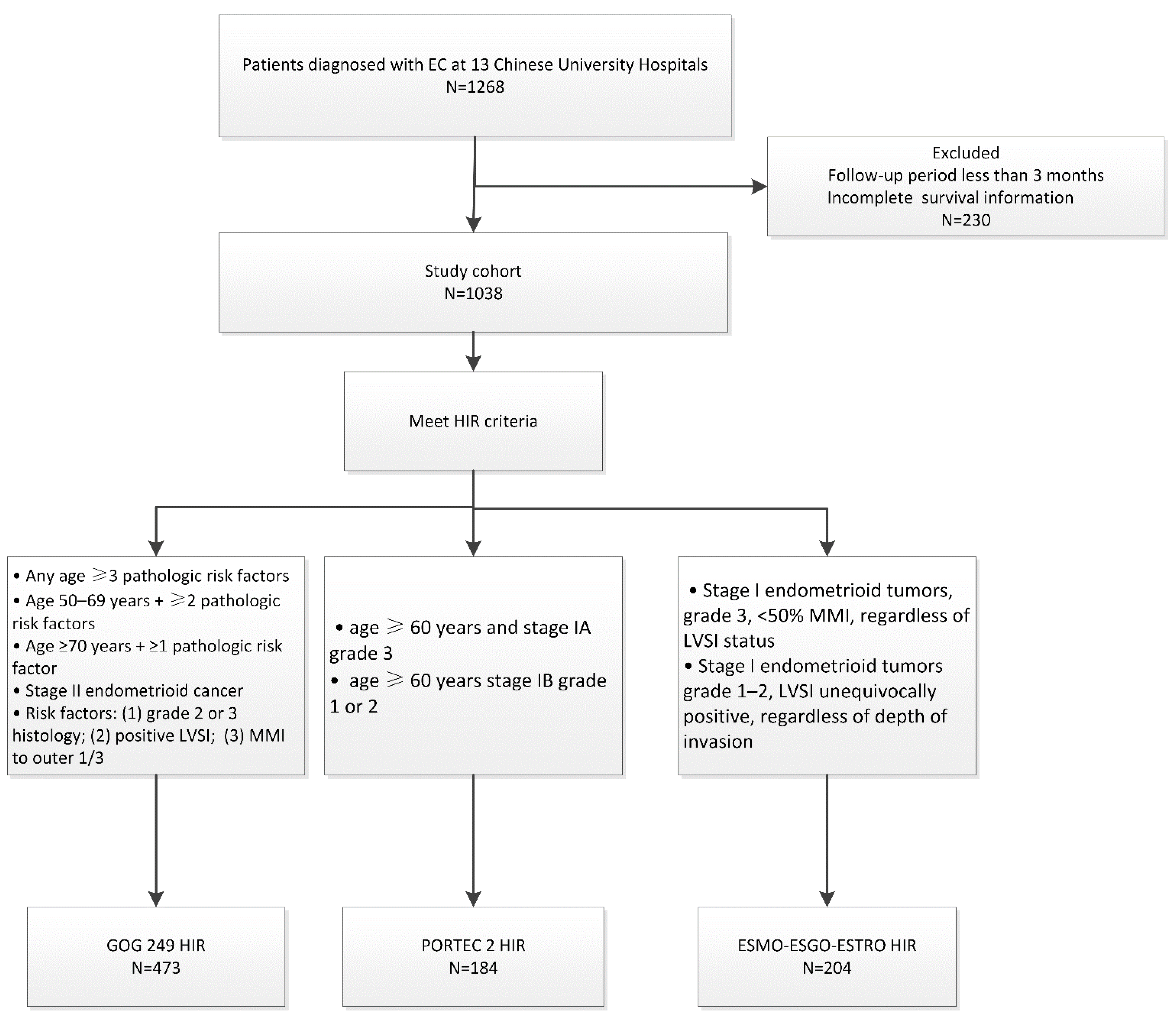
2.1. Patient Eligibility Criteria
2.2. Treatment
2.3. Data Analysis
3. Results
3.1. Patients
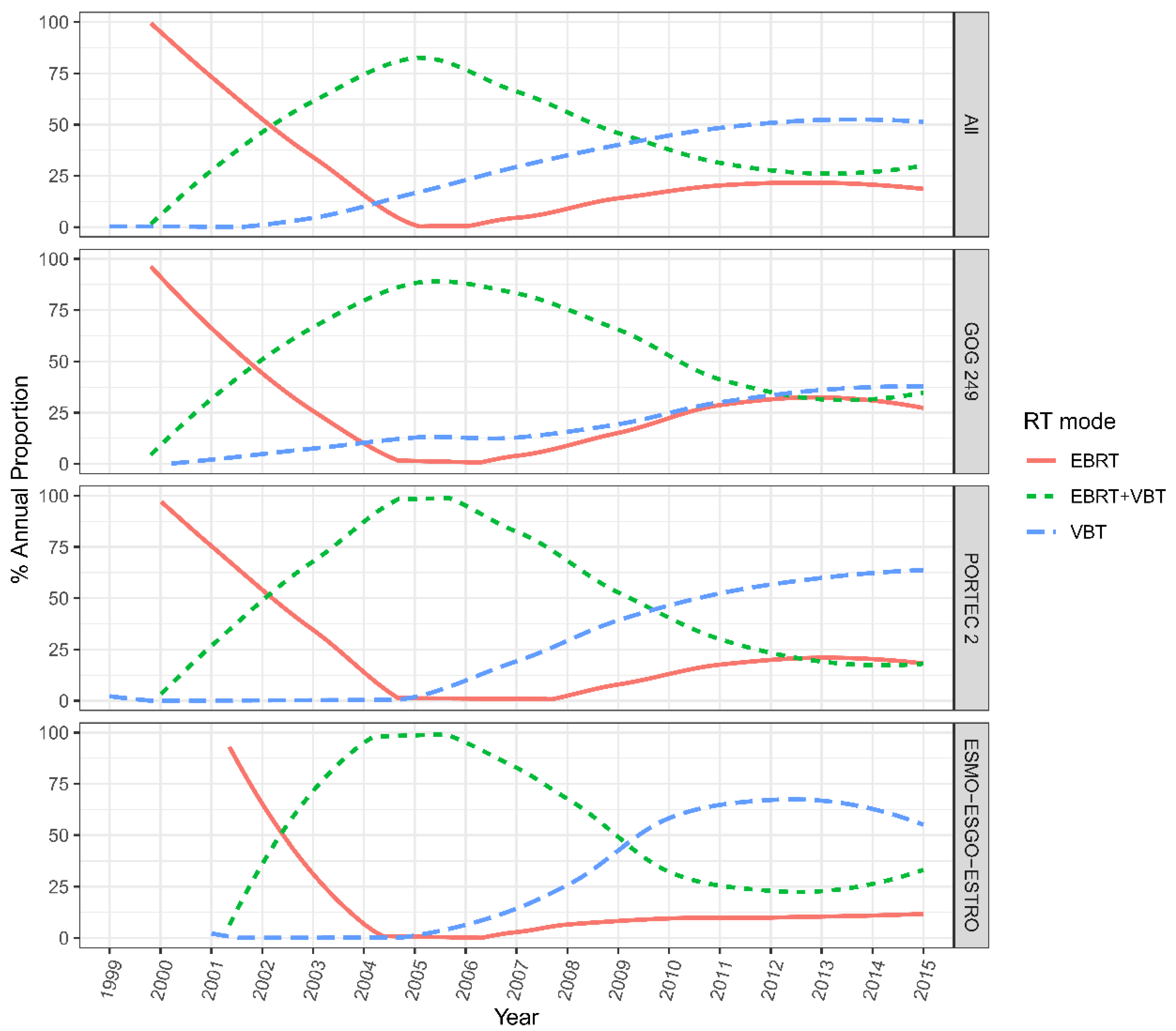
3.2. The Man-Kendall Trend Analysis
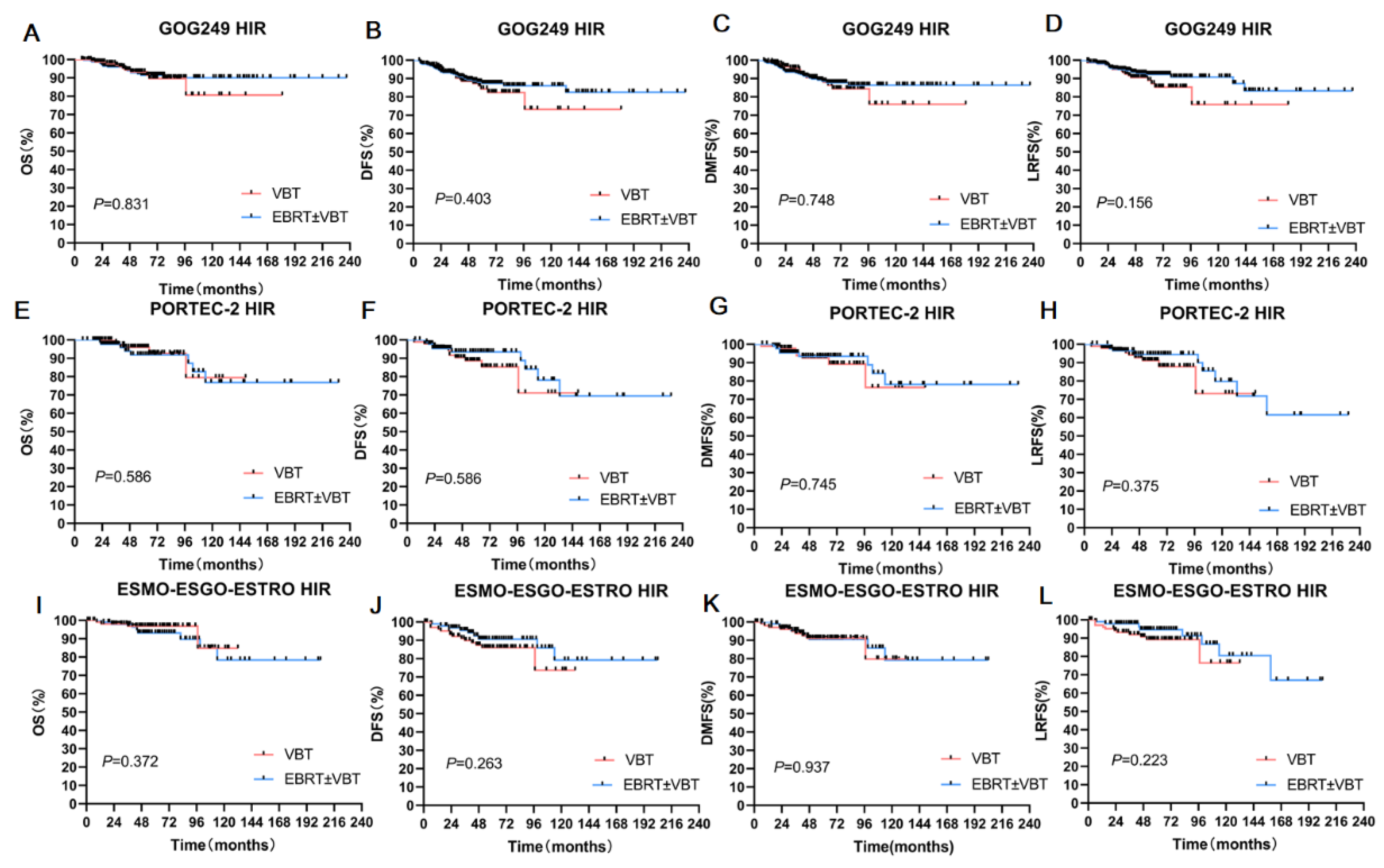
3.3. Survival Analyses in the Three Cohorts
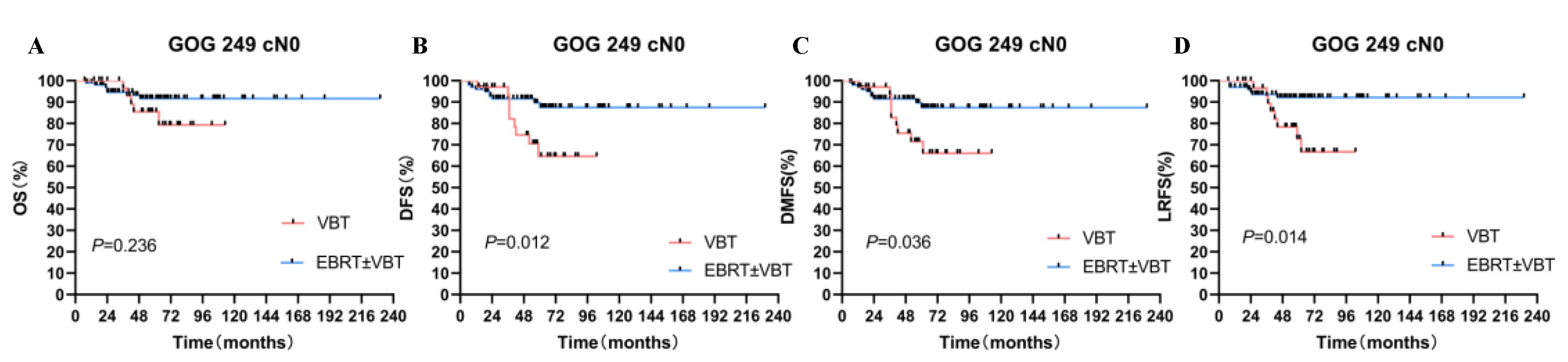
3.4. Subgroup Analyses in the GOG-249 HIR Cohort
3.5. Toxicities
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA A Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Cao, W.; Chen, H.-D.; Yu, Y.-W.; Li, N.; Chen, W.-Q. Changing profiles of cancer burden worldwide and in China: A secondary analysis of the global cancer statistics 2020. Chin. Med. J. 2021, 134, 783–791. [Google Scholar] [CrossRef] [PubMed]
- Baiden-Amissah, R.E.M.; Annibali, D.; Tuyaerts, S.; Amant, F. Endometrial Cancer Molecular Characterization: The Key to Identifying High-Risk Patients and Defining Guidelines for Clinical Decision-Making? Cancers 2021, 13, 3988. [Google Scholar] [CrossRef] [PubMed]
- Bendifallah, S.; Canlorbe, G.; Collinet, P.; Arsène, E.; Huguet, F.; Coutant, C.; Hudry, D.; Graesslin, O.; Raimond, E.; Touboul, C.; et al. Just how accurate are the major risk stratification systems for early-stage endometrial cancer? Br. J. Cancer 2015, 112, 793–801. [Google Scholar] [CrossRef]
- Colombo, N.; Creutzberg, C.; Amant, F.; Bosse, T.; González-Martín, A.; Ledermann, J.; Marth, C.; Nout, R.; Querleu, D.; Mirza, M.R.; et al. ESMO-ESGO-ESTRO Consensus Conference on Endometrial Cancer: Diagnosis, treatment and follow-up. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2016, 27, 16–41. [Google Scholar] [CrossRef]
- Eifel, P.J. High intermediate risk endometrial cancer. What is it? Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2019, 29, 1084–1085. [Google Scholar] [CrossRef]
- Creutzberg, C.L.; van Putten, W.L.; Koper, P.C.; Lybeert, M.L.; Jobsen, J.J.; Wárlám-Rodenhuis, C.C.; De Winter, K.A.; Lutgens, L.C.; van den Bergh, A.C.; van de Steen-Banasik, E.; et al. Surgery and postoperative radiotherapy versus surgery alone for patients with stage-1 endometrial carcinoma: Multicentre randomised trial. PORTEC Study Group. Post Operative Radiation Therapy in Endometrial Carcinoma. Lancet 2000, 355, 1404–1411. [Google Scholar] [CrossRef]
- Concin, N.; Matias-Guiu, X.; Vergote, I.; Cibula, D.; Mirza, M.R.; Marnitz, S.; Ledermann, J.; Bosse, T.; Chargari, C.; Fagotti, A.; et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2021, 31, 12–39. [Google Scholar] [CrossRef]
- Keys, H.M.; Roberts, J.A.; Brunetto, V.L.; Zaino, R.J.; Spirtos, N.M.; Bloss, J.D.; Pearlman, A.; Maiman, M.A.; Bell, J.G. A phase III trial of surgery with or without adjunctive external pelvic radiation therapy in intermediate risk endometrial adenocarcinoma: A Gynecologic Oncology Group study. Gynecol. Oncol. 2004, 92, 744–751. [Google Scholar] [CrossRef]
- Nout, R.A.; Smit, V.T.H.B.M.; Putter, H.; Jürgenliemk-Schulz, I.M.; Jobsen, J.J.; Lutgens, L.C.H.W.; van der Steen-Banasik, E.M.; Mens, J.W.M.; Slot, A.; Kroese, M.C.S.; et al. Vaginal brachytherapy versus pelvic external beam radiotherapy for patients with endometrial cancer of high-intermediate risk (PORTEC-2): An open-label, non-inferiority, randomised trial. Lancet 2010, 375, 816–823. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. Clinical Prace Guidelines in Oncology. Uterine Neoplasms, Version 1. Available online: https://jnccn.org/configurable/content/journals$002fjnccn$002f16$002f2$002farticle-p170.xml?t:ac=journals%24002fjnccn%24002f16%24002f2%24002farticle-p170.xml (accessed on 17 October 2022).
- Kong, A.; Johnson, N.; Kitchener, H.C.; Lawrie, T.A. Adjuvant radiotherapy for stage I endometrial cancer: An updated Cochrane systematic review and meta-analysis. J. Natl. Cancer Inst. 2012, 104, 1625–1634. [Google Scholar] [CrossRef] [PubMed]
- Chodavadia, P.A.; Jacobs, C.D.; Wang, F.; Havrilesky, L.J.; Chino, J.P.; Suneja, G. Off-study utilization of experimental therapies: Analysis of GOG249-eligible cohorts using real world data. Gynecol. Oncol. 2020, 156, 154–161. [Google Scholar] [CrossRef]
- Zakem, S.J.; Robin, T.P.; Smith, D.E.; Amini, A.; Stokes, W.A.; Lefkowits, C.; Fisher, C.M. Evolving trends in the management of high-intermediate risk endometrial cancer in the United States. Gynecol. Oncol. 2019, 152, 522–527. [Google Scholar] [CrossRef] [PubMed]
- Randall, M.E.; Filiaci, V.; McMeekin, D.S.; von Gruenigen, V.; Huang, H.; Yashar, C.M.; Mannel, R.S.; Kim, J.-W.; Salani, R.; DiSilvestro, P.A.; et al. Phase III Trial: Adjuvant Pelvic Radiation Therapy Versus Vaginal Brachytherapy Plus Paclitaxel/Carboplatin in High-Intermediate and High-Risk Early Stage Endometrial Cancer. J. Clin. Oncol. 2019, 37, 1810–1818. [Google Scholar] [CrossRef] [PubMed]
- Wortman, B.G.; Creutzberg, C.L.; Putter, H.; Jürgenliemk-Schulz, I.M.; Jobsen, J.J.; Lutgens, L.C.H.W.; van der Steen-Banasik, E.M.; Mens, J.W.M.; Slot, A.; Kroese, M.C.S.; et al. Ten-year results of the PORTEC-2 trial for high-intermediate risk endometrial carcinoma: Improving patient selection for adjuvant therapy. Br. J. Cancer 2018, 119, 1067–1074. [Google Scholar] [CrossRef] [PubMed]
- Eifel, P.J. The role of adjuvant radiation therapy for stage I endometrial cancer: Does meta-analysis reveal the answer? J. Natl. Cancer Inst. 2012, 104, 1615–1616. [Google Scholar] [CrossRef]
- Zavitsanos, P.J.; Leonard, K.L. Patterns of care in women with high-intermediate risk endometrioid adenocarcinoma in the PORTEC-2 era: A SEER database analysis. Brachytherapy 2017, 16, 109–115. [Google Scholar] [CrossRef]
- Wright, J.D.; Margolis, B.; Hou, J.Y.; Burke, W.M.; Tergas, A.I.; Huang, Y.; Hu, J.C.; Ananth, C.V.; Neugut, A.I.; Hershman, D.L. Overuse of external beam radiotherapy for stage I endometrial cancer. Am. J. Obstet. Gynecol. 2016, 215, 75–77. [Google Scholar] [CrossRef]
- Bottke, D.; Wiegel, T.; Kreienberg, R.; Kurzeder, C.; Sauer, G. Stage IB endometrial cancer. Does lymphadenectomy replace adjuvant radiotherapy? Strahlenther. Onkol. 2007, 183, 600–604. [Google Scholar] [CrossRef]
- Xiang, M.; Kidd, E.A. Survival benefit of radiation in high-risk, early-stage endometrioid carcinoma. J. Gynecol. Oncol. 2020, 31, e39. [Google Scholar] [CrossRef]
- Chen, J.L.-Y.; Huang, C.-Y.; Huang, Y.-S.; Hsu, C.-Y.; Lan, K.-H.; Shih, I.L.; Cheng, W.-F.; Chen, C.-A.; Sheu, B.-C.; Kuo, S.-H. Real-World Evaluation of Modern Adjuvant Radiotherapy in Women with Stage IB Endometrial Cancer. Cancers 2021, 13, 1386. [Google Scholar] [CrossRef] [PubMed]
- Kitchener, H.; Swart, A.M.C.; Qian, Q.; Amos, C.; Parmar, M.K.B. Efficacy of systematic pelvic lymphadenectomy in endometrial cancer (MRC ASTEC trial): A randomised study. Lancet 2009, 373, 125–136. [Google Scholar] [CrossRef] [PubMed]
- Chino, J.P.; Jones, E.; Berchuck, A.; Secord, A.A.; Havrilesky, L.J. The influence of radiation modality and lymph node dissection on survival in early-stage endometrial cancer. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 1872–1879. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.H.; Kim, H.S.; Kim, T.-J.; Chang, S.-J.; Kim, D.-Y.; Ryu, S.-Y.; Kim, B.-G.; Kim, Y.-T.; Bae, D.-S.; Ryu, H.-S.; et al. Survival impact based on the thoroughness of pelvic lymphadenectomy in intermediate- or high-risk groups of endometrioid-type endometrial cancer: A multi-center retrospective cohort analysis. Gynecol. Oncol. 2016, 141, 440–446. [Google Scholar] [CrossRef]
- Abu-Rustum, N.R.; Iasonos, A.; Zhou, Q.; Oke, E.; Soslow, R.A.; Alektiar, K.M.; Chi, D.S.; Barakat, R.R. Is there a therapeutic impact to regional lymphadenectomy in the surgical treatment of endometrial carcinoma? Am. J. Obstet. Gynecol. 2008, 198, 457.e1–457.e6. [Google Scholar] [CrossRef]
- Lutman, C.V.; Havrilesky, L.J.; Cragun, J.M.; Secord, A.A.; Calingaert, B.; Berchuck, A.; Clarke-Pearson, D.L.; Soper, J.T. Pelvic lymph node count is an important prognostic variable for FIGO stage I and II endometrial carcinoma with high-risk histology. Gynecol. Oncol. 2006, 102, 92–97. [Google Scholar] [CrossRef]
- Makker, V.; MacKay, H.; Ray-Coquard, I.; Levine, D.A.; Westin, S.N.; Aoki, D.; Oaknin, A. Endometrial cancer. Nat. Rev. Dis. Primers 2021, 7, 88. [Google Scholar] [CrossRef]
- Buda, A.; Di Martino, G.; Restaino, S.; De Ponti, E.; Monterossi, G.; Giuliani, D.; Ercoli, A.; Dell’Orto, F.; Dinoi, G.; Grassi, T.; et al. The impact on survival of two different staging strategies in apparent early stage endometrial cancer comparing sentinel lymph nodes mapping algorithm and selective lymphadenectomy: An Italian retrospective analysis of two reference centers. Gynecol. Oncol. 2017, 147, 528–534. [Google Scholar] [CrossRef]
- Matsuo, K.; Machida, H.; Ragab, O.M.; Takiuchi, T.; Pham, H.Q.; Roman, L.D. Extent of pelvic lymphadenectomy and use of adjuvant vaginal brachytherapy for early-stage endometrial cancer. Gynecol. Oncol. 2017, 144, 515–523. [Google Scholar] [CrossRef]
- Sun, S.; Zou, L.; Wang, T.; Liu, Z.; He, J.; Sun, X.; Zhong, W.; Zhao, F.; Li, X.; Li, S.; et al. Effect of age as a continuous variable in early-stage endometrial carcinoma: A multi-institutional analysis in China. Aging 2021, 13, 19561–19574. [Google Scholar] [CrossRef]
- Eggemann, H.; Ignatov, T.; Burger, E.; Costa, S.D.; Ignatov, A. Management of elderly women with endometrial cancer. Gynecol. Oncol. 2017, 146, 519–524. [Google Scholar] [CrossRef] [PubMed]
- Bibault, J.-E.; Nickers, P.; Tresch, E.; Cordoba, A.; Leblanc, E.; Comte, P.; Lacornerie, T.; Lartigau, E. Feasibility study of pelvic helical IMRT for elderly patients with endometrial cancer. PLoS ONE 2014, 9, e113279. [Google Scholar] [CrossRef] [PubMed]
- Lachance, J.A.; Stukenborg, G.J.; Schneider, B.F.; Rice, L.W.; Jazaeri, A.A. A cost-effective analysis of adjuvant therapies for the treatment of stage I endometrial adenocarcinoma. Gynecol. Oncol. 2008, 108, 77–83. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| GOG-249 (n = 473) | PORTEC-2 (n = 184) | ESMO-ESGO-ESTRO (n = 204) | |
|---|---|---|---|
| Time periods | |||
| 1999–2005 | 30 (6.3%) | 16 (8.7%) | 10 (4.9%) |
| 2005–2010 | 70 (14.8%) | 27 (14.7%) | 33 (16.2%) |
| 2010–2015 | 373 (78.9%) | 141 (76.6%) | 161 (78.9%) |
| Age | |||
| ≤60 years | 309 (65.3%) | 0 (0%) | 143 (70.1%) |
| >60 years | 164 (34.7%) | 184 (100%) | 61 (29.9%) |
| FIGO stage | |||
| IA | 59 (12.5%) | 29 (15.8%) | 159 (77.9%) |
| IB | 279 (60.0%) | 155 (84.2%) | 45 (22.1%) |
| II | 135 (28.5%) | 0 (0%) | 0 (0%) |
| Lymphovascular invasion | |||
| no | 332 (70.2%) | 163 (88.6%) | 92 (45.1%) |
| yes | 141 (29.8%) | 21 (11.4%) | 112 (54.9%) |
| Histologic grade | |||
| Grade 1 | 66 (14.0%) | 69 (37.5%) | 30 (14.7%) |
| Grade 2 | 278 (58.8%) | 84 (45.7%) | 68 (33.3%) |
| Grade 3 | 129 (27.2%) | 31 (16.8%) | 106 (52%) |
| Radiation therapy modality | |||
| VBT | 147 (31.1%) | 95 (51.6%) | 102 (50%) |
| EBRT ± VBT | 326 (68.9%) | 89 (48.4%) | 102 (50%) |
| Chemotherapy | |||
| yes | 100 (21.1%) | 24 (13%) | 53 (26%) |
| no | 335 (70.8%) | 140 (76.1%) | 133 (65.2%) |
| missing | 38 (8.0%) | 20 (10.9%) | 18 (8.8%) |
| Received lymph node dissection | |||
| yes(pN0) | 339 (71.7%) | 119 (64.5%) | 155 (76%) |
| Full dissection | 303 (89.4%) | 106 (89.1%) | 134 (86.5%) |
| SLN | 36 (10.6%) | 13 (10.9%) | 21 (13.5%) |
| no(cN0) | 134 (28.3%) | 65 (35.3%) | 49 (24.0%) |
| Cohorts | RT Mode | 5-Year OS | 5-Year DFS | 5-Year DMFS | 5-Year LRFS | |
|---|---|---|---|---|---|---|
| GOG-249 | Full cohort | VBT | 93.30% | 84.20% | 87.90% | 89.00% |
| EBRT ± VBT | 91.50% | 87.40% | 87.70% | 92.20% | ||
| P | 0.831 | 0.403 | 0.748 | 0.156 | ||
| After matching | VBT | 93.80% | 84.50% | 88.40% | 89.40% | |
| EBRT ± VBT | 91.90% | 84.60% | 85.30% | 91.20% | ||
| P | 0.855 | 0.834 | 0.855 | 0.311 | ||
| PORTEC-2 | Full cohort | VBT | 96.00% | 93.50% | 92.50% | 91.10% |
| EBRT ± VBT | 91.90% | 88.70% | 93.50% | 94.50% | ||
| P | 0.586 | 0.331 | 0.745 | 0.375 | ||
| After matching | VBT | 96.00% | 88.70% | 92.50% | 91.10% | |
| EBRT ± VBT | 96.40% | 95.10% | 95.10% | 97.10% | ||
| P | 0.976 | 0.186 | 0.462 | 0.174 | ||
| ESMO-ESGO-ESTRO | Full cohort | VBT | 96.90% | 87.40% | 90.60% | 89.20% |
| EBRT ± VBT | 93.10% | 90.60% | 91.20% | 94.60% | ||
| P | 0.372 | 0.263 | 0.937 | 0.223 | ||
| After matching | VBT | 96.90% | 87.40% | 91.20% | 89.20% | |
| EBRT ± VBT | 94.30% | 91.10% | 91.00% | 95.90% | ||
| P | 0.489 | 0.233 | 0.850 | 0.170 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ren, K.; Zou, L.; Wang, T.; Liu, Z.; He, J.; Sun, X.; Zhong, W.; Zhao, F.; Li, X.; Li, S.; et al. Utilization Trend and Comparison of Different Radiotherapy Modes for Patients with Early-Stage High-Intermediate-Risk Endometrial Cancer: A Real-World, Multi-Institutional Study. Cancers 2022, 14, 5129. https://doi.org/10.3390/cancers14205129
Ren K, Zou L, Wang T, Liu Z, He J, Sun X, Zhong W, Zhao F, Li X, Li S, et al. Utilization Trend and Comparison of Different Radiotherapy Modes for Patients with Early-Stage High-Intermediate-Risk Endometrial Cancer: A Real-World, Multi-Institutional Study. Cancers. 2022; 14(20):5129. https://doi.org/10.3390/cancers14205129
Chicago/Turabian StyleRen, Kang, Lijuan Zou, Tiejun Wang, Zi Liu, Jianli He, Xiaoge Sun, Wei Zhong, Fengju Zhao, Xiaomei Li, Sha Li, and et al. 2022. "Utilization Trend and Comparison of Different Radiotherapy Modes for Patients with Early-Stage High-Intermediate-Risk Endometrial Cancer: A Real-World, Multi-Institutional Study" Cancers 14, no. 20: 5129. https://doi.org/10.3390/cancers14205129
APA StyleRen, K., Zou, L., Wang, T., Liu, Z., He, J., Sun, X., Zhong, W., Zhao, F., Li, X., Li, S., Zhu, H., Ma, Z., Sun, S., Wang, W., Hu, K., Zhang, F., Hou, X., & Wei, L. (2022). Utilization Trend and Comparison of Different Radiotherapy Modes for Patients with Early-Stage High-Intermediate-Risk Endometrial Cancer: A Real-World, Multi-Institutional Study. Cancers, 14(20), 5129. https://doi.org/10.3390/cancers14205129