
Molecular Biomarker Expression in Window of Opportunity Studies for Oestrogen Receptor Positive Breast Cancer—A Systematic Review of the Literature



Abstract
Simple Summary
Abstract
1. Introduction
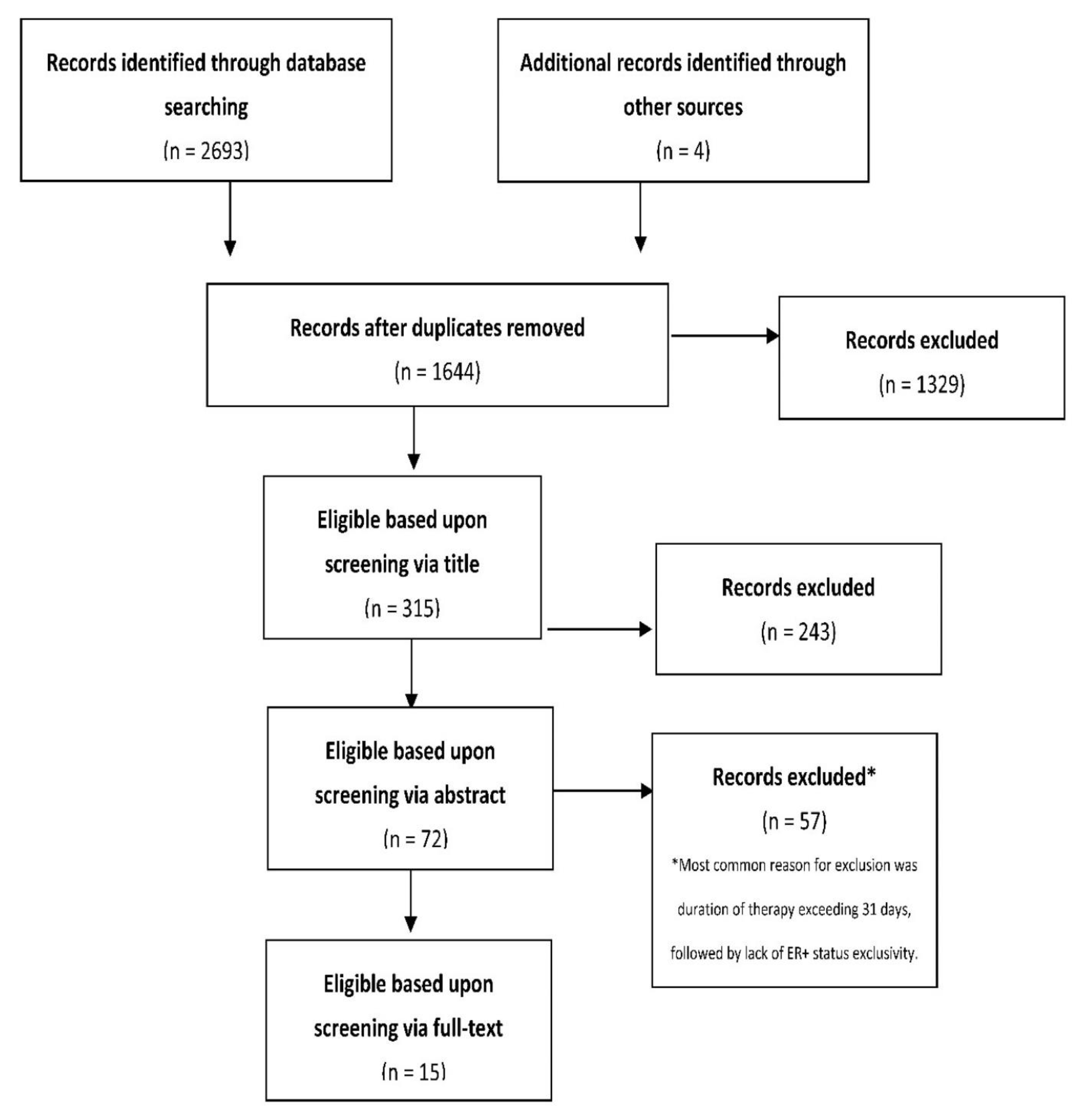
2. Materials and Methods
2.1. Search Strategy and Study Selection
2.2. Data Extraction
3. Results
3.1. General Characteristics
3.2. Changes in Molecular Biomarker Expression in the Window of Opportunity Setting
3.2.1. Aromatase Inhibitors (AIs)
3.2.2. Selective Oestrogen Receptor Degraders (SERDs)
3.2.3. Selective Oestrogen Receptor Modulators (SERMs)
3.2.4. Mammalian Target of Rapamycin (mTOR) Inhibitor
3.2.5. AKT Inhibitor
3.2.6. Oestrogens
4. Discussion
4.1. Changes in Molecular Biomarker Expression in the Window of Opportunity Setting
4.1.1. Aromatase Inhibitors (AIs)
4.1.2. Selective Oestrogen Receptor Degraders (SERDs)
4.1.3. Selective Oestrogen Receptor Modulators (SERMs)
4.1.4. mTOR Inhibitors
4.1.5. AKT Inhibitor
4.1.6. Oestrogen
4.2. Strengths of the Present Review
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Turashvili, G.; Brogi, E. Tumor Heterogeneity in Breast Cancer. Front. Med. 2017, 4, 227. [Google Scholar] [CrossRef]
- Harvey, J.M.; Clark, G.M.; Osborne, C.K.; Allred, D.C. Estrogen receptor status by immunohistochemistry is superior to the ligand-binding assay for predicting response to adjuvant endocrine therapy in breast cancer. J. Clin. Oncol. 1999, 17, 1474–1481. [Google Scholar] [CrossRef] [PubMed]
- Williams, C.; Lin, C.Y. Oestrogen receptors in breast cancer: Basic mechanisms and clinical implications. Ecancermedicalscience 2013, 7, 370. [Google Scholar] [CrossRef] [PubMed]
- Fan, W.; Chang, J.; Fu, P. Endocrine therapy resistance in breast cancer: Current status, possible mechanisms and overcoming strategies. Future Med. Chem. 2015, 7, 1511–1519. [Google Scholar] [CrossRef]
- Lei, J.T.; Anurag, M.; Haricharan, S.; Gou, X.; Ellis, M.J. Endocrine therapy resistance: New insights. Breast 2019, 48 (Suppl. S1), S26–S30. [Google Scholar] [CrossRef]
- Arnaout, A.; Robertson, S.; Kuchuk, I.; Simos, D.; Pond, G.R.; Addison, C.L.; Namazi, M.; Clemons, M. Evaluating the feasibility of performing window of opportunity trials in breast cancer. Int. J. Surg. Oncol. 2015, 2015, 785793. [Google Scholar] [CrossRef]
- Maugeri-Saccà, M.; Barba, M.; Vici, P.; Pizzuti, L.; Sergi, D.; Catenaro, T.; Di Lauro, L.; Mottolese, M.; Santini, D.; Milella, M.; et al. Presurgical window of opportunity trial design as a platform for testing anticancer drugs: Pros, cons and a focus on breast cancer. Crit. Rev. Oncol./Hematol. 2016, 106, 132–142. [Google Scholar] [CrossRef]
- Clarke, R.B.; Laidlaw, I.J.; Jones, L.J.; Howell, A.; Anderson, E. Effect of tamoxifen on Ki67 labelling index in human breast tumours and its relationship to oestrogen and progesterone receptor status. Br. J. Cancer 1993, 67, 606–611. [Google Scholar] [CrossRef]
- Bedard, P.L.; Singhal, S.K.; Ignatiadis, M.; Bradbury, I.; Haibe-Kains, B.; Desmedt, C.; Loi, S.; Evans, D.B.; Michiels, S.; Dixon, J.M.; et al. Low residual proliferation after short-term letrozole therapy is an early predictive marker of response in high proliferative ER-positive breast cancer. Endocr. Relat. Cancer 2011, 18, 721–730. [Google Scholar] [CrossRef]
- Cohen, A.L.; Factor, R.E.; Mooney, K.; Salama, M.E.; Wade, M.; Serpico, V.; Ostrander, E.; Nelson, E.; Porretta, J.; Matsen, C.; et al. POWERPIINC (PreOperative Window of Endocrine TheRapy Provides Information to Increase Compliance) trial: Changes in tumor proliferation index and quality of life with 7 days of preoperative tamoxifen. Breast 2017, 31, 219–223. [Google Scholar] [CrossRef] [PubMed]
- Curigliano, G.; Gómez Pardo, P.; Meric-Bernstam, F.; Conte, P.; Lolkema, M.P.; Beck, J.T.; Bardia, A.; Martínez García, M.; Penault-Llorca, F.; Dhuria, S.; et al. Ribociclib plus letrozole in early breast cancer: A presurgical, window-of-opportunity study. Breast 2016, 28, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Kisanga, E.R.; Gjerde, J.; Guerrieri-Gonzaga, A.; Pigatto, F.; Pesci-Feltri, A.; Robertson, C.; Serrano, D.; Pelosi, G.; Decensi, A.; Lien, E.A. Tamoxifen and metabolite concentrations in serum and breast cancer tissue during three dose regimens in a randomized preoperative trial. Clin. Cancer Res. 2004, 10, 2336–2343. [Google Scholar] [CrossRef] [PubMed]
- Loi, S.; Michiels, S.; Baselga, J.; Bartlett, J.M.S.; Singhal, S.K.; Sabine, V.S.; Sims, A.H.; Sahmoud, T.; Dixon, J.M.; Piccart, M.J.; et al. PIK3CA genotype and a PIK3CA mutation-related gene signature and response to everolimus and letrozole in estrogen receptor positive breast cancer. PLoS ONE 2013, 8, e53292. [Google Scholar] [CrossRef]
- Mattar, A.; Logullo, A.F.; Facina, G.; Nonogaki, S.; Soares, F.A.; Gebrim, L.H. Short-term anastrozole therapy reduces Ki-67 and progesterone receptor expression in invasive breast cancer: A prospective, placebo-controlled, double-blind trial. J. Cancer Res. Clin. Oncol. 2011, 137, 897–905. [Google Scholar] [CrossRef]
- Morrogh, M.; Andrade, V.P.; Patil, A.J.; Qin, L.-X.; Mo, Q.; Sakr, R.; Arroyo, C.D.; Brogi, E.; Morrow, M.; King, T.A. Differentially expressed genes in window trials are influenced by the wound-healing process: Lessons learned from a pilot study with anastrozole. J. Surg. Res. 2012, 176, 121–132. [Google Scholar] [CrossRef]
- Robertson, J.F.; Dixon, J.M.; Sibbering, D.M.; Jahan, A.; Ellis, I.O.; Channon, E.; Hyman-Taylor, P.; Nicholson, R.I.; Gee, J.M. A randomized trial to assess the biological activity of short-term (pre-surgical) fulvestrant 500 mg plus anastrozole versus fulvestrant 500 mg alone or anastrozole alone on primary breast cancer. Breast Cancer Res. 2013, 15, R18. [Google Scholar] [CrossRef]
- Robertson, J.F.; Evans, A.; Henschen, S.; Kirwan, C.C.; Jahan, A.; Kenny, L.M.; Dixon, J.M.; Schmid, P.; Kothari, A.; Mohamed, O.; et al. A randomized, window of opportunity study comparing the effects of the novel oral SERD AZD9496 with fulvestrant in patients with ER+ HER2− primary breast cancer. Clin. Cancer Res. 2020, 26, 4242–4249. [Google Scholar] [CrossRef]
- Robertson, J.F.R.; Coleman, R.E.; Cheung, K.L.; Evans, A.; Holcombe, C.; Skene, A.; Rea, D.; Ahmed, S.; Jahan, A.; Horgan, K.; et al. Proliferation and AKT Activity Biomarker Analyses after Capivasertib (AZD5363) Treatment of Patients with ER+ Invasive Breast Cancer (STAKT). Clin. Cancer Res. 2020, 26, 1574–1585. [Google Scholar] [CrossRef]
- Sabine, V.S.; Sims, A.H.; Macaskill, E.J.; Renshaw, L.; Thomas, J.S.; Dixon, J.M.; Bartlett, J.M. Gene expression profiling of response to mTOR inhibitor everolimus in pre-operatively treated post-menopausal women with oestrogen receptor-positive breast cancer. Breast Cancer Res. Treat. 2010, 122, 419–428. [Google Scholar] [CrossRef]
- Schmid, P.; Pinder, S.E.; Wheatley, D.; Macaskill, J.; Zammit, C.; Hu, J.; Price, R.; Bundred, N.; Hadad, S.; Shia, A.; et al. Phase II Randomized Preoperative Window-of-Opportunity Study of the PI3K Inhibitor Pictilisib Plus Anastrozole Compared With Anastrozole Alone in Patients With Estrogen Receptor-Positive Breast Cancer. J. Clin. Oncol. 2016, 34, 1987–1994. [Google Scholar] [CrossRef]
- Singer, C.F.; Bennink, H.J.; Natter, C.; Steurer, S.; Rudas, M.; Moinfar, F.; Appels, N.; Visser, M.; Kubista, E. Antiestrogenic effects of the fetal estrogen estetrol in women with estrogen-receptor positive early breast cancer. Carcinogenesis 2014, 35, 2447–2451. [Google Scholar] [CrossRef] [PubMed]
- Smith, I.; Robertson, J.; Kilburn, L.; Wilcox, M.; Evans, A.; Holcombe, C.; Horgan, K.; Kirwan, C.; Mallon, E.; Sibbering, M.; et al. Long-term outcome and prognostic value of Ki67 after perioperative endocrine therapy in postmenopausal women with hormone-sensitive early breast cancer (POETIC): An open-label, multicentre, parallel-group, randomised, phase 3 trial. Lancet Oncol. 2020, 21, 1443–1454. [Google Scholar] [CrossRef]
- Schmitz, S.; Duhoux, F.; Machiels, J.-P. Window of opportunity studies: Do they fulfil our expectations? Cancer Treat. Rev. 2016, 43, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Allison, K.H.; Hammond, M.E.H.; Dowsett, M.; McKernin, S.E.; Carey, L.A.; Fitzgibbons, P.L.; Hayes, D.F.; Lakhani, S.R.; Chavez-MacGregor, M.; Perlmutter, J.; et al. Estrogen and Progesterone Receptor Testing in Breast Cancer: ASCO/CAP Guideline Update. J. Clin. Oncol. 2020, 38, 1346–1366. [Google Scholar] [CrossRef] [PubMed]
- Inwald, E.C.; Klinkhammer-Schalke, M.; Hofstädter, F.; Zeman, F.; Koller, M.; Gerstenhauer, M.; Ortmann, O. Ki-67 is a prognostic parameter in breast cancer patients: Results of a large population-based cohort of a cancer registry. Breast Cancer Res. Treat. 2013, 139, 539–552. [Google Scholar] [CrossRef]
- Gerdes, J.; Schwab, U.; Lemke, H.; Stein, H. Production of a mouse monoclonal antibody reactive with a human nuclear antigen associated with cell proliferation. Int. J. Cancer 1983, 31, 13–20. [Google Scholar] [CrossRef]
- Scholzen, T.; Gerdes, J. The Ki-67 protein: From the known and the unknown. J. Cell. Physiol. 2000, 182, 311–322. [Google Scholar] [CrossRef]
- Cabrera-Galeana, P.; Munoz-Montano, W.; Lara-Medina, F.; Alvarado-Miranda, A.; Perez-Sanchez, V.; Villarreal-Garza, C.; Quintero, R.M.; Porras-Reyes, F.; Bargallo-Rocha, E.; Del Carmen, I.; et al. Ki67 Changes Identify Worse Outcomes in Residual Breast Cancer Tumors After Neoadjuvant Chemotherapy. Oncologist 2018, 23, 670–678. [Google Scholar] [CrossRef]
- De Vos, F.Y.; van Laarhoven, H.W.; Laven, J.S.; Themmen, A.P.; Beex, L.V.; Sweep, C.G.; Seynaeve, C.; Jager, A. Menopausal status and adjuvant hormonal therapy for breast cancer patients: A practical guideline. Crit. Rev. Oncol. Hematol. 2012, 84, 252–260. [Google Scholar] [CrossRef]
- Bian, C.; Zhao, Y.; Guo, Q.; Xiong, Y.; Cai, W.; Zhang, J. Aromatase inhibitor letrozole downregulates steroid receptor coactivator-1 in specific brain regions that primarily related to memory, neuroendocrine and integration. J. Steroid Biochem. Mol. Biol. 2014, 141, 37–43. [Google Scholar] [CrossRef]
- Diep, C.H.; Ahrendt, H.; Lange, C.A. Progesterone induces progesterone receptor gene (PGR) expression via rapid activation of protein kinase pathways required for cooperative estrogen receptor alpha (ER) and progesterone receptor (PR) genomic action at ER/PR target genes. Steroids 2016, 114, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Anderson, T.J.; Dixon, J.M.; Stuart, M.; Sahmoud, T.; Miller, W.R. Effect of neoadjuvant treatment with anastrozole on tumour histology in postmenopausal women with large operable breast cancer. Br. J. Cancer 2002, 87, 334–338. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Geisler, J.; Detre, S.; Berntsen, H.; Ottestad, L.; Lindtjorn, B.; Dowsett, M.; Einstein Lonning, P. Influence of neoadjuvant anastrozole (Arimidex) on intratumoral estrogen levels and proliferation markers in patients with locally advanced breast cancer. Clin. Cancer Res. 2001, 7, 1230–1236. [Google Scholar] [PubMed]
- Retsky, M.; Demicheli, R.; Hrushesky, W.J. Does surgery induce angiogenesis in breast cancer? Indirect evidence from relapse pattern and mammography paradox. Int. J. Surg. 2005, 3, 179–187. [Google Scholar] [CrossRef]
- Howell, S.J.; Johnston, S.R.; Howell, A. The use of selective estrogen receptor modulators and selective estrogen receptor down-regulators in breast cancer. Best Pract. Res. Clin. Endocrinol. Metab. 2004, 18, 47–66. [Google Scholar] [CrossRef] [PubMed]
- Fasching, P.A.; Bardia, A.; Quiroga, V.; Park, Y.H.; Blancas, I.; Alonso, J.L.; Vasilyev, A.; Adamchuk, H.; Salgado, M.R.T.; Yardley, D.A.; et al. Neoadjuvant giredestrant (GDC-9545) plus palbociclib (P) versus anastrozole (A) plus P in postmenopausal women with estrogen receptor–positive, HER2-negative, untreated early breast cancer (ER+/HER2− eBC): Final analysis of the randomized, open-label, international phase 2 coopERA BC study. J. Clin. Oncol. 2022, 40 (Suppl. S16), 589. [Google Scholar] [CrossRef]
- Barkhem, T.; Andersson-Ross, C.; Hoglund, M.; Nilsson, S. Characterization of the “estrogenicity” of tamoxifen and raloxifene in HepG2 cells: Regulation of gene expression from an ERE controlled reporter vector versus regulation of the endogenous SHBG and PS2 genes. J. Steroid Biochem. Mol. Biol. 1997, 62, 53–64. [Google Scholar] [CrossRef]
- Derman, O.; Kanbur, N.O.; Tokur, T.E. The effect of tamoxifen on sex hormone binding globulin in adolescents with pubertal gynecomastia. J. Pediatr. Endocrinol. Metab. 2004, 17, 1115–1119. [Google Scholar] [CrossRef]
- Cohen, I. Endometrial pathologies associated with postmenopausal tamoxifen treatment. Gynecol. Oncol. 2004, 94, 256–266. [Google Scholar] [CrossRef]
- Hu, R.; Hilakivi-Clarke, L.; Clarke, R. Molecular mechanisms of tamoxifen-associated endometrial cancer (Review). Oncol. Lett. 2015, 9, 1495–1501. [Google Scholar] [CrossRef] [PubMed]
- NICE. Everolimus with Exemestane for Treating Advanced Breast Cancer after Endocrine Therapy. 2016. Available online: https://www.nice.org.uk/guidance/ta421/chapter/1-Recommendations (accessed on 28 July 2022).
- Martorana, F.; Motta, G.; Pavone, G.; Motta, L.; Stella, S.; Vitale, S.R.; Manzella, L.; Vigneri, P. AKT Inhibitors: New Weapons in the Fight Against Breast Cancer? Front. Pharmacol. 2021, 12, 662232. [Google Scholar] [CrossRef] [PubMed]
- Xing, Y.; Lin, N.U.; Maurer, M.A.; Chen, H.; Mahvash, A.; Sahin, A.; Akcakanat, A.; Li, Y.; Abramson, V.; Litton, J.; et al. Phase II trial of AKT inhibitor MK-2206 in patients with advanced breast cancer who have tumors with PIK3CA or AKT mutations, and/or PTEN loss/PTEN mutation. Breast Cancer Res. 2019, 21, 78. [Google Scholar] [CrossRef] [PubMed]
- NHS. Overview: Breast Cancer in Women. 2019. Available online: https://www.nhs.uk/conditions/breast-cancer/ (accessed on 28 July 2022).
- Goorts, B.; van Nijnatten, T.J.; de Munck, L.; Moossdorff, M.; Heuts, E.M.; de Boer, M.; Lobbes, M.B.; Smidt, M.L. Clinical tumor stage is the most important predictor of pathological complete response rate after neoadjuvant chemotherapy in breast cancer patients. Breast Cancer Res. Treat. 2017, 163, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Nitz, U.; Gluz, O.; Graeser, M.; Christgen, M.; Kuemmel, S.; Grischke, E.-M.; Braun, M.; Augustin, D.; Potenberg, J.; Krauss, K.; et al. De-escalated neoadjuvant pertuzumab plus trastuzumab therapy with or without weekly paclitaxel in HER2-positive, hormone receptor-negative, early breast cancer (WSG-ADAPT-HER2+/HR−): Survival outcomes from a multicentre, open-label, randomised, phase 2 trial. Lancet Oncol. 2022, 23, 625–635. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study No. | Author, Year | Tumour Characteristics | ER+ Status Threshold | Arm 1 Compound | Arm 2 Compound | Arm 3 Compound | Arm 4 Compound | Duration of Therapy (days) | Number of Patients | Biomarker Measured |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. | Arnaout et al., 2015 [7] | Post-menopausal, Stage II–III invasive carcinoma ≥ 2 cm | ≥1% expression | Anastrozole | - | - | - | 15–44 | 20 | Caspase-3, Ki67 |
| 2. | Bedard et al., 2011 [10] | Post-menopausal | Allred Score 5–8 | Letrozole | - | - | - | 10–14 | 52 | Ki67 |
| 3. | Cohen et al., 2017 [11] | Stage I–II invasive cancer | ≥1% expression | Tamoxifen | - | - | - | 7 | 44 | Ki67 |
| 4. | Curigliano et al., 2016 [12] | Post-menopausal, Grade II–III HR+ HER2− invasive cancer | Not stated | Letrozole | Letrozole + ribociclib | Letrozole + ribociclib | - | 14 | 14 | Ki67 |
| 5. | Kisanga et al., 2004 [13] | None stated | ≥20% expression | Tamoxifen (low dose) | Tamoxifen (medium dose) | Tamoxifen (high dose) | Placebo | 28 | 120 | Ki67, SHBG |
| 6. | Loi et al., 2013 [14] | Post-menopausal cancer ≥ 2 cm | Not stated | Everolimus | Letrozole | Letrozole + everolimus | - | 14 | 23 | Ki67, pS6 |
| 7. | Mattar et al., 2011 [15] | None stated | Allred Score ≥2 | Anastrozole | Tamoxifen | - | - | 26 | 58 | ER, PR, Ki67 |
| 8. | Morrogh et al., 2012 [16] | Post-menopausal breast cancer ≥ 1 cm | ≥10% expression | Anastrozole | Placebo | - | - | 10–11 | 26 | CD34, Ki67 |
| 9. | Robertson et al., 2013 [17] | Post-menopausal primary | Not stated | Anastrozole | Fulvestrant | - | - | 14–21 | 121 | ER, PR, Ki67 |
| 10. | Robertson et al., 2020) [18] | Post-menopausal HER2− primary invasive cancer ≥ 1 cm | ≥10% expression | AZD9496 | Fulvestrant | - | - | 5–14 | 46 | ER, casPR, Ki67 |
| 11. | Robertson et al., 2020b [19] | Invasive breast carcinoma | Not stated | Capivasertib | Placebo | - | - | 4.5 | 48 | Ki67, pGSK3B, pPRAS40 |
| 12. | Sabine et al., 2010 [20] | Post-menopausal, early operable breast cancer | Not stated | Everolimus | - | - | - | 11–14 | 32 | Ki67, phospho-AKT |
| 13. | Schmid et al., 2016 [21] | Post-menopausal HER2− invasive breast cancer | ≥1% expression OR Allred Score ≥3 | Anastrozole | Anastrozole + pictilisib | - | - | 14 | 75 | Caspase-3, Ki67, PR, PTEN |
| 14. | Singer et al., 2014 [22] | Early-stage M0 breast cancer | Not stated | Estetrol (E4) | Placebo | - | - | 14 | 30 | Bax, Bcl-2, ERa, ERb, IGF-1, Ki67, PR, prolactin |
| 15. | Smith et al., 2020 [23] | Post-menopausal operable primary, M0 breast cancer ≥ 1.5 cm | ≥1% expression OR Allred Score ≥3 | Anastrozole OR letrozole | Placebo | - | - | 14 | 4480 | Ki67 |
| Class of Drug(s) | Drugs | Molecular Biomarkers Significantly Changed from Baseline |
|---|---|---|
| AIs | Anastrozole, letrozole |
|
| SERDs | AZD9496, fulvestrant |
|
| SERMs | Tamoxifen |
|
| mTOR inhibitors | Everolimus |
|
| AKT inhibitors | Capivasertib |
|
| Oestrogens | Estetrol (E4) |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Francis, J.W.M.; Saundh, M.; Parks, R.M.; Cheung, K.-L. Molecular Biomarker Expression in Window of Opportunity Studies for Oestrogen Receptor Positive Breast Cancer—A Systematic Review of the Literature. Cancers 2022, 14, 5027. https://doi.org/10.3390/cancers14205027
Francis JWM, Saundh M, Parks RM, Cheung K-L. Molecular Biomarker Expression in Window of Opportunity Studies for Oestrogen Receptor Positive Breast Cancer—A Systematic Review of the Literature. Cancers. 2022; 14(20):5027. https://doi.org/10.3390/cancers14205027
Chicago/Turabian StyleFrancis, James W. M., Manmeet Saundh, Ruth M. Parks, and Kwok-Leung Cheung. 2022. "Molecular Biomarker Expression in Window of Opportunity Studies for Oestrogen Receptor Positive Breast Cancer—A Systematic Review of the Literature" Cancers 14, no. 20: 5027. https://doi.org/10.3390/cancers14205027
APA StyleFrancis, J. W. M., Saundh, M., Parks, R. M., & Cheung, K.-L. (2022). Molecular Biomarker Expression in Window of Opportunity Studies for Oestrogen Receptor Positive Breast Cancer—A Systematic Review of the Literature. Cancers, 14(20), 5027. https://doi.org/10.3390/cancers14205027