
Coronary Artery Disease and Cancer: Treatment and Prognosis Regarding Gender Differences

Abstract
:Simple Summary
Abstract
1. Introduction
2. Cancer Patients with Acute Coronary Syndrome (ACS) in General
2.1. In-Hospital Survival and Long-Term Outcomes after AMI in Cancer
2.2. Comorbidities and Adverse Events
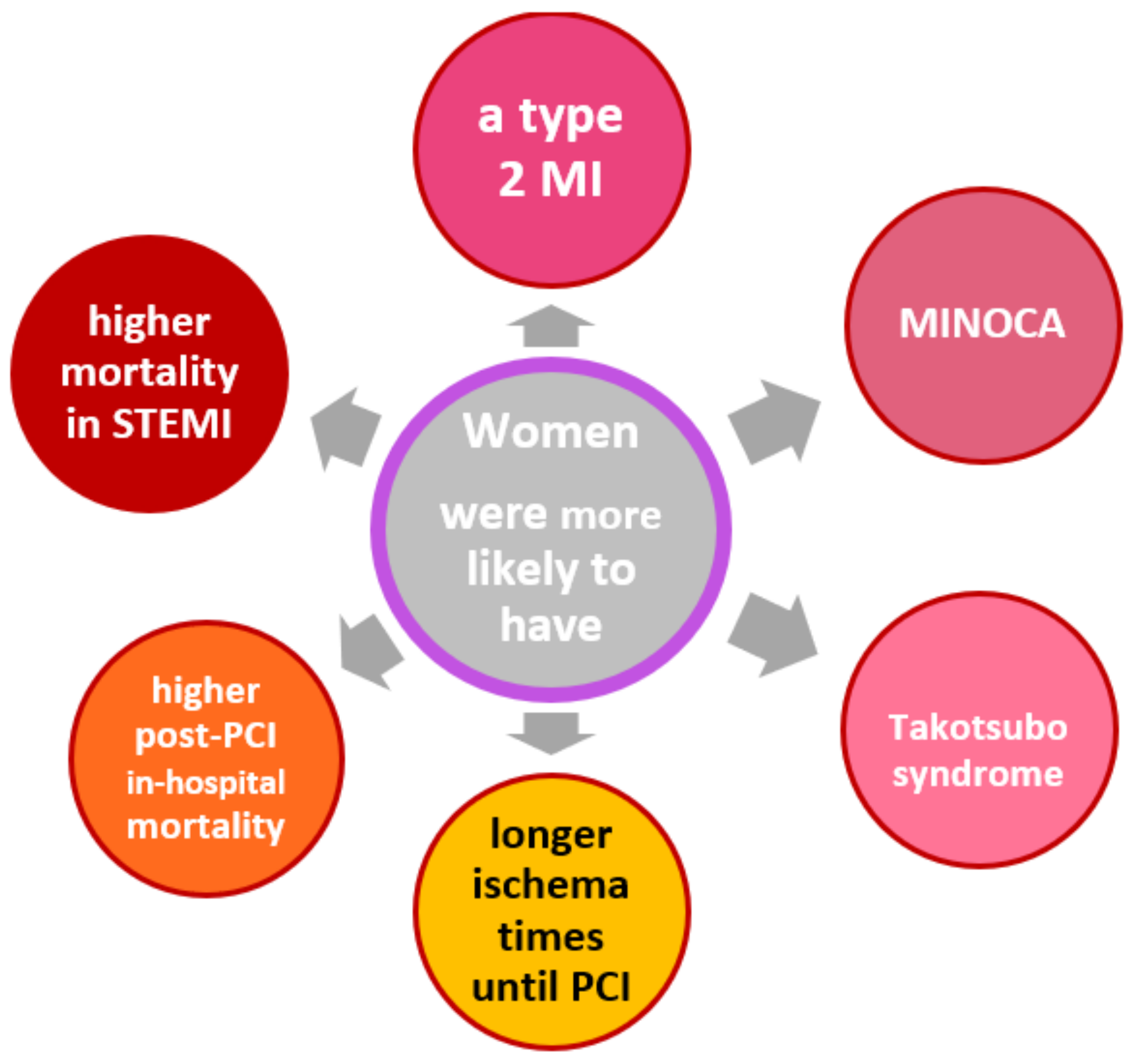
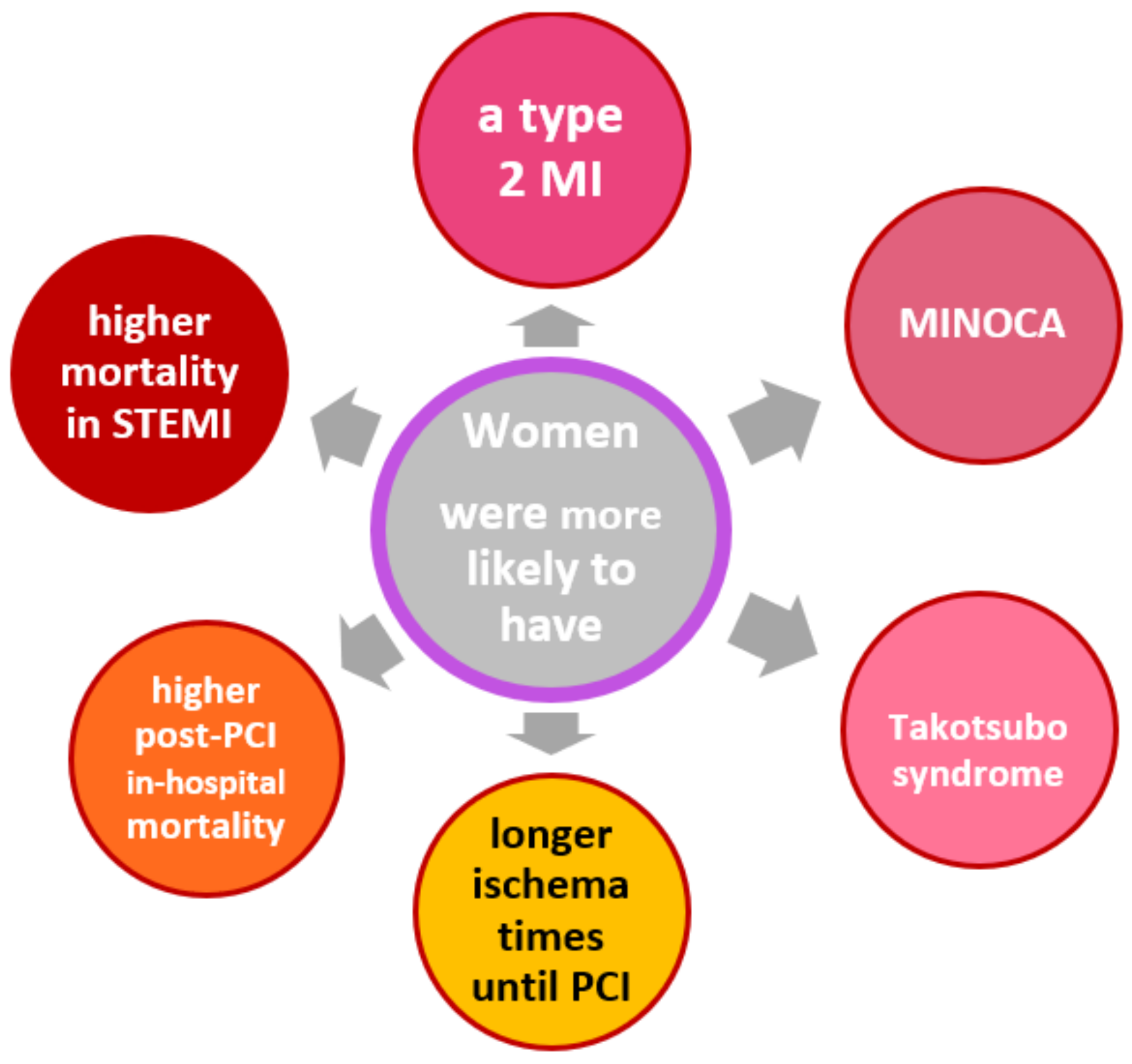
2.3. Gender Aspects
3. Impact of Distinct Cancer Types
3.1. Prostate Cancer
3.2. Breast Cancer
3.3. Colorectal Cancer
3.4. Lung Cancer
3.5. Hematological Malignancies
4. Specific Cancer Treatment and Cardiovascular Side-Effects
4.1. Prostate Cancer
4.2. Breast Cancer
4.3. Colon Cancer
4.4. Lung Cancer
4.5. Hematological Malignancies
5. Outcomes of Revascularization Procedures in Cancer Patients
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ACS | acute coronary syndrome |
| ACT | activated clotting time |
| ALL | acute lymphatic leukemia |
| AMI | acute myocardial infarction |
| AML | acute myeloid leukemia |
| ASA | acetylsalicylic acid |
| BMS | bare metal stent |
| CABG | coronary artery bypass graft (surgery) |
| CAD | coronary artery disease |
| CHOP | Cytoxan, Hydroxyrubicin (Adriamycin), Oncovin (Vincristine), Prednisone (chemotherapy regimen) |
| CI | confidence interval |
| CLL | chronic lymphatic leukemia |
| CML | chronic myeloid leukemia |
| CYP | cytochrome P |
| DAPT | dual antiplatelet therapy |
| DES | drug eluting stent |
| EU | European Union |
| FU | fluorouracil |
| GDP | guanosine 5’-diphosphate |
| HF | heart failure |
| HR | hazard ratio |
| hsCRP | high sensitive C-reactive protein |
| IL | interleukin |
| IVUS | intravascular ultrasound |
| MACCE | major adverse cardiac and cerebrovascular events |
| MACE | major adverse cardiac events |
| MI | myocardial infarction |
| MINOCA | myocardial infarction with nonobstructive coronary arteries |
| NHL | non-Hodgkin lymphoma |
| NSTEMI | non-ST-elevation myocardial infarction |
| OCT | optical coherence tomography |
| OR | odds ratio |
| QoL | quality-of-life |
| PCI | percutaneous coronary intervention |
| POBA | percutaneous old balloon angioplasty |
| SIR | standard incidence ratio |
| STEMI | ST-elevation myocardial infarction |
| TKI | tyrosine kinase inhibitor |
| US | United States |
| VEGF | vascular endothelial growth factor |
References
- Dégano, I.R.; Salomaa, V.; Veronesi, G.; Ferriéres, J.; Kirchberger, I.; Laks, T.; Havulinna, A.S.; Ruidavets, J.B.; Ferrario, M.M.; Meisinger, C.; et al. Acute Myocardial Infarction Trends in Europe (AMITIE) Study Investigators. Twenty-five-year trends in myocardial infarction attack and mortality rates, and case-fatality, in six European populations. Heart 2015, 101, 1413–1421. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer. Available online: https://www.iarc.who.int/ (accessed on 1 August 2021).
- Velders, M.A.; Hagström, E.; James, S.K. Temporal Trends in the Prevalence of Cancer and Its Impact on Outcome in Patients with First Myocardial Infarction: A Nationwide Study. J. Am. Heart Assoc. 2020, 9, e014383. [Google Scholar] [CrossRef]
- Koene, R.J.; Prizment, A.E.; Blaes, A.; Konety, S.H. Shared Risk Factors in Cardiovascular Disease and Cancer. Circulation 2016, 133, 1104–1114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFadyen, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [CrossRef] [PubMed]
- Scholz, K.H.; Maier, S.K.G.; Maier, L.S.; Lengenfelder, B.; Jacobshagen, C.; Jung, J.; Fleischmann, C.; Werner, G.S.; Olbrich, H.G.; Ott, R.; et al. Impact of treatment delay on mortality in ST-segment elevation myocardial infarction (STEMI) patients presenting with and without haemodynamic instability: Results from the German prospective, multicentre FITT-STEMI trial. Eur. Heart J. 2018, 39, 1065–1074. [Google Scholar] [CrossRef] [Green Version]
- Potts, J.E.; Iliescu, C.A.; Lopez-Mattei, J.C.; Martinez, S.C.; Holmvang, L.; Ludman, P.; De Belder, M.A.; Kwok, C.S.; Rashid, M.; Fischman, D.L.; et al. Percutaneous coronary intervention in cancer patients: A report of the prevalence and outcomes in the United States. Eur. Heart J. 2019, 40, 1790–1800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ezekowitz, J.A.; Savu, A.; Welsh, R.C.; McAlister, F.A.; Goodman, S.G.; Kaul, P. Is There a Sex Gap in Surviving an Acute Coronary Syndrome or Subsequent Development of Heart Failure? Circulation 2020, 142, 2231–2239. [Google Scholar] [CrossRef]
- Kuehnemund, L.; Koeppe, J.; Feld, J.; Wiederhold, A.; Illner, J.; Makowski, L.; Gerß, J.; Reinecke, H.; Freisinger, E. Gender differences in acute myocardial infarction—A nationwide German real-life analysis from 2014 to 2017. Clin. Cardiol. 2021, 44, 890–898. [Google Scholar] [CrossRef]
- European Union. ECIS—European Cancer Information System. Available online: https://ecis.jrc.ec.europa.eu (accessed on 10 August 2020).
- Rohrmann, S.; Witassek, F.; Erne, P.; Rickli, H.; Radovanovic, D. Treatment of patients with myocardial infarction depends on history of cancer. Eur. Heart J. Acute Cardiovasc. Care 2018, 7, 639–645. [Google Scholar] [CrossRef]
- Guddati, A.K.; Joy, P.S.; Kumar, G. Analysis of outcomes of percutaneous coronary intervention in metastatic cancer patients with acute coronary syndrome over a 10-year period. J. Cancer Res. Clin. Oncol. 2016, 142, 471–479. [Google Scholar] [CrossRef]
- Park, J.Y.; Guo, W.; Al-Hijji, M.; El Sabbagh, A.; Begna, K.H.; Habermann, T.M.; Witzig, T.E.; Lewis, B.R.; Lerman, A.; Herrmann, J. Acute coronary syndromes in patients with active hematologic malignancie—Incidence, management, and outcomes. Int. J. Cardiol. 2019, 275, 6–12. [Google Scholar] [CrossRef]
- Mohamed, M.O.; Lopez-Mattei, J.C.; Parwani, P.; Iliescu, C.A.; Bharadwaj, A.; Kim, P.Y.; Palaskas, N.L.; Rashid, M.; Potts, J.; Kwok, C.S.; et al. Management strategies and clinical outcomes of acute myocardial infarction in leukaemia patients: Na-tionwide insights from United States hospitalisations. Int. J. Clin. Pract. 2020, 74, e13476. [Google Scholar] [CrossRef] [Green Version]
- Agmon, I.N.; Perl, L.; Bental, T.; Ben Zadok, O.I.; Vaknin-Assa, H.; Codner, P.; Greenberg, G.; Kornowski, R. Temporal trends in short and long-term outcomes after percutaneous coronary interventions among cancer patients. Heart Vessel. 2021, 36, 1283–1289. [Google Scholar] [CrossRef] [PubMed]
- Kurisu, S.; Iwasaki, T.; Ishibashi, K.; Mitsuba, N.; Dohi, Y.; Kihara, Y. Comparison of treatment and outcome of acute myocardial infarction between cancer patients and non-cancer patients. Int. J. Cardiol. 2013, 167, 2335–2337. [Google Scholar] [CrossRef]
- Velders, M.A.; Boden, H.; van Boven, A.J.; van der Hoeven, B.L.; Heestermans, A.A.; Cannegieter, S.C.; Umans, V.A.; Jukema, J.W.; Hofma, S.H.; Schalij, M.J. Influence of Gender on Ischemic Times and Outcomes After ST-Elevation Myocardial Infarction. Am. J. Cardiol. 2013, 111, 312–318. [Google Scholar] [CrossRef]
- Wang, F.; Gulati, R.; Lennon, R.J.; Lewis, B.R.; Park, J.; Sandhu, G.S.; Wright, R.S.; Lerman, A.; Herrmann, J. Cancer History Portends Worse Acute and Long-term Noncardiac (but Not Cardiac) Mortality After Primary Percutaneous Coronary Inter-vention for Acute ST-Segment Elevation Myocardial Infarction. Mayo. Clin. Proc. 2016, 91, 1680–1692. [Google Scholar] [CrossRef] [PubMed]
- Landes, U.; Kornowski, R.; Bental, T.; Assali, A.; Vaknin-Assa, H.; Lev, E.; Iakobishvili, Z. Long-term outcomes after percutaneous coronary interventions in cancer survivors. Coron. Artery Dis. 2017, 28, 5–10. [Google Scholar] [CrossRef]
- Nakatsuma, K.; Shiomi, H.; Morimoto, T.; Watanabe, H.; Nakagawa, Y.; Furukawa, Y.; Kadota, K.; Ando, K.; Ono, K.; Shizuta, S.; et al. Influence of a history of cancer on long-term cardiovascular outcomes after coronary stent implantation (an Obser-vation from Coronary Revascularization Demonstrating Outcome Study-Kyoto Registry Cohort-2). CREDO-Kyoto PCI/CABG Registry Cohort-2 Investigators. Eur. Heart J.-Qual. Care Clin. Outcomes 2018, 4, 200–207. [Google Scholar]
- Iannaccone, M.; D’Ascenzo, F.; Vadalà, P.; Wilton, S.B.; Noussan, P.; Colombo, F.; Raposeiras Roubín, S.; Abu Assi, E.; González-Juanatey, J.R.; Simao Henriques, J.P.; et al. Prevalence and outcome of patients with cancer and acute coronary syndrome undergoing percutaneous coronary intervention: A BleeMACS substudy. Eur. Heart J. Acute Cardiovasc. Care 2018, 7, 631–638. [Google Scholar] [CrossRef]
- Gaddam, A.; Ajibawo, T.; Ravat, V.; Yomi, T.; Patel, R.S. In-Hospital Mortality Risk in Post-Percutaneous Coronary Inter-ventions Cancer Patients: A Nationwide Analysis of 1.1 Million Heart Disease Patients. Cureus 2020, 12, e9071. [Google Scholar] [PubMed]
- Kwok, C.S.; Wong, C.W.; Kontopantelis, E.; Barac, A.; Brown, S.-A.; Velagapudi, P.; Hilliard, A.A.; Bharadwaj, A.S.; Alraies, M.C.; Mohamed, M.; et al. Percutaneous coronary intervention in patients with cancer and readmissions within 90 days for acute myocardial infarction and bleeding in the USA. Eur. Heart J. 2021, 42, 1019–1034. [Google Scholar] [CrossRef]
- Takeuchi, T.; Hikoso, S.; Hattori, S.; Kitamura, T.; Nakatani, D.; Mizuno, H.; Okada, K.; Dohi, T.; Kojima, T.; Kida, H.; et al. The Effect of a Cancer History on Patients with Acute Myocardial Infarction After Percutaneous Coronary Intervention. Int. Heart J. 2021, 62, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Pothineni, N.V.; Shah, N.N.; Rochlani, Y.; Saad, M.; Kovelamudi, S.; Marmagkiolis, K.; Bhatti, S.; Cilingiroglu, M.; Aronow, W.S.; Hakeem, A. Temporal trends and outcomes of acute myocardial infarction in patients with cancer. Ann. Transl. Med. 2017, 5, 482. [Google Scholar] [CrossRef] [Green Version]
- Gong, I.Y.; Yan, A.T.; Ko, D.T.; Earle, C.C.; Cheung, W.Y.; Peacock, S.; Hall, M.; Gale, C.P.; Chan, K.K.W. Temporal changes in treatments and outcomes after acute myocardial infarction among cancer survivors and patients without cancer, 1995 to 2013. Cancer 2018, 124, 1269–1278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ederhy, S.; Cohen, A.; Boccara, F.; Puymirat, E.; Aissaoui, N.; Elbaz, M.; Bonnefoy-Cudraz, E.; Druelles, P.; Andrieu, S.; Angoulvant, D.; et al. In-hospital outcomes and 5-year mortality following an acute myocardial infarction in patients with a history of cancer: Results from the French registry on Acute ST-elevation or non-ST-elevation myocardial infarction (FAST-MI) 2005 cohort. Arch. Cardiovasc. Dis. 2019, 112, 657–669. [Google Scholar] [CrossRef] [PubMed]
- Bharadwaj, A.; Potts, J.; Mohamed, M.O.; Parwani, P.; Swamy, P.; Lopez-Mattei, J.C.; Rashid, M.; Kwok, C.S.; Fischman, D.L.; Vassiliou, V.S.; et al. Acute myocardial infarction treatments and outcomes in 6.5 million patients with a current or historical diagnosis of cancer in the USA. Eur. Heart J. 2020, 41, 2183–2193. [Google Scholar] [CrossRef]
- Strongman, H.; Gadd, S.; Matthews, A.; Mansfield, K.E.; Stanway, S.; Lyon, A.R.; Dos-Santos-Silva, I.; Smeeth, L.; Bhaskaran, K. Medium and long-term risks of specific cardiovascular diseases in survivors of 20 adult cancers: A population-based cohortstudy using multiple linked UK electronic health records databases. Lancet 2019, 394, 1041–1054. [Google Scholar] [CrossRef] [Green Version]
- Zöller, B.; Ji, J.; Sundquist, J.; Sundquist, K. Risk of coronary heart disease in patients with cancer: A nationwide follow-up study from Sweden. Eur. J. Cancer 2012, 48, 121–128. [Google Scholar] [CrossRef]
- Hess, C.N.; Roe, M.T.; Clare, R.M.; Chiswell, K.; Kelly, J.; Tcheng, J.E.; Hagstrom, E.; James, S.K.; Khouri, M.G.; Hirsch, B.R.; et al. Relationship Between Cancer and Cardiovascular Outcomes Following Percutaneous Coronary Intervention. J. Am. Heart Assoc. 2015, 4, 001779. [Google Scholar] [CrossRef] [Green Version]
- Velders, M.A.; Boden, H.; Hofma, S.H.; Osanto, S.; van der Hoeven, B.L.; Heestermans, A.A.; Cannegieter, S.C.; Jukema, J.W.; Umans, V.A.; Schalij, M.J.; et al. Outcome After ST Elevation Myocardial Infarction in Patients With Cancer Treated With Primary Percutaneous Coronary Intervention. Am. J. Cardiol. 2013, 112, 1867–1872. [Google Scholar] [CrossRef]
- Ram, P.; Tiu, A.; Lo, K.B.; Parikh, K.; Shah, M. Trends in the prevalence of malignancy among patients admitted with acute heart failure and associated outcomes: A nationwide population-based study. Heart Fail. Rev. 2019, 24, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Vogel, B.; Acevedo, M.; Appelman, Y.; Merz, C.N.B.; Chieffo, A.; Figtree, G.A.; Guerrero, M.; Kunadian, V.; Lam, C.S.P.; Maas, A.H.E.M.; et al. The Lancet women and cardiovascular disease Commission: Reducing the global burden by 2030. Lancet 2021, 397, 2385–2438. [Google Scholar] [CrossRef]
- Jackson, A.M.; Zhang, R.; Findlay, I.; Robertson, K.; Lindsay, M.; Morris, T.; Forbes, B.; Papworth, R.; McConnachie, A.; Mangion, K.; et al. Healthcare disparities for women hospitalized with myocardial infarction and angina. Eur. Heart J.-Qual. Care Clin. Outcomes 2020, 6, 156–165. [Google Scholar] [CrossRef] [PubMed]
- Munoz, E.; Iliescu, G.; Vejpongsa, P.; Charitakis, K.; Karimzad, K.; Lopez-Mattei, J.; Yusuf, S.W.; Marmagkiolis, K.; Iliescu, C. Takotsubo Stress Cardiomyopathy: “Good News“ in Cancer Patients? J. Am. Coll. Cardiol. 2016, 68, 1143–1144. [Google Scholar] [CrossRef]
- Pancholy, S.B.; Shantha, G.P.; Patel, T.; Cheskin, L.J. Sex differences in short-term and long-term all-cause mortality among patients with ST-segment elevation myocardial infarction treated by primary percutaneous intervention: A meta-analysis. JAMA Intern. Med. 2014, 174, 1822–1830. [Google Scholar] [CrossRef]
- Kleikamp, G.; Schnepper, U.; Körfer, R. Coronary Artery and Aortic Valve Disease as a Long-Term Sequel of Mediastinal and Thoracic Irradiation. Thorac. Cardiovasc. Surg. 1997, 45, 27–31. [Google Scholar] [CrossRef]
- Wang, F.; Shu, X.; Meszoely, I.; Pal, T.; Mayer, I.A.; Yu, Z.; Zheng, W.; Bailey, C.E.; Shu, X.-O. Overall Mortality After Diagnosis of Breast Cancer in Men vs Women. JAMA Oncol. 2019, 5, 1589–1596. [Google Scholar] [CrossRef]
- Abdel-Rahman, O. Causes of death in long-term lung cancer survivors: A SEER database analysis. Curr. Med. Res. Opin. 2017, 33, 1343–1348. [Google Scholar] [CrossRef] [PubMed]
- Radmilovic, J.; Di Vilio, A.; D’Andrea, A.; Pastore, F.; Forni, A.; Desiderio, A.; Ragni, M.; Quaranta, G.; Cimmino, G.; Russo, V.; et al. The Pharmacological Approach to Oncologic Patients with Acute Coronary Syndrome. J. Clin. Med. 2020, 9, 3926. [Google Scholar] [CrossRef] [PubMed]
- Ball, S.; Ghosh, R.K.; Wongsaengsak, S.; Bandyopadhyay, D.; Ghosh, G.; Aronow, W.S.; Fonarow, G.C.; Lenihan, D.J.; Bhatt, D.L. Cardiovascular Toxicities of Immune Checkpoint Inhibitors: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2019, 74, 1714–1727. [Google Scholar] [CrossRef]
- Beyer, A.M.; Bonini, M.G.; Moslehi, J. Cancer therapy-induced cardiovascular toxicity: Old/new problems and old drugs. Am. J. Physiol. Heart Circ. Physiol. 2019, 317, H164–H167. [Google Scholar] [CrossRef]
- Stewart, F.A.; Heeneman, S.; Te Poele, J.; Kruse, J.; Russell, N.S.; Gijbels, M.; Daemen, M. Ionizing radiation accelerates the development of atherosclerotic lesions in ApoE-/- mice and predisposes to an inflammatory plaque phenotype prone to hemorrhage. Am. J. Pathol. 2006, 168, 649–658. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.S.; Finch, W.; Mahmud, E. Cardiovascular Complications of Radiotherapy. Am. J. Cardiol. 2013, 112, 1688–1696. [Google Scholar] [CrossRef] [PubMed]
- Bergom, C.; Bradley, J.A.; Ng, A.K.; Samson, P.; Robinson, C.; Lopez-Mattei, J.; Mitchell, J.D. Past, Present, and Future of Radiation-Induced Cardiotoxicity: Refinements in Targeting, Surveillance, and Risk Stratification. JACC CardioOncol. 2021, 3, 343–359. [Google Scholar] [CrossRef] [PubMed]
- Annest, L.S.; Anderson, R.P.; Li, W.; Hafermann, M.D. Coronary artery disease following mediastinal radiation therapy. J. Thorac. Cardiovasc. Surg. 1983, 85, 257–263. [Google Scholar] [CrossRef]
- Wagner, A.D.; Oertelt-Prigione, S.; Adjei, A.; Buclin, T.; Cristina, V.; Csajka, C.; Coukos, G.; Dafni, U.; Dotto, G.-P.; Ducreux, M.; et al. Gender medicine and oncology: Report and consensus of an ESMO workshop. Ann. Oncol. 2019, 30, 1914–1924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inker, L.A.; Schmid, C.H.; Tighiouart, H.; Eckfeldt, J.H.; Feldman, H.I.; Greene, T.; Kusek, J.W.; Manzi, J.; Van Lente, F.; Zhang, Y.L.; et al. Estimating Glomerular Filtration Rate from Serum Creatinine and Cystatin C. N. Engl. J. Med. 2012, 367, 20–29. [Google Scholar] [CrossRef] [Green Version]
- Nanda, A.; Chen, M.-H.; Braccioforte, M.H.; Moran, B.J.; D’Amico, A.V. Hormonal Therapy Use for Prostate Cancer and Mortality in Men With Coronary Artery Disease–Induced Congestive Heart Failure or Myocardial Infarction. JAMA 2009, 302, 866–873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziehr, D.R.; Chen, M.-H.; Zhang, D.; Braccioforte, M.H.; Moran, B.J.; Mahal, B.A.; Hyatt, A.S.; Basaria, S.S.; Beard, C.J.; Beckman, J.A.; et al. Association of androgen-deprivation therapy with excess cardiac-specific mortality in men with prostate cancer. BJU Int. 2015, 116, 358–365. [Google Scholar] [CrossRef] [Green Version]
- Fizazi, K.; Shore, N.; Tammela, T.L.; Ulys, A.; Vjaters, E.; Polyakov, S.; Jievaltas, M.; Luz, M.; Alekseev, B.; Kuss, I.; et al. ARAMIS Investigators. Darolutamide in Nonmetastatic, Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2019, 380, 1235–1246. [Google Scholar] [CrossRef]
- Di Nunno, V.; Mollica, V.; Santoni, M.; Gatto, L.; Schiavina, R.; Fiorentino, M.; Brunocilla, E.; Ardizzoni, A.; Massari, F. New Hormonal Agents in Patients With Nonmetastatic Castration-Resistant Prostate Cancer: Meta-Analysis of Efficacy and Safety Outcomes. Clin. Genitourin. Cancer 2019, 17, e871–e877. [Google Scholar] [CrossRef]
- Morgans, A.K.; Shore, N.; Cope, D.; McNatty, A.; Moslehi, J.; Gomella, L.; Sartor, O. Androgen receptor inhibitor treatments: Cardiovascular adverse events and comorbidity considerations in patients with non-metastatic prostate cancer. Urol. Oncol. 2021, 39, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.-R.; Duncan, M.S.; Morgans, A.K.; Brown, J.D.; Meijers, W.C.; Freiberg, M.S.; Salem, J.-E.; Beckman, J.A.; Moslehi, J.J. Cardiovascular Effects of Androgen Deprivation Therapy in Prostate Cancer: Contemporary Meta-Analyses. Arter. Thromb. Vasc. Biol. 2020, 40, e55–e64. [Google Scholar] [CrossRef]
- Jafri, M.; Protheroe, A. Cisplatin-associated thrombosis. Anti-Cancer Drugs 2008, 19, 927–929. [Google Scholar] [CrossRef]
- Polk, A.; Vaage-Nilsen, M.; Vistisen, K.; Nielsen, D.L. Cardiotoxicity in cancer patients treated with 5-fluorouracil or cape-citabine: A systematic review of incidence, manifestations and predisposing factors. Cancer Treat. Rev. 2013, 39, 974–984. [Google Scholar] [CrossRef]
- Amir, E.; Seruga, B.; Niraula, S.; Carlsson, L.; Ocana, A. Toxicity of Adjuvant Endocrine Therapy in Postmenopausal Breast Cancer Patients: A Systematic Review and Meta-analysis. J. Natl. Cancer Inst. 2011, 103, 1299–1309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mueller, F.; Büchel, B.; Köberle, D.; Schürch, S.; Pfister, B.; Krähenbühl, S.; Froehlich, T.K.; Largiader, C.R.; Joerger, M. Gender-specific elimination of continuous-infusional 5-fluorouracil in patients with gastrointestinal malignancies: Results from a prospective population pharmacokinetic study. Cancer Chemother. Pharmacol. 2013, 71, 361–370. [Google Scholar] [CrossRef]
- Khosrow-Khavar, F.; Filion, K.; Al-Qurashi, S.; Torabi, N.; Bouganim, N.; Suissa, S.; Azoulay, L. Cardiotoxicity of aromatase inhibitors and tamoxifen in postmenopausal women with breast cancer: A systematic review and meta-analysis of randomized controlled trials. Ann. Oncol. 2017, 28, 487–496. [Google Scholar] [CrossRef]
- Totzeck, M.; Mincu, R.I.; Rassaf, T. Cardiovascular Adverse Events in Patients With Cancer Treated With Bevacizumab: A Meta-Analysis of More Than 20 000 Patients. J. Am. Heart Assoc. 2017, 6, 006278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, L.J.; Meredith, T.; Yu, J.; Patel, A.; Neal, B.; Arnott, C.; Lim, E. Heart Failure Therapies for the Prevention of HER2-Monoclonal Antibody-Mediated Cardiotoxicity: A Systematic Review and Meta-Analysis of Randomized Trials. Cancers 2021, 13, 5527. [Google Scholar] [CrossRef]
- Escalante, C.P.; Chang, Y.C.; Liao, K.; Rouleau, T.; Halm, J.; Bossi, P.; Bhadriraju, S.; Brito-Dellan, N.; Sahai, S.; Yusuf, S.W.; et al. Epidemiology Section of the Mucositis Study Group of the Multinational Association of Supportive Care in Cancer, 2013. Meta-analysis of cardiovascular toxicity risks in cancer patients on selected targeted agents. Support. Care Cancer 2016, 24, 4057–4074. [Google Scholar] [CrossRef] [PubMed]
- Schmoll, H.-J.; Twelves, C.; Sun, W.; O’Connell, M.J.; Cartwright, T.; McKenna, E.; Saif, M.; Lee, S.; Yothers, G.; Haller, D. Effect of adjuvant capecitabine or fluorouracil, with or without oxaliplatin, on survival outcomes in stage III colon cancer and the effect of oxaliplatin on post-relapse survival: A pooled analysis of individual patient data from four randomised controlled trials. Lancet Oncol. 2014, 15, 1481–1492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weidner, K.; Behnes, M.; Haas, J.; Rusnak, J.; Fuerner, P.; Kuska, M.; Mukherji, A.; Borggrefe, M.; Hofheinz, R.-D.; Akin, I. Oxaliplatin-Induced Acute ST Segment Elevation Mimicking Myocardial Infarction: A Case Report. Oncol. Res. Treat. 2018, 41, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Groehs, R.V.; Negrao, M.V.; Hajjar, L.A.; Jordão, C.P.; Carvalho, B.P.; Toschi-Dias, E.; Andrade, A.C.; Hodas, F.P.; Alves, M.J.N.N.; Sarmento, A.O.; et al. Adjuvant Treatment with 5-Fluorouracil and Oxaliplatin Does Not Influence Cardiac Func-tion, Neurovascular Control, and Physical Capacity in Patients with Colon Cancer. Oncologist 2020, 25, e1956–e1967. [Google Scholar] [CrossRef]
- O’Rourke, N.; Roqué, I.; Figuls, M.; Farré Bernadó, N.; Macbeth, F. Concurrent chemoradiotherapy in non-small cell lung cancer. Cochrane Database Syst. Rev. 2010, 6, 002140. [Google Scholar] [CrossRef]
- Dugbartey, G.J.; Peppone, L.J.; de Graaf, I.A. An integrative view of cisplatin-induced renal and cardiac toxicities: Molecular mechanisms, current treatment challenges and potential protective measures. Toxicology 2016, 371, 58–66. [Google Scholar] [CrossRef] [Green Version]
- Shah, K.; Gupta, S.; Ghosh, J.; Bajpai, J.; Maheshwari, A. Acute non-ST elevation myocardial infarction following paclitaxel administration for ovarian carcinoma: A case report and review of literature. J. Cancer Res. Ther. 2012, 8, 442–444. [Google Scholar] [CrossRef]
- Schwarzer, S.; Eber, B.; Greinix, H.; Lind, P. Non-Q-wave myocardial infarction associated with bleomycin and etoposide chemotherapy. Eur. Heart J. 1991, 12, 748–750. [Google Scholar]
- Zerna, C.; Guenther, M.; Folprecht, G.; Puetz, V. Acute ischaemic stroke and myocardial infarction after chemotherapy with vinorelbine for non-small cell lung cancer: A case report. J. Chemother. 2017, 29, 49–53. [Google Scholar] [CrossRef]
- Bergeron, A.; Raffy, O.; Vannetzel, J.M. Myocardial ischemia and infarction associated with vinorelbine. J. Clin. Oncol. 1995, 13, 531–532. [Google Scholar] [CrossRef]
- Zabernigg, A.; Gattringer, C. Myocardial infarction associated with vinorelbine (Navelbine). Eur. J. Cancer 1996, 32, 1618–1619. [Google Scholar] [CrossRef]
- Duvic, M.; Talpur, R.; Wen, S.; Kurzrock, R.; David, C.L.; Apisarnthanarax, N. Phase II evaluation of gemcitabine mono-therapy for cutaneous T-cell lymphoma. Clin. Lymphoma Myeloma 2006, 7, 51–58. [Google Scholar] [CrossRef]
- Kalapura, T.; Krishnamurthy, M.; Reddy, C.V. Acute myocardial infarction following gemcitabine therapy—A case report. Angiology 1999, 50, 1021–1025. [Google Scholar] [CrossRef]
- Ng, K.H.; Dearden, C.; Gruber, P. Rituximab-induced Takotsubo syndrome: More cardiotoxic than it appears? BMJ Case Rep. 2015, 2015, bcr2014208203. [Google Scholar] [CrossRef]
- Varga, A.; Tilea, I.; Petra, D.N.; Tilinca, M.-C.; Gliga, M.L.; Demian, S. Cardiovascular Events throughout the Disease Course in Chronic Myeloid Leukaemia Patients Treated with Tyrosine Kinase Inhibitors—A Single-Centre Retrospective Study. J. Clin. Med. 2020, 9, 3269. [Google Scholar] [CrossRef]
- Vener, C.; Banzi, R.; Ambrogi, F.; Ferrero, A.; Saglio, G.; Pravettoni, G.; Sant, M. First-line imatinib vs second- and third-generation TKIs for chronic-phase CML: A systematic review and meta-analysis. Blood Adv. 2020, 4, 2723–2735. [Google Scholar] [CrossRef] [PubMed]
- Bikiewicz, A.; Banach, M.; von Haehling, S.; Maciejewski, M.; Bielecka-Dabrowa, A. Adjuvant breast cancer treatments car-diotoxicity and modern methods of detection and prevention of cardiac complications. ESC Heart Fail. 2021, 8, 2397–2418. [Google Scholar] [PubMed]
- Nathan, S.; Rao, S.V. Radial versus femoral access for percutaneous coronary intervention: Implications for vascular com-plications and bleeding. Curr. Cardiol. Rep. 2012, 14, 502–509. [Google Scholar] [CrossRef]
- Iliescu, C.A.; Grines, C.L.; Herrmann, J.; Yang, E.H.; Cilingiroglu, M.; Charitakis, K.; Hakeem, A.; Toutouzas, K.P.; Leesar, M.A.; Marmagkiolis, K. SCAI Expert consensus statement: Evaluation, management, and special considerations of car-dio-oncology patients in the cardiac catheterization laboratory (endorsed by the cardiological society of india, and sociedad Latino Americana de Cardiologıa intervencionista). Catheter. Cardiovasc. Interv. 2016, 87, E202–E223. [Google Scholar]
- Urban, P.; Meredith, I.T.; Abizaid, A.; Pocock, S.J.; Carrié, D.; Naber, C.; Lipiecki, J.; Richardt, G.; Iñiguez, A.; Brunel, P.; et al. LEADERS FREE Investigators.Polymer-free Drug-Coated Coronary Stents in Patients at High Bleeding Risk. N. Engl. J. Med. 2015, 373, 2038–2047. [Google Scholar]
- Windecker, S.; Latib, A.; Kedhi, E.; Kirtane, A.J.; Kandzari, D.E.; Mehran, R.; Price, M.J.; Abizaid, A.; Simon, D.I.; Worthley, S.G.; et al. ONYX ONE Investigators. Polymer-based or Polymer-free Stents in Patients at High Bleeding Risk. N. Engl. J. Med. 2020, 382, 1208–1218. [Google Scholar] [CrossRef]
- Benenati, S.; Crimi, G.; Canale, C.; Pescetelli, F.; De Marzo, V.; Vergallo, R.; Galli, M.; Della Bona, R.; Canepa, M.; Ameri, P.; et al. Duration of dual antiplatelet therapy and subsequent monotherapy type in patients undergoing drug eluting stent im-plantation: A network Meta-analysis. Eur. Heart J. Cardiovasc. Pharmacother. 2022, 8, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Shen, Y.; Chen, D.; Zhao, P.; Jiang, J. Efficacy and Safety of Dual Antiplatelet Therapy in Patients Undergoing Coronary Stent Implantation: A Systematic Review and Network Meta-Analysis. J. Interv. Cardiol. 2021, 2021, 9934535. [Google Scholar] [CrossRef] [PubMed]
- Mehran, R.; Baber, U.; Sharma, S.K.; Cohen, D.J.; Angiolillo, D.J.; Briguori, C.; Cha, J.Y.; Collier, T.; Dangas, G.; Dudek, D.; et al. Ticagrelor with or without Aspirin in High-Risk Patients after PCI. N. Engl. J. Med. 2019, 381, 2032–2042. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.W.; Lam, S.C.; Tam, F.C.; Chan, K.K.; Shea, C.P.; Kong, S.L.; Wong, A.Y.; Yung, A.; Zhang, L.W.; Tse, H.-F.; et al. A. Evaluation of early healing profile and neointimal transformation over 24 months using longitudinal sequential optical coherence tomography assessments and 3-year clinical results of the new dual-therapy endothelial progenitor cell capturing sirolimus-eluting combo stent: The EGO-Combo study. Circ. Cardiovasc. Interv. 2016, 9, e003469. [Google Scholar] [PubMed]
- Chevalier, B.; Smits, P.C.; Carrié, D.; Mehilli, J.; Van Boven, A.J.; Regar, E.; Sawaya, F.J.; Chamié, D.; Kraaijeveld, A.O.; Hovasse, T.; et al. Serial Assessment of Strut Coverage of Biodegradable Polymer Drug-Eluting Stent at 1, 2, and 3 Months After Stent Implantation by Optical Frequency Domain Imaging: The DISCOVERY 1TO3 Study (Evaluation With OFDI of Strut Coverage of Terumo New Drug Eluting Stent with Biodegradable Polymer at 1, 2, and 3 Months). Circ. Cardiovasc. Interv. 2017, 10, e004801. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| Author | Year | Study Design | Pat. (n) | ACS/AMI/STEMI | NPL | PCI | Period | Endpoints |
|---|---|---|---|---|---|---|---|---|
| Guddati et al. [12] | 2016 | retrospective registry study, US National Inpatient Database | 49,515 | 100%/67.76%/32.24% | 100% (metastatic disease) | STEMI 24.9%; NSTEMI 9.6% | 2000–2009 | in-hospital mortality, length of hospital stay and discharge disposition |
| Park et al. [13] | 2019 | retrospective register study | 5300 | 1.4%/1.075%/0.189% | 100%, hematol. Malign. | 35.3% | 2004–2014 | Mortality in-hospital, year 1 |
| Mohamed et al. [14] | 2020 | registry study | 6,750,878 | n.i./100%/35.1% | 100%, leukaemia | 42.9% vs. 28.2% w. leukemia | 2004–2014 | MACCE and bleeding |
| Nardi Agmon et al. [15] | 2021 | single center | 3286 | 60%/-/- | 100% | 55%/45% | 1. 2006–2011 2. 2012–2017 | MACE all-cause mortality |
| 6,808,979 | ||||||||
| Kurisu et al. [16] | 2012 | retrospective, single center | 77 | AMI 100% | 23% | 100% | 2006–2011 | all-cause death year 1 |
| Velders et al. [17] | 2013 | multicenter, registry study | 3423 | 0%/0%/100% | 6.1% | 100% | 2006–2009 | all-cause, cardiac mortality year 1 |
| Wang et al. [18] | 2016 | retrospective cohort study | 2346 | n.i./n.i./100% | 11.1% | 100% | 2000–2010 | in-hospital and long-term mortality |
| Landes et al. [19] | 2017 | retrospective registry study | 12,785 | n.i. | 7.8% | 100% | 2004–2014 | all-cause mortality composite of death, nonfatal mi, target vessel revasc, CABG |
| Nakatsuma et al. [20] | 2018 | registry study | 12,180 | AMI w/o: 36%/C: 29% | 9.1% | 100% | 2005–2007 | all-cause death cardiac death, non-cardiac death, heart failure hospitalization, major bleeding, non-CABG surgery, myocardial infarction, definite or probable stent thrombosis, stroke, TLR, any coronary revascularization |
| Iannaccone et al. [21] | 2018 | multicenter observational prospective registry; substudy, BleeMACS project | 15,401 | w/o: 13.2%/28.4%/58.4% C: 16.2%/32.5%/51.3% | 6.4% | 100% | n.a. | composite event of death and re-infarction y1 bleeding events during follow-up |
| Potts et al. [7] | 2019 | registry study | 6,571,034 | n.i./41.05%/22.84%/ 22.95% (NSTEMI) | 1.8% curr., 5.8% prev. C. | 100% | 2004–2014 | Mortality in-hospital in-hospital complication |
| Gaddam et al. [22] | 2020 | retrospective cross-sectional study | 1,131,415 | n.i. | 1.27% | 100% | 2012–2014 | risk of association between comorbid cancer and in-hospital mortality in post-PCI inpatients |
| Kwok et al. [23] | 2021 | register study | 1,933,324 | n.i. | 9.5% | 100% | 2010–2014 | 90-day readmission for AMI 90-day readmission for bleeding |
| Takeuchi et al. [24] | 2021 | retrospective, registry study, OASIS | 3499 | n.i./100%/87.4% | 13.2% | 100% | 1998–2014 | Death from cancer, death from cardiac and other causes |
| 9,685,484 | ||||||||
| Pothineni et al. [25] | 2017 | registry study | 3,794,385 | n.i./n.i./100% | 1.29% (breast 0.15%, lung 0.82%, colon 0.32%) | 46.32% (30.8%, 20.2%, 17.3%) | 2001–2011 | percutaneous coronary intervention (PCI), and in-hospital outcomes in patients |
| Gong et al. [26] | 2018 | registry study, observational | 270,089 | n.i./100%/n.i. | 8.48% | w/o vs. w C: 1995, 5.1% vs. 4.3%; 2013, 58.4% vs. 54.4% | 1995–2013 | Mortality day 30, year1; all-cause mortality overall heart failure, overall myocardial reinfarction, overall stroke |
| Rohrmann et al. [11] | 2018 | Multicenter, propensity score matching, AMIS Plus registry | 35,249 | w/o: 58.1% C: 52.1% STEMI | 5.6% | 73.4% w/o vs. 67.8% w Cancer | 2002-mid 2015 | In-hospital outcome |
| Ederhy et al. [27] | 2019 | registry study, pospective | 3664 | n.i./100%/51.34% | 6.7% | 64.6% w/o, 51.6% w Cancer | 2005 | 5-years mortality |
| Velders et al. [3] | 2020 | registry study | 175,146 | n.i./100%/35.6% | 9.3% | 48% | 2001–2014 | All-cause mortality |
| Bharadwaj et al. [28] | 2020 | registry study | 6,563,255 | n.i./100%/36%, 29% | 2.8% curr, 6.2% prev C. | 43.9% w/o, 21.0% w Cancer | 2004–2014 | In-hospital mortality and adverse events (MACCE, Bleeding, Stroke) |
| 10,841,788 |
| Treatment | Prostate Cancer | Breast Cancer | Colon Cancer | Lung Cancer | Leukemia | No Cancer |
|---|---|---|---|---|---|---|
| Coronarangiography (%) | 47.5 | 47.0 | 44.7 | 34.8 | 48.5 | 64.5–65.2 |
| PCI (%) | 29.3 | 27.4 | 27.6 | 21.0 | 28.2 | 42.9–43.9 |
| DES (%) | 63.3/73.0 * | 57.1/73.1 * | 38.4/68.9 * | 39.3/67.1 * | n.a. | 73.7 |
| BMS (%) | 31.5/23.0 * | 36.1/22.4 * | 46.8/26.8 * | 49.6/27.6 * | n.a. | 21.6 |
| CABG (%) | 6.7 | 4.2 | 5.1 | 2.3 | 6.9 | 8.9–9.1 |
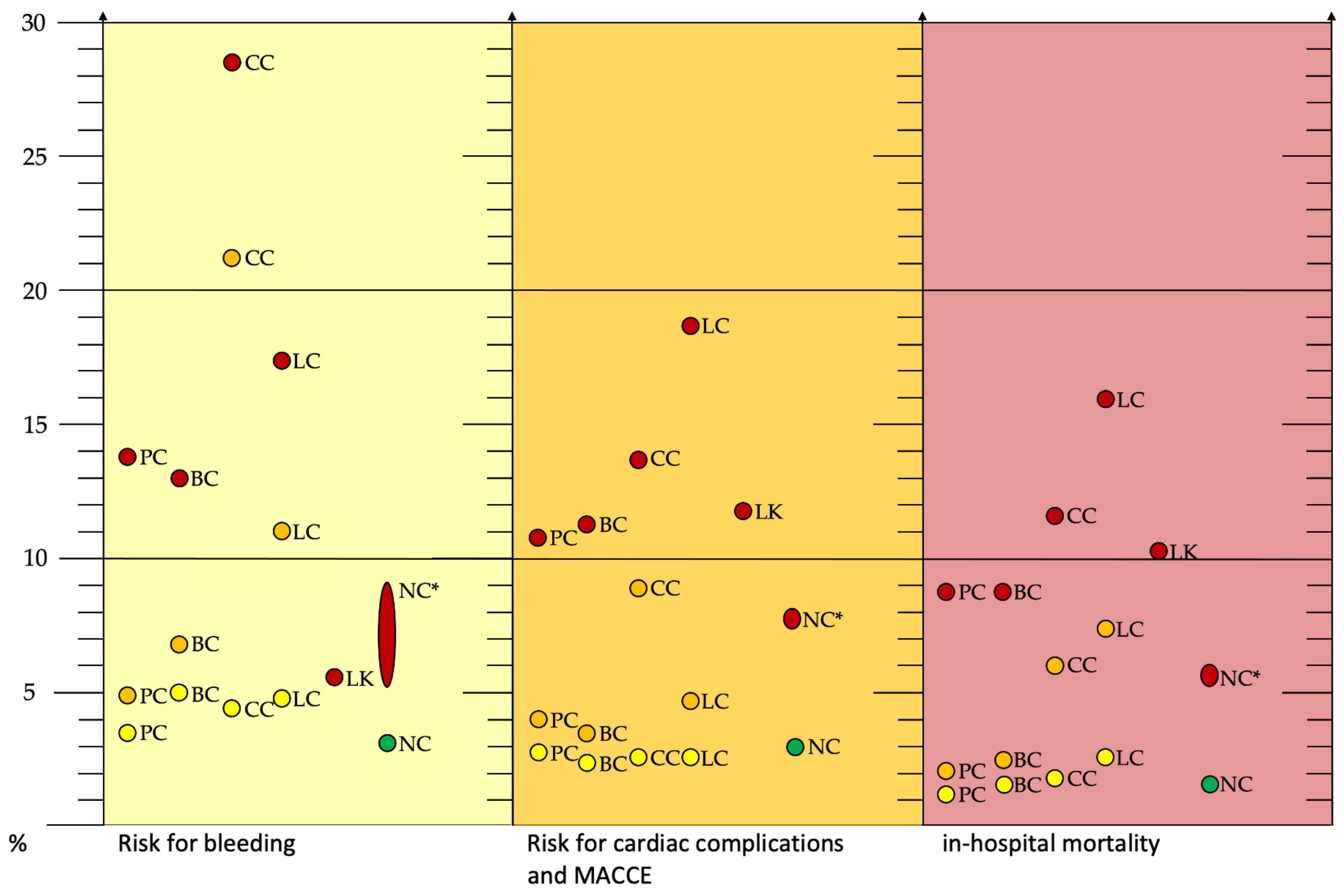
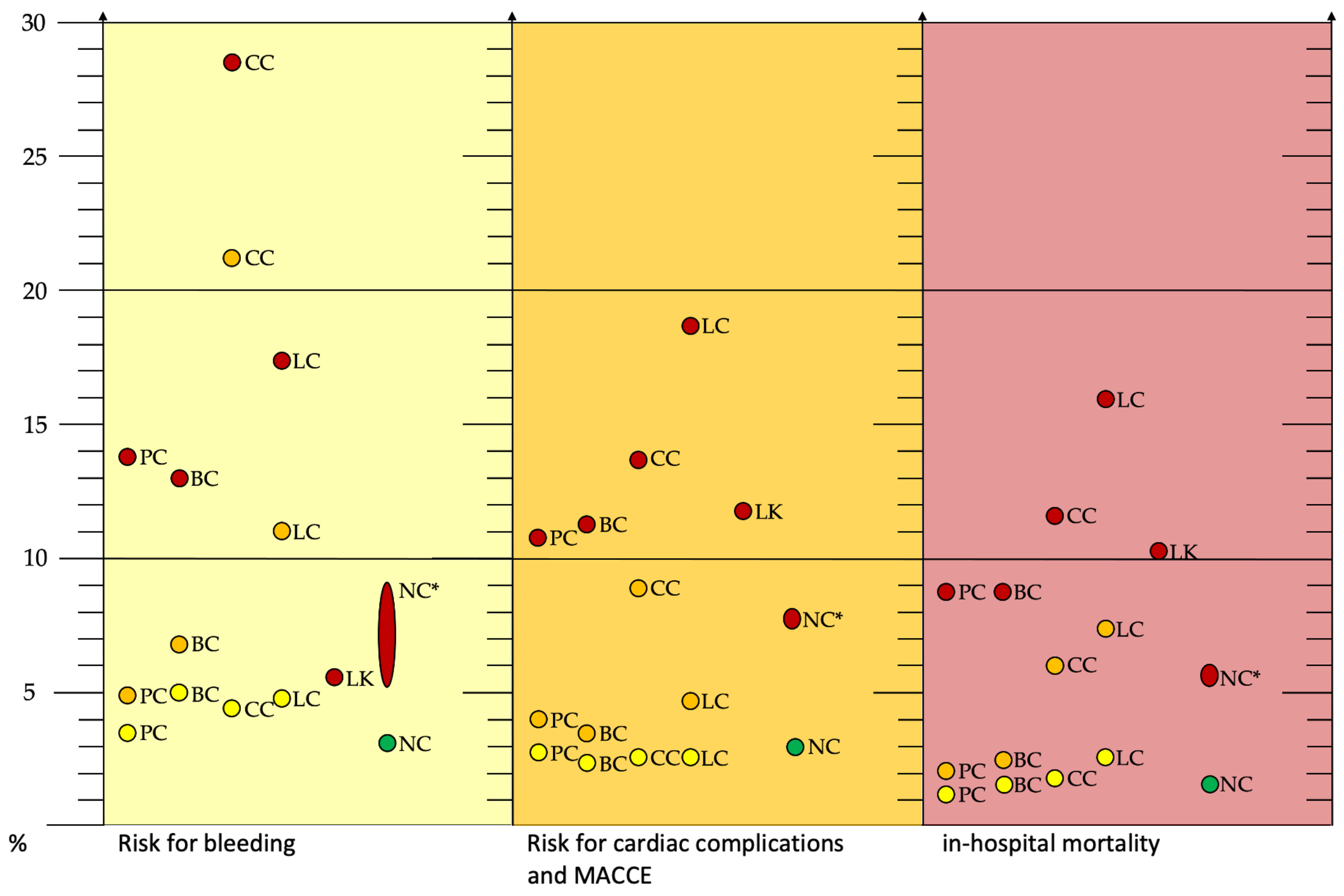
| Treatment | Prostate Cancer | Breast Cancer | Colon Cancer | Lung Cancer | Leukemia ¢ | No Cancer |
|---|---|---|---|---|---|---|
| PCI in | CC/HC/AMI | CC/HC/AMI | CC/HC/AMI | CC/HC/AMI | AMI | No C/AMI |
| In-hospital mortality (%) | 2.1/1.2/8.7 | 2.5/1.6/8.7 | 4.8/1.8/11.6 | 7.4/2.6/15.9 | 10.3 | 1.6/5.7 n.a./5.8 ¢ |
| Any complication (%) | 11.6/9.2/n.a. | 13.7/10.8/n.a. | 30.2/10.5/n.a. | 19.1/11.0/n.a. | n.a. | 8.8/n.a. |
| Bleeding (%) | 4.9/3.5/13.8 | 6.8/5.0/13.0 | 21.2/4.5/28.5 | 11.0/4.8/17.4 | 5.6 | 3.1/8.8 n.a./5.3 ¢ |
| Vascular complication (%) | 0.9/0.8/n.a. | 0.7/1.2/n.a. | 2.0/0.9/n.a. | 1.2/0.8/n.a. | n.a. | 1.0/n.a. |
| Cardiac complications/#MACCE (%) | 4.0/2.8/10.7 # | 3.5/2.4/11.3 # | 8.8/2.6/13.7 # | 4.7/2.6%18.7 # | 0.5/11.8 # | 3.0/7.7 # n.a./0.7/7.8 #¢ |
| Stroke (%) | 3.3/3.3/1.9 | 4.2/3.6/2.4 | 2.8/3.7/2.1 | 4.7/3.9/3.5 | 1.4 | 2.8/1.7 n.a./1.7 ¢ |
| Platelet Count | Additional Considerations | Recommendations |
|---|---|---|
| >50,000/mL |
| |
| <50,000/mL |
| |
| 30,000–50,000/mL |
| |
| <30,000/mL |
| |
| <20,000/mL |
|
|
In solid tumor patients receiving therapy for
| ||
| <10,000/mL | Aspirin administration should be avoided |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lange, S.A.; Reinecke, H. Coronary Artery Disease and Cancer: Treatment and Prognosis Regarding Gender Differences. Cancers 2022, 14, 434. https://doi.org/10.3390/cancers14020434
Lange SA, Reinecke H. Coronary Artery Disease and Cancer: Treatment and Prognosis Regarding Gender Differences. Cancers. 2022; 14(2):434. https://doi.org/10.3390/cancers14020434
Chicago/Turabian StyleLange, Stefan A., and Holger Reinecke. 2022. "Coronary Artery Disease and Cancer: Treatment and Prognosis Regarding Gender Differences" Cancers 14, no. 2: 434. https://doi.org/10.3390/cancers14020434
APA StyleLange, S. A., & Reinecke, H. (2022). Coronary Artery Disease and Cancer: Treatment and Prognosis Regarding Gender Differences. Cancers, 14(2), 434. https://doi.org/10.3390/cancers14020434