
Blinatumomab in Children and Adolescents with Relapsed/Refractory B Cell Precursor Acute Lymphoblastic Leukemia: A Real-Life Multicenter Retrospective Study in Seven AIEOP (Associazione Italiana di Ematologia e Oncologia Pediatrica) Centers

 , , ,
, , ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Study Population
3.2. Safety Profile
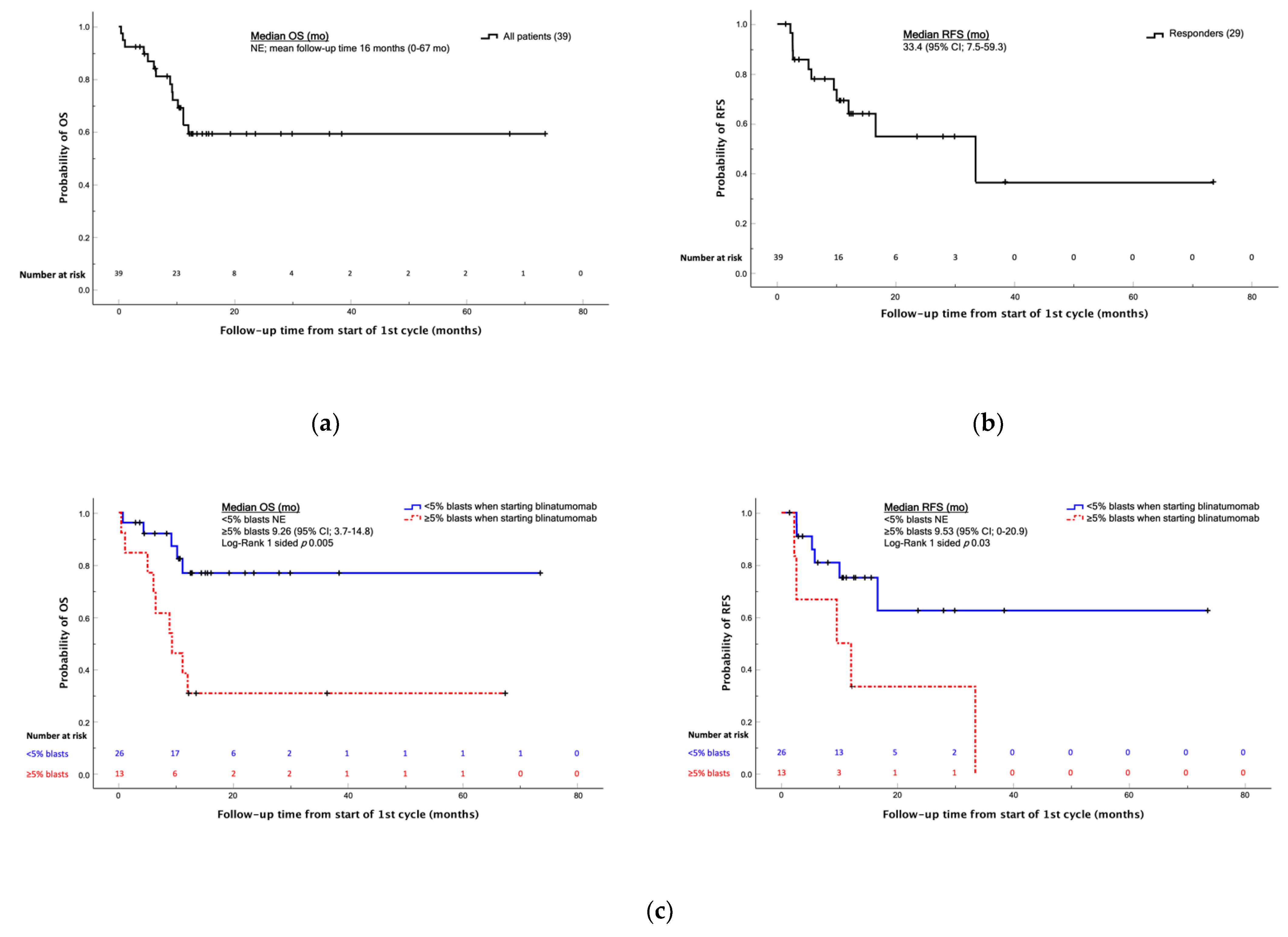
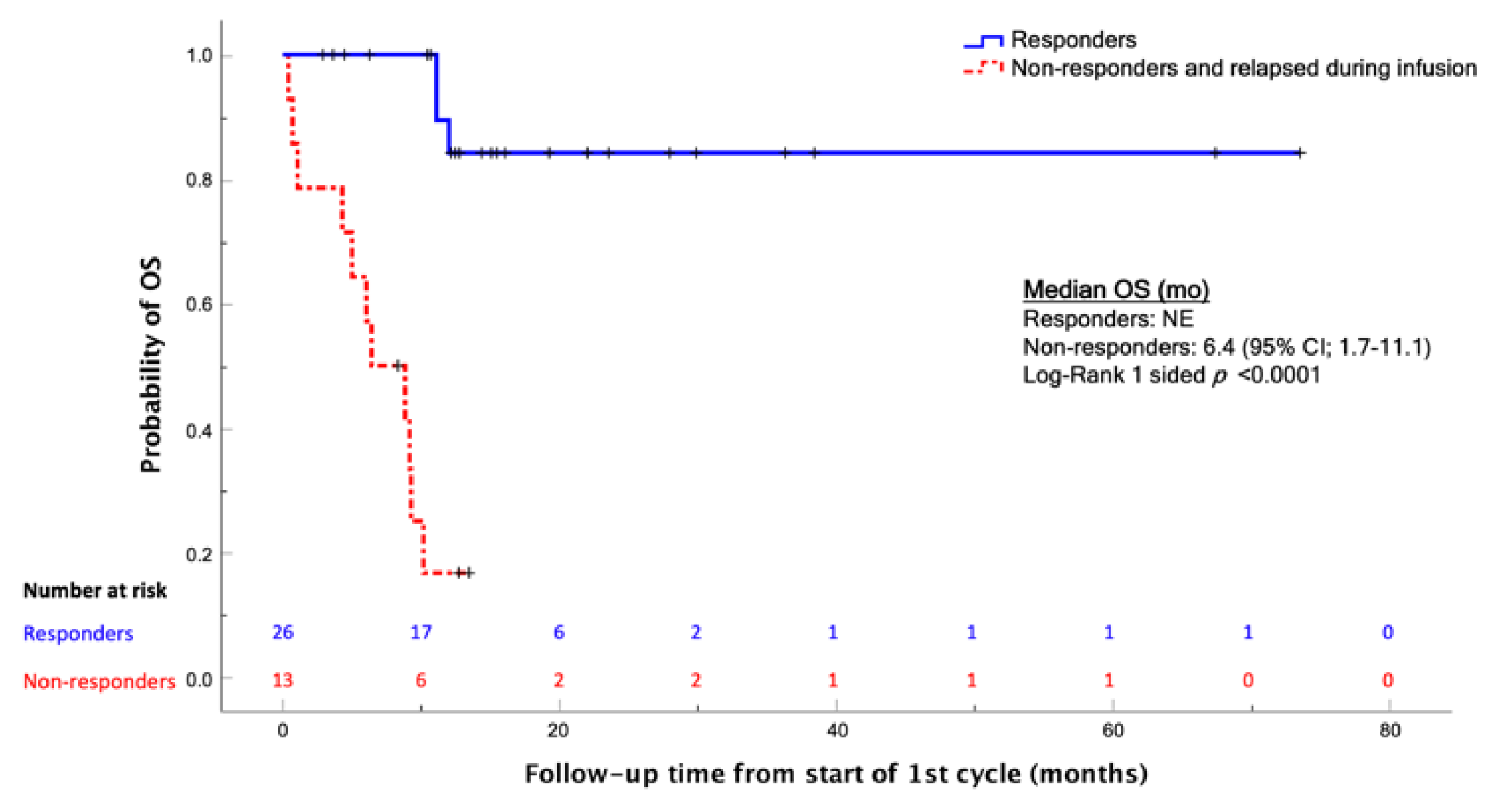
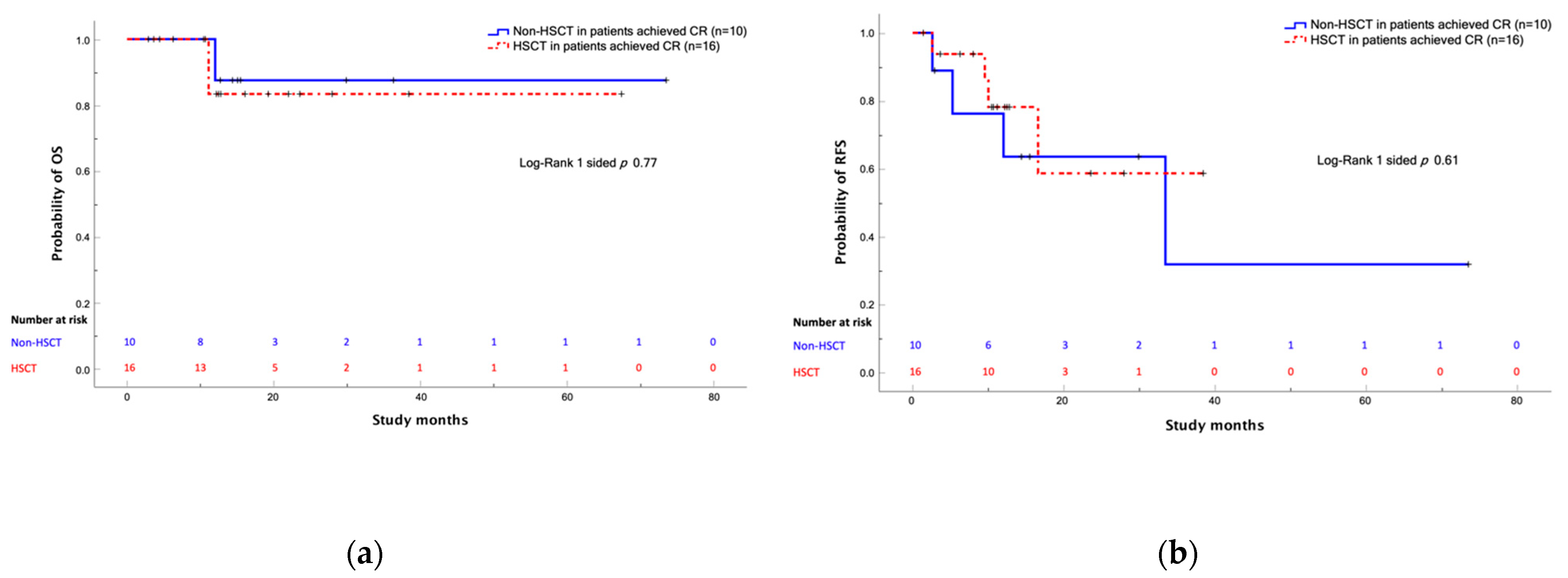
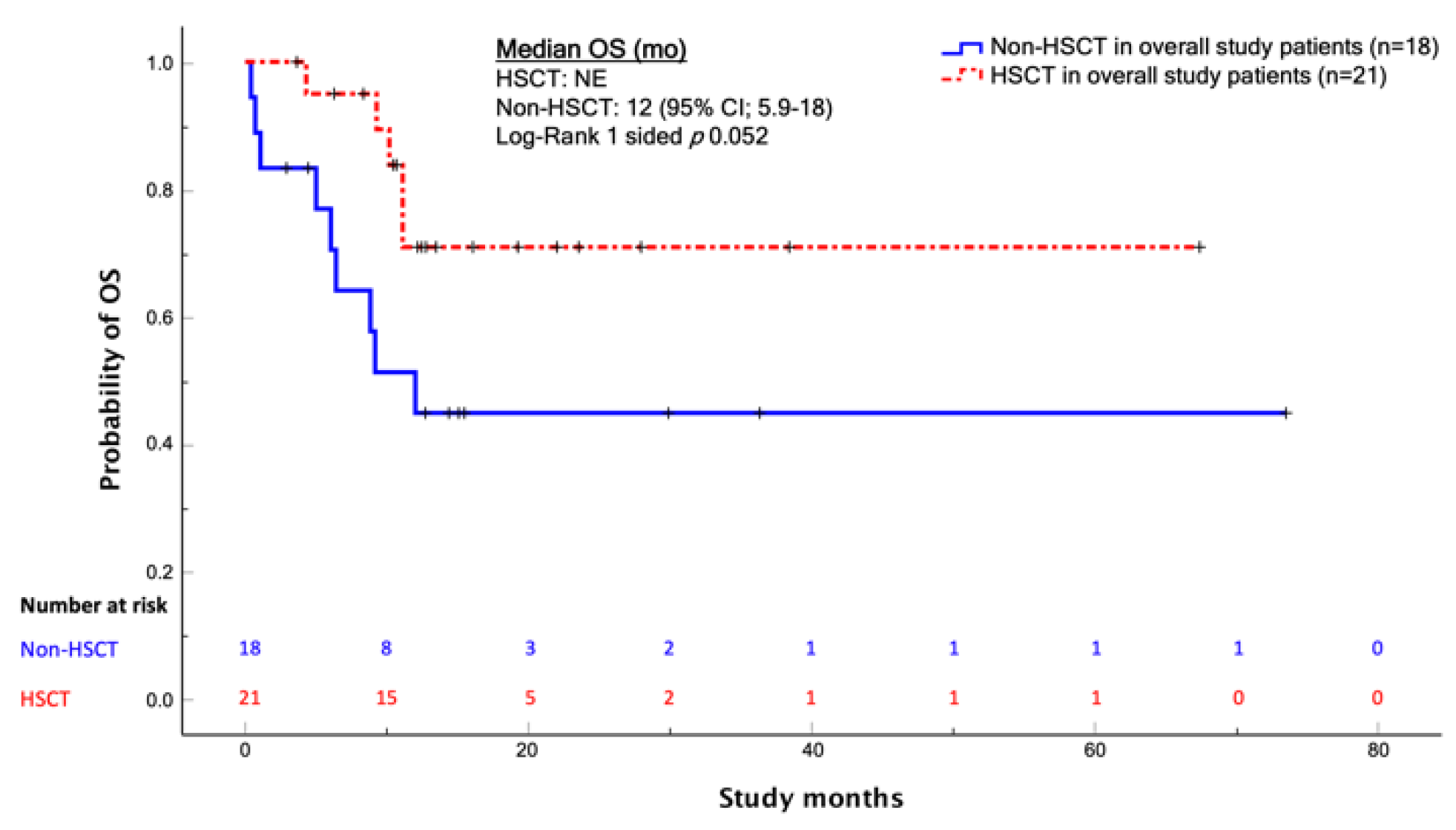
3.3. Treatment Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hunger, S.P.; Mullighan, C.G. Acute Lymphoblastic Leukemia in Children. N. Engl. J. Med. 2015, 373, 1541–1552. [Google Scholar] [CrossRef] [Green Version]
- Inaba, H.; Mullighan, C.G. Pediatric acute lymphoblasticleukemia. Haematologica 2020, 105, 2524–2539. [Google Scholar] [CrossRef]
- Bhojwani, D.; Pui, C.H. Relapsed childhood acute lymphoblastic leukaemia. Lancet Oncol. 2013, 14, e205–e217. [Google Scholar] [CrossRef]
- Locatelli, F.; Schrappe, M.; Bernardo, M.E.; Rutella, S. How I treat relapsed childhood acute lymphoblastic leukemia. Blood 2012, 120, 2807–2816. [Google Scholar] [CrossRef] [Green Version]
- Hunger, S.P.; Raetz, E.A. How I treat relapsed acute lymphoblastic leukemia in the pediatric population. Blood 2020, 136, 1803–1812. [Google Scholar] [CrossRef] [PubMed]
- Karol, S.E.; Pui, C.H. Personalized therapy in pediatric high-risk B-cell acute lymphoblastic leukemia. Ther. Adv. Hematol. 2020, 11, 1–16. [Google Scholar] [CrossRef]
- Inaba, H.; Pui, C. Immunotherapy in pediatric acute lymphoblastic leukemia. Cancer Metastasis Rev. 2019, 38, 595–610. [Google Scholar] [CrossRef]
- Pui, C.H. Precision medicine in acute lymphoblastic leukemia. Front. Med. 2020, 14, 689–700. [Google Scholar] [CrossRef]
- Brischwein, K.; Schlereth, B.; Guller, B.; Steiger, C.; Wolf, R.; Lutterbuese, R.; Offner, S.; Locher, M.; Urbig, T.; Raum, T.; et al. MT110: A novel bispecific single-chain antibody construct with high efficacy in eradicating established tumors. Mol. Immunol. 2006, 43, 1129–1143. [Google Scholar] [CrossRef] [PubMed]
- Topp, M.S.; Gökbuget, N.; Zugmaier, G.; Klappers, P.; Stelljes, M.; Neumann, S.; Viardot, A.; Marks, R.; Diedrich, H.; Faul, C.; et al. Phase II trial of the anti-CD19 bispecific T cell-engager blinatumomab shows hematologic and molecular remissions in patients with relapsed or refractory B-precursor acute lymphoblastic leukemia. J. Clin. Oncol. 2014, 32, 4134–4140. [Google Scholar] [CrossRef]
- Topp, M.S.; Gökbuget, N.; Stein, A.S.; Zugmaier, G.; O’Brien, S.; Bargou, R.C.; Dombret, H.; Fielding, A.K.; Heffner, L.; Larson, R.A.; et al. Safety and activity of blinatumomab for adult patients with relapsed or refractory B-precursor acute lymphoblastic leukaemia: A multicentre, single-arm, phase 2 study. Lancet Oncol. 2015, 16, 57–66. [Google Scholar] [CrossRef]
- Kantarjian, H.; Stein, A.; Gokbuget, N.; Fielding, A.K.; Schuh, A.C.; Ribera, J.M.; Wei, A.; Dombret, H.; Foà, R.; Bassan, R.; et al. Blinatumomab versus Chemotherapy for Advanced Acute Lymphoblastic Leukemia. N. Engl. J. Med. 2017, 376, 836–847. [Google Scholar] [CrossRef] [PubMed]
- Gokbuget, N.; Dombret, H.; Bonifacio, M.; Reichle, A.; Graux, C.; Faul, C.; Diedrich, H.; Topp, M.S.; Brüggemann, M.; Horst, H.A.; et al. Blinatumomab for minimal residual disease in adults with B-cell precursor acute lymphoblastic leukemia. Blood 2018, 131, 1522–1531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pulte, E.D.; Vallejo, J.; Przepiorka, D.; Nie, L.; Farrell, A.T.; Goldberg, K.B.; McKee, A.E.; Pazdur, R. FDA Supplemental Approval: Blinatumomab for Treatment of Relapsed and Refractory Precursor B-Cell Acute Lymphoblastic Leukemia. Oncologist 2018, 23, 1366–1371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinelli, G.; Boissel, N.; Chevallier, P.; Ottmann, O.; Gökbuget, N.; Topp, M.S.; Fielding, A.K.; Rambaldi, A.; Ritchie, E.K.; Papayannidis, C.; et al. Complete Hematologic and Molecular Response in Adult Patients With Relapsed/Refractory Philadelphia Chromosome-Positive B-Precursor Acute Lymphoblastic Leukemia Following Treatment with Blinatumomab: Results From a Phase II, Single-Arm, Multicenter Study. J. Clin. Oncol. 2017, 35, 1795–1802. [Google Scholar] [CrossRef]
- Queudeville, M.; Schlegel, P.; Heinz, A.T.; Lenz, T.; Döring, M.; Holzer, U.; Hartmann, U.; Kreyenberg, H.; von Stackelberg, A.; Schrappe, M.; et al. Blinatumomab in pediatric patients with relapsed/refractory B-cell precursor acute lymphoblastic leukemia. Eur. J. Haematol. 2021, 106, 473–483. [Google Scholar] [CrossRef]
- Algeri, M.; Del Bufalo, F.; Galaverna, F.; Locatelli, F. Current and future role of bispecific T-cell engagers in pediatric acute lymphoblastic leukemia. Expert. Rev. Hematol. 2018, 11, 945–956. [Google Scholar] [CrossRef]
- Shukla, N.; Sulis, M.L. Blinatumomab for Treatment of Children with High-risk Relapsed B-Cell Acute Lymphoblastic Leukemia. JAMA 2021, 325, 830–832. [Google Scholar] [CrossRef]
- Hoffman, L.M.; Gore, L. Blinatumomab, a Bi-Specific Anti-CD19/CD3 BiTE(®) Antibody for the Treatment of Acute Lymphoblastic Leukemia: Perspectives and Current Pediatric Applications. Front. Oncol. 2014, 4, 63. [Google Scholar] [CrossRef] [Green Version]
- Franca, R.; Favretto, D.; Granzotto, M.; Decorti, G.; Rabusin, M.; Stocco, G. Epratuzumab and Blinatumomab as Therapeutic Antibodies for Treatment of Pediatric Acute Lymphoblastic Leukemia: Current Status and Future Perspectives. Curr. Med. Chem. 2017, 24, 1050–1065. [Google Scholar] [CrossRef]
- Queudeville, M.; Ebinger, M. Blinatumomab in Pediatric Acute Lymphoblastic Leukemia-From Salvage to First Line Therapy (A Systematic Review). J. Clin. Med. 2021, 10, 2544. [Google Scholar] [CrossRef]
- Von Stackelberg, A.; Locatelli, F.; Zugmaier, G.; Handgretinger, R.; Trippett, T.M.; Rizzari, C.; Bader, P.; O’Brien, M.M.; Brethon, B.; Bhojwani, D.; et al. Phase I/II study of blinatumomab in pediatric patients with relapsed/refractory acute lymphoblastic leukemia. J. Clin. Oncol. 2016, 34, 4381–4389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Locatelli, F.; Zugmaier, G.; Mergen, N.; Bader, P.; Jeha, S.; Schlegel, P.G.; Bourquin, J.P.; Handgretinger, R.; Brethon, B.; Rossig, C.; et al. Blinatumomab in pediatric patients with relapsed/refractory acute lymphoblastic leukemia: Results of the RIALTO trial, an expanded access study. Blood Cancer J. 2020, 10, 77. [Google Scholar] [CrossRef]
- Contreras, C.F.; Higham, C.S.; Behnert, A.; Kim, K.; Stieglitz, E.; Tasian, S.K. Clinical utilization of blinatumomab and inotuzumab immunotherapy in children with relapsed or refractory B-acute lymphoblastic leukemia. Pediatric Blood Cancer 2021, 68, e28718. [Google Scholar] [CrossRef] [PubMed]
- Fuster, J.L.; Molinos-Quintana, A.; Fuentes, C.; Fernández, J.M.; Velasco, P.; Pascual, T.; Rives, S.; Dapena, J.L.; Sisinni, L.; López-Godino, O.; et al. Blinatumomab and inotuzumab for B cell precursor acute lymphoblastic leukaemia in children: A retrospective study from the Leukemia Working Group of the Spanish Society of Pediatric Hematology and Oncology (SEHOP). Br. J. Hematol. 2020, 190, 764–771. [Google Scholar] [CrossRef] [PubMed]
- Ampatzidou, M.; Kattamis, A.; Baka, M.; Paterakis, G.; Anastasiou, T.; Tzanoudaki, M.; Kaisari, A.; Avgerinou, G.; Doganis, D.; Papadakis, V.; et al. Insights from the Greek experience of the use of Blinatumomab in pediatric relapsed and refractory acutelymphoblastic leukemia patients. Neoplasma 2020, 67, 1424–1430. [Google Scholar] [CrossRef]
- Klinger, M.; Zugmaier, G.; Nägele, V.; Goebeler, M.E.; Brandl, C.; Stelljes, M.; Lassmann, H.; von Stackelberg, A.; Bargou, R.C.; Kufer, P. Adhesion of T Cells to Endothelial Cells Facilitates Blinatumomab-Associated Neurologic Adverse Events. Cancer Res. 2020, 80, 91–101. [Google Scholar] [CrossRef] [Green Version]
- Sutton, R.; Pozza, L.D.; Khaw, S.L.; Fraser, C.; Revesz, T.; Chamberlain, J.; Mitchell, R.; Trahair, T.N.; Bateman, C.M.; Venn, N.C.; et al. Outcomes for Australian children with relapsed/refractory acute lymphoblastic leukaemia treated with blinatumomab. Pediatric Blood Cancer 2021, 68, e28922. [Google Scholar] [CrossRef] [PubMed]
- Jabbour, E.J.; Gökbuget, N.; Kantarjian, H.; Thomas, X.; Larson, R.A.; Yoon, S.S.; Ghobadi, A.; Topp, M.S.; Tran, Q.; Franklin, J.L.; et al. Transplantation in adults with relapsed/refractory acute lymphoblastic leukemia who are treated with blinatumomab from a phase 3 study. Cancer 2019, 125, 4181–4192. [Google Scholar] [CrossRef]
- Locatelli, F.; Whitlock, J.A.; Peters, C.; Chen-Santel, C.; Chia, V.; Dennis, R.M.; Heym, K.M.; Katz, A.J.; Kelsh, M.A.; Sposto, R.; et al. Blinatumomab versus historical standard therapy in pediatric patients with relapsed/refractory Ph-negative B-cell precursor acute lymphoblastic leukemia. Leukemia 2020, 34, 2473–2478. [Google Scholar] [CrossRef]
- Brown, P.A.; Ji, L.; Xu, X.; Devidas, M.; Hogan, L.E.; Borowitz, M.J.; Raetz, E.A.; Zugmaier, G.; Sharon, E.; Bernhardt, M.B.; et al. Effect of Postreinduction Therapy Consolidation WithBlinatumomab vs. Chemotherapy on Disease-Free Survival in Children, Adolescents, and Young Adults With First Relapse of B-Cell Acute Lymphoblastic Leukemia: A Randomized Clinical Trial. JAMA 2021, 325, 833–842. [Google Scholar] [CrossRef] [PubMed]
- Locatelli, F.; Zugmaier, G.; Rizzari, C.; Morris, J.D.; Gruhn, B.; Klingebiel, T.; Parasole, R.; Linderkamp, C.; Flotho, C.; Petit, A.; et al. Effect of Blinatumomab vs. Chemotherapy on Event-Free Survival Among Children With High-risk First-Relapse B-Cell Acute Lymphoblastic Leukemia: A Randomized Clinical Trial. JAMA 2021, 325, 843–854. [Google Scholar] [CrossRef] [PubMed]
- Locatelli, F.; Maschan, A.; Boissel, N.; Strocchio, L.; Alam, N.; Pezzani, I.; Brescianini, A.; Kreuzbauer, G.; Baruchel, A. Treatment with blinatumomab of paediatric patients with acute lymphoblastic leukaemia treated in a real-world setting: Results from the NEUF study. HemaSphere 2020, 4, 1–1168. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n (%) |
|---|---|
| Total Patients | 39 |
| Sex | |
| Male | 22 (56.4) |
| Female | 17 (43.6) |
| Age at initial diagnosis | |
| Median, years (IQR) | 5.3 (0.2–20.4) |
| <12 months | 3 (7.7) |
| 1–18 years | 35 (89.7) |
| >18 years | 1 (2.6) |
| Immunophenotype | |
| pre-B (EGIL B-I) | 8 (20.5) |
| Common (EGIL B-II) | 27 (69.2) |
| pro-B (EGIL B-III) | 4 (10.3) |
| Karyotype | |
| Hyperdiploid | 7 (17.9) |
| t (12; 21) | 1 (2.6) |
| t (3; 9) | 1 (2.6) |
| Other chromosomal aberrations | 3 (7.7) |
| Normal karyotype | 9 (23.1) |
| Unknown cytogenetic status | 18 (46.1) |
| Molecular abnormalities | |
| iAMP21 | 1 (2.6) |
| Ph-like | 2 (5.1) |
| KMT2A-rearrangement | 4 (10.3) |
| Absence of mutations | 24 (61.5) |
| Unknown mutational status | 8 (20.5) |
| First-line risk stratification | |
| Standard Risk | 4 (10.3) |
| Medium Risk | 13 (33.3) |
| High risk | 15 (38.5) |
| Unknown | 7 (17.9) |
| Months from diagnosis to blinatumomab treatment | |
| Median (IQR) | 6 (0.7–20.1) |
| <18 months | 9 (23.1) |
| 18 months–30 months | 8 (20.5) |
| >30 months | 22 (56.4) |
| Age at treatment | |
| Median, years (IQR) | 9.2 (2.3–21.5) |
| <12 months | 0 (0) |
| 1–18 years | 36 (92.3) |
| >18 years | 3 (7.7) |
| Therapeutic line | |
| Front line | 4 (10.2) |
| First relapse | 23 (59) |
| Second or greater relapse | 12 (30.8) |
| Refractory | 4 (10.2) |
| Relapses | 35 (89.7) |
| Site of relapse | |
| Bone Marrow | 24(68.5) |
| Molecular relapse | 3(8.6) |
| Combined relapse | 8 (22.9) |
| HSCT pre blinatumomab | |
| Yes | 10 (25.6) |
| No | 29 (74.4) |
| Blinatumomab courses | |
| 1 | 17 (43.6) |
| 2 | 18 (46.2) |
| >2 | 4 (10.2) |
| Bone marrow blasts before blinatumomab <5% | 26 (66.7) |
| After debulking chemotherapy | 18 (46.2) |
| PCR-MRD positive | 5 (12.8) |
| FC-MRD positive | 3 (7.7) |
| Bone marrow blasts before blinatumomab ≥5% | 13 (33.3) |
| >5–25% blasts | 6 (15.4) |
| >25% blasts | 7 (17.9) |
| Toxicities During Blinatumomab | Grade 1–2 | Grade 3 | Grade 4 | Unknown Grade | Total | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | |
| Patients with at least one adverse event | 22 | 56.40% | ||||||||
| Total adverse events | 46 | 100% | ||||||||
| Neurotoxicity | 7 | 15.2% | 9 | 19.6% | 1 | 2.2% | 1 | 2.2% | 18 | 39.1% |
| Unspecified neurotoxicity | 3 | 6.5% | 2 | 4.3% | - | - | - | - | 5 | 10.9% |
| Altered mental status | 1 | 2.2% | 1 | 2.2% | - | - | - | - | 2 | 4.3% |
| Dysmetria | - | - | 1 | 2.2% | - | - | - | - | 1 | 2.2% |
| Aphasia | - | - | 1 | 2.2% | - | - | - | - | 1 | 2.2% |
| Dysarthria | - | - | 1 | 2.2% | - | - | - | - | 1 | 2.2% |
| Seizure | 1 | 2.2% | 1 | 2.2% | 1 | 2.2% | - | - | 3 | 6.5% |
| Tremor | 1 | 2.2% | 1 | 2.2% | - | - | 1 | 2.2% | 3 | 6.5% |
| Polyneuropathy | 1 | 2.2% | 1 | 2.2% | - | - | - | - | 2 | 4.3% |
| Hepatotoxicity | 3 | 6.5% | 1 | 2.2% | - | - | - | - | 4 | 8.7% |
| Fever | 8 | 17.4% | 1 | 2.2% | - | - | 2 | 4.3% | 11 | 24% |
| Rash | 2 | 4.3% | - | - | - | - | - | - | 2 | 4.3% |
| Hematological toxicity | 3 | 6.5% | 2 | 4.3% | - | - | - | - | 5 | 10.9% |
| Thrombocytopenia | 1 | 2.2% | 1 | 2.2% | - | - | - | - | 2 | 4.3% |
| Anemia | 1 | 2.2% | 1 | 2.2% | - | - | - | - | 2 | 4.3% |
| Neutropenia | 1 | 2.2% | - | - | - | - | - | - | 1 | 2.2% |
| Progressive candidiasis | - | - | 1 | 2.2% | - | - | - | - | 1 | 2.2% |
| Pneumocystosis | - | - | 1 | 2.2% | - | - | - | - | 1 | 2.2% |
| Ascites | 1 | 2.2% | - | - | - | - | - | - | 1 | 2.2% |
| Hypogammaglobulinemia | 2 | 4.3% | - | - | - | - | - | - | 2 | 4.3% |
| Autoimmune arthritis | 1 | 2.2% | - | - | - | - | - | - | 1 | 2.2% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beneduce, G.; De Matteo, A.; Stellato, P.; Testi, A.M.; Bertorello, N.; Colombini, A.; Putti, M.C.; Rizzari, C.; Cesaro, S.; Cellini, M.; et al. Blinatumomab in Children and Adolescents with Relapsed/Refractory B Cell Precursor Acute Lymphoblastic Leukemia: A Real-Life Multicenter Retrospective Study in Seven AIEOP (Associazione Italiana di Ematologia e Oncologia Pediatrica) Centers. Cancers 2022, 14, 426. https://doi.org/10.3390/cancers14020426
Beneduce G, De Matteo A, Stellato P, Testi AM, Bertorello N, Colombini A, Putti MC, Rizzari C, Cesaro S, Cellini M, et al. Blinatumomab in Children and Adolescents with Relapsed/Refractory B Cell Precursor Acute Lymphoblastic Leukemia: A Real-Life Multicenter Retrospective Study in Seven AIEOP (Associazione Italiana di Ematologia e Oncologia Pediatrica) Centers. Cancers. 2022; 14(2):426. https://doi.org/10.3390/cancers14020426
Chicago/Turabian StyleBeneduce, Giuliana, Antonia De Matteo, Pio Stellato, Anna M. Testi, Nicoletta Bertorello, Antonella Colombini, Maria C. Putti, Carmelo Rizzari, Simone Cesaro, Monica Cellini, and et al. 2022. "Blinatumomab in Children and Adolescents with Relapsed/Refractory B Cell Precursor Acute Lymphoblastic Leukemia: A Real-Life Multicenter Retrospective Study in Seven AIEOP (Associazione Italiana di Ematologia e Oncologia Pediatrica) Centers" Cancers 14, no. 2: 426. https://doi.org/10.3390/cancers14020426
APA StyleBeneduce, G., De Matteo, A., Stellato, P., Testi, A. M., Bertorello, N., Colombini, A., Putti, M. C., Rizzari, C., Cesaro, S., Cellini, M., Barisone, E., Petruzziello, F., Menna, G., & Parasole, R. (2022). Blinatumomab in Children and Adolescents with Relapsed/Refractory B Cell Precursor Acute Lymphoblastic Leukemia: A Real-Life Multicenter Retrospective Study in Seven AIEOP (Associazione Italiana di Ematologia e Oncologia Pediatrica) Centers. Cancers, 14(2), 426. https://doi.org/10.3390/cancers14020426