
The Alliance AMBUSH Trial: Rationale and Design

Abstract
:Simple Summary
Abstract
1. Introduction
2. Classification of Medulloblastoma
3. Rationale to Include Non-SHH-MB, High-Risk MB, and Pineal Tumors
4. Backbone of AMBUSH Therapeutic Strategy
4.1. Surgery
4.2. Radiotherapy
4.3. Chemotherapy
4.4. Targeted Therapy
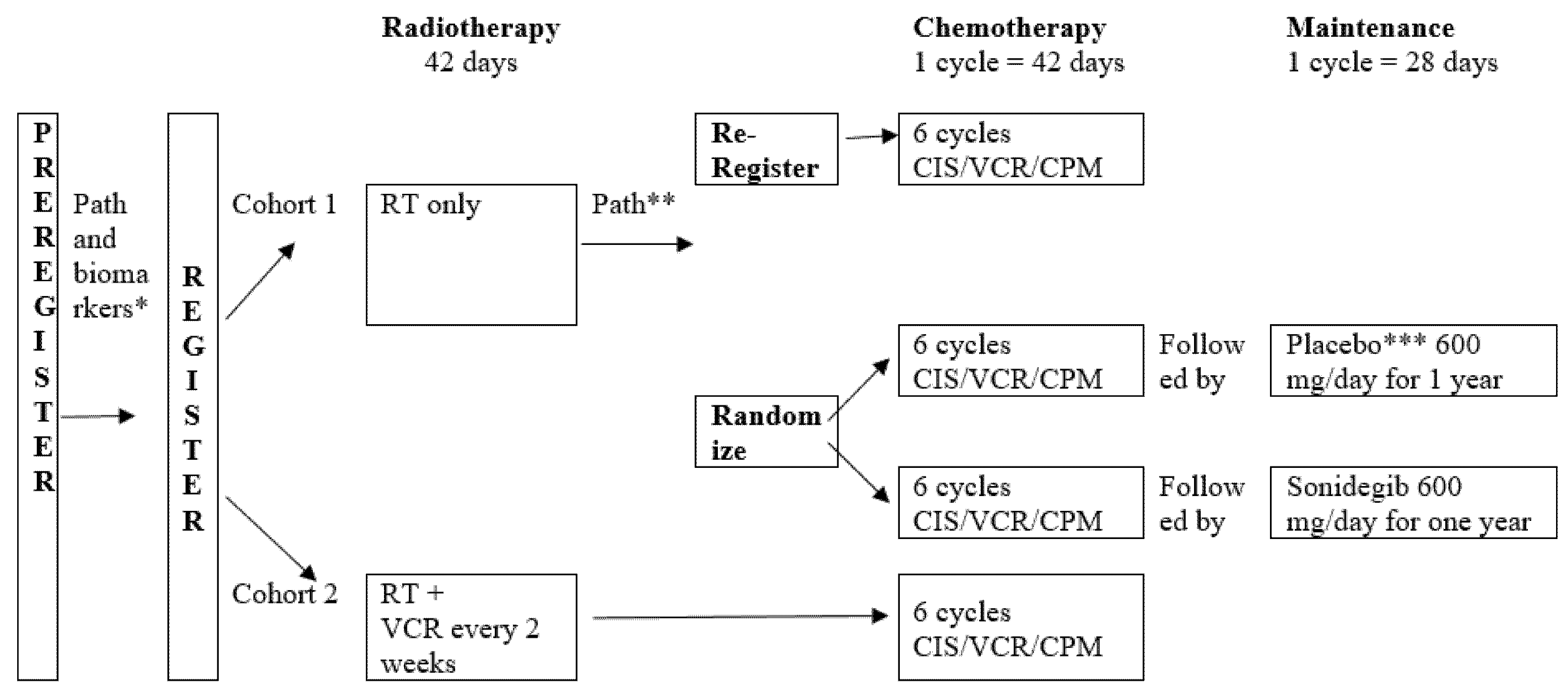
5. Trial Design
6. Objectives
7. Accrual Goal
8. Translational Research
8.1. Neurocognitive Function
8.2. Health Related Quality of Life
8.3. Neuroendocrine, Auditory, and Visual Functions
8.4. Radiotherapy Modality
8.5. Effect of Memantine
8.6. CSF and Plasma Banking
8.7. Comparison to Contemporaneous Trials
9. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Giordana, M.T.; Schiffer, P.; Lanotte, M.; Girardi, P.; Chio, A. Epidemiology of adult medulloblastoma. Int. J. Cancer 1999, 80, 689–692. [Google Scholar] [CrossRef]
- Ostrom, Q.T.; Gittleman, H.; Fulop, J.; Liu, M.; Blanda, R.; Kromer, C.; Wolinsky, Y.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2009–2013. Neuro Oncol. 2016, 18, v1–v75. [Google Scholar] [CrossRef] [Green Version]
- Gajjar, A.; Chintagumpala, M.; Ashley, D.; Kellie, S.; Kun, L.E.; Merchant, T.E.; Woo, S.; Wheeler, G.; Ahern, V.; Krasin, M.J.; et al. Risk-adapted craniospinal radiotherapy followed by high-dose chemotherapy and stem-cell rescue in children with newly diagnosed medulloblastoma (St Jude Medulloblastoma-96): Long-term results from a prospective, multicentre trial. Lancet Oncol. 2006, 7, 813–820. [Google Scholar] [CrossRef]
- Packer, R.J.; Gajjar, A.; Vezina, G.; Rorke-Adams, L.; Burger, P.C.; Robertson, P.L.; Bayer, L.; LaFond, D.; Donahue, B.R.; Marymont, M.H.; et al. Phase III Study of Craniospinal Radiation Therapy Followed by Adjuvant Chemotherapy for Newly Diagnosed Average-Risk Medulloblastoma. J. Clin. Oncol. 2006, 24, 4202–4208. [Google Scholar] [CrossRef] [PubMed]
- Von Bueren, A.O.; Kortmann, R.-D.; Von Hoff, K.; Friedrich, C.; Mynarek, M.; Müller, K.; Goschzik, T.; Mühlen, A.Z.; Gerber, N.; Warmuth-Metz, M.; et al. Treatment of Children and Adolescents With Metastatic Medulloblastoma and Prognostic Relevance of Clinical and Biologic Parameters. J. Clin. Oncol. 2016, 34, 4151–4160. [Google Scholar] [CrossRef]
- Lannering, B.; Rutkowski, S.; Doz, F.; Pizer, B.; Gustafsson, G.; Navajas, A.; Massimino, M.; Reddingius, R.; Benesch, M.; Carrie, C.; et al. Hyperfractionated Versus Conventional Radiotherapy Followed by Chemotherapy in Standard-Risk Medulloblastoma: Results From the Randomized Multicenter HIT-SIOP PNET 4 Trial. J. Clin. Oncol. 2012, 30, 3187–3193. [Google Scholar] [CrossRef]
- Michalski, J.M.; Janss, A.J.; Vezina, L.G.; Smith, K.S.; Billups, C.A.; Burger, P.C.; Embry, L.M.; Cullen, P.L.; Hardy, K.K.; Pomeroy, S.L.; et al. Children’s Oncology Group Phase III Trial of Reduced-Dose and Reduced-Volume Radiotherapy With Chemotherapy for Newly Diagnosed Average-Risk Medulloblastoma. J. Clin. Oncol. 2021, 39, 2685–2697. [Google Scholar] [CrossRef]
- Thomas, P.R.M.; Deutsch, M.; Kepner, J.L.; Boyett, J.M.; Krischer, J.; Aronin, P.; Albright, L.; Allen, J.; Packer, R.J.; Linggood, R.; et al. Low-Stage Medulloblastoma: Final Analysis of Trial Comparing Standard-Dose With Reduced-Dose Neuraxis Irradiation. J. Clin. Oncol. 2000, 18, 3004–3011. [Google Scholar] [CrossRef]
- Cosman, R.; Brown, C.; De Braganca, K.; Khasraw, M. Patterns of care in adult medulloblastoma: Results of an international online survey. J. Neuro-Oncology 2014, 120, 125–129. [Google Scholar] [CrossRef] [Green Version]
- Patil, R.; Gupta, T.; Maitre, M.; Dasgupta, A.; Sahay, A.; Epari, S.; Shirsat, N.; Chatterjee, A.; Krishnatry, R.; Goda, J.S.; et al. Clinical Audit of Survival Outcomes and Prognostic Factors in Adolescents and Adults with Medulloblastoma. J. Adolesc. Young-Adult Oncol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Penas-Prado, M.; Theeler, B.J.; Cordeiro, B.; Dunkel, I.J.; Hau, P.; Mahajan, A.; Robinson, G.W.; Willmarth, N.; Aboud, O.; Aldape, K.; et al. Proceedings of the Comprehensive Oncology Network Evaluating Rare CNS Tumors (NCI-CONNECT) Adult Medulloblastoma Workshop. Neuro-Oncology Adv. 2020, 2, vdaa097. [Google Scholar] [CrossRef]
- Brandes, A.A.; Ermani, M.; Amista, P.; Basso, U.; Vastola, F.; Gardiman, M.; Iuzzolino, P.; Turazzi, S.; Rotilio, A.; Volpin, L.; et al. The treatment of adults with medulloblastoma: A prospective study. Int. J. Radiat. Oncol. 2003, 57, 755–761. [Google Scholar] [CrossRef]
- Northcott, P.A.; Korshunov, A.; Pfister, S.; Taylor, M. The clinical implications of medulloblastoma subgroups. Nat. Rev. Neurol. 2012, 8, 340–351. [Google Scholar] [CrossRef]
- Ramaswamy, V.; Taylor, M. Medulloblastoma: From Myth to Molecular. J. Clin. Oncol. 2017, 35, 2355–2363. [Google Scholar] [CrossRef]
- Schwalbe, E.; Lindsey, J.C.; Nakjang, S.; Crosier, S.; Smith, A.J.; Hicks, D.; Rafiee, G.; Hill, R.M.; Iliasova, A.; Stone, T.; et al. Novel molecular subgroups for clinical classification and outcome prediction in childhood medulloblastoma: A cohort study. Lancet Oncol. 2017, 18, 958–971. [Google Scholar] [CrossRef] [Green Version]
- Sengupta, S.; Krummel, D.P.; Pomeroy, S. The evolution of medulloblastoma therapy to personalized medicine. F1000Research 2017, 6, 490. [Google Scholar] [CrossRef] [Green Version]
- Northcott, P.A.; Dubuc, A.M.; Pfister, S.; Taylor, M.D. Molecular subgroups of medulloblastoma. Expert Rev. Neurother. 2012, 12, 871–884. [Google Scholar] [CrossRef] [Green Version]
- Remke, M.; Hielscher, T.; Northcott, P.A.; Witt, H.; Ryzhova, M.; Wittmann, A.; Benner, A.; von Deimling, A.; Scheurlen, W.; Perry, A.; et al. Adult Medulloblastoma Comprises Three Major Molecular Variants. J. Clin. Oncol. 2011, 29, 2717–2723. [Google Scholar] [CrossRef] [PubMed]
- Zhao, F.; Ohgaki, H.; Xu, L.; Giangaspero, F.; Li, C.; Li, P.; Yang, Z.; Wang, B.; Wang, X.; Wang, Z.; et al. Molecular subgroups of adult medulloblastoma: A long-term single-institution study. Neuro-Oncology 2016, 18, 982–990. [Google Scholar] [CrossRef] [PubMed]
- Coltin, H.; Sundaresan, L.; Smith, K.S.; Skowron, P.; Massimi, L.; Eberhart, C.G.; Schreck, K.C.; Gupta, N.; Weiss, W.A.; Tirapelli, D.; et al. Subgroup and subtype-specific outcomes in adult medulloblastoma. Acta Neuropathol. 2021, 142, 859–871. [Google Scholar] [CrossRef] [PubMed]
- Ellison, D.W.; Dalton, J.; Kocak, M.; Nicholson, S.L.; Fraga, C.; Neale, G.; Kenney, A.M.; Brat, D.J.; Perry, A.; Yong, W.H.; et al. Medulloblastoma: Clinicopathological correlates of SHH, WNT, and non-SHH/WNT molecular subgroups. Acta Neuropathol. 2011, 121, 381–396. [Google Scholar] [CrossRef] [Green Version]
- Zhukova, N.; Ramaswamy, V.; Remke, M.; Pfaff, E.; Shih, D.J.H.; Martin, D.C.; Castelo-Branco, P.; Baskin, B.; Ray, P.N.; Bouffet, E.; et al. Subgroup-Specific Prognostic Implications of TP53 Mutation in Medulloblastoma. J. Clin. Oncol. 2013, 31, 2927–2935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrlinger, U.; Steinbrecher, A.; Rieger, J.; Hau, P.; Kortmann, R.D.; Meyermann, R.; Schabet, M.; Bamberg, M.; Dichgans, J.; Bogdahn, U.; et al. Adult medulloblastoma: Prognostic factors and response to therapy at diagnosis and at relapse. J. Neurol. 2005, 252, 291–299. [Google Scholar] [CrossRef] [Green Version]
- Takase, H.; Tanoshima, R.; Singla, N.; Nakamura, Y.; Yamamoto, T. Pineal parenchymal tumor of intermediate differentiation: A systematic review and contemporary management of 389 cases reported during the last two decades. Neurosurg Rev. 2021. online ahead of print. [Google Scholar] [CrossRef]
- Jakacki, R.I.; Zeltzer, P.M.; Boyett, J.M.; Albright, A.L.; Allen, J.C.; Geyer, J.R.; Rorke, L.B.; Stanley, P.; Stevens, K.R.; Wisoff, J. Survival and prognostic factors following radiation and/or chemotherapy for primitive neuroectodermal tumors of the pineal region in infants and children: A report of the Childrens Cancer Group. J. Clin. Oncol. 1995, 13, 1377–1383. [Google Scholar] [CrossRef]
- Massimino, M.; Sunyach, M.P.; Barretta, F.; Gandola, L.; Garegnani, A.; Pecori, E.; Spreafico, F.; Bonneville-Levard, A.; Meyronet, D.; Mottolese, C.; et al. Reduced-dose craniospinal irradiation is feasible for standard-risk adult medulloblastoma patients. J. Neuro-Oncology 2020, 148, 619–628. [Google Scholar] [CrossRef] [PubMed]
- Paterson, E.; Farr, R.F. Cerebellar Medulloblastoma: Treatment by Irradiation of the Whole Central Nervous System. Acta Radiol. 1953, 39, 323–336. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, C.; von Bueren, A.O.; von Hoff, K.; Kwiecien, R.; Pietsch, T.; Warmuth-Metz, M.; Hau, P.; Deinlein, F.; Kuehl, J.; Kortmann, R.D.; et al. Treatment of adult nonmetastatic medulloblastoma patients according to the paediatric HIT 2000 protocol: A prospective observational multicentre study. Eur. J. Cancer 2012, 49, 893–903. [Google Scholar] [CrossRef] [PubMed]
- Majd, N.K.; Mastall, M.; Lin, H.; Dibaj, S.S.; Hess, K.R.; Yuan, Y.; Garcia, M.M.; Fuller, G.N.; Alfaro, K.D.; Gule-Monroe, M.K.; et al. Clinical characterization of adult medulloblastoma and the effect of first-line therapies on outcome; The MD Anderson Cancer Center experience. Neurooncol Adv. 2021, 3, vdab079. [Google Scholar] [CrossRef]
- Beier, D.; Proescholdt, M.; Reinert, C.; Pietsch, T.; Jones, D.T.W.; Pfister, S.M.; Hattingen, E.; Seidel, C.; Dirven, L.; Luerding, R.; et al. Multicenter pilot study of radiochemotherapy as first-line treatment for adults with medulloblastoma (NOA-07). Neuro-Oncology 2017, 20, 400–410. [Google Scholar] [CrossRef] [PubMed]
- Von Bueren, A.O.; Friedrich, C.; Von Hoff, K.; Kwiecien, R.; Müller, K.; Pietsch, T.; Warmuth-Metz, M.; Hau, P.; Benesch, M.; Kuehl, J.; et al. Metastatic medulloblastoma in adults: Outcome of patients treated according to the HIT2000 protocol. Eur. J. Cancer 2015, 51, 2434–2443. [Google Scholar] [CrossRef]
- Carballo, G.B.; Honorato, J.R.; De Lopes, G.P.F.; Spohr, T.C.L.D.S.E. A highlight on Sonic hedgehog pathway. Cell Commun. Signal. 2018, 16, 11. [Google Scholar] [CrossRef]
- Kieran, M.W. Targeted treatment for sonic hedgehog-dependent medulloblastoma. Neuro-Oncology 2014, 16, 1037–1047. [Google Scholar] [CrossRef] [Green Version]
- Kool, M.; Jones, D.T.W.; Jaeger, N.; Northcott, P.A.; Pugh, T.J.; Hovestadt, V.; Piro, R.M.; Esparza, L.A.; Markant, S.L.; Remke, M.; et al. Genome Sequencing of SHH Medulloblastoma Predicts Genotype-Related Response to Smoothened Inhibition. Cancer Cell 2014, 25, 393–405. [Google Scholar] [CrossRef] [Green Version]
- Kieran, M.W.; Chisholm, J.; Casanova, M.; Brandes, A.A.; Aerts, I.; Bouffet, E.; Bailey, S.; Leary, S.; Macdonald, T.J.; Mechinaud, F.; et al. Phase I study of oral sonidegib (LDE225) in pediatric brain and solid tumors and a phase II study in children and adults with relapsed medulloblastoma. Neuro-Oncology 2017, 19, 1542–1552. [Google Scholar] [CrossRef]
- Dummer, R.; Guminksi, A.; Gutzmer, R.; Lear, J.T.; Lewis, K.D.; Chang, A.L.S.; Combemale, P.; Dirix, L.; Kaatz, M.; Kudchadkar, R.; et al. Long-term efficacy and safety of sonidegib in patients with advanced basal cell carcinoma: 42-month analysis of the phase II randomized, double-blind BOLT study. Br. J. Dermatol. 2020, 182, 1369–1378. [Google Scholar] [CrossRef] [PubMed]
- Khanna, V.; Achey, R.L.; Ostrom, Q.; Block-Beach, H.; Kruchko, C.; Barnholtz-Sloan, J.S.; de Blank, P. Incidence and survival trends for medulloblastomas in the United States from 2001 to 2013. J. Neuro-Oncology 2017, 135, 433–441. [Google Scholar] [CrossRef]
- Li, Q.; Dai, Z.; Cao, Y.; Wang, L. Comparing children and adults with medulloblastoma: A SEER based analysis. Oncotarget 2018, 9, 30189–30198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrison, R.A.; Kesler, S.R.; Johnson, J.; Penas-Prado, M.; Sullaway, C.M.; Wefel, J.S. Neurocognitive dysfunction in adult cerebellar medulloblastoma. Psycho-Oncology 2018, 28, 131–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dirven, L.; Luerding, R.; Beier, D.; Bumes, E.; Reinert, C.; Seidel, C.; Bonsanto, M.M.; Bremer, M.; Rieken, S.; Combs, S.E.; et al. Neurocognitive functioning and health-related quality of life in adult medulloblastoma patients: Long-term outcomes of the NOA-07 study. J. Neuro-Oncology 2020, 148, 117–130. [Google Scholar] [CrossRef]
- Gibson, T.M.; Mostoufi-Moab, S.; Stratton, K.L.; Leisenring, W.; Barnea, D.; Chow, E.; Donaldson, S.S.; Howell, R.M.; Hudson, M.M.; Mahajan, A.; et al. Temporal patterns in the risk of chronic health conditions in survivors of childhood cancer diagnosed 1970–99: A report from the Childhood Cancer Survivor Study cohort. Lancet Oncol. 2018, 19, 1590–1601. [Google Scholar] [CrossRef]
- Moeller, B.J.; Chintagumpala, M.; Philip, J.J.; Grosshans, D.R.; McAleer, M.F.; Woo, S.Y.; Gidley, P.W.; Vats, T.S.; Mahajan, A. Low early ototoxicity rates for pediatric medulloblastoma patients treated with proton radiotherapy. Radiat. Oncol. 2011, 6, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paulino, A.C.; Mahajan, A.; Ye, R.; Grosshans, D.R.; Okcu, M.F.; Su, J.; McAleer, M.F.; McGovern, S.; Mangona, V.A.; Chintagumpala, M. Ototoxicity and cochlear sparing in children with medulloblastoma: Proton vs. photon radiotherapy. Radiother. Oncol. 2018, 128, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Aldrich, K.D.; Horne, V.E.; Bielamowicz, K.; Sonabend, R.Y.; Scheurer, M.E.; Paulino, A.C.; Mahajan, A.; Chintagumpala, M.; Okcu, M.F.; Brown, A.L. Comparison of hypothyroidism, growth hormone deficiency, and adrenal insufficiency following proton and photon radiotherapy in children with medulloblastoma. J. Neuro-Oncology 2021, 155, 93–100. [Google Scholar] [CrossRef]
- Bielamowicz, K.; Okcu, M.F.; Sonabend, R.; Paulino, A.C.; Hilsenbeck, S.G.; Dreyer, Z.; Suzawa, H.; Bryant, R.; Adesina, A.; Dauser, R.; et al. Hypothyroidism after craniospinal irradiation with proton or photon therapy in patients with medulloblastoma. Pediatr. Hematol. Oncol. 2018, 35, 257–267. [Google Scholar] [CrossRef] [PubMed]
- Vatner, R.E.; Niemierko, A.; Misra, M.; Weyman, E.A.; Goebel, C.P.; Ebb, D.H.; Jones, R.M.; Huang, M.S.; Mahajan, A.; Grosshans, D.R.; et al. Endocrine Deficiency As a Function of Radiation Dose to the Hypothalamus and Pituitary in Pediatric and Young Adult Patients With Brain Tumors. J. Clin. Oncol. 2018, 36, 2854–2862. [Google Scholar] [CrossRef]
- Brown, A.P.; Barney, C.L.; Grosshans, D.R.; McAleer, M.F.; de Groot, J.F.; Puduvalli, V.K.; Tucker, S.L.; Crawford, C.N.; Khan, M.; Khatua, S.; et al. Proton Beam Craniospinal Irradiation Reduces Acute Toxicity for Adults With Medulloblastoma. Int. J. Radiat. Oncol. 2013, 86, 277–284. [Google Scholar] [CrossRef] [Green Version]
- Zhang, R.; Howell, R.M.; Taddei, P.J.; Giebeler, A.; Mahajan, A.; Newhauser, W.D. A comparative study on the risks of radiogenic second cancers and cardiac mortality in a set of pediatric medulloblastoma patients treated with photon or proton craniospinal irradiation. Radiother Oncol. 2014, 113, 84–88. [Google Scholar] [CrossRef] [Green Version]
- Brown, P.D.; Gondi, V.; Pugh, S.; Tome, W.A.; Wefel, J.S.; Armstrong, T.S.; Bovi, J.A.; Robinson, C.; Konski, A.; Khuntia, D.; et al. Hippocampal Avoidance During Whole-Brain Radiotherapy Plus Memantine for Patients With Brain Metastases: Phase III Trial NRG Oncology CC001. J. Clin. Oncol. 2020, 38, 1019–1029. [Google Scholar] [CrossRef]
- Laack, N.N.; Pugh, S.L.; Brown, P.D.; Fox, S.; Wefel, J.S.; Meyers, C.; Choucair, A.; Khuntia, D.; Suh, J.H.; Roberge, D.; et al. The association of health-related quality of life and cognitive function in patients receiving memantine for the prevention of cognitive dysfunction during whole-brain radiotherapy. Neuro-Oncology Pract. 2018, 6, 274–282. [Google Scholar] [CrossRef]
- Brown, P.D.; Pugh, S.; Laack, N.N.; Wefel, J.S.; Khuntia, D.; Meyers, C.; Choucair, A.; Fox, S.; Suh, J.H.; Roberge, D.; et al. Memantine for the prevention of cognitive dysfunction in patients receiving whole-brain radiotherapy: A randomized, double-blind, placebo-controlled trial. Neuro-Oncology 2013, 15, 1429–1437. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Tx Phase | CHEMO | AMBUSH | A9961 | ACNS0331 | NOA-7 | SJMB03 | SJMB12 |
|---|---|---|---|---|---|---|---|
| Number of cycles, (doses mg/m2) | 6 cycles as tolerated | A 8 (ccnu/cis/vcr) vs. B 8 (cpm/cis/vcr) | A 6 (ccnu/cis/vcr) B 3 (cpm/vcr) AAB | ADULT | A 4 (vcr/cpm/cis) | A 4 (vcr/cpm/cis) | |
| RT | VCR | None | 8 (1.5) | 6 (1.5) | 3 (1.5) | none | none |
| MAINTENANCE | VCR | 6 (1.5 × 2) max (2) mg | 8 (1.5 × 3) | A 6 (1.5 × 3) + B 3 (1.5 × 2) | 6 (1.5 × 2) | 4 (1.0 × 2) | 4 (1.0 × 2) |
| CIS | 6 (75) | 8 (75) | A 6 (75) | 6 (70) | 4 (75) | 4 (75) | |
| CCNU | none | 8 (75) | A 6 (75) | 6 (75) | none | none | |
| CPM | 6 (1000 × 2) | 8 (1000 × 2) | B 3 (1000 × 2) | none | 4 (2000 × 2) | 4 (1500 × 2) | |
| VP16 | none | none | none | none | none | none | |
| Comments | 6 cycles if tolerated | reg A = B | std COG | tolerated | stem cell rescue ×4 | SHH: vismodegib maintenance | |
| Tx Phase | CHEMO | AMBUSH | ACNS 0332 | SJMB03 | SJMB12- SHH | SJMB12 |
|---|---|---|---|---|---|---|
| All doses mg/m2 | 6 cycles as tolerated | 6 cycles | 4 (vcr/cpm/cis) | 4 (vcr/cpm/cis) | A 4 (vcr/cpm/cis) B 3 (paclitaxel/gem) AABAABB | |
| RT | VCR | 6 (1.5) q2 wk | 6 (1.5) weekly | none | none | none |
| Carboplatin | none | 30 (35) daily | none | none | none | |
| MAINTENANCE | VCR | 6 (1.5 × 2) | 6 (1.5 × 2) | 4 (1.0 × 2) | 4 (1.0 × 2) | 4 (1.0 × 2) |
| CIS | 6 (75) | 6 (75) | 4 (75) | 4 (75) | 4 (75) | |
| CPM | 6 (1000 × 2) | 6 (1000 × 2) | 4 (2000 × 2) | 4 (1500 × 2) | 4 (1500 × 2) | |
| Paclitaxel | none | none | none | none | 3 (600 × 2) | |
| Gemcitibine | none | none | none | none | 3 (1250 × 2) | |
| COMMENTS | 6 cycles if tolerated | daily carbo randomized | 4 × stem cell rescue | vismodegib maintenance | intermediate, HR Non-SHH | |
| Test or Observation | Baseline | Weekly during RT | Prior to Chemo | Chemo × 4 Cycles | Pre Sonidegib/Placebo | Monthly | Annually Post Completions | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Approximate Wk, Wk 0 = RT start | Wk | Wk | Wk | Wk | Wk | Wk | Wk 52 | ||||
| −4 to 2 | 0 to 6 | 9 to 10 | 10 to 26 | 26 to 30 | 30 to 82 | ||||||
| Tests and Observations | |||||||||||
| History and Physical | pre RT | x | x | x | x | each visit | x | ||||
| Weight (each visit) | pre RT | x | x | prn | x | x | x | ||||
| Hearing | x | x | x | y 1, 3, 5 | |||||||
| Vision | x | x | y 1, 3, 5 | ||||||||
| CompNeurocog | x | y 1, 3, 5 | |||||||||
| Short Neurocog | x | x | x | x | x | x | x | ||||
| QOL/PRO-CTCAE | x | x | x | x | x | y 1, 3, 5 | |||||
| Laboratory Studies | |||||||||||
| CBC | pre RT | x | x | x | x | x | x | x | x | x | x |
| Blood Chemistries | x | x | prn | x | x | x | x | x | x | x | |
| Endocrine | x | x | y 1, 3, 5 | ||||||||
| Creatine Kinase | x | x | x | x | x | x | x | x | x | x | |
| BUN/Creatinine | x | x | x (1) | x | x | x | x | x | x | x | |
| Staging | |||||||||||
| Tumor Imaging | pre RT | x | post cycle 2 | x | |||||||
| Research Studies for Banking | tumor, CSF, plasma | plasma | plasma | ||||||||
| plasma and CSF if Recurrence | |||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahajan, A.; Shih, H.; Penas-Prado, M.; Ligon, K.; Aldape, K.; Hu, L.S.; Loughan, A.R.; Basso, M.R.; Leeper, H.E.; Nahed, B.V.; et al. The Alliance AMBUSH Trial: Rationale and Design. Cancers 2022, 14, 414. https://doi.org/10.3390/cancers14020414
Mahajan A, Shih H, Penas-Prado M, Ligon K, Aldape K, Hu LS, Loughan AR, Basso MR, Leeper HE, Nahed BV, et al. The Alliance AMBUSH Trial: Rationale and Design. Cancers. 2022; 14(2):414. https://doi.org/10.3390/cancers14020414
Chicago/Turabian StyleMahajan, Anita, Helen Shih, Marta Penas-Prado, Keith Ligon, Kenneth Aldape, Leland S. Hu, Ashlee R. Loughan, Michael R. Basso, Heather E. Leeper, Brian V. Nahed, and et al. 2022. "The Alliance AMBUSH Trial: Rationale and Design" Cancers 14, no. 2: 414. https://doi.org/10.3390/cancers14020414
APA StyleMahajan, A., Shih, H., Penas-Prado, M., Ligon, K., Aldape, K., Hu, L. S., Loughan, A. R., Basso, M. R., Leeper, H. E., Nahed, B. V., Stott, S. L., Geyer, S., Giannini, C., & Galanis, E. (2022). The Alliance AMBUSH Trial: Rationale and Design. Cancers, 14(2), 414. https://doi.org/10.3390/cancers14020414