
Environmental Risk Factors for Childhood Acute Lymphoblastic Leukemia: An Umbrella Review

 ,
,  , , and
, , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Umbrella Review Methods
2.2. Eligibility Criteria
2.3. Information Sources
Search Strategy and Data Extraction
2.4. Quality Assessment and Risk of Bias in Systematic Reviews
2.5. Evidence for Risk Factors of Childhood Leukemia
3. Results
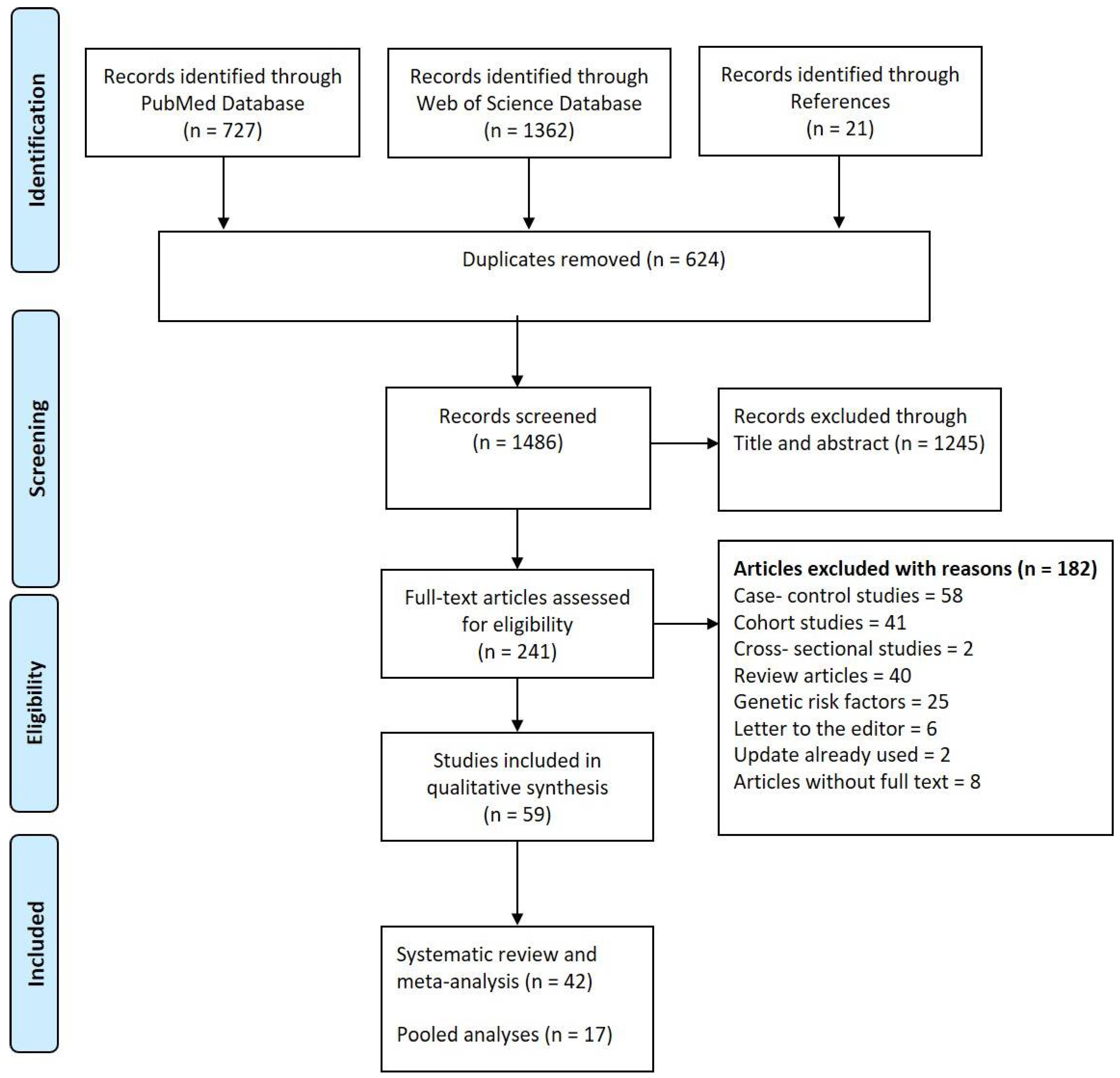
3.1. Search Strategy Outcome
3.2. Quality Assessment and Bias
3.3. Environmental Risk Factors
3.4. Paternal Preconception Exposure
3.5. Maternal Preconception/Pregnancy Exposure
3.6. Postnatal Exposure
3.7. Prevalence of Childhood ALL
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Disclaimer
References
- Steliarova-Foucher, E.; Colombet, M.; Ries, L.A.G.; Moreno, F.; Dolya, A.; Bray, F.; Hesseling, P.; Shin, H.Y.; Stiller, C.A.; Bouzbid, S.; et al. International incidence of childhood cancer, 2001–2010: A population-based registry study. Lancet Oncol. 2017, 18, 719–731. [Google Scholar] [CrossRef]
- Force, L.M.; Abdollahpour, I.; Advani, S.M.; Agius, D.; Ahmadian, E.; Alahdab, F.; Alam, T.; Alebel, A.; Alipour, V.; Allen, C.A.; et al. The global burden of childhood and adolescent cancer in 2017: An analysis of the Global Burden of Disease Study 2017. Lancet Oncol. 2019, 20, 1211–1225. [Google Scholar] [CrossRef]
- Erdmann, F.; Kaatsch, P.; Grabow, D.; Spix, C. German Childhood Cancer Registry—Annual Report 2019 (1980–2018); Institute of Medical Biostatistics, Epidemiology and Informatics (IMBEI) at the University Medical Center of the Johannes Gutenberg University: Mainz, Germany, 2020. [Google Scholar]
- Namayandeh, S.M.; Khazaei, Z.; Lari Najafi, M.; Goodarzi, E.; Moslem, A. GLOBAL Leukemia in Children 0-14 Statistics 2018, Incidence and Mortality and Human Development Index (HDI): GLOBOCAN Sources and Methods. Asian Pac. J. Cancer Prev. APJCP 2020, 21, 1487–1494. [Google Scholar] [CrossRef] [PubMed]
- Huang, F.-L.; Liao, E.-C.; Li, C.-L.; Yen, C.-Y.; Yu, S.-J. Pathogenesis of pediatric B-cell acute lymphoblastic leukemia: Molecular pathways and disease treatments. Oncol. Lett. 2020, 20, 448–454. [Google Scholar] [CrossRef]
- Greaves, M. A causal mechanism for childhood acute lymphoblastic leukaemia. Nat. Rev. Cancer 2018, 18, 471–484. [Google Scholar] [CrossRef] [PubMed]
- Greaves, M.F. Aetiology of acute leukaemia. Lancet 1997, 349, 344–349. [Google Scholar] [CrossRef]
- Schüz, J.; Erdmann, F. Environmental Exposure and Risk of Childhood Leukemia: An Overview. Arch. Med. Res. 2016, 47, 607–614. [Google Scholar] [CrossRef]
- Walsh, L.; Kaiser, J.C. Multi-model inference of adult and childhood leukaemia excess relative risks based on the Japanese A-bomb survivors mortality data (1950–2000). Radiat. Environ. Biophys. 2011, 50, 21–35. [Google Scholar] [CrossRef]
- Ozasa, K.; Shimizu, Y.; Suyama, A.; Kasagi, F.; Soda, M.; Grant, E.J.; Sakata, R.; Sugiyama, H.; Kodama, K. Studies of the mortality of atomic bomb survivors, Report 14, 1950–2003: An overview of cancer and noncancer diseases. Radiat. Res. 2012, 177, 229–243. [Google Scholar] [CrossRef] [PubMed]
- Preston, D.L.; Kusumi, S.; Tomonaga, M.; Izumi, S.; Ron, E.; Kuramoto, A.; Kamada, N.; Dohy, H.; Matsuo, T.; Matsui, T.; et al. Cancer incidence in atomic bomb survivors. Part III. Leukemia, lymphoma and multiple myeloma, 1950–1987. Radiat. Res. 1994, 137, S68–S97. [Google Scholar] [CrossRef]
- Preston, D.L.; Pierce, D.A.; Shimizu, Y.; Cullings, H.M.; Fujita, S.; Funamoto, S.; Kodama, K. Effect of recent changes in atomic bomb survivor dosimetry on cancer mortality risk estimates. Radiat. Res. 2004, 162, 377–389. [Google Scholar] [CrossRef] [PubMed]
- Preston, D.L.; Cullings, H.; Suyama, A.; Funamoto, S.; Nishi, N.; Soda, M.; Mabuchi, K.; Kodama, K.; Kasagi, F.; Shore, R.E. Solid cancer incidence in atomic bomb survivors exposed in utero or as young children. J. Natl. Cancer Inst. 2008, 100, 428–436. [Google Scholar] [CrossRef] [PubMed]
- Richardson, D.; Sugiyama, H.; Nishi, N.; Sakata, R.; Shimizu, Y.; Grant, E.J.; Soda, M.; Hsu, W.L.; Suyama, A.; Kodama, K.; et al. Ionizing radiation and leukemia mortality among Japanese Atomic Bomb Survivors, 1950–2000. Radiat. Res. 2009, 172, 368–382. [Google Scholar] [CrossRef] [PubMed]
- Wakeford, R. The risk of childhood leukaemia following exposure to ionising radiation—A review. J. Radiol. Prot. 2013, 33, 1. [Google Scholar] [CrossRef] [PubMed]
- Łęcka, M.; Słomka, A.; Albrecht, K.; Żekanowska, E.; Romiszewski, M.; Styczyński, J. Unbalance in Iron Metabolism in Childhood Leukemia Converges with Treatment Intensity: Biochemical and Clinical Analysis. Cancers 2021, 13, 3029. [Google Scholar] [CrossRef] [PubMed]
- Stiller, C.A. Epidemiology and genetics of childhood cancer. Oncogene 2004, 23, 6429–6444. [Google Scholar] [CrossRef]
- Buffler, P.A.; Kwan, M.L.; Reynolds, P.; Urayama, K.Y. Environmental and genetic risk factors for childhood leukemia: Appraising the evidence. Cancer Investig. 2005, 23, 60–75. [Google Scholar] [CrossRef]
- Belson, M.; Kingsley, B.; Holmes, A. Risk factors for acute leukemia in children: A review. Environ. Health Perspect. 2007, 115, 138–145. [Google Scholar] [CrossRef]
- Biondi-Zoccai, G. Umbrella Reviews: Evidence Synthesis with Overviews of Reviews and Meta-Epidemiologic Studies; Springer International Publishing Switzerland: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- Fusar-Poli, P.; Radua, J. Ten simple rules for conducting umbrella reviews. Evid. Based Ment. Health 2018, 21, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Koch-Institut, R. Der Bundes-Gesundheitssurvey–Baustein der Gesundheitssurveillance in Deutschland. Available online: https://www.rki.de/DE/Content/Gesundheitsmonitoring/Gesundheitsberichterstattung/GBEDownloadsB/bausteine_gesundheitssurveillance.pdf?__blob=publicationFile (accessed on 12 November 2021).
- Statistisches Bundesamt. Available online: https://de.statista.com/statistik/daten/studie/217/umfrage/kinder-in-tageseinrichtungen-nach-altersgruppen/ (accessed on 12 November 2021).
- Kersting, M.; Hockamp, N.; Burak, C.; Lücke, T. Studie zur Erhebung von Daten zum Stillen und zur Säuglingsernährung in Deutschland–SuSe II. In: Deutsche Gesellschaft für Ernährung (Hrsg.): 14. DGE-Ernährungsbericht. Vorveröffentlichung Kapitel 3. Bonn (2020) V1–V 34. Available online: http://www.dge.de/14-dge-eb/vvoe/kap3 (accessed on 12 November 2021).
- SuSeII. Available online: https://www.dge.de/fileadmin/public/doc/ws/dgeeb/14-dge-eb/14-DGE-EB-Vorveroeffentlichung-Kapitel3.pdf (accessed on 12 November 2021).
- Rudnicka, J. Verteilung der Kinder in Tageseinrichtungen nach Altersgruppen. Available online: https://de.statista.com/statistik/daten/studie/217/umfrage/kinder-in-tageseinrichtungen-nach-altersgruppen/ (accessed on 12 November 2021).
- KiGGS2. Available online: https://www.rki.de/DE/Content/Gesundheitsmonitoring/Gesundheitsberichterstattung/GBEDownloadsJ/FactSheets/JoHM_01_2018_Rauchen_Schwangerschaft_KiGGS-Welle2.pdf?__blob=publicationFile (accessed on 12 November 2021).
- Die soziale Situation in Deutschland. Available online: https://www.bpb.de/nachschlagen/zahlen-und-fakten/soziale-situation-in-deutschland/61597/haushalte-nach-zahl-der-kinder (accessed on 12 November 2021).
- Robert Koch-Institut. Available online: https://www.rki.de/DE/Content/Gesundheitsmonitoring/Studien/Adipositas_Monitoring/Vor_und_nach_Geburt/PDF_Themenblatt_Geburtsgewicht.pdf?__blob=publicationFile (accessed on 12 November 2021).
- KiKK. Available online: https://www.ippnw.de/commonFiles/pdfs/Atomenergie/bfs_KiKK-Studie.pdf (accessed on 12 November 2021).
- Bundesministerium für Familie, Senioren, Frauen und Jugend. Available online: https://www.bmfsfj.de/resource/blob/161018/2027ee7422f420d004ebcb026bbb277b/ungewollte-kinderlosigkeit-2020-data.pdf (accessed on 12 November 2021).
- Bergmann, K.E.; Bergmann, R.L.; Ellert, U.; Dudenhausen, J.W. Perinatale Einflussfaktoren auf die spätere Gesundheit. Bundesgesundheitsblatt Gesundh. 2007, 50, 670–676. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bergmann, R.L.; Spohr, H.L.; Dudenhausen, J.W. Alkohol in der Schwangerschaft: Häufigkeit und Folgen; Urban und Vogel: Munich, Germany, 2006. [Google Scholar]
- Cornelia, L.; Kristin, M.; Benjamin, K. Alcohol consumption among adults in Germany: Risky drinking levels. J. Health Monit. 2017, 2. [Google Scholar] [CrossRef]
- Kaletsch, U.; Kaatsch, P.; Meinert, R.; Schuz, J.; Czarwinski, R.; Michaelis, J. Childhood cancer and residential radon exposure—Results of a population-based case-control study in Lower Saxony (Germany). Radiat. Environ. Biophys. 1999, 38, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Merzenich, H.; Schmiedel, S.; Bennack, S.; Brüggemeyer, H.; Philipp, J.; Blettner, M.; Schüz, J. Childhood Leukemia in Relation to Radio Frequency Electromagnetic Fields in the Vicinity of TV and Radio Broadcast Transmitters. Am. J. Epidemiol. 2008, 168, 1169–1178. [Google Scholar] [CrossRef] [PubMed]
- Michaelis, J.; Schüz, J.; Meinert, R.; Menger, M.; Grigat, J.P.; Kaatsch, P.; Kaletsch, U.; Miesner, A.; Stamm, A.; Brinkmann, K.; et al. Childhood leukemia and electromagnetic fields: Results of a population-based case-control study in Germany. Cancer Causes Control 1997, 8, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Statistisches Bundesamt. Available online: https://www.destatis.de/DE/Presse/Pressemitteilungen/2020/10/PD20_411_12.html (accessed on 12 November 2021).
- Bailey, H.D.; Fritschi, L.; Metayer, C.; Infante-Rivard, C.; Magnani, C.; Petridou, E.; Roman, E.; Spector, L.G.; Kaatsch, P.; Clavel, J.; et al. Parental occupational paint exposure and risk of childhood leukemia in the offspring: Findings from the Childhood Leukemia International Consortium. Cancer Causes Control 2014, 25, 1351–1367. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed]
- Talibov, M.; Olsson, A.; Bailey, H.; Erdmann, F.; Metayer, C.; Magnani, C.; Petridou, E.; Auvinen, A.; Spector, L.; Clavel, J.; et al. Parental occupational exposure to low-frequency magnetic fields and risk of leukaemia in the offspring: Findings from the Childhood Leukaemia International Consortium (CLIC). Occup. Environ. Med. 2019, 76, 746–753. [Google Scholar] [CrossRef] [PubMed]
- Petridou, E.T.; Georgakis, M.K.; Erdmann, F.; Ma, X.; Heck, J.E.; Auvinen, A.; Mueller, B.A.; Spector, L.G.; Roman, E.; Metayer, C.; et al. Advanced parental age as risk factor for childhood acute lymphoblastic leukemia: Results from studies of the Childhood Leukemia International Consortium. Eur. J. Epidemiol. 2018, 33, 965–976. [Google Scholar] [CrossRef] [PubMed]
- Bailey, H.D.; Metayer, C.; Milne, E.; Petridou, E.T.; Infante-Rivard, C.; Spector, L.G.; Clavel, J.; Dockerty, J.D.; Zhang, L.P.; Armstrong, B.K.; et al. Home paint exposures and risk of childhood acute lymphoblastic leukemia: Findings from the Childhood Leukemia International Consortium. Cancer Causes Control 2015, 26, 1257–1270. [Google Scholar] [CrossRef]
- Bailey, H.D.; Infante-Rivard, C.; Metayer, C.; Clavel, J.; Lightfoot, T.; Kaatsch, P.; Roman, E.; Magnani, C.; Spector, L.G.; Th Petridou, E.; et al. Home pesticide exposures and risk of childhood leukemia: Findings from the childhood leukemia international consortium. Int. J. Cancer 2015, 137, 2644–2663. [Google Scholar] [CrossRef]
- Bailey, H.D.; Fritschi, L.; Infante-Rivard, C.; Glass, D.C.; Miligi, L.; Dockerty, J.D.; Lightfoot, T.; Clavel, J.; Roman, E.; Spector, L.G.; et al. Parental occupational pesticide exposure and the risk of childhood leukemia in the offspring: Findings from the childhood leukemia international consortium. Int. J. Cancer 2014, 135, 2157–2172. [Google Scholar] [CrossRef]
- Van Maele-Fabry, G.; Gamet-Payrastre, L.; Lison, D. Household exposure to pesticides and risk of leukemia in children and adolescents: Updated systematic review and meta-analysis. Int. J. Hyg. Environ. Health 2019, 222, 49–67. [Google Scholar] [CrossRef] [PubMed]
- Vinson, F.; Merhi, M.; Baldi, I.; Raynal, H.; Gamet-Payrastre, L. Exposure to pesticides and risk of childhood cancer: A meta-analysis of recent epidemiological studies. Occup. Environ. Med. 2011, 68, 694–702. [Google Scholar] [CrossRef]
- Wigle, D.T.; Turner, M.C.; Krewski, D. A Systematic Review and Meta-analysis of Childhood Leukemia and Parental Occupational Pesticide Exposure. Environ. Health Perspect. 2009, 117, 1505–1513. [Google Scholar] [CrossRef]
- Chunxia, D.; Meifang, W.; Jianhua, Z.; Ruijuan, Z.; Xiue, L.; Zhuanzhen, Z.; Linhua, Y. Tobacco smoke exposure and the risk of childhood acute lymphoblastic leukemia and acute myeloid leukemia: A meta-analysis. Medicine 2019, 98, e16454. [Google Scholar] [CrossRef]
- Liu, R.; Zhang, L.; McHale, C.M.; Hammond, S.K. Paternal Smoking and Risk of Childhood Acute Lymphoblastic Leukemia: Systematic Review and Meta-Analysis. J. Oncol. 2011, 2011, 854584. [Google Scholar] [CrossRef]
- Cao, Y.; Lu, J.; Lu, J. Paternal Smoking before Conception and During Pregnancy Is Associated With an Increased Risk of Childhood Acute Lymphoblastic Leukemia: A Systematic Review and Meta-Analysis of 17 Case-Control Studies. J. Pediatric Hematol. Oncol. 2020, 42, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Karalexi, M.A.; Dessypris, N.; Thomopoulos, T.P.; Ntouvelis, E.; Kantzanou, M.; Diamantaras, A.A.; Moschovi, M.; Baka, M.; Hatzipantelis, E.; Kourti, M.; et al. Parental alcohol consumption and risk of leukemia in the offspring: A systematic review and meta-analysis. Eur. J. Cancer Prev. 2017, 26, 433–441. [Google Scholar] [CrossRef]
- Zhou, Y.F.; Zhang, S.Z.; Li, Z.; Zhu, J.; Bi, Y.Y.; Bai, Y.; Wang, H. Maternal Benzene Exposure during Pregnancy and Risk of Childhood Acute Lymphoblastic Leukemia: A Meta-Analysis of Epidemiologic Studies. PLoS ONE 2014, 9, e110466. [Google Scholar] [CrossRef] [PubMed]
- Turner, M.C.; Wigle, D.T.; Krewski, D. Residential pesticides and childhood leukemia: A systematic review and meta-analysis. Environ. Health Perspect. 2010, 118, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Latino-Martel, P.; Chan, D.S.; Druesne-Pecollo, N.; Barrandon, E.; Hercberg, S.; Norat, T. Maternal alcohol consumption during pregnancy and risk of childhood leukemia: Systematic review and meta-analysis. Cancer Epidemiol. Biomark. Prev. 2010, 19, 1238–1260. [Google Scholar] [CrossRef]
- Milne, E.; Greenop, K.R.; Petridou, E.; Bailey, H.D.; Orsi, L.; Kang, A.Y.; Baka, M.; Bonaventure, A.; Kourti, M.; Metayer, C.; et al. Maternal consumption of coffee and tea during pregnancy and risk of childhood ALL: A pooled analysis from the childhood Leukemia International Consortium. Cancer Causes Control 2018, 29, 539–550. [Google Scholar] [CrossRef]
- Thomopoulos, T.P.; Ntouvelis, E.; Diamantaras, A.A.; Tzanoudaki, M.; Baka, M.; Hatzipantelis, E.; Kourti, M.; Polychronopoulou, S.; Sidi, V.; Stiakaki, E.; et al. Maternal and childhood consumption of coffee, tea and cola beverages in association with childhood leukemia: A meta-analysis. Cancer Epidemiol. 2015, 39, 1047–1059. [Google Scholar] [CrossRef]
- Cheng, J.; Su, H.; Zhu, R.; Wang, X.; Peng, M.; Song, J.; Fan, D. Maternal coffee consumption during pregnancy and risk of childhood acute leukemia: A metaanalysis. Am. J. Obs. Gynecol. 2014, 210, 151.e1–151.e10. [Google Scholar] [CrossRef]
- Klimentopoulou, A.; Antonopoulos, C.N.; Papadopoulou, C.; Kanavidis, P.; Tourvas, A.D.; Polychronopoulou, S.; Baka, M.; Athanasiadou-Piperopoulou, F.; Kalmanti, M.; Sidi, V.; et al. Maternal smoking during pregnancy and risk for childhood leukemia: A nationwide case-control study in Greece and meta-analysis. Pediatr. Blood Cancer 2012, 58, 344–351. [Google Scholar] [CrossRef]
- Hargreave, M.; Jensen, A.; Deltour, I.; Brinton, L.A.; Andersen, K.K.; Kjaer, S.K. Increased risk for cancer among offspring of women with fertility problems. Int. J. Cancer 2013, 133, 1180–1186. [Google Scholar] [CrossRef]
- Metayer, C.; Milne, E.; Dockerty, J.D.; Clavel, J.; Pombo-de-Oliveira, M.S.; Wesseling, C.; Spector, L.G.; Schüz, J.; Petridou, E.; Ezzat, S.; et al. Maternal supplementation with folic acid and other vitamins and risk of leukemia in offspring: A Childhood Leukemia International Consortium study. Epidemiology 2014, 25, 811–822. [Google Scholar] [CrossRef]
- Ismail, W.R.W.; Rahman, R.A.; Rahman, N.A.A.; Atil, A.; AM, N. The Protective Effect of Maternal Folic Acid Supplementation on Childhood Cancer: A Systematic Review and Meta-analysis of Case-control Studies. J. Prev. Med. Public Health 2019, 52, 205–213. [Google Scholar] [CrossRef]
- Son, M.; Kim, J.; Oh, J.; Kawachi, I. Inequalities in childhood cancer mortality according to parental socioeconomic position: A birth cohort study in South Korea. Soc. Sci. Med. 2011, 72, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Caughey, R.W.; Michels, K.B. Birth weight and childhood leukemia: A meta-analysis and review of the current evidence. Int. J. Cancer 2009, 124, 2658–2670. [Google Scholar] [CrossRef]
- Hjalgrim, L.L.; Westergaard, T.; Rostgaard, K.; Schmiegelow, K.; Melbye, M.; Hjalgrim, H.; Engels, E.A. Birth weight as a risk factor for childhood leukemia: A meta-analysis of 18 epidemiologic studies. Am. J. Epidemiol. 2003, 158, 724–735. [Google Scholar] [CrossRef] [PubMed]
- Milne, E.; Greenop, K.R.; Metayer, C.; Schüz, J.; Petridou, E.; Pombo-de-Oliveira, M.S.; Infante-Rivard, C.; Roman, E.; Dockerty, J.D.; Spector, L.G.; et al. Fetal growth and childhood acute lymphoblastic leukemia: Findings from the childhood leukemia international consortium. Int. J. Cancer 2013, 133, 2968–2979. [Google Scholar] [CrossRef]
- Che, H.; Long, D.; Sun, Q.; Wang, L.; Li, Y. Birth Weight and Subsequent Risk of Total Leukemia and Acute Leukemia: A Systematic Review and Meta-Analysis. Front. Pediatrics 2021, 9, 722471. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Gao, P.; Liang, G.; Zhang, N.; Wang, C.; Wang, Y.; Nie, L.; Lv, X.; Li, W.; Guo, Q.; et al. Maternal prenatal exposure to environmental factors and risk of childhood acute lymphocytic leukemia: A hospital-based case-control study in China. Cancer Epidemiol. 2019, 58, 146–152. [Google Scholar] [CrossRef]
- Huang, Q.; Gao, Y.; Zhong, M.L.; Yan, Y. Preterm Birth and Subsequent Risk of Acute Childhood Leukemia: A Meta-Analysis of Observational Studies. Cell Physiol. Biochem. 2016, 2016, 1229–1238. [Google Scholar] [CrossRef]
- Orsi, L.; Magnani, C.; Petridou, E.T.; Dockerty, J.D.; Metayer, C.; Milne, E.; Bailey, H.D.; Dessypris, N.; Kang, A.Y.; Wesseling, C.; et al. Living on a farm, contact with farm animals and pets, and childhood acute lymphoblastic leukemia: Pooled and meta-analyses from the Childhood Leukemia International Consortium. Cancer Med. 2018, 7, 2665–2681. [Google Scholar] [CrossRef]
- Marcotte, E.L.; Richardson, M.R.; Roesler, M.A.; Spector, L.G. Cesarean Delivery and Risk of Infant Leukemia: A Report from the Children’s Oncology Group. Cancer Epidemiol. Biomark. Prev. 2018, 27, 473–478. [Google Scholar] [CrossRef]
- Sun, X.X.; Zhang, S.S.; Ma, X.L. No association between traffic density and risk of childhood leukemia: A meta-analysis. Asian Pac. J. Cancer Prev. 2014, 15, 5229–5232. [Google Scholar] [CrossRef]
- Filippini, T.; Hatch, E.E.; Rothman, K.J.; Heck, J.E.; Park, A.S.; Crippa, A.; Orsini, N.; Vinceti, M. Association between Outdoor Air Pollution and Childhood Leukemia: A Systematic Review and Dose Response Meta-Analysis. Environ. Health Perspect. 2019, 127. [Google Scholar] [CrossRef]
- Filippini, T.; Heck, J.E.; Malagoli, C.; Del Giovane, C.; Vinceti, M. A review and meta-analysis of outdoor air pollution and risk of childhood leukemia. J. Environ. Sci. Health C Environ. Carcinog. Ecotoxicol. Rev. 2015, 33, 36–66. [Google Scholar] [CrossRef] [PubMed]
- Schüz, J.; Svendsen, A.L.; Linet, M.S.; McBride, M.L.; Roman, E.; Feychting, M.; Kheifets, L.; Lightfoot, T.; Mezei, G.; Simpson, J.; et al. Nighttime exposure to electromagnetic fields and childhood leukemia: An extended pooled analysis. Am. J. Epidemiol. 2007, 166, 263–269. [Google Scholar] [CrossRef]
- Ahlbom, A.; Day, N.; Feychting, M.; Roman, E.; Skinner, J.; Dockerty, J.; Linet, M.; McBride, M.; Michaelis, J.; Olsen, J.H.; et al. A pooled analysis of magnetic fields and childhood leukaemia. Br. J. Cancer 2000, 83, 692–698. [Google Scholar] [CrossRef]
- Greenland, S.; Sheppard, A.; Kaune, W.; Poole, C.; Kelsh, M. A Pooled Analysis of Magnetic Fields, Wire Codes, and Childhood Leukemia. Epidemiology 2000, 11, 624–634. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Liu, X.; Wang, C.; Yan, K.; Lin, X.; Li, S.; Bao, H.; Liu, X. Magnetic fields exposure and childhood leukemia risk: A meta-analysis based on 11,699 cases and 13,194 controls. Leuk. Res. 2014, 38, 269–274. [Google Scholar] [CrossRef]
- Amoon, A.T.; Swanson, J.; Magnani, C.; Johansen, C.; Kheifets, L. Pooled analysis of recent studies of magnetic fields and childhood leukemia. Environ. Res. 2021, 204, 111993. [Google Scholar] [CrossRef]
- Seomun, G.; Lee, J.; Park, J. Exposure to extremely low-frequency magnetic fields and childhood cancer: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0251628. [Google Scholar] [CrossRef]
- Kheifets, L.; Crespi, C.M.; Hooper, C.; Cockburn, M.; Amoon, A.T.; Vergara, X.P. Residential magnetic fields exposure and childhood leukemia: A population-based case–control study in California. Cancer Causes Control 2017, 28, 1117–1123. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, C.; Johansen, C.; Schuz, J.; Olsen, J.H.; Raaschou-Nielsen, O. Residential exposure to extremely low-frequency magnetic fields and risk of childhood leukaemia, CNS tumour and lymphoma in Denmark. Br. J. Cancer 2015, 113, 1370–1374. [Google Scholar] [CrossRef]
- Salvan, A.; Ranucci, A.; Lagorio, S.; Magnani, C.; On behalf of the SETIL Research Group. Childhood Leukemia and 50 Hz Magnetic Fields: Findings from the Italian SETIL Case-Control Study. Int. J. Environ. Res. Public Health 2015, 12, 2184–2204. [Google Scholar] [CrossRef] [PubMed]
- Bunch, K.J.; Swanson, J.; Vincent, T.J.; Murphy, M.F. Epidemiological study of power lines and childhood cancer in the UK: Further analyses. J. Radiol. Prot. 2016, 36, 437–455. [Google Scholar] [CrossRef]
- Rudant, J.; Lightfoot, T.; Urayama, K.Y.; Petridou, E.; Dockerty, J.D.; Magnani, C.; Milne, E.; Spector, L.G.; Ashton, L.J.; Dessypris, N.; et al. Childhood Acute Lymphoblastic Leukemia and Indicators of Early Immune Stimulation: A Childhood Leukemia International Consortium Study. Am. J. Epidemiol. 2015, 181, 549–562. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.M.; Gunnell, D.; Owen, C.G.; Smith, G.D. Breast-feeding and childhood cancer: A systematic review with metaanalysis. Int. J. Cancer 2005, 117, 1020–1031. [Google Scholar] [CrossRef] [PubMed]
- Amitay, E.L.; Dubnov Raz, G.; Keinan-Boker, L. Breastfeeding, Other Early Life Exposures and Childhood Leukemia and Lymphoma. Nutr. Cancer 2016, 68, 968–977. [Google Scholar] [CrossRef]
- Kwan, M.L.; Buffler, P.A.; Abrams, B.; Kiley, V.A. Breastfeeding and the risk of childhood leukemia: A meta-analysis. Public Health Rep. 2004, 119, 521–535. [Google Scholar] [CrossRef]
- Urayama, K.Y.; Buffler, P.A.; Gallagher, E.R.; Ayoob, J.M.; Ma, X. A meta-analysis of the association between day-care attendance and childhood acute lymphoblastic leukaemia. Int. J. Epidemiol. 2010, 39, 718–732. [Google Scholar] [CrossRef]
- Chen, M.; Chang, C.H.; Tao, L.; Lu, C. Residential Exposure to Pesticide during Childhood and Childhood Cancers: A Meta-Analysis. Pediatrics 2015, 136, 719–729. [Google Scholar] [CrossRef]
- Little, M.P.; Wakeford, R.; Borrego, D.; French, B.; Zablotska, L.B.; Adams, M.J.; Allodji, R.; de Vathaire, F.; Lee, C.; Brenner, A.V.; et al. Leukaemia and myeloid malignancy among people exposed to low doses (<100 mSv) of ionising radiation during childhood: A pooled analysis of nine historical cohort studies. Lancet Haematol. 2018, 5, e346–e358. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Liu, L.; Chen, Q.; Wei, J.; Cao, G.; Zhang, J. Domestic radon exposure and risk of childhood leukemia: A meta-analysis. J. Buon. 2020, 25, 1035–1041. [Google Scholar]
- Baker, P.J.; Hoel, D.G. Meta-analysis of standardized incidence and mortality rates of childhood leukaemia in proximity to nuclear facilities. Eur. J. Cancer Care 2007, 16, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Nasterlack, M. Pesticides and childhood cancer: An update. Int. J. Hyg. Environ. Health 2007, 210, 645–657. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, S.; Ali, S.; Ali, I. Maternal pesticide exposure and its relation to childhood cancer: An umbrella review of meta-analyses. Int. J. Environ. Health Res. 2021, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Boros, L.G.; Williams, R.D. Isofenphos induced metabolic changes in K562 myeloid blast cells1This work was supported by the PHS M01-RR00425 of the General Clinical Research Unit and by P01-CA42710 of the UCLA Clinical Nutrition Research Unit Stable Isotope Core.1. Leuk. Res. 2001, 25, 883–890. [Google Scholar] [CrossRef]
- Williams, R.D.; Boros, L.G.; Kolanko, C.J.; Jackman, S.M.; Eggers, T.R. Chromosomal aberrations in human lymphocytes exposed to the anticholinesterase pesticide isofenphos with mechanisms of leukemogenesis. Leuk. Res. 2004, 28, 947–958. [Google Scholar] [CrossRef]
- IARC. Non-ionizing radiation, Part 1: Static and extremely low-frequency (ELF) electric and magnetic fields. IARC Monogr. Eval. Carcinog. Risks Hum. 2002, 80, 1–395. [Google Scholar]
- Wakeford, R.; Little, M.P.; Kendall, G.M. Risk of childhood leukemia after low-level exposure to ionizing radiation. Expert Rev. Hematol. 2010, 3, 251–254. [Google Scholar] [CrossRef] [PubMed]
- Bergsagel, D.E.; Wong, O.; Bergsagel, P.L.; Alexanian, R.; Anderson, K.; Kyle, R.A.; Raabe, G.K. Benzene and multiple myeloma: Appraisal of the scientific evidence. Blood 1999, 94, 1174–1182. [Google Scholar]
- Onyije, F.M.; Hosseini, B.; Togawa, K.; Schüz, J.; Olsson, A. Cancer Incidence and Mortality among Petroleum Industry Workers and Residents Living in Oil Producing Communities: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 4343. [Google Scholar] [CrossRef]
- McKenzie, L.M.; Allshouse, W.B.; Byers, T.E.; Bedrick, E.J.; Serdar, B.; Adgate, J.L. Childhood hematologic cancer and residential proximity to oil and gas development. PLoS ONE 2017, 12, e0170423. [Google Scholar] [CrossRef]
- Carlos-Wallace, F.M.; Zhang, L.; Smith, M.T.; Rader, G.; Steinmaus, C. Parental, In Utero, and Early-Life Exposure to Benzene and the Risk of Childhood Leukemia: A Meta-Analysis. Am. J. Epidemiol. 2016, 183, 1–14. [Google Scholar] [CrossRef]
- Mosallanejad, Z.; Fakhri, Y.; Ferrante, M.; Zandsalimi, Y.; Amirhajeloo, L.R.; Amanidaz, N.; Moradi, B.; Keramati, H. Association between benzene exposure and childhood leukemia: A systematic review and meta-analysis updated to July 2016. Int. J. Pharm. Technol. 2016, 8, 4640–4652. [Google Scholar]
- Scelo, G.; Metayer, C.; Zhang, L.P.; Wiemels, J.L.; Aldrich, M.C.; Selvin, S.; Month, S.; Smith, M.T.; Buffler, P.A. Household Exposure to Paint and Petroleum Solvents, Chromosomal Translocations, and the Risk of Childhood Leukemia. Environ. Health Perspect. 2009, 117, 133–139. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bailey, H.D.; Milne, E.; de Klerk, N.H.; Fritschi, L.; Attia, J.; Cole, C.; Armstrong, B.K. Exposure to house painting and the use of floor treatments and the risk of childhood acute lymphoblastic leukemia. Int. J. Cancer 2011, 128, 2405–2414. [Google Scholar] [CrossRef] [PubMed]
- Lowengart, R.A.; Peters, J.M.; Cicioni, C.; Buckley, J.; Bernstein, L.; Preston-Martin, S.; Rappaport, E. Childhood leukemia and parents’ occupational and home exposures. J. Natl. Cancer Inst. 1987, 79, 39–46. [Google Scholar]
- Freedman, D.M.; Stewart, P.; Kleinerman, R.A.; Wacholder, S.; Hatch, E.E.; Tarone, R.E.; Robison, L.L.; Linet, M.S. Household solvent exposures and childhood acute lymphoblastic leukemia. Am. J. Public Health 2001, 91, 564–567. [Google Scholar] [CrossRef][Green Version]
- Schuz, J.; Spector, L.G.; Ross, J.A. Bias in studies of parental self-reported occupational exposure and childhood cancer. Am. J. Epidemiol. 2003, 158, 710–716. [Google Scholar] [CrossRef] [PubMed]
- Kyrgiou, M.; Kalliala, I.; Markozannes, G.; Gunter, M.J.; Paraskevaidis, E.; Gabra, H.; Martin-Hirsch, P.; Tsilidis, K.K. Adiposity and cancer at major anatomical sites: Umbrella review of the literature. BMJ 2017, 356, j477. [Google Scholar] [CrossRef] [PubMed]
- Ge, C.B.; Friesen, M.C.; Kromhout, H.; Peters, S.; Rothman, N.; Lan, Q.; Vermeulen, R. Use and Reliability of Exposure Assessment Methods in Occupational Case–Control Studies in the General Population: Past, Present, and Future. Ann. Work Expo. Health 2018, 62, 1047–1063. [Google Scholar] [CrossRef]
- Stewart, P. Challenges to retrospective exposure assessment. Scand. J. Work Environ. Health 1999, 25, 505–510. [Google Scholar] [CrossRef]
- Lunny, C.; Pieper, D.; Thabet, P.; Kanji, S. Managing overlap of primary study results across systematic reviews: Practical considerations for authors of overviews of reviews. BMC Med. Res. Methodol. 2021, 21, 140. [Google Scholar] [CrossRef]
- Urayama, K.Y.; Ma, X.; Buffler, P.A. Exposure to infections through day-care attendance and risk of childhood leukaemia. Radiat. Prot. Dosim. 2008, 132, 259–266. [Google Scholar] [CrossRef][Green Version]


{kind=link}
| Authors | Study Design | Number of Study | Exposure Group | Exposure Type/Agent | * Evidence | Leukemia | † Prevalence | ‡ RR 95% CI |
|---|---|---|---|---|---|---|---|---|
| Talibov et al., 2019 | Pooled analysis | 11 | Electromagnetic fields | >0.2 µT | 1.09, 0.99–1.19 | |||
| >0.1–≤0.2 µT | 0.93, 0.86–1.00 | |||||||
| >0.2–≤1 µT | 1.04, 0.93–1.16 | |||||||
| >1 µT | No | B-lineage ALL | Rare | 0.91, 0.62–1.31 | ||||
| Petridou et al., 2018 | Pooled analysis | 15 | Intrinsic | Paternal age (increased age) | Little | ALL | Rare | 1.05, 1.00–1.11 |
| Karalexi et al., 2017 | Systematic review | 9 | Lifestyle, behaviour, infection | Paternal alcohol | No | ALL | Moderate | 1.10, 0.93–1.30 |
| Chunxia et al., 2019 | Systematic review | 8 | Lifestyle, behaviour, infection | Paternal smoking (Preconception) | 1.15, 1.01–1.30 | |||
| Liu et al. 2011 | Systematic review | 13 | Paternal smoking | 1.25, 1.08–1.46 | ||||
| Cao et al., 2020 | Systematic review | 8 | Paternal smoking | Some | ALL | High | 1.15, 1.04–1.27 | |
| Bailey et al., 2014b | Pooled analysis | 12 | Paint | Occupational painting | 0.94, 0.76–1.15 | |||
| Bailey et al., 2015b | Pooled analysis | 5 | Domestic painting within 1–3 months before conception | 1.52, 1.25–1.86 | ||||
| 2 | Domestic painting within the year before conception | Little | B-lineage ALL | Rare | 1.01, 0.86–1.19 | |||
| Van Maele-Fabry et al., 2019 | Systematic review | 4 | Pesticides | General | ALL | 1.30, 1.12–1.51 | ||
| Bailey et al., 2014a | Pooled analysis | 14 | General-paternal occupational pesticide | B-lineage ALL | 1.14, 0.85–1.54 | |||
| Bailey et al., 2015a | Pooled analysis | 2 | General-occupational pest control treatments | B-lineage ALL | 1.24, 1.03–1.50 | |||
| Vinson et al., 2011 | Systematic review | 18 | General | Leukemia | 1.32, 1.20–1.46 | |||
| Wigle et al., 2009 | Systematic review | 30 | General | Some | Leukemia | Modest | 1.09, 0.88–1.34 | |
| Bailey et al., 2015a | Pooled analysis | 12 | Pesticides | Home pesticide | 1.41, 1.25–1.59 | |||
| 5 | Household insecticide/miticide | 1.34, 1.19–1.51 | ||||||
| 5 | Insecticide or fungicide | Strong | B-lineage ALL | Modest | 1.49, 1.14–1.95 | |||
| 5 | Pesticide used on pets | Little | B-lineage ALL | NA | 1.17, 1.02–1.34 | |||
| 5 | Herbicide | 1.23, 1.04–1.45 | ||||||
| 5 | Rodenticide | 1.39, 1.10–1.76 | ||||||
| 5 | Molluscicide | Some | B-lineage ALL | Modest | 1.06, 0.79–1.43 |
| Authors | Study Design | Number of Study | Exposure Group | Exposure Type/Agent | * Evidence | Leukemia | † Prevalence | ‡ RR 95% CI |
|---|---|---|---|---|---|---|---|---|
| Talibov et al., 2019 | Pooled analysis | 11 | Electromagnetic fields | >0.2 | 0.98, 0.85–1.12 | |||
| >0.1–≤0.2 | 0.95, 0.89–1.02 | |||||||
| >0.2 | No | B-lineage ALL | Rare | 0.96, 0.83–1.10 | ||||
| Karalexi et al., 2017 | Systematic review | 24 | Lifestyle, behaviour, infection | Maternal alcohol | ALL | 0.97, 0.85–1.11 | ||
| Systematic review | 8 | Maternal alcohol-moderate | 1.13, 0.84–1.52 | |||||
| Systematic review | 8 | Maternal alcohol-high | 0.98, 0.71–1.36 | |||||
| Latino-Martel et al., 2010 | Systematic review | 11 | Maternal alcohol | No | ALL | Moderate | 1.10, 0.93–1.29 | |
| Thomopoulos et al., 2015 | Systematic review | 8 | Lifestyle, behaviour, infection | Maternal coffee consumption (High) | ALL | 1.43, 1.22–1.68 | ||
| Systematic review | 9 | Maternal coffee consumption (Low to moderate) | 1.01, 0.90–1.13 | |||||
| Milne et al., 2018 | Pooled analysis | 7 | Coffee > 2 cups/day | B-lineage ALL | 1.28, 1.09–1.50 | |||
| Cheng et al., 2014 | Systematic review | 5 | Maternal coffee consumption (ever drinkers) | Some | ALL | NA | 1.26, 1.05–1.50 | |
| Milne et al., 2018 | Pooled analysis | 5 | Lifestyle, behaviour, infection | Maternal tea consumption >2 cups/day | B-lineage ALL | 0.99, 0.80–1.24 | ||
| Thomopoulos et al., 2015 | Systematic review | 6 | Maternal tea consumption (High) | ALL | 0.99, 0.84–1.18 | |||
| Systematic review | 8 | Maternal tea consumption (Low to moderate) | No | ALL | NA | 0.90, 0.79–1.04 | ||
| Thomopoulos et al., 2015 | Systematic review | 2 | Lifestyle, behaviour, infection | Maternal cola consumption (High) | ALL | 1.25, 0.95–1.66 | ||
| 3 | Maternal cola consumption (Low to moderate) | 1.24, 1.03–1.49 | ||||||
| Cheng et al., 2014 | Systematic review | 5 | Maternal cola consumption (Low to moderate) | ALL | 1.09, 0.91–1.31 | |||
| 5 | Maternal cola consumption (High) | Some | NA | 1.65, 1.28–2.12 | ||||
| Chunxia et al., 2019 | Systematic review | 9 | Lifestyle, behaviour, infection | Maternal smoking (preconception) | ALL | Common | 1.05, 0.97–1.12 | |
| Chunxia et al., 2019 | Systematic review | 8 | Paternal smoking during pregnancy | ALL | High | 1.23, 0.99–1.53 | ||
| Klimentopoulou et al., 2012 | Systematic review | 20 | Maternal smoking during pregnancy | ALL | Common | 1.03, 0.95–1.12 | ||
| Chunxia et al., 2019 | Systematic review | 12 | Maternal smoking during pregnancy | ALL | Common | 0.97, 0.90–1.05 | ||
| Zhou et al., 2014 | Systematic review | 18 | Maternal smoking during pregnancy | ALL | Common | 0.99, 0.96–109 | ||
| Liu et al., 2011 | Systematic review | 8 | Paternal smoking during pregnancy | ALL | High | 1.24, 1.07–1.43 | ||
| Cao et al., 2020 | Systematic review | 9 | Paternal smoking during pregnancy | Little | ALL | Common | 1.20, 1.12–1.28 | |
| Hargreave et al., 2014 | Systematic review | 11 | Lifestyle, behaviour, infection | Fertility treatment | Some | Leukemia | Modest | 1.65, 1.35–2.01 |
| Metayer et al., 2014 | Pooled analysis | 8 | Maternal Folic Acid | ALL | 0.80, 0.71–0.89 | |||
| Ismail et al., 2019 | Systematic review | 11 | Maternal Folic Acid | ALL | 0.75, 0.66–0.86 | |||
| Metayer et al., 2014 | Pooled analysis | 12 | Vitamin | ALL | 0.85, 0.78–0.92 | |||
| Goh et al., 2007 | Systematic review | 2 | Multivitamin Supplementation | Some(inverse) | ALL | High | 0.61, 0.50–0.74 | |
| Rudant et al., 2015 | Pooled analysis | 11 | Intrinsic | Birth order ≥ 2 | ALL | 0.94, 0.88–1.00 | ||
| Birth order 2 | High | 0.95, 0.88–1.01 | ||||||
| Birth order 3 | Common | 0.95, 0.87–1.05 | ||||||
| Birth order 4 | Modest | 0.86, 0.73–1.00 | ||||||
| Birth order 5 | Rare | 0.92, 0.70–1.21 | ||||||
| Birth order ≥ 6 | No | Rare | 0.93, 0.68–1.29 | |||||
| Milne et al., 2013 | Pooled analysis | 12 | Intrinsic | Weight (large-for-gestational-age) | ALL | 1.21, 1.11–1.32 | ||
| Hjalgrim et al., 2003 | Systematic review | 18 | High birth weight = ≥4000 g | ALL | 1.26, 1.17–1.37 | |||
| Caughey et al., 2009 | Systematic review | 23 | High birth weight | ALL | 1.23, 1.15–1.32 | |||
| Che et al., 2021 | Systematic review | 25 | High birth weight | Some | ALL | Rare | 1.28, 1.20–1.35 | |
| Wang et al., 2018 | Systematic review | 11 | Intrinsic | Preterm birth | ALL | 1.04, 0.97–1.11 | ||
| Huang et al., 2016 | Systematic review | 8 | Preterm Birth | ALL | 1.04, 0.96–1.13 | |||
| Caughey et al., 2009 | Systematic review | 10 | Low birth weight | ALL | 0.97, 0.81–1.16 | |||
| Wang et al., 2018 | Systematic review | 10 | Gestational age-post-term birth | ALL | 1.03, 0.95–1.12 | |||
| Che et al., 2021 | Systematic review | 27 | Low birth weight | No | ALL | NA | 0.83, 0.75–0.92 | |
| Marcotte et al., 2016 | Pooled analysis | 13 | Intrinsic | Caesarean delivery | ALL | 1.06, 0.99–1.13 | ||
| Prelabour caesarean delivery | Little | NA | 1.23, 1.04–1.47 | |||||
| Petridou et al., 2018 | Pooled analysis | 15 | Intrinsic | Maternal age (increased) | ALL | 1.05, 1.00–1.08 | ||
| Orsi et al., 2018 | Maternal age > 35 | Little | ALL | Rare | 0.98, 0.89–1.08 | |||
| Pooled analysis | 13 | Maternal age < 25 | Some | ALL | Rare | 1.20, 1.11–1.29 | ||
| Yan et al., 2020 | Systematic review | 9 | Intrinsic | Maternal diabetes | Some | ALL | NA | 1.44, 1.27–1.64 |
| Bailey et al., 2014b | Pooled analysis | 4 | Paint | Occupational paint (Maternal) | B-lineage ALL | 0.79, 0.36–1.71 | ||
| Bailey et al., 2015b | Pooled analysis | 8 | Home paint-Any paint exposure | B-lineage ALL | 1.14, 1.04–1.25 | |||
| 8 | Home paint-Mother used paint | Little | Rare | 1.13, 0.95–1.33 | ||||
| Wigle et al., 2009 | Systematic review | 16 | Pesticides | General | Leukemia | 2.09, 1.51–2.88 | ||
| Vinson et al., 2011 | Systematic review | 25 | General | Leukemia | 1.48, 1.26–1.75 | |||
| Turner et al., 2010 | Systematic review | 5 | General | ALL | 2.04, 1.54–2.68 | |||
| 4 | General-Indoor exposure | 1.86, 1.25–2.77 | ||||||
| 5 | General-Outdoor exposure | 1.50, 0.98–2.32 | ||||||
| Bailey et al., 2014a | Pooled analysis | 12 | General-maternal occupational | B-lineage ALL | 1.04, 0.78–1.38 | |||
| Bailey et al., 2015a | Pooled analysis | 6 | General-maternal professional pest control | 1.19, 1.04–1.36 | ||||
| Van Maele-Fabry et al., 2019 | Systematic review | 5 | General | ALL | 1.39, 1.21–1.60 | |||
| 5 | General-Indoor exposure | Strong | Modest | 1.27, 1.07–1.51 | ||||
| Bailey et al., 2015a | Pooled analysis | 12 | Pesticides | Home pesticide | B-lineage ALL | 1.47, 1.35–1.61 | ||
| 6 | Pesticides | Household insecticide/miticide | Some | Modest | 1.28, 1.18–1.38 | |||
| Turner et al., 2010 | Systematic review | 4 | Pesticides | Insecticides | 2.14, 1.83–2.50 | |||
| Herbicides | 1.73, 1.28–2.35 | |||||||
| Van Maele-Fabry et al., 2019 | Systematic review | 5 | Insecticides | ALL | 1.28, 1.07–1.53 | |||
| 3 | Herbicides | 1.34, 1.32–1.36 | ||||||
| Bailey et al., 2015a | Pooled analysis | 2 | Insect repellent (Personal) | B-lineage ALL | 1.42, 1.15–1.77 | |||
| 6 | Herbicide | 1.34, 1.19–1.50 | ||||||
| 3 | Rodenticide | 1.42, 1.17–1.73 | ||||||
| 3 | Molluscicide | 1.01, 0.79–1.28 | ||||||
| 6 | Insecticide or fungicide | Some | Modest | 1.26, 1.11–1.44 | ||||
| Bailey et al., 2015a | Pooled analysis | 5 | Pesticides | Pesticide used on pets | Little | B-lineage ALL | NA | 1.15, 1.03–1.29 |
| Zhou et al., 2014 | Systematic review | 7 | Chemicals | Solvent | 1.25, 1.09–1.45 | |||
| 7 | Petroleum | Some | ALL | NA | 1.42, 1.10–1.84 |
| Authors | Study Design | Number of Study | Exposure Group | Exposure Type/Agent | * Evidence | Leukemia/Sub Type | † Prevalence | ‡ RR 95% CI |
|---|---|---|---|---|---|---|---|---|
| Sun et al., 2014 | Systematic review | 11 | Air pollution | Traffic density | Leukemia | 1.03, 0.98–1.09 | ||
| Filippini et al., 2019 | Systematic review | 16 | Traffic density | Leukemia | 1.09, 1.00–1.20 | |||
| 9 | Traffic density | ALL | 1.05, 0.96–1.16 | |||||
| 3 | Traffic density <6 years | Little | ALL | NA | 1.02, 0.99–1.05 | |||
| 7 | Nitrogen Dioxide | Leukemia | 1.04, 0.90–1.19 | |||||
| 4 | Nitrogen Dioxide | ALL | 1.02, 0.89–1.18 | |||||
| 2 | Nitrogen Dioxide children <6 years | No | ALL | High | 1.10, 0.92–1.32 | |||
| Filippini et al., 2015 | Systematic review | 4 | Chemicals | Proximity to petrol station | Leukemia | 1.83, 1.42–2.36 | ||
| Filippini et al., 2019 | Systematic review | 8 | Benzene | Leukemia | 1.27, 1.03–1.56 | |||
| 7 | Benzene | ALL | 1.09, 0.88–1.36 | |||||
| Benzene children < 6 years | Some | ALL | NA | 1.19, 1.00–1.40 | ||||
| Schuz et al., 2007 | Pooled analysis | 4 | Electromagnetic fields | ELF-MF (10:00 p.m.–6:00 a.m.) 0.1 ≤ 0.2 µT | Leukemia | 1.11, 0.91–1.36 | ||
| ELF-MF (10:00 p.m.–6:00 a.m.) 0.2 ≤ 0.4 µT | 1.37, 0.99–1.90 | |||||||
| ELF-MF (10:00 p.m.–6:00 a.m.) ≥ 0.4 µT | 1.93, 1.11–3.35 | |||||||
| ELF-MF 24-/48-h 0.1 ≤ 0.2 µT | 1.09, 0.89–1.32 | |||||||
| ELF-MF 24-/48-h 0.2 ≤ 0.4 µT | 1.20, 0.89–1.06 | |||||||
| ELF-MF24-/48-h ≥ 0.4 µT | 1.98, 1.18–3.35 | |||||||
| Ahlbom et al., 2000 | Pooled analysis | 9 | ELF-MF 0.1 ≤ 0.2 µT | Leukemia | 1.08, 0.88–1.32 | |||
| 9 | ELF-MF 0.2 ≤ 0.4 µT | 1.12, 0.84–1.51 | ||||||
| 9 | ELF-MF ≥ 0.4 µT | 2.08, 1.30–3.33 | ||||||
| 7 | ELF-MF 0.1 ≤ 0.2 µT | 1.07, 0.81–1.41 | ||||||
| 7 | ELF-MF 0.2 ≤ 0.3 µT | 1.16, 0.69–1.93 | ||||||
| 7 | ELF-MF ≥ 0.3 µT | 1.44, 0.88–2.36 | ||||||
| Greenland et al., 2000 | Pooled analysis | 12 | ELF-MF 0.1–0.2 µT—Wire Code Alone | Leukemia | 1.02, 0.81–1.29 | |||
| ELF-MF 0.2–0.3 µT—Wire Code Alone | 1.01, 0.69–1.48 | |||||||
| ELF-MF > 0.3 µT—Wire Code Alone | 1.38, 0.89–2.13 | |||||||
| Zhao et al., 2014 | Systematic review | 7 | ELF-MF 0.1 ≤ 0.2 µT | ALL | 1.09, 0.85–1.39 | |||
| ELF-MF 0.2 ≤ 0.4 µT | ALL | 1.04, 0.73–1.48 | ||||||
| ELF-MF ≥ 0.4 µT | ALL | 2.43, 1.30–4.55 | ||||||
| Greenland et al., 2000 | Pooled analysis | 12 | ELF-MF 2 µT | Leukemia | 1.08, 0.86–1.35 | |||
| ELF-MF 0.2–0.3 µT | 1.10, 0.76–1.60 | |||||||
| ELF-MF > 0.3 µT | 1.52, 0.99–2.33 | |||||||
| Amoon et al., 2021 | Pooled analysis | 4 | ELF-MF ≥ 0.4 μT | Leukemia | 1.01, 0.61–1.66 | |||
| ELF-MF 0.1 ≤ 0.2 μT | 1.10, 0.80–1.53 | |||||||
| ELF-MF 0.2 ≤ 0.4 μT | 0.75, 0.46–1.21 | |||||||
| Seomun et al., 2021 | Systematic review | 27 | ELF-MF 0.4µT | Some | Leukemia | Rare | 1.72, 1.25–2.35 | |
| Liu et al., 2011 | Systematic review | 7 | Lifestyle, behaviour, infection | Paternal smoking | High | 1.24, 0.96–1.60 | ||
| Chunxia et al., 2019 | Systematic review | 3 | Maternal smoking | Common | 0.84, 0.59–1.19 | |||
| Rudant et al., 2015 | Pooled analysis | 11 | Lifestyle, behaviour, infection | Breastfeeding | ALL | 0.95, 0.89–1.02 | ||
| Breastfeeding < 6 months | 1.01, 0.94–1.08 | |||||||
| Breastfeeding ≥ 6 months | 0.86, 0.79–0.94 | |||||||
| Breastfeeding | 0.95, 0.89–1.02 | |||||||
| Breastfeeding < 6 months | 1.01, 0.94–1.08 | |||||||
| Breastfeeding ≥ 6 months | 0.86, 0.79–0.94 | |||||||
| Martin et al., 2005 | Systematic review | 17 | Breastfeeding | 0.91, 0.84–0.98 | ||||
| Amitay et al., 2015 | Systematic review | 11 | Breastfeeding | 0.82, 0.73–0.93 | ||||
| Kwan et al., 2004 | Systematic review | 14 | Breastfeeding | High | 0.76, 0.68–0.84 | |||
| Urayama et al., 2010 | Systematic review | 9 | Lifestyle, behaviour, infection | Day-care attendance any time | 0.81, 0.70–0.94 | |||
| 11 | Day-care attendance at age ≤ 2 | 0.79, 0.65–0.95 | ||||||
| Rudant et al., 2015 | Pooled analysis | 11 | Day-care centre attendance at <1 year of age | 0.77, 0.71–0.84 | ||||
| 11 | Day-care centre attendance at <1 year of age | Some(inverse) | High | 0.77, 0.71–0.84 | ||||
| Orsi et al., 2018 | Pooled analysis | 13 | Lifestyle, behaviour, infection | Living on a farm | No | ALL | NA | 1.09, 0.86–1.36 |
| Orsi et al., 2018 | Pooled analysis | 13 | Lifestyle, behaviour, infection | Contact with any pets | Some(inverse) | ALL | 0.90, 0.84–0.96 | |
| Bailey et al., 2015b | Pooled analysis | 4 | Paint | Home paint-Any paint exposure | Some | B-lineage ALL | Rare | 1.22, 1.07–1.39 |
| Bailey et al., 2015a | Pooled analysis | 5 | General-Professional pest control treatments | B-lineage ALL | Modest | 1.28,1.14–1.45 | ||
| Van Maele-Fabry et al., 2019 | Systematic review | 8 | Pesticides | General | ALL | 1.42, 1.13–1.80 | ||
| 3 | General | 1.24, 0.90–1.70 | ||||||
| 3 | General-Indoor exposure | 1.19, 0.90–1.57 | ||||||
| 3 | General-Out door exposure | 1.27, 0.93–1.72 | ||||||
| Turner et al., 2010 | Systematic review | 4 | General | ALL | 1.40, 0.90–2.16 | |||
| Turner et al., 2010 | Systematic review | 3 | General-Indoor exposure | 1.56, 1.02–2.39 | ||||
| Turner et al., 2010 | Systematic review | 4 | General-Outdoor exposure | 1.40, 1.05–1.87 | ||||
| Chen et al., 2015 | Systematic review | 6 | General-Indoor | ALL | 1.59, 1.40–1.80 | |||
| Chen et al., 2015 | Systematic review | 6 | General-Outdoor | 1.15, 0.95–1.38 | ||||
| Chen et al., 2015 | Systematic review | 7 | General-Indoor pesticides-professional home | Some | Modest | 1.55, 1.38–1.75 | ||
| Chen et al., 2015 | Systematic review | 7 | Home pesticide | 1.46, 1.29–1.65 | ||||
| Chen et al., 2015 | Systematic review | 5 | Insecticides indoor | 1.59, 1.39–1.81 | ||||
| Bailey et al., 2015a | Pooled analysis | 12 | Home pesticide | 1.35, 1.21, 1.52 | ||||
| Bailey et al., 2015a | Pooled analysis | 5 | Household insecticide/miticide | Some | B-lineage ALL | Modest | 1.23, 1.12–1.34 | |
| Vinson et al., 2011 | Systematic review | 20 | Pesticides | Herbicides | Leukemia | 1.26, 1.14–1.39 | ||
| Vinson et al., 2011 | Systematic review | 45 | Insecticides | 1.17, 1.03–1.33 | ||||
| Bailey et al., 2015a | Pooled analysis | 5 | Insecticide or fungicide | B-lineage ALL | 1.41, 1.26–1.59 | |||
| Bailey et al., 2015a | Pooled analysis | 2 | Insect repellent (Personal) | 1.02, 0.86–1.20 | ||||
| Bailey et al., 2015a | Pooled analysis | 5 | Herbicide | 1.34, 1.21–1.48 | ||||
| Bailey et al., 2015a | Pooled analysis | 3 | Rodenticide | 1.32, 1.12–1.56 | ||||
| Bailey et al., 2015a | Pooled analysis | 3 | Molluscicide | B-lineage ALL | 1.06, 0.87–1.30 | |||
| Chen et al., 2015 | Systematic review | 9 | Insecticides-Outdoor | 1.11, 0.60–2.05 | ||||
| Chen et al., 2015 | Systematic review | 5 | Herbicides Outdoor | 1.26, 1.10–1.44 | ||||
| Van Maele-Fabry et al., 2019 | Systematic review | 3 | Insecticides | ALL | 1.19, 0.90–1.57 | |||
| Van Maele-Fabry et al., 2019 | Systematic review | 3 | Herbicides | 1.24, 0.96–1.60 | ||||
| Turner et al., 2010 | Systematic review | 3 | Insecticides | ALL | 1.35, 0.76–2.38 | |||
| Turner et al., 2010 | Systematic review | 4 | Herbicides | Some | Modest | 0.85, 0.43–1.66 | ||
| Bailey et al., 2015a | Pooled analysis | 6 | Pesticide used on pets | B-lineage ALL | NA | 1.15, 1.03–1.29 | ||
| Baker and Hoel, 2007 | Systematic review | 6 | Radiation | Proximity to nuclear facilities Incidence All | 1.25, 1.13–1.38 | |||
| 6 | Radiation | Proximity to nuclear facilities Incidence < 16 km | 1.23, 1.07–1.40 | |||||
| 6 | Radiation | Proximity to nuclear facilities Mortality All | 1.06, 1.01–1.11 | |||||
| 6 | Radiation | Proximity to nuclear facilities Mortality < 16 km | Some | Leukemia | Modest | 1.23, 1.04–1.46 | ||
| Lu et al., 2020 | Systematic review | 8 | Radiation | Domestic radon | 1.22, 1.01–1.42 | |||
| 2 | Radiation | Domestic radon | Conflicting | Leukemia | Moderate | 0.97, 0.81–1.15 | ||
| Little et al., 2018 | Systematic review | 7 | Radiation | Low doses of ionising radiation 5–9.99 mSv | ALL | 2.41, 0.64–8.65 | ||
| Radiation | Low doses of ionising radiation 10–19.99 mSv | 4.45, 1.50–14.08 | ||||||
| Radiation | Low doses of ionising radiation 20–49.99 mSv | 4.20, 1.35–13.28 | ||||||
| Radiation | Low doses of ionising radiation 50–100 mSv | 3.97, 0.97–14.15 | ||||||
| Radiation | Low doses of ionising radiation RR at 100 mSv | Strong | Modest | 5.66, 1.35–19.71 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Onyije, F.M.; Olsson, A.; Baaken, D.; Erdmann, F.; Stanulla, M.; Wollschläger, D.; Schüz, J. Environmental Risk Factors for Childhood Acute Lymphoblastic Leukemia: An Umbrella Review. Cancers 2022, 14, 382. https://doi.org/10.3390/cancers14020382
Onyije FM, Olsson A, Baaken D, Erdmann F, Stanulla M, Wollschläger D, Schüz J. Environmental Risk Factors for Childhood Acute Lymphoblastic Leukemia: An Umbrella Review. Cancers. 2022; 14(2):382. https://doi.org/10.3390/cancers14020382
Chicago/Turabian StyleOnyije, Felix M., Ann Olsson, Dan Baaken, Friederike Erdmann, Martin Stanulla, Daniel Wollschläger, and Joachim Schüz. 2022. "Environmental Risk Factors for Childhood Acute Lymphoblastic Leukemia: An Umbrella Review" Cancers 14, no. 2: 382. https://doi.org/10.3390/cancers14020382
APA StyleOnyije, F. M., Olsson, A., Baaken, D., Erdmann, F., Stanulla, M., Wollschläger, D., & Schüz, J. (2022). Environmental Risk Factors for Childhood Acute Lymphoblastic Leukemia: An Umbrella Review. Cancers, 14(2), 382. https://doi.org/10.3390/cancers14020382