
Emerging Novel Therapeutic Approaches for Treatment of Advanced Cutaneous Melanoma

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Novel Immunecheckpoint Inhbitors
3.1.1. Anti-LAG3
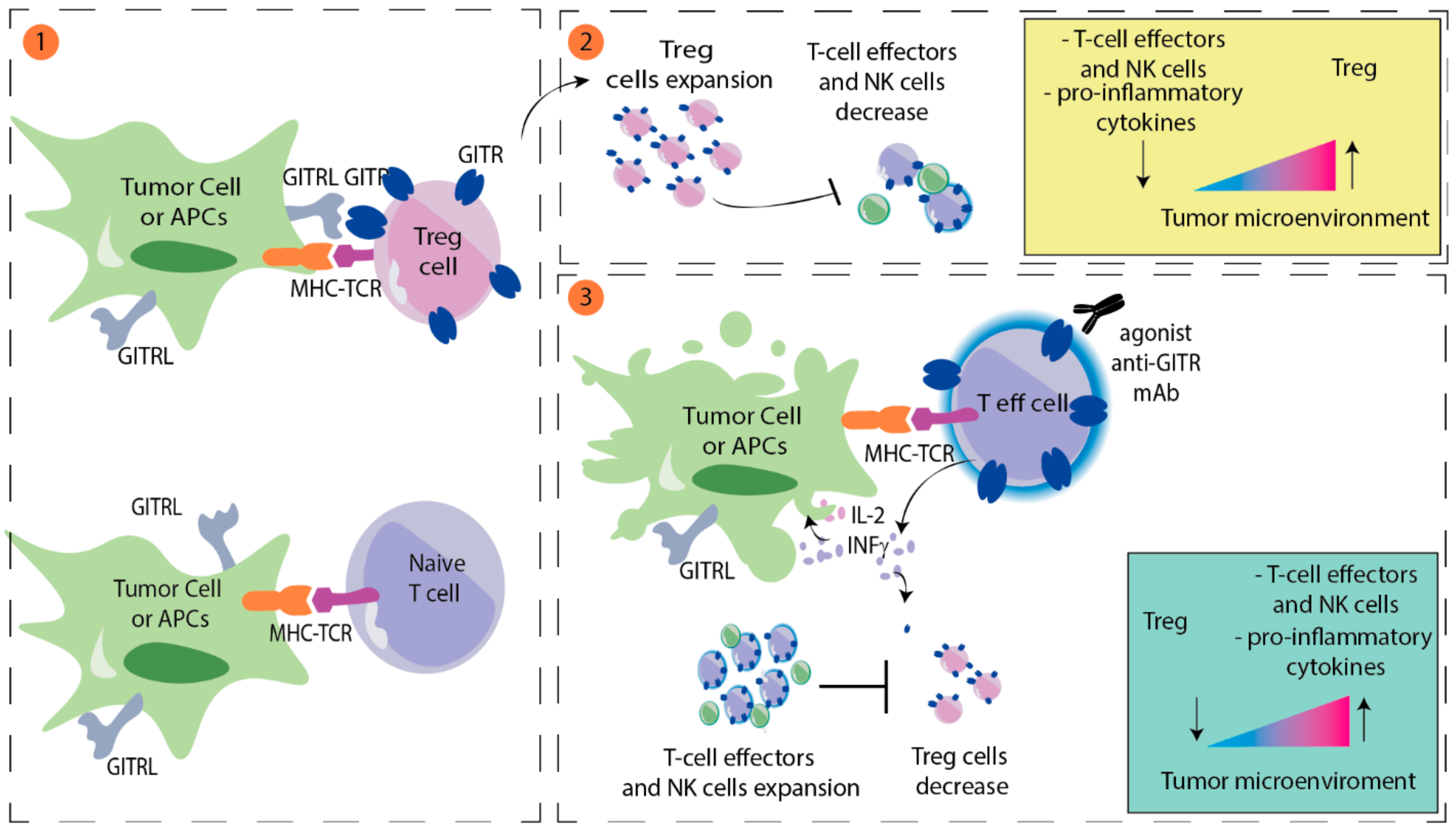
3.1.2. GITR Agonist
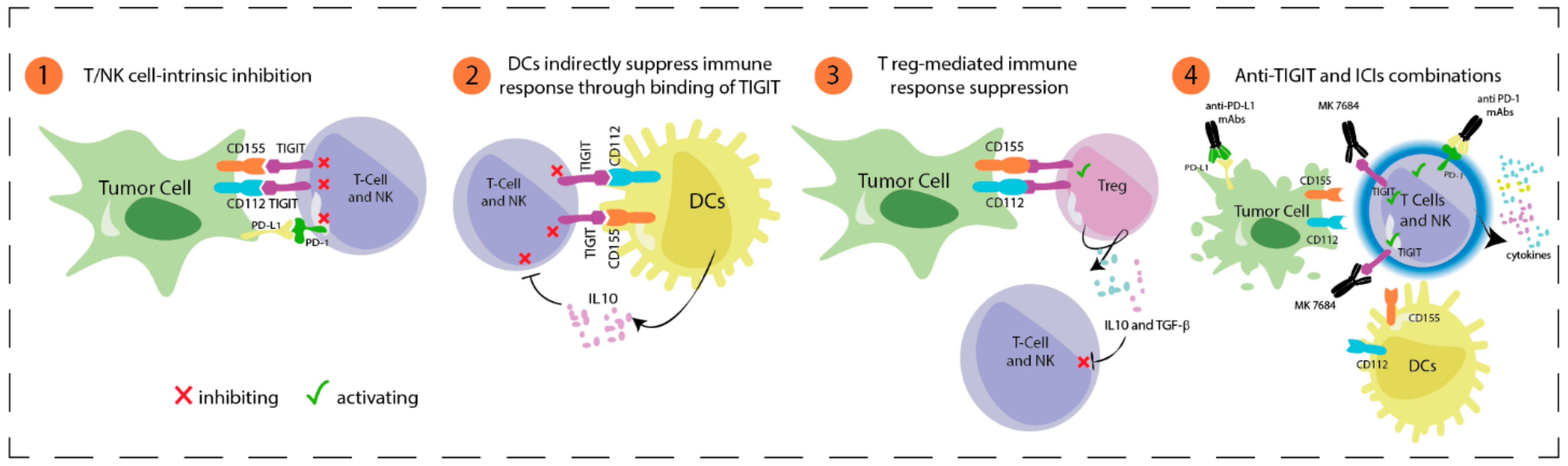
3.1.3. Anti-TIGIT
3.2. Adoptive Cell Therapy
3.3. Vaccines
3.3.1. Peptide Vaccines
3.3.2. Dendritic Cell Vaccines
3.3.3. RNA Vaccines
3.4. Engineered TCR Therapy
3.5. Interleukin-2
3.6. Targeted Therapy
3.6.1. New MEK or RAF Inhibitors
3.6.2. CDK4/6 Inhibitors
3.6.3. ERK Inhibitors
3.6.4. HDAC Inhibitors
3.6.5. IDO Inhibitors
3.6.6. Anti-Angiogenic Therapy
3.6.7. AXL Inhibitors
3.6.8. PARP Inhibitors
3.6.9. ATR Inhibitors
3.7. Combination of Intratumoral and Systemic Immunotherapy
3.7.1. Oncolytic Virus
3.7.2. Toll-like Receptor (TLR) 9 Agonist
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Schadendorf, D.; van Akkooi, A.C.J.; Berking, C.; Griewank, K.G.; Gutzmer, R.; Hauschild, A.; Stang, A.; Roesch, A.; Ugurel, S. Melanoma. Lancet 2018, 392, 971–984. [Google Scholar] [CrossRef]
- Robert, C.; Thomas, L.; Bondarenko, I.; O’Day, S.; Weber, J.; Garbe, C.; Lebbe, C.; Baurain, J.-F.; Testori, A.; Grob, J.-J.; et al. Ipilimumab plus Dacarbazine for Previously Untreated Metastatic Melanoma. N. Engl. J. Med. 2011, 364, 2517–2526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robert, C.; Long, G.V.; Brady, B.; Dutriaux, C.; Maio, M.; Mortier, L.; Hassel, J.C.; Rutkowski, P.; McNeil, C.; Kalinka-Warzocha, E.; et al. Nivolumab in Previously Untreated Melanoma without BRAF Mutation. N. Engl. J. Med. 2015, 372, 320–330. [Google Scholar] [CrossRef] [Green Version]
- Robert, C.; Schachter, J.; Long, G.V.; Arance, A.; Grob, J.J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.; Lotem, M.; et al. Pembrolizumab versus Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2015, 372, 2521–2532. [Google Scholar] [CrossRef] [PubMed]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Dummer, R.; Smylie, M.; Rutkowski, P.; et al. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma. N. Engl. J. Med. 2015, 373, 23–34. [Google Scholar] [CrossRef] [Green Version]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Five-Year Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2019, 381, 1535–1546. [Google Scholar] [CrossRef] [Green Version]
- Hamid, O.; Robert, C.; Daud, A.; Hodi, F.S.; Hwu, W.J.; Kefford, R.; Wolchok, J.D.; Hersey, P.; Joseph, R.; Weber, J.S.; et al. Five-Year Survival Outcomes for Patients with Advanced Melanoma Treated with Pembrolizumab in KEYNOTE-001. Ann. Oncol. 2019, 30, 582–588. [Google Scholar] [CrossRef]
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. CheckMate 067: 6.5-Year Outcomes in Patients (Pts) with Advanced Melanoma. J. Clin. Oncol. 2021, 39, 9506. [Google Scholar] [CrossRef]
- Chapman, P.B.; Hauschild, A.; Robert, C.; Haanen, J.B.; Ascierto, P.; Larkin, J.; Dummer, R.; Garbe, C.; Testori, A.; Maio, M.; et al. Improved Survival with Vemurafenib in Melanoma with BRAF V600E Mutation. N. Engl. J. Med. 2011, 364, 2507–2516. [Google Scholar] [CrossRef] [Green Version]
- Hauschild, A.; Grob, J.-J.; Demidov, L.V.; Jouary, T.; Gutzmer, R.; Millward, M.; Rutkowski, P.; Blank, C.U.; Miller, W.H.; Kaempgen, E.; et al. Dabrafenib in BRAF-Mutated Metastatic Melanoma: A Multicentre, Open-Label, Phase 3 Randomised Controlled Trial. Lancet 2012, 380, 358–365. [Google Scholar] [CrossRef]
- Robert, C.; Karaszewska, B.; Schachter, J.; Rutkowski, P.; Mackiewicz, A.; Stroiakovski, D.; Lichinitser, M.; Dummer, R.; Grange, F.; Mortier, L.; et al. Improved Overall Survival in Melanoma with Combined Dabrafenib and Trametinib. N. Engl. J. Med. 2014, 372, 30–39. [Google Scholar] [CrossRef] [Green Version]
- Ascierto, P.A.; McArthur, G.A.; Dréno, B.; Atkinson, V.; Liszkay, G.; Di Giacomo, A.M.; Mandalà, M.; Demidov, L.; Stroyakovskiy, D.; Thomas, L.; et al. Cobimetinib Combined with Vemurafenib in Advanced BRAFV600-Mutant Melanoma (CoBRIM): Updated Efficacy Results from a Randomised, Double-Blind, Phase 3 Trial. Lancet Oncol. 2016, 17, 1248–1260. [Google Scholar] [CrossRef]
- Robert, C.; Grob, J.J.; Stroyakovskiy, D.; Karaszewska, B.; Hauschild, A.; Levchenko, E.; Chiarion Sileni, V.; Schachter, J.; Garbe, C.; Bondarenko, I.; et al. Five-Year Outcomes with Dabrafenib plus Trametinib in Metastatic Melanoma. N. Engl. J. Med. 2019, 381, 626–636. [Google Scholar] [CrossRef] [PubMed]
- Ascierto, P.A.; Dummer, R.; Gogas, H.J.; Flaherty, K.T.; Arance, A.; Mandala, M.; Liszkay, G.; Garbe, C.; Schadendorf, D.; Krajsova, I.; et al. Update on Tolerability and Overall Survival in COLUMBUS: Landmark Analysis of a Randomised Phase 3 Trial of Encorafenib plus Binimetinib vs Vemurafenib or Encorafenib in Patients with BRAF V600–Mutant Melanoma. Eur. J. Cancer 2020, 126, 33–44. [Google Scholar] [CrossRef] [Green Version]
- Dummer, R.; Flaherty, K.; Robert, C.; Arance, A.M.; de Groot, J.W.; Garbe, C.; Gogas, H.; Gutzmer, R.; Krajsová, I.; Liszkay, G.; et al. Five-Year Overall Survival (OS) in COLUMBUS: A Randomized Phase 3 Trial of Encorafenib plus Binimetinib versus Vemurafenib or Encorafenib in Patients (Pts) with BRAF V600-Mutant Melanoma. J. Clin. Oncol. 2021, 39, 9507. [Google Scholar] [CrossRef]
- Qin, S.; Xu, L.; Yi, M.; Yu, S.; Wu, K.; Luo, S. Novel Immune Checkpoint Targets: Moving beyond PD-1 and CTLA-4. Mol. Cancer 2019, 18, 155. [Google Scholar] [CrossRef] [PubMed]
- Ascierto, P.A.; Bono, P.; Bhatia, S.; Melero, I.; Nyakas, M.S.; Svane, I.-M.; Larkin, J.; Gomez-Roca, C.; Schadendorf, D.; Dummer, R.; et al. Efficacy of BMS-986016, a Monoclonal Antibody That Targets Lymphocyte Activation Gene-3 (LAG-3), in Combination with Nivolumab in Pts with Melanoma Who Progressed during Prior Anti–PD-1/PD-L1 Therapy (Mel Prior IO) in All-Comer and Biomarker-Enriched Populations. Ann. Oncol. 2017, 28, v611–v612. [Google Scholar] [CrossRef]
- Lipson, E.J.; Tawbi, H.A.-H.; Schadendorf, D.; Ascierto, P.A.; Matamala, L.; Gutiérrez, E.C.; Rutkowski, P.; Gogas, H.; Lao, C.D.; Janoski de Menezes, J.; et al. Relatlimab (RELA) plus Nivolumab (NIVO) versus NIVO in First-Line Advanced Melanoma: Primary Phase III Results from RELATIVITY-047 (CA224-047). J. Clin. Oncol. 2021, 39, 9503. [Google Scholar] [CrossRef]
- Rohatgi, A.; Massa, R.C.; Gooding, W.E.; Bruno, T.C.; Vignali, D.; Kirkwood, J.M. A Phase II Study of Anti-PD1 Monoclonal Antibody (Nivolumab) Administered in Combination with Anti-LAG3 Monoclonal Antibody (Relatlimab) in Patients with Metastatic Melanoma Naive to Prior Immunotherapy in the Metastatic Setting. J. Clin. Oncol. 2020, 38, TPS10085. [Google Scholar] [CrossRef]
- Hamid, O.; Wang, D.; Kim, T.M.; Kim, S.-W.; Lakhani, N.J.; Johnson, M.L.; Groisberg, R.; Papadopoulos, K.P.; Kaczmar, J.M.; Middleton, M.R.; et al. Clinical Activity of Fianlimab (REGN3767), a Human Anti-LAG-3 Monoclonal Antibody, Combined with Cemiplimab (Anti-PD-1) in Patients (Pts) with Advanced Melanoma. J. Clin. Oncol. 2021, 39, 9515. [Google Scholar] [CrossRef]
- Legg, J.; McGuinness, B.; Arasanz, H.; Bocanegra, A.; Bartlett, P.; Benedetti, G.; Birkett, N.; Cox, C.; Juan, E.; Enever, C.; et al. Abstract 930: CB213: A Half-Life Extended Bispecific Humabody V H Delivering Dual Checkpoint Blockade to Reverse the Dysfunction of LAG3 + PD-1 + Double-Positive T Cells; American Association for Cancer Research: Philadelphia, PA, USA, 2020; p. 930. [Google Scholar]
- Liu, B.; Li, Z.; Mahesh, S.P.; Pantanelli, S.; Hwang, F.S.; Siu, W.O.; Nussenblatt, R.B. Glucocorticoid-Induced Tumor Necrosis Factor Receptor Negatively Regulates Activation of Human Primary Natural Killer (NK) Cells by Blocking Proliferative Signals and Increasing NK Cell Apoptosis. J. Biol. Chem. 2008, 283, 8202–8210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoenhals, J.E.; Cushman, T.R.; Barsoumian, H.B.; Li, A.; Cadena, A.P.; Niknam, S.; Younes, A.I.; Caetano, M.D.S.; Cortez, M.A.; Welsh, J.W. Anti-Glucocorticoid-Induced Tumor Necrosis Factor–Related Protein (GITR) Therapy Overcomes Radiation-Induced Treg Immunosuppression and Drives Abscopal Effects. Front. Immunol. 2018, 9, 2170. [Google Scholar] [CrossRef] [Green Version]
- Sukumar, S.; Wilson, D.C.; Yu, Y.; Wong, J.; Naravula, S.; Ermakov, G.; Riener, R.; Bhagwat, B.; Necheva, A.S.; Grein, J.; et al. Characterization of MK-4166, a Clinical Agonistic Antibody That Targets Human GITR and Inhibits the Generation and Suppressive Effects of T Regulatory Cells. Cancer Res. 2017, 77, 4378–4388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaer, D.A.; Murphy, J.T.; Wolchok, J.D. Modulation of GITR for Cancer Immunotherapy. Curr. Opin. Immunol. 2012, 24, 217–224. [Google Scholar] [CrossRef] [Green Version]
- Narumi, K.; Miyakawa, R.; Shibasaki, C.; Henmi, M.; Mizoguchi, Y.; Ueda, R.; Hashimoto, H.; Hiraoka, N.; Yoshida, T.; Aoki, K. Local Administration of GITR Agonistic Antibody Induces a Stronger Antitumor Immunity than Systemic Delivery. Sci. Rep. 2019, 9, 5562. [Google Scholar] [CrossRef]
- Clouthier, D.L.; Watts, T.H. Cell-Specific and Context-Dependent Effects of GITR in Cancer, Autoimmunity, and Infection. Cytokine Growth Factor Rev. 2014, 25, 91–106. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, J.; Yamazaki, S.; Takahashi, T.; Ishida, Y.; Sakaguchi, S. Stimulation of CD25+CD4+ Regulatory T Cells through GITR Breaks Immunological Self-Tolerance. Nat. Immunol. 2002, 3, 135–142. [Google Scholar] [CrossRef]
- Heinhuis, K.M.; Carlino, M.; Joerger, M.; Di Nicola, M.; Meniawy, T.; Rottey, S.; Moreno, V.; Gazzah, A.; Delord, J.-P.; Paz-Ares, L.; et al. Safety, Tolerability, and Potential Clinical Activity of a Glucocorticoid-Induced TNF Receptor–Related Protein Agonist Alone or in Combination with Nivolumab for Patients with Advanced Solid Tumors. JAMA Oncol. 2020, 6, 100–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papadopoulos, K.P.; Autio, K.; Golan, T.; Dobrenkov, K.; Chartash, E.; Chen, Q.; Wnek, R.; Long, G.V. Phase I Study of MK-4166, an Anti-Human Glucocorticoid-Induced TNF Receptor Antibody, Alone or with Pembrolizumab in Advanced Solid Tumors. Clin. Cancer Res. 2021, 27, 1904–1911. [Google Scholar] [CrossRef]
- Chauvin, J.-M.; Zarour, H.M. TIGIT in Cancer Immunotherapy. J. Immunother. Cancer 2020, 8, e000957. [Google Scholar] [CrossRef]
- Chauvin, J.-M.; Pagliano, O.; Fourcade, J.; Sun, Z.; Wang, H.; Sander, C.; Kirkwood, J.M.; Chen, T.T.; Maurer, M.; Korman, A.J.; et al. TIGIT and PD-1 Impair Tumor Antigen–Specific CD8+ T Cells in Melanoma Patients. J. Clin. Investig. 2015, 125, 2046–2058. [Google Scholar] [CrossRef]
- Rosenberg, S.A.; Packard, B.S.; Aebersold, P.M.; Solomon, D.; Topalian, S.L.; Toy, S.T.; Simon, P.; Lotze, M.T.; Yang, J.C.; Seipp, C.A.; et al. Use of Tumor-Infiltrating Lymphocytes and Interleukin-2 in the Immunotherapy of Patients with Metastatic Melanoma. N. Engl. J. Med. 1988, 319, 1676–1680. [Google Scholar] [CrossRef]
- Nguyen, L.T.; Saibil, S.D.; Sotov, V.; Le, M.X.; Khoja, L.; Ghazarian, D.; Bonilla, L.; Majeed, H.; Hogg, D.; Joshua, A.M.; et al. Phase II Clinical Trial of Adoptive Cell Therapy for Patients with Metastatic Melanoma with Autologous Tumor-Infiltrating Lymphocytes and Low-Dose Interleukin-2. Cancer Immunol. Immunother. 2019, 68, 773–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenberg, S.A.; Yang, J.C.; Sherry, R.M.; Kammula, U.S.; Hughes, M.S.; Phan, G.Q.; Citrin, D.E.; Restifo, N.P.; Robbins, P.F.; Wunderlich, J.R.; et al. Durable Complete Responses in Heavily Pretreated Patients with Metastatic Melanoma Using T-Cell Transfer Immunotherapy. Clin. Cancer Res. 2011, 17, 4550–4557. [Google Scholar] [CrossRef] [Green Version]
- Dafni, U.; Michielin, O.; Lluesma, S.M.; Tsourti, Z.; Polydoropoulou, V.; Karlis, D.; Besser, M.J.; Haanen, J.; Svane, I.M.; Ohashi, P.S.; et al. Efficacy of Adoptive Therapy with Tumor-Infiltrating Lymphocytes and Recombinant Interleukin-2 in Advanced Cutaneous Melanoma: A Systematic Review and Meta-Analysis. Ann. Oncol. 2019, 30, 1902–1913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borch, T.H.; Andersen, R.; Ellebaek, E.; Met, Ö.; Donia, M.; Marie Svane, I. Future Role for Adoptive T-Cell Therapy in Checkpoint Inhibitor-Resistant Metastatic Melanoma. J. Immunother. Cancer 2020, 8, e000668. [Google Scholar] [CrossRef]
- Sarnaik, A.; Khushalani, N.I.; Chesney, J.A.; Lewis, K.D.; Medina, T.M.; Kluger, H.M.; Thomas, S.S.; Domingo Musibay, E.; Pavlick, A.C.; Whitman, E.D.; et al. Long-Term Follow up of Lifileucel (LN-144) Cryopreserved Autologous Tumor Infiltrating Lymphocyte Therapy in Patients with Advanced Melanoma Progressed on Multiple Prior Therapies. J. Clin. Oncol. 2020, 38, 10006. [Google Scholar] [CrossRef]
- Larkin, J.; Sarnaik, A.; Chesney, J.A.; Khushalani, N.I.; Kirkwood, J.M.; Weber, J.S.; Lewis, K.D.; Medina, T.M.; Kluger, H.M.; Thomas, S.S.; et al. Lifileucel (LN-144), a Cryopreserved Autologous Tumor Infiltrating Lymphocyte (TIL) Therapy in Patients with Advanced Melanoma: Evaluation of Impact of Prior Anti-PD-1 Therapy. J. Clin. Oncol. 2021, 39, 9505. [Google Scholar] [CrossRef]
- Mullinax, J.E.; Hall, M.; Prabhakaran, S.; Weber, J.; Khushalani, N.; Eroglu, Z.; Brohl, A.S.; Markowitz, J.; Royster, E.; Richards, A.; et al. Combination of Ipilimumab and Adoptive Cell Therapy with Tumor-Infiltrating Lymphocytes for Patients with Metastatic Melanoma. Front. Oncol. 2018, 8, 44. [Google Scholar] [CrossRef] [PubMed]
- Deniger, D.C.; Kwong, M.L.M.; Pasetto, A.; Dudley, M.E.; Wunderlich, J.R.; Langhan, M.M.; Lee, C.-C.R.; Rosenberg, S.A. A Pilot Trial of the Combination of Vemurafenib with Adoptive Cell Therapy in Patients with Metastatic Melanoma. Clin. Cancer Res. 2017, 23, 351–362. [Google Scholar] [CrossRef] [Green Version]
- Kwak, M.; Leick, K.M.; Melssen, M.M.; Slingluff, C.L., Jr. Vaccine Strategy in Melanoma. Surg. Oncol. Clin. N. Am. 2019, 28, 337–351. [Google Scholar] [CrossRef] [PubMed]
- Ott, P.A.; Hu, Z.; Keskin, D.B.; Shukla, S.A.; Sun, J.; Bozym, D.J.; Zhang, W.; Luoma, A.; Giobbie-Hurder, A.; Peter, L.; et al. An Immunogenic Personal Neoantigen Vaccine for Patients with Melanoma. Nature 2017, 547, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Slingluff, C.L.; Petroni, G.R.; Chianese-Bullock, K.A.; Smolkin, M.E.; Ross, M.I.; Haas, N.B.; von Mehren, M.; Grosh, W.W. Randomized Multicenter Trial of the Effects of Melanoma-Associated Helper Peptides and Cyclophosphamide on the Immunogenicity of a Multipeptide Melanoma Vaccine. J. Clin. Oncol. 2011, 29, 2924–2932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teixeira, L.; Medioni, J.; Garibal, J.; Adotevi, O.; Doucet, L.; Durey, M.-A.D.; Ghrieb, Z.; Kiladjian, J.-J.; Brizard, M.; Laheurte, C.; et al. A First-in-Human Phase I Study of INVAC-1, an Optimized Human Telomerase DNA Vaccine in Patients with Advanced Solid Tumors. Clin. Cancer Res. 2020, 26, 588–597. [Google Scholar] [CrossRef] [Green Version]
- Aamdal, E.; Inderberg, E.M.; Ellingsen, E.B.; Rasch, W.; Brunsvig, P.F.; Aamdal, S.; Heintz, K.-M.; Vodák, D.; Nakken, S.; Hovig, E.; et al. Combining a Universal Telomerase Based Cancer Vaccine with Ipilimumab in Patients With Metastatic Melanoma—Five-Year Follow Up of a Phase I/IIa Trial. Front. Immunol. 2021, 12, 663865. [Google Scholar] [CrossRef]
- Zakharia, Y.; O’Day, S.; Rasch, W.; Milhem, M.M. A Phase I Clinical Trial Investigating the Telomerase Vaccine UV1 in Combination with Pembrolizumab in Patients with Advanced Melanoma. J. Clin. Oncol. 2021, 39, 2620. [Google Scholar] [CrossRef]
- Svane, I.-M.; Kjeldsen, J.W.; Lorentzen, C.L.; Martinenaite, E.; Andersen, M.H. LBA48 Clinical Efficacy and Immunity of Combination Therapy with Nivolumab and IDO/PD-L1 Peptide Vaccine in Patients with Metastatic Melanoma: A Phase I/II Trial. Ann. Oncol. 2020, 31, S1176. [Google Scholar] [CrossRef]
- Ambrosi, L.; Khan, S.; Carvajal, R.D.; Yang, J. Novel Targets for the Treatment of Melanoma. Curr. Oncol. Rep. 2019, 21, 97. [Google Scholar] [CrossRef]
- Schreibelt, G.; Bol, K.F.; Westdorp, H.; Wimmers, F.; Aarntzen, E.H.J.G.; Duiveman-de Boer, T.; van de Rakt, M.W.M.M.; Scharenborg, N.M.; de Boer, A.J.; Pots, J.M.; et al. Effective Clinical Responses in Metastatic Melanoma Patients after Vaccination with Primary Myeloid Dendritic Cells. Clin. Cancer Res. 2016, 22, 2155–2166. [Google Scholar] [CrossRef] [Green Version]
- Hickerson, A.; Clifton, G.T.; Brown, T.A.; Campf, J.; Myers, J.W.; Vreeland, T.J.; Hale, D.F.; Peace, K.M.; Jackson, D.O.; Yu, X.; et al. Clinical Efficacy of Vaccination with the Autologous Tumor Lysate Particle Loaded Dendritic Cell (TLPLDC) Vaccine in Metastatic Melanoma. J. Clin. Oncol. 2019, 37, e21025. [Google Scholar] [CrossRef]
- Zinkernagel, R.M.; Doherty, P.C. The Discovery of MHC Restriction. Immunol. Today 1997, 18, 14–17. [Google Scholar] [CrossRef]
- Sahin, U.; Oehm, P.; Derhovanessian, E.; Jabulowsky, R.A.; Vormehr, M.; Gold, M.; Maurus, D.; Schwarck-Kokarakis, D.; Kuhn, A.N.; Omokoko, T.; et al. An RNA Vaccine Drives Immunity in Checkpoint-Inhibitor-Treated Melanoma. Nature 2020, 585, 107–112. [Google Scholar] [CrossRef]
- Simon, B.; Uslu, U. CAR-T Cell Therapy in Melanoma: A Future Success Story? Exp. Dermatol. 2018, 27, 1315–1321. [Google Scholar] [CrossRef] [Green Version]
- Waldman, A.D.; Fritz, J.M.; Lenardo, M.J. A Guide to Cancer Immunotherapy: From T Cell Basic Science to Clinical Practice. Nat. Rev. Immunol. 2020, 20, 651–668. [Google Scholar] [CrossRef]
- Eddy, K.; Chen, S. Overcoming Immune Evasion in Melanoma. Int. J. Mol. Sci. 2020, 21, 8984. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.A.; Morgan, R.A.; Dudley, M.E.; Cassard, L.; Yang, J.C.; Hughes, M.S.; Kammula, U.S.; Royal, R.E.; Sherry, R.M.; Wunderlich, J.R.; et al. Gene Therapy with Human and Mouse T-Cell Receptors Mediates Cancer Regression and Targets Normal Tissues Expressing Cognate Antigen. Blood 2009, 114, 535–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charych, D.; Khalili, S.; Dixit, V.; Kirk, P.; Chang, T.; Langowski, J.; Rubas, W.; Doberstein, S.K.; Eldon, M.; Hoch, U.; et al. Modeling the Receptor Pharmacology, Pharmacokinetics, and Pharmacodynamics of NKTR-214, a Kinetically-Controlled Interleukin-2 (IL2) Receptor Agonist for Cancer Immunotherapy. PLoS ONE 2017, 12, e0179431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khushalani, N.I.; Diab, A.; Ascierto, P.A.; Larkin, J.; Sandhu, S.; Sznol, M.; Koon, H.B.; Jarkowski, A.; Zhou, M.; Statkevich, P.; et al. Bempegaldesleukin plus Nivolumab in Untreated, Unresectable or Metastatic Melanoma: Phase III PIVOT IO 001 Study Design. Future Oncol. 2020, 16, 2165–2175. [Google Scholar] [CrossRef]
- Alva, A.; Daniels, G.A.; Wong, M.K.K.; Kaufman, H.L.; Morse, M.A.; McDermott, D.F.; Clark, J.I.; Agarwala, S.S.; Miletello, G.; Logan, T.F.; et al. Contemporary Experience with High-Dose Interleukin-2 Therapy and Impact on Survival in Patients with Metastatic Melanoma and Metastatic Renal Cell Carcinoma. Cancer Immunol. Immunother. 2016, 65, 1533–1544. [Google Scholar] [CrossRef] [Green Version]
- Diab, A.; Tykodi, S.S.; Daniels, G.A.; Maio, M.; Curti, B.D.; Lewis, K.D.; Jang, S.; Kalinka, E.; Puzanov, I.; Spira, A.I.; et al. Bempegaldesleukin Plus Nivolumab in First-Line Metastatic Melanoma. J. Clin. Oncol. 2021, 39, 2914–2925. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Cappuzzo, F.; Rodriguez-Abreu, D.; Cho, D.C.; Schwarz, J.K.; Riese, M.J.; Gupta, A.; Chan, T.; Saab, R.; Singel, S.; et al. 127TiP PROPEL: A Phase I/II Trial of Bempegaldesleukin (NKTR-214) in Combination with Pembrolizumab (Pembro) in Patients (Pts) with Advanced Solid Tumours. Ann. Oncol. 2019, 30, xi46–xi47. [Google Scholar] [CrossRef]
- Diab, A.; Marcondes, M.; Kotzin, B.; Tagliaferri, M.A.; Hoch, U.; Li, Y.; Cattaruzza, F.; Zalevsky, J.; Brohl, A.S.; Brugarolas, J.; et al. Phase Ib: Preliminary Clinical Activity and Immune Activation for NKTR-262 [TLR 7/8 Agonist] plus NKTR-214 [CD122-Biased Agonist] in Patients (Pts) with Locally Advanced or Metastatic Solid Tumors (REVEAL Phase Ib/II Trial). J. Clin. Oncol. 2019, 37, 26. [Google Scholar] [CrossRef]
- Lopes, J.E.; Fisher, J.L.; Flick, H.L.; Wang, C.; Sun, L.; Ernstoff, M.S.; Alvarez, J.C.; Losey, H.C. ALKS 4230: A Novel Engineered IL-2 Fusion Protein with an Improved Cellular Selectivity Profile for Cancer Immunotherapy. J. Immunother. Cancer 2020, 8, e000673. [Google Scholar] [CrossRef]
- Kim, K.; Leong, S.P.L.; Singer, M.I.; Parrett, B.M.; Moretto, J.; Minor, D.R.; Vosoughi, E.; Millis, S.Z.; Ross, J.S.; Kashani-Sabet, M. Frequency of Genetic Homologous Recombination (HR) Alterations in Metastatic Cutaneous Melanoma. J. Clin. Oncol. 2017, 35, e21033. [Google Scholar] [CrossRef]
- Dummer, R.; Schadendorf, D.; Ascierto, P.A.; Arance, A.; Dutriaux, C.; Di Giacomo, A.M.; Rutkowski, P.; Del Vecchio, M.; Gutzmer, R.; Mandala, M.; et al. Binimetinib versus Dacarbazine in Patients with Advanced NRAS-Mutant Melanoma (NEMO): A Multicentre, Open-Label, Randomised, Phase 3 Trial. Lancet Oncol. 2017, 18, 435–445. [Google Scholar] [CrossRef]
- Lebbé, C.; Dutriaux, C.; Lesimple, T.; Kruit, W.; Kerger, J.; Thomas, L.; Guillot, B.; de Braud, F.; Garbe, C.; Grob, J.-J.; et al. Pimasertib Versus Dacarbazine in Patients with Unresectable NRAS-Mutated Cutaneous Melanoma: Phase II, Randomized, Controlled Trial with Crossover. Cancers 2020, 12, 1727. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.J.; Lee, J.; Kim, T.M.; Kim, J.-S.; Kim, Y.J.; Hong, Y.S.; Kim, S.Y.; Kim, J.E.; Lee, D.H.; Hong, Y.; et al. A Phase Ib Trial of Belvarafenib in Combination with Cobimetinib in Patients with Advanced Solid Tumors: Interim Results of Dose-Escalation and Patients with NRAS-Mutant Melanoma of Dose-Expansion. J. Clin. Oncol. 2021, 39, 3007. [Google Scholar] [CrossRef]
- Monaco, K.-A.; Delach, S.; Yuan, J.; Mishina, Y.; Fordjour, P.; Labrot, E.; McKay, D.; Guo, R.; Higgins, S.; Wang, H.Q.; et al. LXH254, a Potent and Selective ARAF-Sparing Inhibitor of BRAF and CRAF for the Treatment of MAPK-Driven Tumors. Clin. Cancer Res. 2021, 27, 2061–2073. [Google Scholar] [CrossRef]
- Julve, M.; Clark, J.J.; Lythgoe, M.P. Advances in Cyclin-Dependent Kinase Inhibitors for the Treatment of Melanoma. Expert Opin. Pharmacother. 2021, 22, 351–361. [Google Scholar] [CrossRef]
- Taylor, M.; Sosman, J.; Gonzalez, R.; Carlino, M.S.; Kittaneh, M.; Lolkema, M.P.; Miller, W.; Marino, A.; Zhang, V.; Bhansali, S.G.; et al. 1086O—Phase Ib/Ii Study of Lee011 (Cdk4/6 Inhibitor) and Lgx818 (Braf Inhibitor) in Braf-Mutant Melanoma. Ann. Oncol. 2014, 25, iv374. [Google Scholar] [CrossRef]
- Ascierto, P.A.; Flaherty, K.; Goff, S. Emerging Strategies in Systemic Therapy for the Treatment of Melanoma. Am. Soc. Clin. Oncol. Educ. B. 2018, 751–758. [Google Scholar] [CrossRef]
- Schuler, M.H.; Ascierto, P.A.; De Vos, F.Y.F.L.; Postow, M.A.; Van Herpen, C.M.L.; Carlino, M.S.; Sosman, J.A.; Berking, C.; Long, G.V.; Weise, A.; et al. Phase 1b/2 Trial of Ribociclib+binimetinib in Metastatic NRAS-Mutant Melanoma: Safety, Efficacy, and Recommended Phase 2 Dose (RP2D). J. Clin. Oncol. 2017, 35, 9519. [Google Scholar] [CrossRef]
- Ascierto, P.A.; Bechter, O.; Wolter, P.; Lebbe, C.; Elez, E.; Miller, W.H.; Long, G.V.; Omlin, A.G.; Siena, S.; Calvo, E.; et al. A Phase Ib/II Dose-Escalation Study Evaluating Triple Combination Therapy with a BRAF (Encorafenib), MEK (Binimetinib), and CDK 4/6 (Ribociclib) Inhibitor in Patients (Pts) with BRAF V600-Mutant Solid Tumors and Melanoma. J. Clin. Oncol. 2017, 35, 9518. [Google Scholar] [CrossRef]
- Mao, L.; Cao, Y.; Sheng, X.; Bai, X.; Chi, Z.; Cui, C.; Wang, X.; Tang, B.; Lian, B.; Yan, X.; et al. Palbociclib (P) in Advanced Acral Lentiginous Melanoma (ALM) with CDK4 Pathway Gene Aberrations. J. Clin. Oncol. 2019, 37, 9528. [Google Scholar] [CrossRef]
- Sullivan, R.J.; Infante, J.R.; Janku, F.; Wong, D.J.L.; Sosman, J.A.; Keedy, V.; Patel, M.R.; Shapiro, G.I.; Mier, J.W.; Tolcher, A.W.; et al. First-in-Class ERK1/2 Inhibitor Ulixertinib (BVD-523) in Patients with MAPK Mutant Advanced Solid Tumors: Results of a Phase I Dose-Escalation and Expansion Study. Cancer Discov. 2018, 8, 184–195. [Google Scholar] [CrossRef] [Green Version]
- Tolcher, A.W.; Sullivan, R.J.; Rasco, D.W.; Eroglu, Z.; Lakhani, N.; Kessler, D.; Usansky, H.; Reddy, S.; Denis, L.J.; Janku, F. Abstract PR09: Phase 1 Clinical Safety and Efficacy of ASN007, a Novel Oral ERK1/2 Inhibitor, in Patients with RAS, RAF or MEK Mutant Advanced Solid Tumors. Mol. Cancer Ther. 2019, 18, PR09 LP-PR09. [Google Scholar] [CrossRef]
- Huijberts, S.; Wang, L.; de Oliveira, R.L.; Rosing, H.; Nuijen, B.; Beijnen, J.; Bernards, R.; Schellens, J.; Wilgenhof, S. Vorinostat in Patients with Resistant BRAFV600E Mutated Advanced Melanoma: A Proof of Concept Study. Future Oncol. 2020, 16, 619–629. [Google Scholar] [CrossRef]
- Murciano-Goroff, Y.R.; Warner, A.B.; Wolchok, J.D. The Future of Cancer Immunotherapy: Microenvironment-Targeting Combinations. Cell Res. 2020, 30, 507–519. [Google Scholar] [CrossRef] [PubMed]
- Bretz, A.C.; Parnitzke, U.; Kronthaler, K.; Dreker, T.; Bartz, R.; Hermann, F.; Ammendola, A.; Wulff, T.; Hamm, S. Domatinostat Favors the Immunotherapy Response by Modulating the Tumor Immune Microenvironment (TIME). J. Immunother. Cancer 2019, 7, 294. [Google Scholar] [CrossRef] [Green Version]
- Hassel, J.C.; Berking, C.; Schlaak, M.; Eigentler, T.; Gutzmer, R.; Ascierto, P.A.; Schilling, B.; Hamm, S.; Hermann, F.; Reimann, P.G.; et al. Results from the Phase Ib of the SENSITIZE Trial Combining Domatinostat with Pembrolizumab in Advanced Melanoma Patients Refractory to Prior Checkpoint Inhibitor Therapy. J. Clin. Oncol. 2021, 39, 9545. [Google Scholar] [CrossRef]
- Agarwala, S.S.; Moschos, S.J.; Johnson, M.L.; Opyrchal, M.; Gabrilovich, D.; Danaher, P.; Wang, F.; Brouwer, S.; Ordentlich, P.; Sankoh, S.; et al. Efficacy and Safety of Entinostat (ENT) and Pembrolizumab (PEMBRO) in Patients with Melanoma Progressing on or after a PD-1/L1 Blocking Antibody. J. Clin. Oncol. 2018, 36, 9530. [Google Scholar] [CrossRef]
- Khushalani, N.I.; Markowitz, J.; Eroglu, Z.; Giuroiu, I.; Ladanova, V.; Reiersen, P.; Rich, J.; Thapa, R.; Schell, M.J.; Sotomayor, E.M.; et al. A Phase I Trial of Panobinostat with Ipilimumab in Advanced Melanoma. J. Clin. Oncol. 2017, 35, 9547. [Google Scholar] [CrossRef]
- Khushalani, N.; Brohl, A.; Markowitz, J.; Bazhenova, L.; Daniels, G.; Yeckes-Rodin, H.; Fu, S.; McCormick, L.; Kurman, M.; Gillings, M.; et al. 797 Significant Anti-Tumor Activity of HBI-8000, a Class I Histone Deacetylase Inhibitor (HDACi) in Combination with Nivolumab (NIVO) in Anti-PD1 Therapy-Naïve Advanced Melanoma (TN-Mel). J. Immunother. Cancer 2020, 8, A476–A477. [Google Scholar] [CrossRef]
- Moon, Y.W.; Hajjar, J.; Hwu, P.; Naing, A. Targeting the Indoleamine 2,3-Dioxygenase Pathway in Cancer. J. Immunother. Cancer 2015, 3, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beatty, G.L.; O’Dwyer, P.J.; Clark, J.; Shi, J.G.; Bowman, K.J.; Scherle, P.A.; Newton, R.C.; Schaub, R.; Maleski, J.; Leopold, L.; et al. First-in-Human Phase I Study of the Oral Inhibitor of Indoleamine 2,3-Dioxygenase-1 Epacadostat (INCB024360) in Patients with Advanced Solid Malignancies. Clin. Cancer Res. 2017, 23, 3269–3276. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, T.C.; Hamid, O.; Smith, D.C.; Bauer, T.M.; Wasser, J.S.; Olszanski, A.J.; Luke, J.J.; Balmanoukian, A.S.; Schmidt, E.V.; Zhao, Y.; et al. Epacadostat Plus Pembrolizumab in Patients with Advanced Solid Tumors: Phase I Results from a Multicenter, Open-Label Phase I/II Trial (ECHO-202/KEYNOTE-037). J. Clin. Oncol. 2018, 36, 3223–3230. [Google Scholar] [CrossRef]
- Long, G.V.; Dummer, R.; Hamid, O.; Gajewski, T.F.; Caglevic, C.; Dalle, S.; Arance, A.; Carlino, M.S.; Grob, J.-J.; Kim, T.M.; et al. Epacadostat plus Pembrolizumab versus Placebo plus Pembrolizumab in Patients with Unresectable or Metastatic Melanoma (ECHO-301/KEYNOTE-252): A Phase 3, Randomised, Double-Blind Study. Lancet Oncol. 2019, 20, 1083–1097. [Google Scholar] [CrossRef]
- Daud, A.; Saleh, M.N.; Hu, J.; Bleeker, J.S.; Riese, M.J.; Meier, R.; Zhou, L.; Serbest, G.; Lewis, K.D. Epacadostat plus Nivolumab for Advanced Melanoma: Updated Phase 2 Results of the ECHO-204 Study. J. Clin. Oncol. 2018, 36, 9511. [Google Scholar] [CrossRef]
- Siu, L.; Gelmon, K.; Chu, Q.; Pachynski, R.; Alese, O.; Basciano, P.; Walker, J.; Mitra, P.; Zhu, L.; Phillips, P.; et al. Abstract CT116: BMS-986205, an Optimized Indoleamine 2,3-Dioxygenase 1 (IDO1) Inhibitor, Is Well Tolerated with Potent Pharmacodynamic (PD) Activity, Alone and in Combination with Nivolumab (Nivo) in Advanced Cancers in a Phase 1/2a Trial. Cancer Res. 2017, 77, CT116. [Google Scholar] [CrossRef]
- Zakharia, Y.; McWilliams, R.R.; Rixe, O.; Drabick, J.; Shaheen, M.F.; Grossmann, K.F.; Kolhe, R.; Pacholczyk, R.; Sadek, R.; Tennant, L.L.; et al. Phase II Trial of the IDO Pathway Inhibitor Indoximod plus Pembrolizumab for the Treatment of Patients with Advanced Melanoma. J. Immunother. Cancer 2021, 9, e002057. [Google Scholar] [CrossRef]
- Sheng, X.; Yan, X.; Chi, Z.; Si, L.; Cui, C.; Tang, B.; Li, S.; Mao, L.; Lian, B.; Wang, X.; et al. Axitinib in Combination with Toripalimab, a Humanized Immunoglobulin G4 Monoclonal Antibody Against Programmed Cell Death-1, in Patients with Metastatic Mucosal Melanoma: An Open-Label Phase IB Trial. J. Clin. Oncol. 2019, 37, 2987–2999. [Google Scholar] [CrossRef] [PubMed]
- Taylor, M.H.; Lee, C.-H.; Makker, V.; Rasco, D.; Dutcus, C.E.; Wu, J.; Stepan, D.E.; Shumaker, R.C.; Motzer, R.J. Phase IB/II Trial of Lenvatinib Plus Pembrolizumab in Patients with Advanced Renal Cell Carcinoma, Endometrial Cancer, and Other Selected Advanced Solid Tumors. J. Clin. Oncol. 2020, 38, 1154–1163. [Google Scholar] [CrossRef] [PubMed]
- Arance, A.M.; de la Cruz-Merino, L.; Petrella, T.M.; Jamal, R.; Ny, L.; Carneiro, A.; Berrocal, A.; Marquez-Rodas, I.; Spreafico, A.; Atkinson, V.; et al. Lenvatinib (Len) plus Pembrolizumab (Pembro) for Patients (Pts) with Advanced Melanoma and Confirmed Progression on a PD-1 or PD-L1 Inhibitor: Updated Findings of LEAP-004. J. Clin. Oncol. 2021, 39, 9504. [Google Scholar] [CrossRef]
- Fernandez, A.M.A.; O’Day, S.J.; de la Merino, L.C.; Petrella, T.; Jamal, R.; Ny, L.; Carneiro, A.; Berrocal, A.; Márquez-Rodas, I.; Spreafico, A.; et al. LBA44 Lenvatinib (Len) plus Pembrolizumab (Pembro) for Advanced Melanoma (MEL) That Progressed on a PD-1 or PD-L1 Inhibitor: Initial Results of LEAP-004. Ann. Oncol. 2020, 31, S1173. [Google Scholar] [CrossRef]
- Mahalingam, D.; Malik, L.; Beeram, M.; Rodon, J.; Sankhala, K.; Mita, A.; Benjamin, D.; Ketchum, N.; Michalek, J.; Tolcher, A.; et al. Phase II Study Evaluating the Efficacy, Safety, and Pharmacodynamic Correlative Study of Dual Antiangiogenic Inhibition Using Bevacizumab in Combination with Sorafenib in Patients with Advanced Malignant Melanoma. Cancer Chemother. Pharmacol. 2014, 74, 77–84. [Google Scholar] [CrossRef]
- Ferrucci, P.F.; Minchella, I.; Mosconi, M.; Gandini, S.; Verrecchia, F.; Cocorocchio, E.; Passoni, C.; Pari, C.; Testori, A.; Coco, P.; et al. Dacarbazine in Combination with Bevacizumab for the Treatment of Unresectable/Metastatic Melanoma: A Phase II Study. Melanoma Res. 2015, 25, 239–245. [Google Scholar] [CrossRef]
- Hodi, F.S.; Lawrence, D.; Lezcano, C.; Wu, X.; Zhou, J.; Sasada, T.; Zeng, W.; Giobbie-Hurder, A.; Atkins, M.B.; Ibrahim, N.; et al. Bevacizumab plus Ipilimumab in Patients with Metastatic Melanoma. Cancer Immunol. Res. 2014, 2, 632–642. [Google Scholar] [CrossRef] [Green Version]
- Straume, O.; Lorens, J.B.; Gausdal, G.; Gjertsen, B.T.; Schuster, C. A Randomized Phase Ib/II Study of the Selective Small Molecule Axl Inhibitor Bemcentinib (BGB324) in Combination with Either Dabrafenib/Trametinib (D/T) or Pembrolizumab in Patients with Metastatic Melanoma. Ann. Oncol. 2019, 30, v563. [Google Scholar] [CrossRef]
- Sussman, T.A.; Wei, W.; Hobbs, B.; Diaz-Montero, C.M.; Ni, Y.; Arbesman, J.; Ko, J.S.; Gastman, B.; Funchain, P. A Phase II Trial of Nivolumab in Combination with Talazoparib in Unresectable or Metastatic Melanoma Patients with Mutations in BRCA or BRCAness. J. Clin. Oncol. 2020, 38, TPS10082. [Google Scholar] [CrossRef]
- Marechal, A.; Zou, L. DNA Damage Sensing by the ATM and ATR Kinases. Cold Spring Harb. Perspect. Biol. 2013, 5, a012716. [Google Scholar] [CrossRef]
- Schoppy, D.W.; Ragland, R.L.; Gilad, O.; Shastri, N.; Peters, A.A.; Murga, M.; Fernandez-Capetillo, O.; Diehl, J.A.; Brown, E.J. Oncogenic Stress Sensitizes Murine Cancers to Hypomorphic Suppression of ATR. J. Clin. Investig. 2012, 122, 241–252. [Google Scholar] [CrossRef] [Green Version]
- Höglund, A.; Nilsson, L.M.; Muralidharan, S.V.; Hasvold, L.A.; Merta, P.; Rudelius, M.; Nikolova, V.; Keller, U.; Nilsson, J.A. Therapeutic Implications for the Induced Levels of Chk1 in Myc-Expressing Cancer Cells. Clin. Cancer Res. 2011, 17, 7067–7079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murga, M.; Campaner, S.; Lopez-Contreras, A.J.; Toledo, L.I.; Soria, R.; Montaña, M.F.; D’Artista, L.; Schleker, T.; Guerra, C.; Garcia, E.; et al. Exploiting Oncogene-Induced Replicative Stress for the Selective Killing of Myc-Driven Tumors. Nat. Struct. Mol. Biol. 2011, 18, 1331–1335. [Google Scholar] [CrossRef] [PubMed]
- Gilad, O.; Nabet, B.Y.; Ragland, R.L.; Schoppy, D.W.; Smith, K.D.; Durham, A.C.; Brown, E.J. Combining ATR Suppression with Oncogenic Ras Synergistically Increases Genomic Instability, Causing Synthetic Lethality or Tumorigenesis in a Dosage-Dependent Manner. Cancer Res. 2010, 70, 9693–9702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foote, K.M.; Lau, A.; M Nissink, J.W. Drugging ATR: Progress in the Development of Specific Inhibitors for the Treatment of Cancer. Future Med. Chem. 2015, 7, 873–891. [Google Scholar] [CrossRef]
- Foote, K.M.; Nissink, J.W.M.; McGuire, T.; Turner, P.; Guichard, S.; Yates, J.W.T.; Lau, A.; Blades, K.; Heathcote, D.; Odedra, R.; et al. Discovery and Characterization of AZD6738, a Potent Inhibitor of Ataxia Telangiectasia Mutated and Rad3 Related (ATR) Kinase with Application as an Anticancer Agent. J. Med. Chem. 2018, 61, 9889–9907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.T.; Smith, S.A.; Mortimer, P.; Loembé, A.-B.; Cho, H.; Kim, K.-M.; Smith, C.; Willis, S.; Irurzun-Arana, I.; Berges, A.; et al. Phase I Study of Ceralasertib (AZD6738), a Novel DNA Damage Repair Agent, in Combination with Weekly Paclitaxel in Refractory Cancer. In Clinical Cancer Research; American Association for Cancer Research: Philadelphia, PA, USA, 2021; Volume 27. [Google Scholar] [CrossRef]
- Kwon, M.; Kim, S.T.; Smith, S.; Smith, C.; Mortimer, P.G.; LoembE, B.; Kozarewa, I.; Dean, E.; Lee, J. Phase II Study of Ceralasertib (AZD6738), in Combination with Durvalumab in Patients with Metastatic Melanoma Who Have Failed Prior Anti-PD-1 Therapy. J. Clin. Oncol. 2021, 39, 9514. [Google Scholar] [CrossRef]
- Andtbacka, R.H.I.; Kaufman, H.L.; Collichio, F.; Amatruda, T.; Senzer, N.; Chesney, J.; Delman, K.A.; Spitler, L.E.; Puzanov, I.; Agarwala, S.S.; et al. Talimogene Laherparepvec Improves Durable Response Rate in Patients with Advanced Melanoma. J. Clin. Oncol. 2015, 33, 2780–2788. [Google Scholar] [CrossRef]
- Andtbacka, R.H.I.; Collichio, F.; Harrington, K.J.; Middleton, M.R.; Downey, G.; Öhrling, K.; Kaufman, H.L. Final Analyses of OPTiM: A Randomized Phase III Trial of Talimogene Laherparepvec versus Granulocyte-Macrophage Colony-Stimulating Factor in Unresectable Stage III–IV Melanoma. J. Immunother. Cancer 2019, 7, 145. [Google Scholar] [CrossRef] [Green Version]
- Kohlhapp, F.J.; Kaufman, H.L. Molecular Pathways: Mechanism of Action for Talimogene Laherparepvec, a New Oncolytic Virus Immunotherapy. Clin. Cancer Res. 2016, 22, 1048–1054. [Google Scholar] [CrossRef] [Green Version]
- Chesney, J.; Puzanov, I.; Collichio, F.; Singh, P.; Milhem, M.M.; Glaspy, J.; Hamid, O.; Ross, M.; Friedlander, P.; Garbe, C.; et al. Randomized, Open-Label Phase II Study Evaluating the Efficacy and Safety of Talimogene Laherparepvec in Combination with Ipilimumab versus Ipilimumab Alone in Patients with Advanced, Unresectable Melanoma. J. Clin. Oncol. 2018, 36, 1658–1667. [Google Scholar] [CrossRef] [PubMed]
- Long, G.; Dummer, R.; Johnson, D.; Michielin, O.; Martin-Algarra, S.; Treichel, S.; Chan, E.; Diede, S.; Ribas, A. 429 Long-Term Analysis of MASTERKEY-265 Phase 1b Trial of Talimogene Laherparepvec (T-VEC) plus Pembrolizumab in Patients with Unresectable Stage IIIB-IVM1c Melanoma. J. Immunother. Cancer 2020, 8, A261. [Google Scholar] [CrossRef]
- Ribas, A.; Chesney, J.; Long, G.V.; Kirkwood, J.M.; Dummer, R.; Puzanov, I.; Hoeller, C.; Gajewski, T.F.; Gutzmer, R.; Rutkowski, P.; et al. 1037O MASTERKEY-265: A Phase III, Randomized, Placebo (Pbo)-Controlled Study of Talimogene Laherparepvec (T) plus Pembrolizumab (P) for Unresectable Stage IIIB–IVM1c Melanoma (MEL). Ann. Oncol. 2021, 32, S868–S869. [Google Scholar] [CrossRef]
- Yokota, K.; Isei, T.; Uhara, H.; Fujisawa, Y.; Takenouchi, T.; Kiyohara, Y.; Uchi, H.; Saruta, H.; Ihn, H.; Inozume, T.; et al. Final Results from Phase II of Combination with Canerpaturev (Formerly HF10), an Oncolytic Viral Immunotherapy, and Ipilimumab in Unresectable or Metastatic Melanoma in Second-or Later Line Treatment. Ann. Oncol. 2019, 30, v557. [Google Scholar] [CrossRef]
- Diab, A.; Rahimian, S.; Haymaker, C.L.; Bernatchez, C.; Andtbacka, R.H.I.; James, M.; Johnson, D.B.; Markowitz, J.; Murthy, R.; Puzanov, I.; et al. A Phase 2 Study to Evaluate the Safety and Efficacy of Intratumoral (IT) Injection of the TLR9 Agonist IMO-2125 (IMO) in Combination with Ipilimumab (Ipi) in PD-1 Inhibitor Refractory Melanoma. J. Clin. Oncol. 2018, 36, 9515. [Google Scholar] [CrossRef]
- Haymaker, C.; Johnson, D.H.; Murthy, R.; Bentebibel, S.-E.; Uemura, M.I.; Hudgens, C.W.; Safa, H.; James, M.; Andtbacka, R.H.I.; Johnson, D.B.; et al. Tilsotolimod with Ipilimumab Drives Tumor Responses in Anti-PD-1 Refractory Melanoma. Cancer Discov. 2021, 11, 1996–2013. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Lemke-Miltner, C.D.; Wongpattaraworakul, W.; Wang, Z.; Chan, C.H.F.; Salem, A.K.; Weiner, G.J.; Simons, A.L. In Situ Immunization of a TLR9 Agonist Virus-like Particle Enhances Anti-PD1 Therapy. J. Immunother. Cancer 2020, 8, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Milhem, M.M.; Long, G.V.; Hoimes, C.J.; Amin, A.; Lao, C.D.; Conry, R.M.; Hunt, J.; Daniels, G.A.; Almubarak, M.; Shaheen, M.F.; et al. Phase 1b/2, Open Label, Multicenter, Study of the Combination of SD-101 and Pembrolizumab in Patients with Advanced Melanoma Who Are Naïve to Anti-PD-1 Therapy. J. Clin. Oncol. 2019, 37, 9534. [Google Scholar] [CrossRef]
- Zager, J.S.; Sarnaik, A.S.; Pilon-Thomas, S.; Beatty, M.; Han, D.; Lu, G.; Agarwala, S.S.; Ross, M.; Shirai, K.; Essner, R.; et al. 1123P A Phase Ib Study of Rose Bengal Disodium and Anti-PD-1 in Metastatic Cutaneous Melanoma: Initial Results in Patients Refractory to Checkpoint Blockade. Ann. Oncol. 2020, 31, S755–S756. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Agent | Class | Phase | Trial ID | Status on ClinicalTrials.gov (Accessed on 10 October 2021) |
|---|---|---|---|---|
| relatlimab + nivolumab (RELATIVITY-047) | anti-LAG3 + anti-PD-1 | II/III | NCT03470922 | active, not recruiting |
| relatlimab + nivolumab | anti-LAG3 + anti-PD-1 | II | NCT03743766 | recruiting |
| vibostolimab + pembrolizumab | anti-TIGIT + anti-PD-1 | I/II | NCT04305054 | recruiting |
| vibostolimab + pembrolizumab + quavonlimab | anti-TIGIT + anti-PD-1 + anti-CTLA-4 | I/II | NCT04305041 | recruiting |
| Agent | Class | Phase | Trial ID | Status on ClinicalTrials.gov (Accessed on 10 October 2021) |
|---|---|---|---|---|
| Lifileucel | TILs | II | NCT02360579 | active, not recruiting |
| TILs | TILs | III | NCT02278887 | recruiting |
| ITIL-168 | TILs | II | NCT05050006 | recruiting |
| TILs + nivolumab | TILs + anti-PD-1 | I | NCT04165967 | recruiting |
| TILs + nivolumab | TILs + anti-PD-1 | I | NCT03475134 | recruiting |
| TILs + nivolumab | TILs + anti-PD-1 | I/II | NCT03374839 | recruiting |
| TILs + nivolumab | TILs + anti-PD-1 | I/II | NCT03638375 | recruiting |
| Agent | Class | Phase | Trial ID | Status on ClinicalTrials.gov (Accessed on 10 October 2021) |
|---|---|---|---|---|
| UV1 vaccine + ipilimumab | peptide vaccine + anti-CTLA-4 | I/II | NCT02275416 | active, not recruiting |
| UV1 vaccine + pembrolizumab | peptide vaccine + anti-PD1 | I | NCT03538314 | active, non recruiting |
| UV1 vaccine + nivolumab + ipilimumab | peptide vaccine + anti-PD1 + anti-CTLA-4 | II | NCT04382664 | recruiting |
| 6MHP + NeoAg-mBRAF | peptide vaccine + neoantigen vaccine | I/II | NCT04364230 | recruiting |
| neoantigen vaccine toripalimab + imiquimod 5% topical cream | neoantigen vaccine + anti-PD1 + topical cream | I | NCT04072900 | recruiting |
| NeoVax + montanide + ipilimumab + nivolumab | neoantigen vaccine + anti-PD1 + anti-CTLA-4 | I | NCT03929029 | recruiting |
| TLPLDC | dendritic cells vaccine | I/II | NCT02678741 | completed |
| mature dendritic cell vaccine + pembrolizumab | dendritic cells vaccine + anti-PD-1 | I | NCT03092453 | recruiting |
| BNT111 + cemiplimab | mRNA vaccine + anti-PD1 | II | NCT04526899 | recruiting |
| Agent | Class | Phase | Trial ID | Status on ClinicalTrials.gov (Accessed on 10 October 2021) |
|---|---|---|---|---|
| MB-CART20.1 | CAR-T cells | I (15 pts) | NCT03893019 | recruiting |
| IL13Ralpha2 CAR T cells | CAR-T cells | I (24 pts) | NCT04119024 | recruiting |
| GPA-TriMAR-T | CAR-T cells | I (6 pts) | NCT03649529 | recruiting |
| IMA202 product | TCR engineered T cells | I (15 pts) | NCT03441100 | recruiting |
| IMA203 product +/− atezolizumab | TCR engineered T cells +/− anti PD-1 | I (42 pts) | NCT03686124 | recruiting |
| Bempegaldesleukin + nivolumab | IL-2 + anti-PD-1 | III | NCT03635983 | recruiting |
| Nemvaleukin Alfa | IL-2 | II | NCT04830124 | recruiting |
| Hu14.18-IL2 + RT + nivolumab + ipilimumab | IL-2 + anti-PD-1 + anti-CTLA-4 | I/II | NCT03958383 | recruiting |
| IL2 + ipilimumab followed by nivolumab | IL-2 + anti-CTLA-4 + anti-PD-1 | II | NCT04562129 | recruiting |
| Agent | Class | Phase | Trial ID | Status on ClinicalTrials.gov (Accessed on 10 October 2021) |
|---|---|---|---|---|
| FCN-159 | MEK inhibitor | I | NCT03932253 | recruiting |
| HL-085 | MEK inhibitor | I/II | NCT03973151 | recruiting |
| belvarafenib + cobimetinib + atezolizumab | RAF inhibitor + MEKi + anti-PD-L1 | I | NCT0483805 | recruiting |
| LXH254 + LTT462 or trametinib or ribociclib | BRAF and CRAF inhibitor + ERK inhibitor or MEKi or CDK4/6 inhibitor | NCT0483805 | recruiting | |
| palbociclib + encorafenib + binimetinib | CDK4/6 inhibitor + BRAFi + MEKi | Ib/II | NCT04720768 | recruiting |
| ulixertinib | ERK inhibitor | expanded access | NCT04566393 | available |
| domatinostat + pembrolizumab | HDAC inhibitor + anti-PD-1 | Ib/II | NCT03278665 | recruiting |
| entinostat + pembrolizumab | HDAC inhibitor + anti-PD-1 | II | NCT03765229 | recruiting |
| HBI-8000 + nivolumab | HDAC inhibitor + anti-PD-1 | III | NCT04674683 | recruiting |
| lenvatinib + pembrolizumab | anti-VEGFR + anti-PD-1 | III | NCT03820986 | active, not recruiting |
| axitinib + nivolumab | anti-VEGFR + anti-PD-1 | II | NCT04493203 | recruiting |
| bevacizumab + ipilimumab | anti-VEGF + anti-CTLA-4 | II | NCT01950390 | active, non recruiting |
| bevacizumab + atezolizumab | anti-VEGF + anti-PD-L1 | II | NCT04356729 | recruiting |
| pembrolizumab or dabrafenib/trametinib + bemcentinib | anti-PD-1 or BRAFi/MEKi + Axl inhibitor | Ib/II | NCT02872259 | recruiting |
| niraparib | PARP inhibitor | II | NCT03925350 | recruiting |
| olaparib + pembrolizumab | PARP inhibitor + anti-PD-1 | II | NCT04633902 | recruiting |
| talazoparib + nivolumab | PARP inhibitor | II | NCT04187833 | recruiting |
| Agent | Class | Phase | Trial ID | Status on ClinicalTrials.gov (Accessed on 10 Ocober 2021) |
|---|---|---|---|---|
| Talimogene laherparepvec + pembrolizumab | modified oncolytic HSV 1 + anti-PD-1 | II | NCT02965716 | active, non recruiting |
| Talimogene laherparepvec + pembrolizumab | modified oncolytic HSV 1 + anti-PD-1 | II | NCT04068181 | active, non recruiting |
| CMP-001 + nivolumab | TLR9 agonist + anti-PD-1 | II | NCT04698187 | recruiting |
| CMP-001 + nivolumab | TLR9 agonist + anti-PD-1 | II/III | NCT04695977 | recruiting |
| PV-10 + pembrolizumab | small molecule autolytic immunotherapy + anti-PD-1 | I/II | NCT02557321 | recruiting |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Comito, F.; Pagani, R.; Grilli, G.; Sperandi, F.; Ardizzoni, A.; Melotti, B. Emerging Novel Therapeutic Approaches for Treatment of Advanced Cutaneous Melanoma. Cancers 2022, 14, 271. https://doi.org/10.3390/cancers14020271
Comito F, Pagani R, Grilli G, Sperandi F, Ardizzoni A, Melotti B. Emerging Novel Therapeutic Approaches for Treatment of Advanced Cutaneous Melanoma. Cancers. 2022; 14(2):271. https://doi.org/10.3390/cancers14020271
Chicago/Turabian StyleComito, Francesca, Rachele Pagani, Giada Grilli, Francesca Sperandi, Andrea Ardizzoni, and Barbara Melotti. 2022. "Emerging Novel Therapeutic Approaches for Treatment of Advanced Cutaneous Melanoma" Cancers 14, no. 2: 271. https://doi.org/10.3390/cancers14020271
APA StyleComito, F., Pagani, R., Grilli, G., Sperandi, F., Ardizzoni, A., & Melotti, B. (2022). Emerging Novel Therapeutic Approaches for Treatment of Advanced Cutaneous Melanoma. Cancers, 14(2), 271. https://doi.org/10.3390/cancers14020271