
Clinical and Sociodemographic Determinants of Adherence to World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) Recommendations in Breast Cancer Survivors—Health-EpiGEICAM Study
 , , , , , , ,
, , , , , , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Variables
2.3. WCRF/AICR Score Construction
2.4. Statistical Analyses
3. Results

{kind=link}
{kind=link}
| 2018 WCRF/AICR Recommendations | Operationalization | Adherence | |
|---|---|---|---|
| (N = 420) | |||
| Points | n (%) | ||
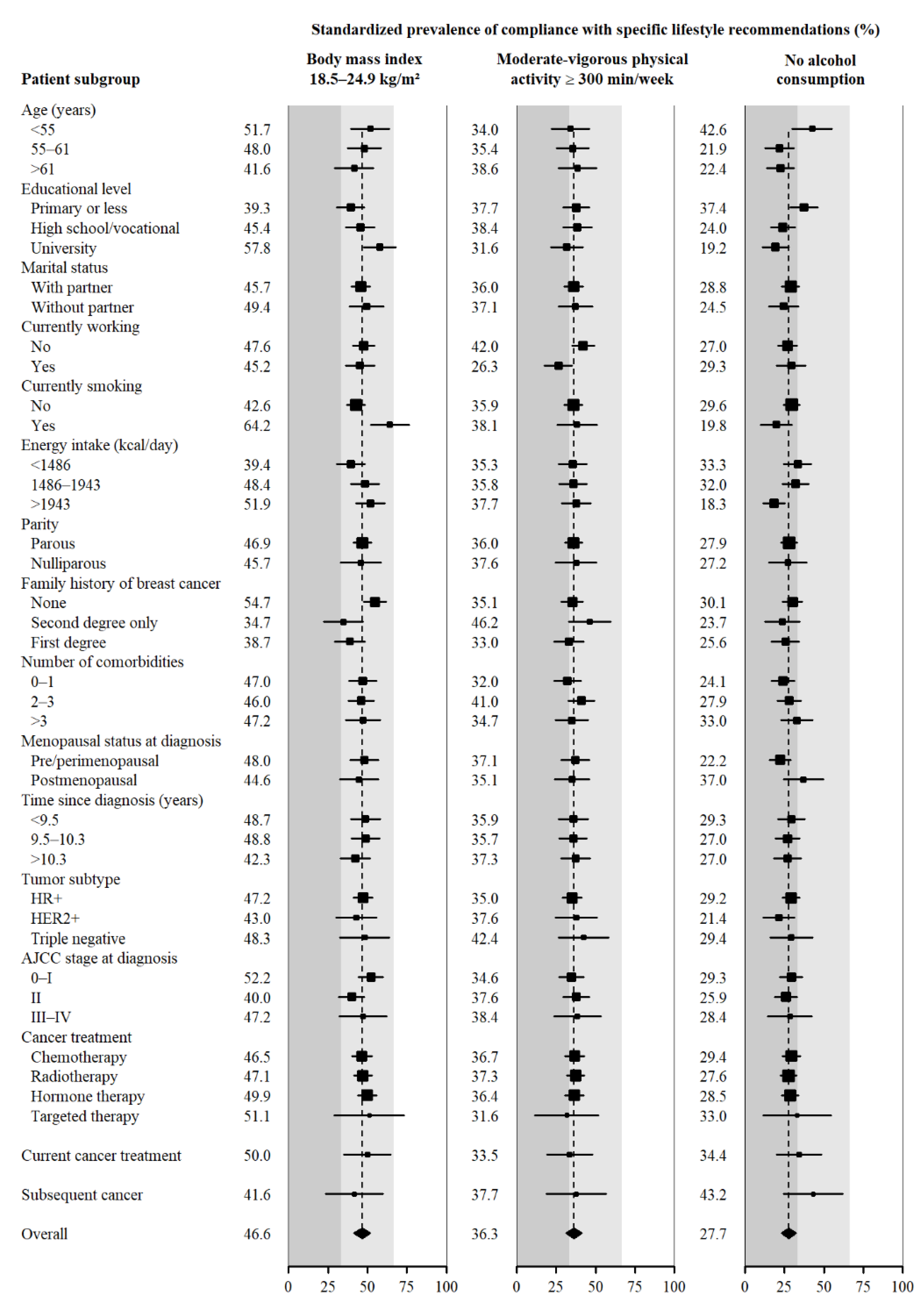
| 1. Be a healthy weight | BMI (kg/m2): | ||
| 18.5–24.9 | 1 | 192 (45.7) | |
| 25–29.9 | 0.5 | 155 (36.9) | |
| <18.5 or >30 | 0 | 73 (17.4) | |
| 2. Be physically active | Total moderate-vigorous physical activity (min/wk): | ||
| >300 | 1 | 145 (34.5) | |
| 150-<300 | 0.5 | 121 (28.8) | |
| <150 | 0 | 154 (36.7) | |
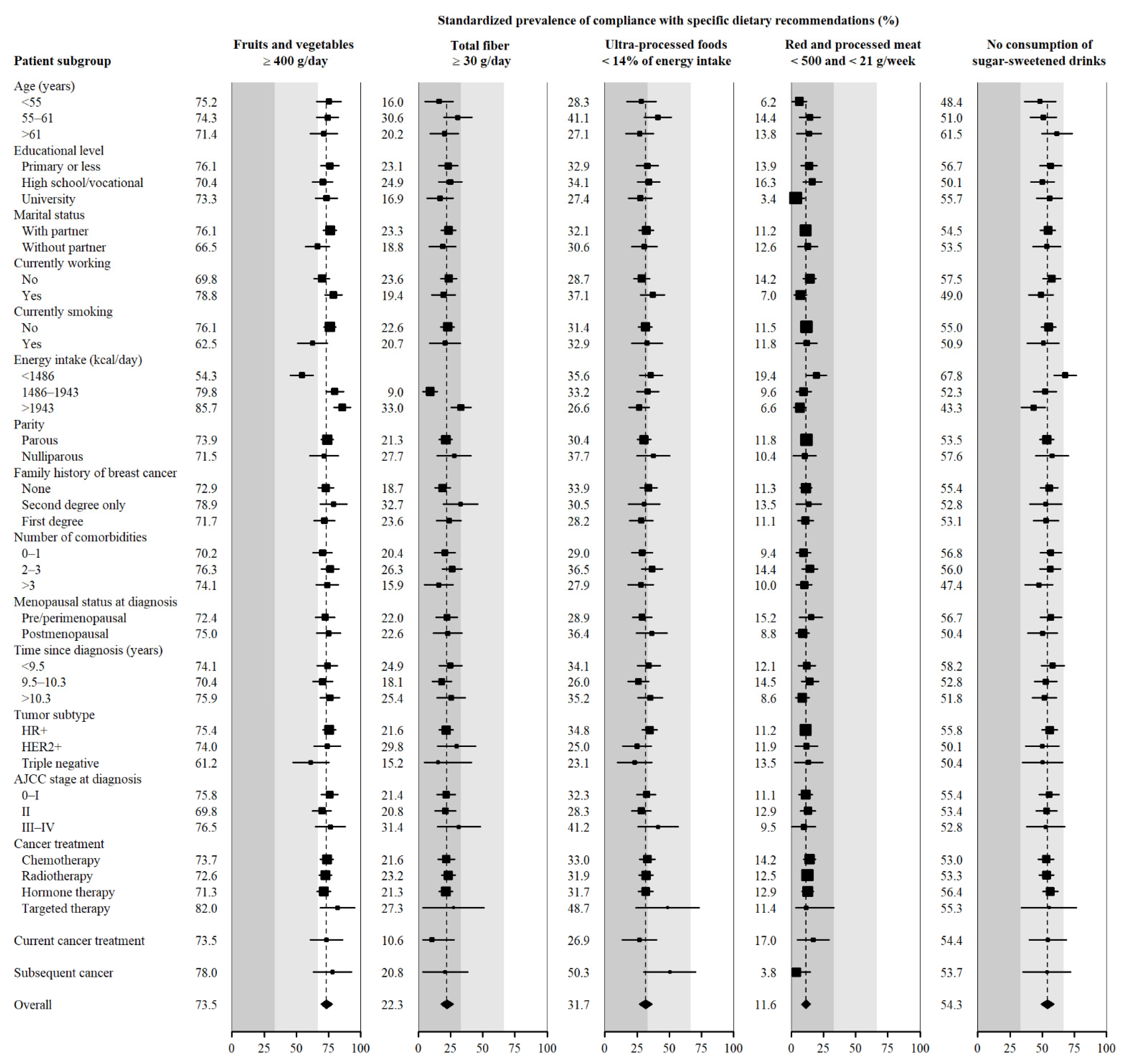
| 3. Eat a diet rich in wholegrains, vegetables, fruit and beans | Fruits and vegetables (g/day): | ||
| >400 | 0.5 | 309 (73.6) | |
| 200-<400 | 0.25 | 85 (20.2) | |
| <200 | 0 | 26 (6.2) | |
| Total fibre (g/day): | |||
| >30 | 0.5 | 57 (13.6) | |
| 15-<30 | 0.25 | 247 (58.8) | |
| <15 | 0 | 116 (27.6) | |
| 4. Limit consumption of “fast foods” and other processed foods high in fat, starches or sugars | Percent of total kcal from ultra-processed foods (aUPFs): | ||
| Tertile 1 (<14.0) | 1 | 140 (33.3) | |
| Tertile 2 (14.0–20.9) | 0.5 | 140 (33.3) | |
| Tertile 3 (>20.9) | 0 | 140 (33.3) | |
| 5. Limit consumption of red and processed meat | Total red meat (g/wk) and processed meat (g/wk): | ||
| Red meat <500 and processed meat <21 | 1 | 45 (10.7) | |
| Red meat <500 and processed meat 21-<100 | 0.5 | 134 (31.9) | |
| Red meat >500 or processed meat >100 | 0 | 241 (57.4) | |
| 6. Limit consumption of sugar-sweetened drinks | Total sugar-sweetened drinks (g/day): | ||
| 0 | 1 | 229 (54.5) | |
| >0-<250 | 0.5 | 176 (41.9) | |
| >250 | 0 | 15 (3.6) | |
| 7. Limit alcohol consumption | Total ethanol (g/day): | ||
| 0 | 1 | 121 (28.8) | |
| <14 (1 drink) | 0.5 | 260 (61.9) | |
| >14 (1 drink) | 0 | 39 (9.3) | |
4. Discussion
4.1. Be a Healthy Weight
4.2. Be Physically Active
4.3. Limit Alcohol Consumption
4.4. Eat a Diet Rich in Wholegrains, Vegetables, Fruit and Beans
4.5. Limit Consumption of “Fast Foods” and Other Processed Foods High in Fat, Starches or Sugars
4.6. Limit Consumption of Red and Processed Meat
4.7. Limit Consumption of Sugar-Sweetened Drinks
4.8. Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. Available online: https://gco.iarc.fr/today/home (accessed on 6 September 2022).
- ECIS European Cancer Information System. European Union. 2022. Available online: https://ecis.jrc.ec.europa.eu/ (accessed on 6 September 2022).
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Tomorrow. Lyon, France: International Agency for Research on Cancer. Available online: https://gco.iarc.fr/tomorrow/home (accessed on 6 September 2022).
- CNE Servidor Interactivo de Información Epidemiológica (ARIADNA). Centro Nacional de Epidemiología. Instituto de Salud Carlos III. Available online: http://ariadna.cne.isciii.es/ (accessed on 6 September 2022).
- Guevara, M.; Molinuevo, A.; Salmerón, D.; Marcos-Gragera, R.; Chirlaque, M.D.; Quirós, J.R.; Alemán, A.; Rojas, D.; Sabater, C.; Chico, M.; et al. Supervivencia de Cáncer En España, 2002–2013; Red Española de Registros de Cáncer (REDECAN). 2019. Available online: https://redecan.org/storage/documents/3878edcf-11e6-43c8-93dd-157a5ada4fb2.pdf (accessed on 6 September 2022).
- Red Española de Registros de Cáncer (REDECAN) La Prevalencia Del Cáncer En España a 31-12-2020; 2021. Available online: https://redecan.org/storage/documents/7e2ebf44-6440-4c69-b4e5-bff37d4f5420.pdf (accessed on 6 September 2022).
- World Cancer Research Fund/American Institute for Cancer Research. Food, Nutrition, Physical Activity, and the Prevention of Cancer: A Global Perspective; World Cancer Research Fund/American Institute for Cancer Research, Ed.; American Institute for Cancer Research: Washington, DC, USA, 2007; ISBN 978-0-9722522-2-5. [Google Scholar]
- World Cancer Research Fund/American Institute for Cancer Research. Diet, Nutrition, Physical Activity and Cancer: A Global Perspective. Third Expert Report. 2018. Available online: https://www.wcrf.org/wp-content/uploads/2021/02/Summary-of-Third-Expert-Report-2018.pdf (accessed on 6 September 2022).
- World Cancer Research Fund/American Institute for Cancer Research. Continuous Update Project Expert Report 2018. Recommendations and Public Health and Policy Implications. 2018. Available online: https://www.wcrf.org/wp-content/uploads/2021/01/Recommendations.pdf (accessed on 6 September 2022).
- Solans, M.; Chan, D.S.M.; Mitrou, P.; Norat, T.; Romaguera, D. A Systematic Review and Meta-Analysis of the 2007 WCRF/AICR Score in Relation to Cancer-Related Health Outcomes. Ann. Oncol. 2020, 31, 352–368. [Google Scholar] [CrossRef] [PubMed]
- Turati, F.; Dalmartello, M.; Bravi, F.; Serraino, D.; Augustin, L.; Giacosa, A.; Negri, E.; Levi, F.; La Vecchia, C. Adherence to the World Cancer Research Fund/American Institute for Cancer Research Recommendations and the Risk of Breast Cancer. Nutrients 2020, 12, 607. [Google Scholar] [CrossRef] [PubMed]
- Barrios-Rodríguez, R.; Toledo, E.; Martinez-Gonzalez, M.A.; Aguilera-Buenosvinos, I.; Romanos-Nanclares, A.; Jiménez-Moleón, J.J. Adherence to the 2018 World Cancer Research Fund/American Institute for Cancer Research Recommendations and Breast Cancer in the SUN Project. Nutrients 2020, 12, 2076. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, I.; Taljaard-Krugell, C.; Wicks, M.; Cubasch, H.; Joffe, M.; Laubscher, R.; Romieu, I.; Biessy, C.; Gunter, M.J.; Huybrechts, I.; et al. Adherence to Cancer Prevention Recommendations Is Associated with a Lower Breast Cancer Risk in Black Urban South African Women. Br. J. Nutr. 2022, 127, 927–938. [Google Scholar] [CrossRef] [PubMed]
- Castelló, A.; Martín, M.; Ruiz, A.; Casas, Á.M.; Baena-Cañada, J.M.; Lope, V.; Antolín, S.; Sánchez, P.; Ramos, M.; Antón, A.; et al. Lower Breast Cancer Risk among Women Following the World Cancer Research Fund and American Institute for Cancer Research Lifestyle Recommendations: EpiGEICAM Case-Control Study. PLoS ONE 2015, 10, e0126096. [Google Scholar] [CrossRef] [PubMed]
- Handbook of Cancer Survivorship, 2nd ed.; Feuerstein, M., Nekhlyudov, L., Eds.; Springer: Cham, Switzerland, 2018; ISBN 978-3-319-77430-5. [Google Scholar]
- World Cancer Research Fund/American Institute for Cancer Research. Continuous Update Project Expert Report 2018. Survivors of Breast and Other Cancers. 2018. Available online: https://www.wcrf.org/wp-content/uploads/2021/02/Cancer-Survivors.pdf (accessed on 6 September 2022).
- Tollosa, D.N.; Tavener, M.; Hure, A.; James, E.L. Adherence to Multiple Health Behaviours in Cancer Survivors: A Systematic Review and Meta-Analysis. J. Cancer Surviv. 2019, 13, 327–343. [Google Scholar] [CrossRef] [PubMed]
- Springfield, S.; Odoms-Young, A.; Tussing-Humphreys, L.; Freels, S.; Stolley, M. Adherence to American Cancer Society and American Institute of Cancer Research Dietary Guidelines in Overweight African American Breast Cancer Survivors. J. Cancer Surviv. 2019, 13, 257–268. [Google Scholar] [CrossRef]
- Tollosa, D.N.; Tavener, M.; Hure, A.; James, E.L. Compliance with Multiple Health Behaviour Recommendations: A Cross-Sectional Comparison between Female Cancer Survivors and Those with No Cancer History. Int. J. Environ. Res. Public Health 2019, 16, 1345. [Google Scholar] [CrossRef]
- Castelló, A.; Pollán, M.; Buijsse, B.; Ruiz, A.; Casas, Á.M.; Baena-Cañada, J.M.; Lope, V.; Antolín, S.; Ramos, M.; Muñoz, M.; et al. Spanish Mediterranean Diet and Other Dietary Patterns and Breast Cancer Risk: Case-Control EpiGEICAM Study. Br. J. Cancer 2014, 111, 1454–1462. [Google Scholar] [CrossRef]
- Lope, V.; Martín, M.; Castelló, A.; Casla, S.; Ruiz, A.; Baena-Cañada, J.M.; Casas, Á.M.; Calvo, L.; Bermejo, B.; Muñoz, M.; et al. Physical Activity and Breast Cancer Risk by Pathological Subtype. Gynecol. Oncol. 2017, 144, 577–585. [Google Scholar] [CrossRef]
- Vioque, J.; Navarrete-Muñoz, E.-M.; Gimenez-Monzó, D.; García-de-la-Hera, M.; Granado, F.; Young, I.S.; Ramón, R.; Ballester, F.; Murcia, M.; Rebagliato, M.; et al. Reproducibility and Validity of a Food Frequency Questionnaire among Pregnant Women in a Mediterranean Area. Nutr. J. 2013, 12, 26. [Google Scholar] [CrossRef]
- Moreiras, O.; Carbajal, A.; Cabrera, L.; Cuadrado, C. Tablas de Composición de Alimentos: Guía de Prácticas; Piramide: Madrid, Spain, 2018. [Google Scholar]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th Edition of the AJCC Cancer Staging Manual and the Future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef]
- Shams-White, M.M.; Brockton, N.T.; Mitrou, P.; Romaguera, D.; Brown, S.; Bender, A.; Kahle, L.L.; Reedy, J. Operationalizing the 2018 World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) Cancer Prevention Recommendations: A Standardized Scoring System. Nutrients 2019, 11, 1572. [Google Scholar] [CrossRef]
- Shams-White, M.M.; Romaguera, D.; Mitrou, P.; Reedy, J.; Bender, A.; Brockton, N.T. Further Guidance in Implementing the Standardized 2018 World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) Score. Cancer Epidemiol. Biomark. Prev. 2020, 29, 889–894. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Cannon, G.; Lawrence, M.; Costa Louzada, M.L.; Pereira Machado, P. Ultra-Processed Foods, Diet Quality, and Health Using the NOVA Classification System; FAO: Rome, Italy, 2019; Available online: https://www.fao.org/3/ca5644en/ca5644en.pdf (accessed on 6 September 2022).
- Ministerio de Sanidad, Servicios Sociales e Igualdad. Actividad Física Para La Salud y Reducción Del Sedentarismo. Recomendaciones Para La Población. Estrategia de Promoción de La Salud y Prevención En El SNS; Ministerio de Sanidad, Servicios Sociales e Igualdad: Madrid, Spain, 2015. Available online: https://www.sanidad.gob.es/profesionales/saludPublica/prevPromocion/Estrategia/docs/Recomendaciones_ActivFisica_para_la_Salud.pdf (accessed on 6 September 2022).
- Greenland, S. Model-Based Estimation of Relative Risks and Other Epidemiologic Measures in Studies of Common Outcomes and in Case-Control Studies. Am. J. Epidemiol. 2004, 160, 301–305. [Google Scholar] [CrossRef]
- Localio, A.R.; Margolis, D.J.; Berlin, J.A. Relative Risks and Confidence Intervals Were Easily Computed Indirectly from Multivariable Logistic Regression. J. Clin. Epidemiol. 2007, 60, 874–882. [Google Scholar] [CrossRef]
- Tollosa, D.N.; Holliday, E.; Hure, A.; Tavener, M.; James, E.L. A 15-Year Follow-up Study on Long-Term Adherence to Health Behaviour Recommendations in Women Diagnosed with Breast Cancer. Breast Cancer Res. Treat. 2020, 182, 727–738. [Google Scholar] [CrossRef]
- Ramirez, L.A.; Chung, Y.; Wonsuk, Y.; Fontenot, B.; Ansa, B.E.; Whitehead, M.S.; Smith, S.A. Determinants of Adherence to Nutrition-Related Cancer Prevention Guidelines among African American Breast Cancer Survivors. J. Ga. Public Health Assoc. 2016, 6, 210–222. [Google Scholar] [CrossRef]
- Paxton, R.J.; Garner, W.; Dean, L.T.; Logan, G.; Allen-Watts, K. Health Behaviors and Lifestyle Interventions in African American Breast Cancer Survivors: A Review. Front. Oncol. 2019, 9, 3. [Google Scholar] [CrossRef]
- Instituto Nacional de Estadística Encuesta Europea de Salud En España (EESE). INEbase. 2020. Available online: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736176784&menu=resultados&idp=1254735573175 (accessed on 6 September 2022).
- Rogers, l.Q.; Carter, S.J.; Williams, G.; Courneya, K.S. Physical Activity. In Handbook of Cancer Survivorship; Feuerstein, M., Nekhlyudov, L., Eds.; Springer: Cham, Switzerland, 2018; pp. 287–307. ISBN 978-3-319-77430-5. [Google Scholar]
- Vance, V.; Mourtzakis, M.; McCargar, L.; Hanning, R. Weight Gain in Breast Cancer Survivors: Prevalence, Pattern and Health Consequences. Obes. Rev. 2011, 12, 282–294. [Google Scholar] [CrossRef]
- Pageot, Y.K.; Stanton, A.L.; Ganz, P.A.; Irwin, M.R.; Cole, S.W.; Crespi, C.M.; Breen, E.C.; Kuhlman, K.R.; Bower, J.E. Socioeconomic Status and Inflammation in Women with Early-Stage Breast Cancer: Mediation by Body Mass Index. Brain Behav. Immun. 2022, 99, 307–316. [Google Scholar] [CrossRef]
- Audrain-McGovern, J.; Benowitz, N.L. Cigarette Smoking, Nicotine, and Body Weight. Clin. Pharmacol. Ther. 2011, 90, 164–168. [Google Scholar] [CrossRef]
- Harvie, M.N.; Bokhari, S.; Shenton, A.; Ashcroft, L.; Evans, G.; Swindell, R.; Howell, A. Adult Weight Gain and Central Obesity in Women with and without a Family History of Breast Cancer: A Case Control Study. Fam. Cancer 2007, 6, 287–294. [Google Scholar] [CrossRef]
- Spei, M.-E.; Samoli, E.; Bravi, F.; La Vecchia, C.; Bamia, C.; Benetou, V. Physical Activity in Breast Cancer Survivors: A Systematic Review and Meta-Analysis on Overall and Breast Cancer Survival. Breast 2019, 44, 144–152. [Google Scholar] [CrossRef]
- Blanchard, C.M.; Courneya, K.S.; Stein, K. American Cancer Society’s SCS-II Cancer Survivors’ Adherence to Lifestyle Behavior Recommendations and Associations with Health-Related Quality of Life: Results from the American Cancer Society’s SCS-II. J. Clin. Oncol. 2008, 26, 2198–2204. [Google Scholar] [CrossRef]
- Littman, A.J.; Tang, M.-T.; Rossing, M.A. Longitudinal Study of Recreational Physical Activity in Breast Cancer Survivors. J. Cancer Surviv. 2010, 4, 119–127. [Google Scholar] [CrossRef]
- Mason, C.; Alfano, C.M.; Smith, A.W.; Wang, C.-Y.; Neuhouser, M.L.; Duggan, C.; Bernstein, L.; Baumgartner, K.B.; Baumgartner, R.N.; Ballard-Barbash, R.; et al. Long-Term Physical Activity Trends in Breast Cancer Survivors. Cancer Epidemiol. Biomark. Prev. 2013, 22, 1153–1161. [Google Scholar] [CrossRef]
- Bruno, E.; Gargano, G.; Villarini, A.; Traina, A.; Johansson, H.; Mano, M.P.; Santucci De Magistris, M.; Simeoni, M.; Consolaro, E.; Mercandino, A.; et al. Adherence to WCRF/AICR Cancer Prevention Recommendations and Metabolic Syndrome in Breast Cancer Patients. Int. J. Cancer 2016, 138, 237–244. [Google Scholar] [CrossRef]
- Llamosas-Falcón, L.; Manthey, J.; Rehm, J. Changes in Alcohol Consumption in Spain between 1990 and 2019. Adicciones 2020, 34, 61–72. [Google Scholar] [CrossRef]
- Kwok, A.; Dordevic, A.L.; Paton, G.; Page, M.J.; Truby, H. Effect of Alcohol Consumption on Food Energy Intake: A Systematic Review and Meta-Analysis. Br. J. Nutr. 2019, 121, 481–495. [Google Scholar] [CrossRef]
- Observatorio Español de las Drogas y las Adicciones Monografía Alcohol 2021. Consumo y Consecuencias; Ministerio de Sanidad. Delegación del Gobierno para el Plan Nacional sobre Drogas: Madrid, Spain, 2021; p. 109. Available online: https://www.observatoriodelainfancia.es/ficherosoia/documentos/7689_d_Alcohol-2021.pdf (accessed on 6 September 2022).
- He, J.; Gu, Y.; Zhang, S. Consumption of Vegetables and Fruits and Breast Cancer Survival: A Systematic Review and Meta-Analysis. Sci. Rep. 2017, 7, 599. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.; Luo, W.-P.; Zhang, C.-X. Fruit and Vegetable Intake and Breast Cancer Prognosis: A Meta-Analysis of Prospective Cohort Studies. Br. J. Nutr. 2017, 117, 737–749. [Google Scholar] [CrossRef]
- World Cancer Research Fund/American Institute for Cancer Research. Continuous Update Project Expert Report 2018. Diet, Nutrition, Physical Activity and Breast Cancer Survivors; Revised 2018. Available online: https://www.aicr.org/wp-content/uploads/2020/01/2014-breast-cancer-survivorship-cup.pdf (accessed on 6 September 2022).
- Park, S.-H.; Hoang, T.; Kim, J. Dietary Factors and Breast Cancer Prognosis among Breast Cancer Survivors: A Systematic Review and Meta-Analysis of Cohort Studies. Cancers 2021, 13, 5329. [Google Scholar] [CrossRef] [PubMed]
- Jayedi, A.; Emadi, A.; Khan, T.A.; Abdolshahi, A.; Shab-Bidar, S. Dietary Fiber and Survival in Women with Breast Cancer: A Dose-Response Meta-Analysis of Prospective Cohort Studies. Nutr. Cancer 2021, 73, 1570–1580. [Google Scholar] [CrossRef] [PubMed]
- Dennis Parker, E.A.; Sheppard, V.B.; Adams-Campbell, L. Compliance with National Nutrition Recommendations among Breast Cancer Survivors in “Stepping Stone”. Integr. Cancer Ther. 2014, 13, 114–120. [Google Scholar] [CrossRef] [PubMed]
- González-Rodríguez, L.G.; Perea Sánchez, J.M.; Aranceta-Bartrina, J.; Gil, Á.; González-Gross, M.; Serra-Majem, L.; Varela-Moreiras, G.; Ortega, R.M. Intake and Dietary Food Sources of Fibre in Spain: Differences with Regard to the Prevalence of Excess Body Weight and Abdominal Obesity in Adults of the ANIBES Study. Nutrients 2017, 9, 326. [Google Scholar] [CrossRef]
- Dehghan, M.; Akhtar-Danesh, N.; Merchant, A.T. Factors Associated with Fruit and Vegetable Consumption among Adults. J. Hum. Nutr. Diet 2011, 24, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Azagba, S.; Sharaf, M.F. Disparities in the Frequency of Fruit and Vegetable Consumption by Socio-Demographic and Lifestyle Characteristics in Canada. Nutr. J. 2011, 10, 118. [Google Scholar] [CrossRef]
- Blanco-Rojo, R.; Sandoval-Insausti, H.; López-Garcia, E.; Graciani, A.; Ordovás, J.M.; Banegas, J.R.; Rodríguez-Artalejo, F.; Guallar-Castillón, P. Consumption of Ultra-Processed Foods and Mortality: A National Prospective Cohort in Spain. Mayo Clin. Proc. 2019, 94, 2178–2188. [Google Scholar] [CrossRef]
- Kenkhuis, M.-F.; van der Linden, B.W.A.; Breedveld-Peters, J.J.L.; Koole, J.L.; van Roekel, E.H.; Breukink, S.O.; Mols, F.; Weijenberg, M.P.; Bours, M.J.L. Associations of the Dietary World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) Recommendations with Patient-Reported Outcomes in Colorectal Cancer Survivors 2-10 Years Post-Diagnosis: A Cross-Sectional Analysis. Br. J. Nutr. 2021, 125, 1188–1200. [Google Scholar] [CrossRef]
- Fiolet, T.; Srour, B.; Sellem, L.; Kesse-Guyot, E.; Allès, B.; Méjean, C.; Deschasaux, M.; Fassier, P.; Latino-Martel, P.; Beslay, M.; et al. Consumption of Ultra-Processed Foods and Cancer Risk: Results from NutriNet-Santé Prospective Cohort. BMJ 2018, 360, k322. [Google Scholar] [CrossRef]
- Romaguera, D.; Fernández-Barrés, S.; Gracia-Lavedán, E.; Vendrell, E.; Azpiri, M.; Ruiz-Moreno, E.; Martín, V.; Gómez-Acebo, I.; Obón, M.; Molinuevo, A.; et al. Consumption of Ultra-Processed Foods and Drinks and Colorectal, Breast, and Prostate Cancer. Clin. Nutr. 2021, 40, 1537–1545. [Google Scholar] [CrossRef]
- Karavasiloglou, N.; Hüsing, A.; Masala, G.; van Gils, C.H.; Turzanski Fortner, R.; Chang-Claude, J.; Huybrechts, I.; Weiderpass, E.; Gunter, M.; Arveux, P.; et al. Adherence to the World Cancer Research Fund/American Institute for Cancer Research Cancer Prevention Recommendations and Risk of in Situ Breast Cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC) Cohort. BMC Med. 2019, 17, 221. [Google Scholar] [CrossRef]
- van Veen, M.R.; Mols, F.; Bours, M.J.L.; Weijenberg, M.P.; Kampman, E.; Beijer, S. Adherence to the World Cancer Research Fund/American Institute for Cancer Research Recommendations for Cancer Prevention Is Associated with Better Health-Related Quality of Life among Long-Term Colorectal Cancer Survivors: Results of the PROFILES Registry. Support. Care Cancer 2019, 27, 4565–4574. [Google Scholar] [CrossRef]
- FAOSTAT Food Balances (2010-). Food and Agriculture Organization of the United Nations. Available online: https://www.fao.org/faostat/en/#data/FBS (accessed on 6 September 2022).
- Ministerio de Agricultura, Pesca y Alimentación. Informe Del Consumo de Alimentación En España 2019; Ministerio de Agricultura, Pesca y Alimentación: Madrid, Spain, 2020. Available online: https://www.mapa.gob.es/ca/alimentacion/temas/consumo-tendencias/informe2019_v2_tcm34-540250.pdf (accessed on 6 September 2022).
- Ministerio de Agricultura, Pesca y Alimentación. Informe Del Consumo de Alimentación En España 2020; Ministerio de Agricultura, Pesca y Alimentación: Madrid, Spain, 2021. Available online: https://www.mapa.gob.es/ca/alimentacion/temas/consumo-tendencias/informe-anual-consumo-2020-v2-nov2021-baja-res_tcm34-562704.pdf (accessed on 6 September 2022).
- De Cicco, P.; Catani, M.V.; Gasperi, V.; Sibilano, M.; Quaglietta, M.; Savini, I. Nutrition and Breast Cancer: A Literature Review on Prevention, Treatment and Recurrence. Nutrients 2019, 11, 1514. [Google Scholar] [CrossRef]
- Jochems, S.H.J.; Van Osch, F.H.M.; Bryan, R.T.; Wesselius, A.; van Schooten, F.J.; Cheng, K.K.; Zeegers, M.P. Impact of Dietary Patterns and the Main Food Groups on Mortality and Recurrence in Cancer Survivors: A Systematic Review of Current Epidemiological Literature. BMJ Open 2018, 8, e014530. [Google Scholar] [CrossRef]
- World Cancer Research Fund/American Institute for Cancer Research. Continuous Update Project Expert Report 2018. Meat, Fish and Dairy Products and the Risk of Cancer; World Cancer Research Fund International: London, UK, 2018; Available online: https://www.wcrf.org/wp-content/uploads/2021/02/Meat-fish-and-dairy-products.pdf (accessed on 6 September 2022).
- McCullough, M.L.; Gapstur, S.M.; Shah, R.; Campbell, P.T.; Wang, Y.; Doyle, C.; Gaudet, M.M. Pre- and Postdiagnostic Diet in Relation to Mortality among Breast Cancer Survivors in the CPS-II Nutrition Cohort. Cancer Causes Control 2016, 27, 1303–1314. [Google Scholar] [CrossRef]
- de Vries, Y.C.; van den Berg, M.M.G.A.; de Vries, J.H.M.; Boesveldt, S.; de Kruif, J.T.C.M.; Buist, N.; Haringhuizen, A.; Los, M.; Sommeijer, D.W.; Timmer-Bonte, J.H.N.; et al. Differences in Dietary Intake during Chemotherapy in Breast Cancer Patients Compared to Women without Cancer. Support. Care Cancer 2017, 25, 2581–2591. [Google Scholar] [CrossRef]
- Boltong, A.; Keast, R. The Influence of Chemotherapy on Taste Perception and Food Hedonics: A Systematic Review. Cancer Treat. Rev. 2012, 38, 152–163. [Google Scholar] [CrossRef]
- Romanos-Nanclares, A.; Toledo, E.; Gardeazabal, I.; Jiménez-Moleón, J.J.; Martínez-González, M.A.; Gea, A. Sugar-Sweetened Beverage Consumption and Incidence of Breast Cancer: The Seguimiento Universidad de Navarra (SUN) Project. Eur. J. Nutr. 2019, 58, 2875–2886. [Google Scholar] [CrossRef]
- Rothman, K.J. Six Persistent Research Misconceptions. J. Gen. Intern. Med. 2014, 29, 1060–1064. [Google Scholar] [CrossRef] [PubMed]


| Adherence to WCRF/AICR Recommendations | ||||||
| Total | Low | Moderate | High | |||
| (1.25–3.25) | (3.50–4.25) | (4.50–7) | ||||
| n (%) | n (%) | n (%) | n (%) | p-value | ||
| Total | 420 (100.0) | 139 (33.1) | 151 (36.0) | 130 (31.0) | ||
| Adherence score, mean (SD) | 3.9 (1.0) | |||||
| Age, mean (SD) | 59.1 (9.0) | 57.6 (8.9) | 59.5 (9.2) | 60.2 (8.8) | 0.014 | |
| Educational level | ||||||
| Primary education or less | 156 (37.7) | 46 (33.6) | 56 (37.8) | 54 (41.9) | 0.016 | |
| High school/vocational training | 133 (32.1) | 49 (35.8) | 36 (24.3) | 48 (37.2) | ||
| University graduate | 125 (30.2) | 42 (30.7) | 56 (37.8) | 27 (20.9) | ||
| Marital status | ||||||
| With partner | 308 (73.5) | 99 (71.2) | 113 (75.3) | 96 (73.8) | 0.727 | |
| Without partner | 111 (26.5) | 40 (28.8) | 37 (24.7) | 34 (26.2) | ||
| Currently working | ||||||
| No | 250 (60.7) | 70 (51.5) | 92 (61.7) | 88 (69.3) | 0.012 | |
| Yes | 162 (39.3) | 66 (48.5) | 57 (38.3) | 39 (30.7) | ||
| Currently smoking | ||||||
| No | 340 (81.3) | 101 (73.2) | 125 (82.8) | 114 (88.4) | 0.005 | |
| Yes | 78 (18.7) | 37 (26.8) | 26 (17.2) | 15 (11.6) | ||
| Energy intake kcal/d, mean (SD) | 1775.0 (571.2) | 1865.5 (628.8) | 1746.0 (520.0) | 1711.9 (555.4) | 0.026 | |
| Parity | ||||||
| Parous | 346 (82.8) | 120 (86.3) | 119 (79.3) | 107 (82.9) | 0.289 | |
| Nulliparous | 72 (17.2) | 19 (13.7) | 31 (20.7) | 22 (17.1) | ||
| Family history of breast cancer | ||||||
| None | 227 (54.0) | 73 (52.5) | 71 (47.0) | 83 (63.8) | 0.062 | |
| Second degree only | 67 (16.0) | 22 (15.8) | 26 (17.2) | 19 (14.6) | ||
| First degree | 126 (30.0) | 44 (31.7) | 54 (35.8) | 28 (21.5) | ||
| Number of comorbidities | ||||||
| ≤1 | 134 (35.4) | 53 (41.7) | 42 (30.9) | 39 (33.6) | 0.396 | |
| 2–3 | 152 (40.1) | 44 (34.6) | 58 (42.6) | 50 (43.1) | ||
| >3 | 93 (24.5) | 30 (23.6) | 36 (26.5) | 27 (23.3) | ||
| Menopausal status at diagnosis | ||||||
| Pre/perimenopausal | 240 (61.9) | 85 (67.5) | 84 (60.0) | 71 (58.2) | 0.276 | |
| Postmenopausal | 148 (38.1) | 41 (32.5) | 56 (40.0) | 51 (41.8) | ||
| Years since diagnosis | 10.0 (1.0) | 9.9 (0.9) | 10.0 (1.0) | 10.0 (1.0) | 0.792 | |
| Tumour subtype a | ||||||
| HR+ | 301 (71.7) | 97 (69.8) | 108 (71.5) | 96 (73.8) | 0.704 | |
| HER2+ | 72 (17.1) | 28 (20.1) | 23 (15.2) | 21 (16.2) | ||
| TN | 47 (11.2) | 14 (10.1) | 20 (13.2) | 13 (10.0) | ||
| AJCC stage at diagnosis b | ||||||
| 0–I | 189 (45.4) | 57 (42.2) | 74 (49.0) | 58 (44.6) | 0.290 | |
| II | 176 (42.3) | 66 (48.9) | 56 (37.1) | 54 (41.5) | ||
| III–IV | 51 (12.3) | 12 (8.9) | 21 (13.9) | 18 (13.0) | ||
| Cancer treatment | ||||||
| Chemotherapy | 311 (74.4) | 106 (76.8) | 110 (72.8) | 95 (73.6) | 0.722 | |
| Radiotherapy | 326 (78.0) | 106 (76.3) | 114 (75.5) | 106 (82.8) | 0.283 | |
| Hormonetherapy | 340 (81.0) | 111 (79.9) | 121 (80.1) | 108 (83.1) | 0.758 | |
| Targeted therapy | 63 (15.0) | 23 (16.5) | 21 (13.9) | 19 (14.6) | 0.812 | |
| Current cancer treatment | 57 (13.7) | 24 (17.5) | 17 (11.3) | 16 (12.4) | 0.267 | |
| Subsequent cancer c | 50 (11.9) | 18 (13.0) | 15 (9.9) | 17 (13.1) | 0.638 | |
| Standardized Prevalence Ratio (95% CI) a | |||
| Moderate Compliance | High Compliance | ||
| Age, y b | |||
| <55 | 1.00 | 1.00 | |
| 55–61 | 1.01 (0.67–1.53) | 1.17 (0.79–1.74) | |
| >61 | 1.30 (0.74–2.28) | 0.74 (0.39–1.41) | |
| Educational level | |||
| Primary education or less | 1.00 | 1.00 | |
| High school/vocational training | 0.89 (0.61–1.30) | 0.97 (0.68–1.38) | |
| University graduate | 1.39 (0.98–1.98) | 0.59 (0.36–0.96) | |
| Marital status | |||
| With partner | 1.00 | 1.00 | |
| Without partner | 0.94 (0.67–1.34) | 0.83 (0.55–1.26) | |
| Currently working | |||
| No | 1.00 | 1.00 | |
| Yes | 0.86 (0.60–1.24) | 0.96 (0.65–1.41) | |
| Currently smoking | |||
| No | 1.00 | 1.00 | |
| Yes | 1.12 (0.78–1.61) | 0.69 (0.42–1.16) | |
| Energy intake, kcal/d b | |||
| <1486 | 1.00 | 1.00 | |
| 1486–1943 | 1.22 (0.87–1.71) | 0.81 (0.55–1.19) | |
| >1943 | 1.00 (0.68–1.46) | 0.91 (0.62–1.33) | |
| Parity | |||
| Parous | 1.00 | 1.00 | |
| Nulliparous | 1.27 (0.90–1.80) | 1.03 (0.67–1.59) | |
| Family history of breast cancer | |||
| None | 1.00 | 1.00 | |
| Second degree only | 1.12 (0.72–1.72) | 0.79 (0.50–1.24) | |
| First degree | 1.61 (1.19–2.19) | 0.60 (0.39–0.92) | |
| Number of comorbidities | |||
| ≤1 | 1.00 | 1.00 | |
| 2–3 | 1.25 (0.89–1.77) | 1.16 (0.81–1.68) | |
| >3 | 1.35 (0.92–1.99) | 0.98 (0.63–1.53) | |
| Menopausal status at diagnosis | |||
| Pre/perimenopausal | 1.00 | 1.00 | |
| Postmenopausal | 0.90 (0.55–1.45) | 1.38 (0.83–2.30) | |
| Years since diagnosis b | |||
| <9.53 | 1.00 | 1.00 | |
| 9.54–10.28 | 1.13 (0.79–1.60) | 0.75 (0.50–1.14) | |
| >10.28 | 1.00 (0.68–1.48) | 1.03 (0.70–1.53) | |
| Tumour subtype c | |||
| HR+ | 1.00 | 1.00 | |
| HER2+ | 0.84 (0.54–1.30) | 0.75 (0.47–1.22) | |
| TN | 1.10 (0.71–1.71) | 0.78 (0.44–1.39) | |
| AJCC stage at diagnosis d | |||
| 0–I | 1.00 | 1.00 | |
| II | 0.83 (0.60–1.15) | 0.97 (0.68–1.40) | |
| III–IV | 0.91 (0.57–1.44) | 1.33 (0.85–2.09) | |
| Cancer treatment | |||
| Chemotherapy | 0.91 (0.63–1.31 ) | 1.14 (0.74–1.76) | |
| Radiotherapy | 0.78 (0.57–1.07) | 1.39 (0.89–2.20) | |
| Hormonetherapy | 0.99 (0.63–1.57) | 1.20 (0.69–2.08) | |
| Targeted therapy | 1.29 (0.72–2.32) | 1.12 (0.54–2.30) | |
| Current cancer treatment | 0.89 (0.56–1.41) | 0.85 (0.50–1.44) | |
| Subsequent cancer e | 1.01 (0.58–1.76) | 1.06 (0.58–1.97) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lope, V.; Guerrero-Zotano, A.; Ruiz-Moreno, E.; Bermejo, B.; Antolín, S.; Montaño, Á.; Baena-Cañada, J.M.; Ramos Vázquez, M.; Fernández de Larrea-Baz, N.; Chacón, J.I.; et al. Clinical and Sociodemographic Determinants of Adherence to World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) Recommendations in Breast Cancer Survivors—Health-EpiGEICAM Study. Cancers 2022, 14, 4705. https://doi.org/10.3390/cancers14194705
Lope V, Guerrero-Zotano A, Ruiz-Moreno E, Bermejo B, Antolín S, Montaño Á, Baena-Cañada JM, Ramos Vázquez M, Fernández de Larrea-Baz N, Chacón JI, et al. Clinical and Sociodemographic Determinants of Adherence to World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) Recommendations in Breast Cancer Survivors—Health-EpiGEICAM Study. Cancers. 2022; 14(19):4705. https://doi.org/10.3390/cancers14194705
Chicago/Turabian StyleLope, Virginia, Angel Guerrero-Zotano, Emma Ruiz-Moreno, Begoña Bermejo, Silvia Antolín, Álvaro Montaño, José Manuel Baena-Cañada, Manuel Ramos Vázquez, Nerea Fernández de Larrea-Baz, José Ignacio Chacón, and et al. 2022. "Clinical and Sociodemographic Determinants of Adherence to World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) Recommendations in Breast Cancer Survivors—Health-EpiGEICAM Study" Cancers 14, no. 19: 4705. https://doi.org/10.3390/cancers14194705
APA StyleLope, V., Guerrero-Zotano, A., Ruiz-Moreno, E., Bermejo, B., Antolín, S., Montaño, Á., Baena-Cañada, J. M., Ramos Vázquez, M., Fernández de Larrea-Baz, N., Chacón, J. I., García-Sáenz, J. A., Olier, C., Muñoz, M., Antón, A., Sánchez Rovira, P., Arcusa Lanza, A., González, S., Oltra, A., Brunet, J., ... Pollán, M. (2022). Clinical and Sociodemographic Determinants of Adherence to World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) Recommendations in Breast Cancer Survivors—Health-EpiGEICAM Study. Cancers, 14(19), 4705. https://doi.org/10.3390/cancers14194705