
The Feasibility of Stereotactic Body Proton Beam Therapy for Pancreatic Cancer

 ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
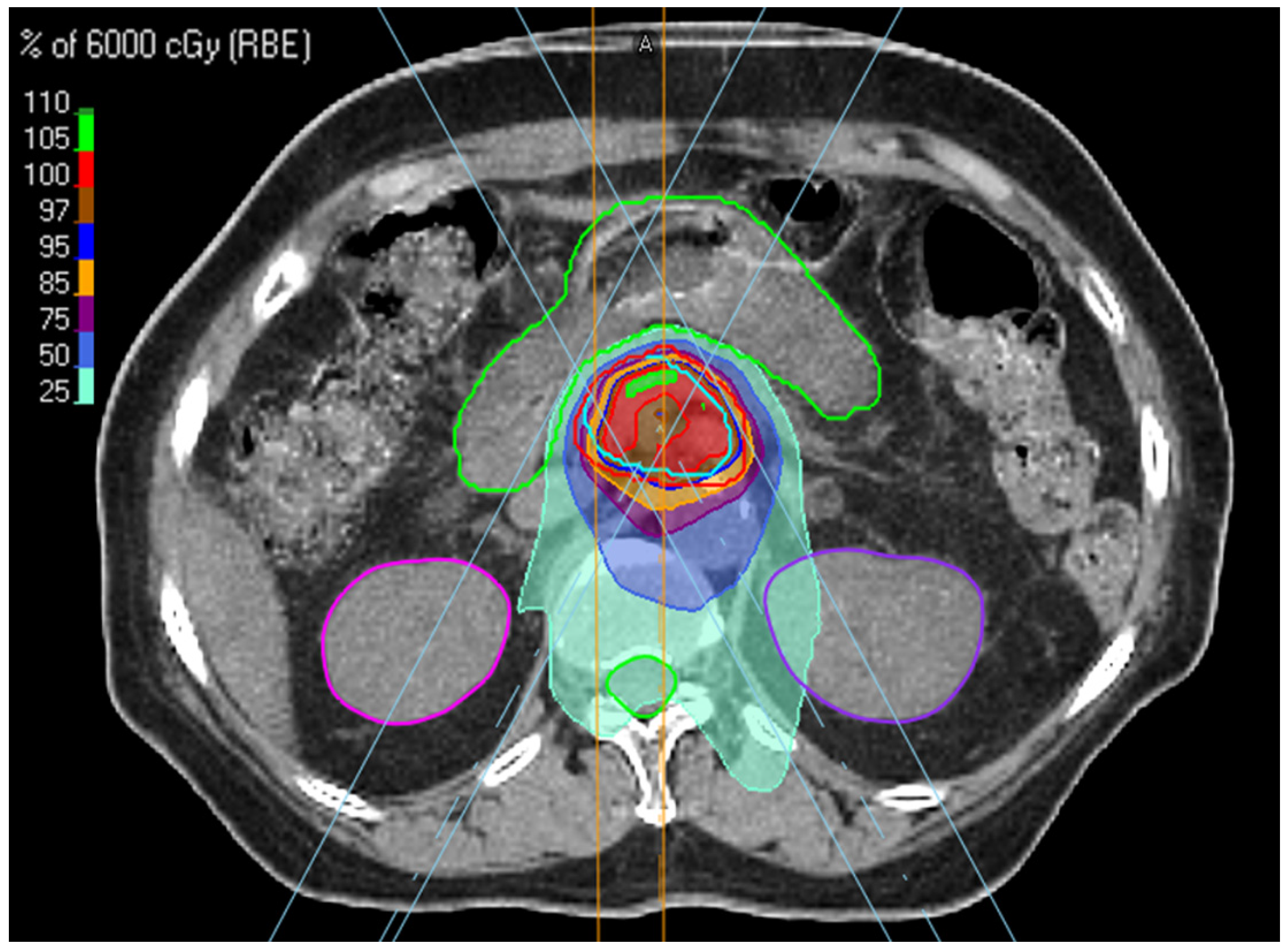
2.2. Treatment
2.3. Endpoints and Statistical Analysis
3. Results
3.1. Patient Characteristics
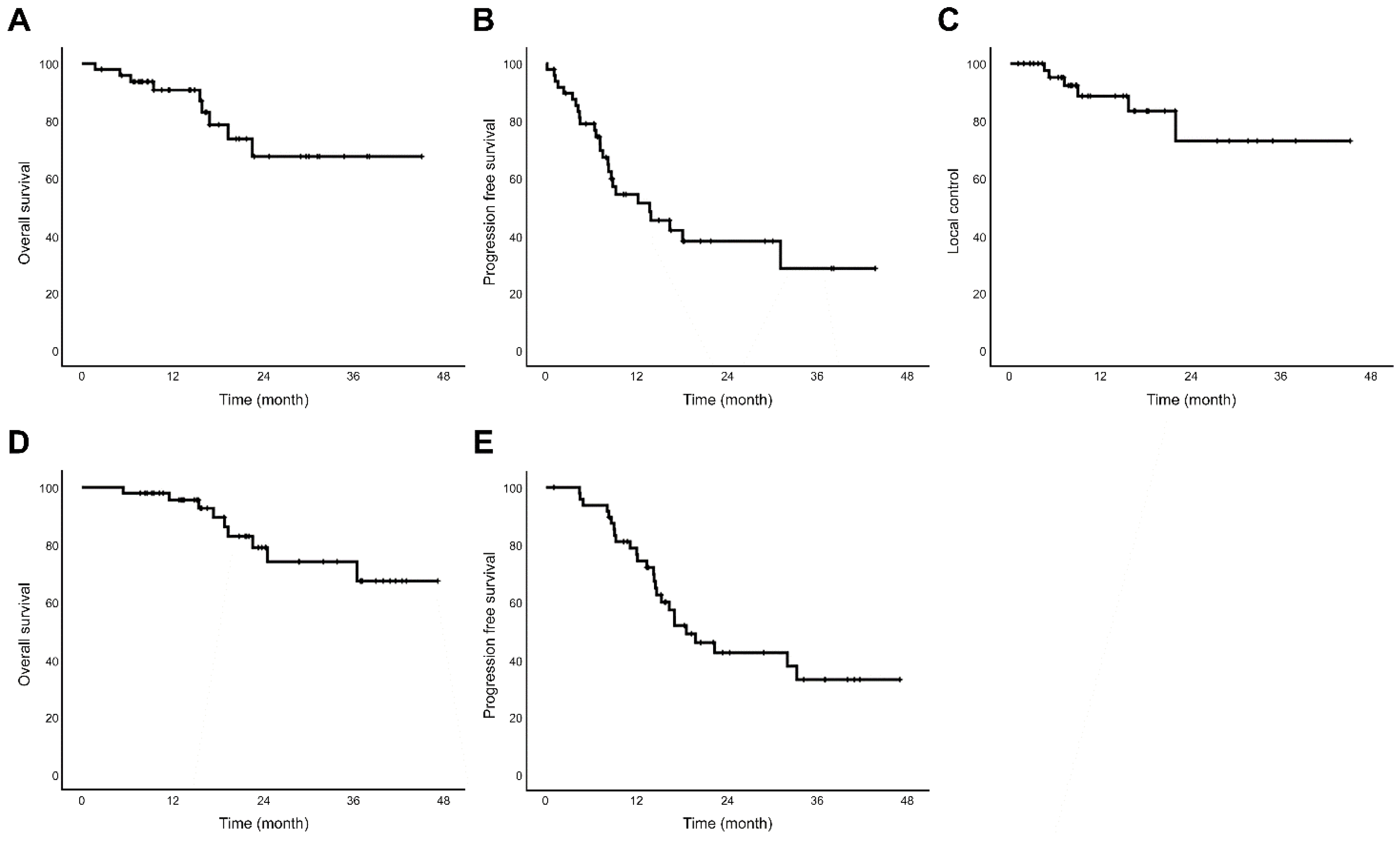
3.2. Survival Outcomes and Prognostic Factors
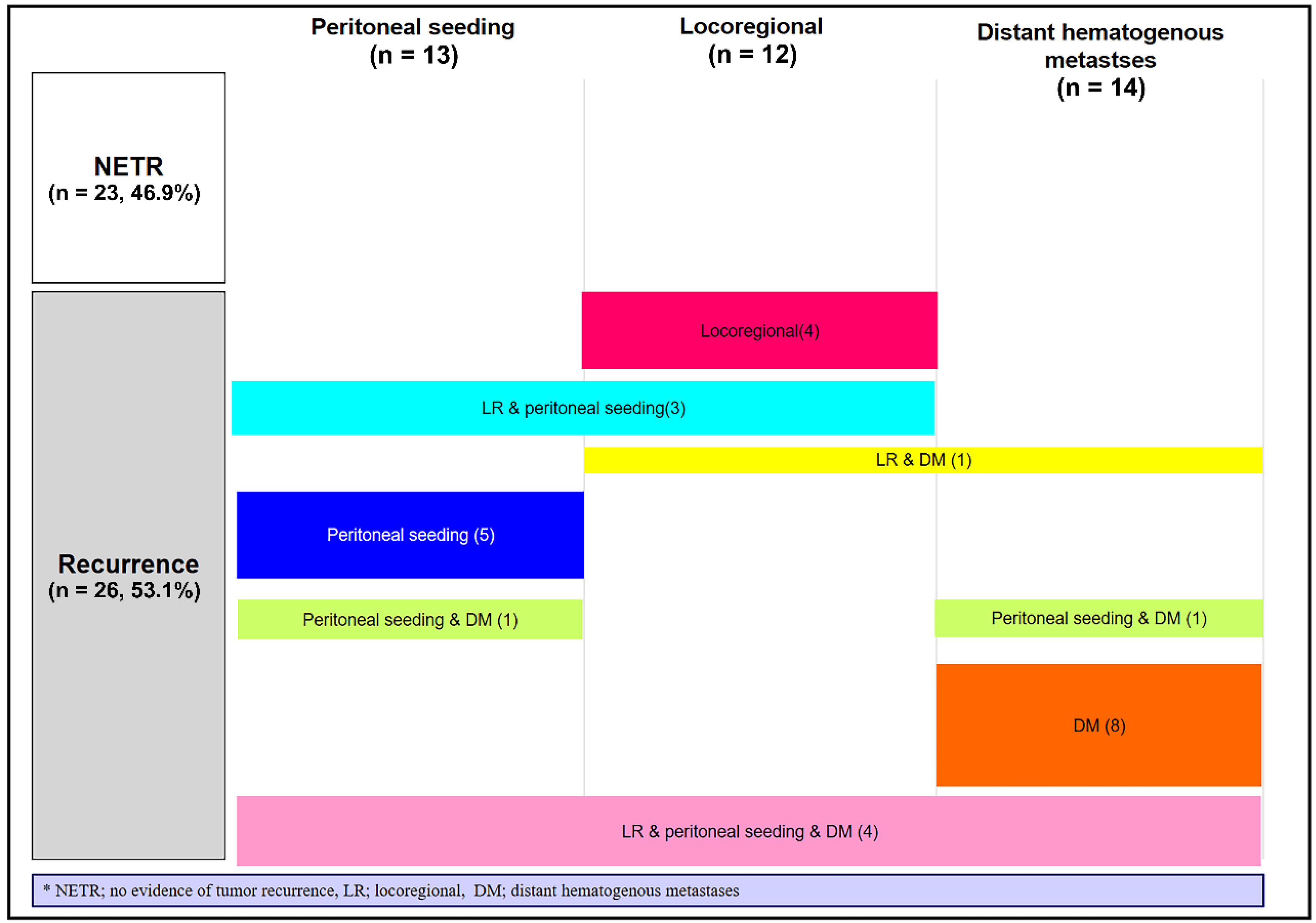
3.3. Treatment Response and Patterns of Failure
3.4. Treatment-Related Gastroduodenal Toxicity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.J.; Won, Y.-J.; Lee, J.J.; Jung, K.-W.; Kim, H.-J.; Kong, H.-J.; Im, J.-S.; Seo, H.G. Cancer Statistics in Korea: Incidence, Mortality, Survival, and Prevalence in 2019. Cancer Res. Treat 2022, 54, 330–344. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA A Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef]
- Tempero, M.A.; Malafa, M.P.; Al-Hawary, M.; Behrman, S.W.; Benson, A.B.; Cardin, D.B.; Chiorean, E.G.; Chung, V.; Czito, B.; Del Chiaro, M.; et al. Pancreatic Adenocarcinoma, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. JNCCN 2021, 19, 439–457. [Google Scholar] [CrossRef]
- Jones, R.P.; Psarelli, E.-E.; Jackson, R.; Ghaneh, P.; Halloran, C.M.; Palmer, D.H.; Campbell, F.; Valle, J.W.; Faluyi, O.; O’Reilly, D.A.; et al. Patterns of Recurrence After Resection of Pancreatic Ductal Adenocarcinoma: A Secondary Analysis of the ESPAC-4 Randomized Adjuvant Chemotherapy Trial. JAMA Surg. 2019, 154, 1038–1048. [Google Scholar] [CrossRef] [PubMed]
- Blakaj, A.; Stein, S.M.; Khan, S.A.; Johung, K.L. Review and current state of radiation therapy for locally advanced pancreatic adenocarcinoma. J. Gastrointest. Oncol. 2018, 9, 1027–1036. [Google Scholar] [CrossRef] [PubMed]
- Iacobuzio-Donahue, C.A.; Fu, B.; Yachida, S.; Luo, M.; Abe, H.; Henderson, C.M.; Vilardell, F.; Wang, Z.; Keller, J.W.; Banerjee, P.; et al. DPC4 Gene Status of the Primary Carcinoma Correlates with Patterns of Failure in Patients with Pancreatic Cancer. J. Clin. Oncol. 2009, 27, 1806–1813. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, S.; Chang, B.W. New possibilities and potential benefits for local control in locally recurrent pancreatic cancer. J. Gastrointest. Oncol. 2013, 4, 340–342. [Google Scholar]
- Hammel, P.; Huguet, F.; van Laethem, J.-L.; Goldstein, D.; Glimelius, B.; Artru, P.; Borbath, I.; Bouché, O.; Shannon, J.; André, T.; et al. Effect of Chemoradiotherapy vs Chemotherapy on Survival in Patients with Locally Advanced Pancreatic Cancer Controlled After 4 Months of Gemcitabine with or without Erlotinib: The LAP07 Randomized Clinical Trial. JAMA 2016, 315, 1844–1853. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.H.; Lee, W.J.; Woo, S.M.; Kim, H.; Oh, E.S.; Lee, J.H.; Han, S.-S.; Park, S.-J.; Suh, Y.-G.; Moon, S.H.; et al. Effectiveness and Safety of Simultaneous Integrated Boost-Proton Beam Therapy for Localized Pancreatic Cancer. Technol. Cancer Res. Treat. 2018, 17, 1533033818783879. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, S.; Chadha, A.S.; Suh, Y.; Chen, H.C.; Rao, A.; Das, P.; Minsky, B.D.; Mahmood, U.; Delclos, M.E.; Sawakuchi, G.O.; et al. Focal Radiation Therapy Dose Escalation Improves Overall Survival in Locally Advanced Pancreatic Cancer Patients Receiving Induction Chemotherapy and Consolidative Chemoradiation. Int. J. Radiat. Oncol. Biol. Phys. 2016, 94, 755–765. [Google Scholar] [CrossRef] [PubMed]
- Rutenberg, M.S.; Nichols, R.C. Proton beam radiotherapy for pancreas cancer. J. Gastrointest. Oncol. 2019, 11, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Chuong, M.; Badiyan, S.N.; Yam, M.; Li, Z.; Langen, K.; Regine, W.; Morris, C.; Snider Iii, J.; Mehta, M.; Huh, S.; et al. Pencil beam scanning versus passively scattered proton therapy for unresectable pancreatic cancer. J. Gastrointest. Oncol. 2018, 9, 687–693. [Google Scholar] [CrossRef]
- Kobeissi, J.M.; Simone, C.B.; Lin, H.; Hilal, L.; Hajj, C. Proton Therapy in the Management of Pancreatic Cancer. Cancers 2022, 14, 2789. [Google Scholar] [CrossRef] [PubMed]
- Nichols, R.C.; Huh, S.N.; Prado, K.L.; Yi, B.Y.; Sharma, N.K.; Ho, M.W.; Hoppe, B.S.; Mendenhall, N.P.; Li, Z.; Regine, W.F. Protons Offer Reduced Normal-Tissue Exposure for Patients Receiving Postoperative Radiotherapy for Resected Pancreatic Head Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Thompson, R.F.; Mayekar, S.U.; Zhai, H.; Both, S.; Apisarnthanarax, S.; Metz, J.M.; Plastaras, J.P.; Ben-Josef, E. A dosimetric comparison of proton and photon therapy in unresectable cancers of the head of pancreas. Med. Phys. 2014, 41, 081711. [Google Scholar] [CrossRef]
- Verma, V.; Lin, S.H.; Simone Ii, C.B.; Mehta, M.P. Clinical outcomes and toxicities of proton radiotherapy for gastrointestinal neoplasms: A systematic review. J. Gastrointest. Oncol. 2016, 7, 644. [Google Scholar] [CrossRef]
- Zurlo, A.; Lomax, A.; Hoess, A.; Bortfeld, T.; Russo, M.; Goitein, G.; Valentini, V.; Marucci, L.; Capparella, R.; Loasses, A. The role of proton therapy in the treatment of large irradiation volumes: A comparative planning study of pancreatic and biliary tumors. Int. J. Radiat. Oncol. Biol. Phys. 2000, 48, 277–288. [Google Scholar] [CrossRef]
- Brunner, T.B.; Haustermans, K.; Huguet, F.; Morganti, A.G.; Mukherjee, S.; Belka, C.; Krempien, R.; Hawkins, M.A.; Valentini, V.; Roeder, F. ESTRO ACROP guidelines for target volume definition in pancreatic cancer. Radiother. Oncol. 2021, 154, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Yoo, G.S.; Yu, J.I.; Cho, S.; Jung, S.H.; Han, Y.; Park, S.; Oh, Y.; Lee, B.; Park, H.C.; Lim, D.H.; et al. Comparison of clinical outcomes between passive scattering versus pencil-beam scanning proton beam therapy for hepatocellular carcinoma. Radiother. Oncol. 2020, 146, 187–193. [Google Scholar] [CrossRef]
- Ben-Josef, E.; Lawrence, T.S. Radiotherapy: The importance of local control in pancreatic cancer. Nat. Rev. Clin. Oncol. 2011, 9, 9–10. [Google Scholar] [CrossRef] [PubMed]
- Wei, Q.; Yu, W.; Rosati, L.M.; Herman, J.M. Advances of stereotactic body radiotherapy in pancreatic cancer. Chin. J. Cancer Res. 2015, 27, 349–357. [Google Scholar] [PubMed]
- Balaban, E.P.; Mangu, P.B.; Khorana, A.A.; Shah, M.A.; Mukherjee, S.; Crane, C.H.; Javle, M.M.; Eads, J.R.; Allen, P.; Ko, A.H.; et al. Locally Advanced, Unresectable Pancreatic Cancer: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2016, 34, 2654–2668. [Google Scholar] [CrossRef]
- Jung, J.; Yoon, S.M.; Park, J.H.; Seo, D.W.; Lee, S.S.; Kim, M.H.; Lee, S.K.; Park, D.H.; Song, T.J.; Ryoo, B.Y.; et al. Stereotactic body radiation therapy for locally advanced pancreatic cancer. PLoS ONE 2019, 14, e0214970. [Google Scholar] [CrossRef]
- Koong, A.C.; Christofferson, E.; Le, Q.T.; Goodman, K.A.; Ho, A.; Kuo, T.; Ford, J.M.; Fisher, G.A.; Greco, R.; Norton, J.; et al. Phase II study to assess the efficacy of conventionally fractionated radiotherapy followed by a stereotactic radiosurgery boost in patients with locally advanced pancreatic cancer. Int. J. Radiat. Oncol. Biol. Phys. 2005, 63, 320–323. [Google Scholar] [CrossRef] [PubMed]
- Koong, A.C.; Le, Q.T.; Ho, A.; Fong, B.; Fisher, G.; Cho, C.; Ford, J.; Poen, J.; Gibbs, I.C.; Mehta, V.K.; et al. Phase I study of stereotactic radiosurgery in patients with locally advanced pancreatic cancer. Int. J. Radiat. Oncol. Biol. Phys. 2004, 58, 1017–1021. [Google Scholar] [CrossRef]
- Schellenberg, D.; Goodman, K.A.; Lee, F.; Chang, S.; Kuo, T.; Ford, J.M.; Fisher, G.A.; Quon, A.; Desser, T.S.; Norton, J.; et al. Gemcitabine chemotherapy and single-fraction stereotactic body radiotherapy for locally advanced pancreatic cancer. Int. J. Radiat. Oncol. Biol. Phys. 2008, 72, 678–686. [Google Scholar] [CrossRef] [PubMed]
- Schellenberg, D.; Kim, J.; Christman-Skieller, C.; Chun, C.L.; Columbo, L.A.; Ford, J.M.; Fisher, G.A.; Kunz, P.L.; Van Dam, J.; Quon, A.; et al. Single-fraction stereotactic body radiation therapy and sequential gemcitabine for the treatment of locally advanced pancreatic cancer. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 181–188. [Google Scholar] [CrossRef]
- Dell’Oro, M.; Short, M.; Wilson, P.; Bezak, E. Clinical Limitations of Photon, Proton and Carbon Ion Therapy for Pancreatic Cancer. Cancers 2020, 12, 163. [Google Scholar] [CrossRef]
- Mahadevan, A.; Miksad, R.; Goldstein, M.; Sullivan, R.; Bullock, A.; Buchbinder, E.; Pleskow, D.; Sawhney, M.; Kent, T.; Vollmer, C.; et al. Induction gemcitabine and stereotactic body radiotherapy for locally advanced nonmetastatic pancreas cancer. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, e615–e622. [Google Scholar] [CrossRef]
- Kim, T.H.; Lee, W.J.; Woo, S.M.; Oh, E.S.; Youn, S.H.; Jang, H.Y.; Han, S.S.; Park, S.J.; Suh, Y.G.; Moon, S.H.; et al. Efficacy and feasibility of proton beam radiotherapy using the simultaneous integrated boost technique for locally advanced pancreatic cancer. Sci. Rep. 2020, 10, 21712. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.; Myoung Noh, J.; Lee, W.; Park, B.; Park, H.; Young Park, J.; Pyo, H. Proton beam therapy reduces the risk of severe radiation-induced lymphopenia during chemoradiotherapy for locally advanced non-small cell lung cancer: A comparative analysis of proton versus photon therapy. Radiother. Oncol. 2021, 156, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Wild, A.T.; Herman, J.M.; Dholakia, A.S.; Moningi, S.; Lu, Y.; Rosati, L.M.; Hacker-Prietz, A.; Assadi, R.K.; Saeed, A.M.; Pawlik, T.M.; et al. Lymphocyte-Sparing Effect of Stereotactic Body Radiation Therapy in Patients with Unresectable Pancreatic Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2016, 94, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Terashima, K.; Demizu, Y.; Hashimoto, N.; Jin, D.; Mima, M.; Fujii, O.; Niwa, Y.; Takatori, K.; Kitajima, N.; Sirakawa, S.; et al. A phase I/II study of gemcitabine-concurrent proton radiotherapy for locally advanced pancreatic cancer without distant metastasis. Radiother. Oncol. 2012, 103, 25–31. [Google Scholar] [CrossRef]
- Faisal, F.; Tsai, H.-L.; Blackford, A.; Olino, K.; Xia, C.; De Jesus-Acosta, A.; Le, D.T.; Cosgrove, D.; Azad, N.; Rasheed, Z.; et al. Longer Course of Induction Chemotherapy Followed by Chemoradiation Favors Better Survival Outcomes for Patients with Locally Advanced Pancreatic Cancer. Am. J. Clin. Oncol. 2016, 39, 18. [Google Scholar] [CrossRef]
- Chuong, M.D.; Springett, G.M.; Freilich, J.M.; Park, C.K.; Weber, J.M.; Mellon, E.A.; Hodul, P.J.; Malafa, M.P.; Meredith, K.L.; Hoffe, S.E.; et al. Stereotactic body radiation therapy for locally advanced and borderline resectable pancreatic cancer is effective and well tolerated. Int. J. Radiat. Oncol. Biol. Phys. 2013, 86, 516–522. [Google Scholar] [CrossRef]
- Gurka, M.K.; Kim, C.; He, A.R.; Charabaty, A.; Haddad, N.; Turocy, J.; Johnson, L.; Jackson, P.; Weiner, L.M.; Marshall, J.L.; et al. Stereotactic Body Radiation Therapy (SBRT) Combined with Chemotherapy for Unresected Pancreatic Adenocarcinoma. Am. J. Clin. Oncol. 2017, 40, 152. [Google Scholar] [CrossRef]
- Herman, J.M.; Chang, D.T.; Goodman, K.A.; Dholakia, A.S.; Raman, S.P.; Hacker-Prietz, A.; Iacobuzio-Donahue, C.A.; Griffith, M.E.; Pawlik, T.M.; Pai, J.S.; et al. Phase 2 multi-institutional trial evaluating gemcitabine and stereotactic body radiotherapy for patients with locally advanced unresectable pancreatic adenocarcinoma. Cancer 2015, 121, 1128–1137. [Google Scholar] [CrossRef]
- Hoyer, M.; Roed, H.; Sengelov, L.; Traberg, A.; Ohlhuis, L.; Pedersen, J.; Nellemann, H.; Kiil Berthelsen, A.; Eberholst, F.; Engelholm, S.A.; et al. Phase-II study on stereotactic radiotherapy of locally advanced pancreatic carcinoma. Radiother. Oncol. 2005, 76, 48–53. [Google Scholar] [CrossRef]
- Macchia, G.; Morganti, A.G.; Cilla, S.; Ippolito, E.; Massaccesi, M.; Picardi, V.; Mattiucci, G.C.; Bonomo, P.; Tambaro, R.; Pacelli, F.; et al. Quality of life and toxicity of stereotactic radiotherapy in pancreatic tumors: A case series. Cancer Investig. 2012, 30, 149–155. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | N (%) |
|---|---|
| Median age (years, range) | 61 (46–90) |
| Sex | |
| Male | 31 (63.3) |
| Female | 18 (36.7) |
| Tumor stage | |
| T1 | 0 (0) |
| T2 | 2 (4.1) |
| T3 | 9 (18.4) |
| T4 | 38 (77.6) |
| Lymph node metastasis | |
| N0 | 22 (44.9) |
| N1 | 23 (46.9) |
| N2 | 4 (8.2) |
| Distant metastasis | |
| No | 43 (87.8) |
| Yes | 6 (12.2) |
| Primary site | |
| Head | 23 (46.9) |
| Body | 22 (44.9) |
| Tail | 4 (8.2) |
| Resectability | |
| Unresectable | 40 (81.5) |
| Borderline resectable | 5 (10.3) |
| Resectable | 4 (8.2) |
| Pre-SBPT CA19-9 (U/mL, median, range) | 65.40 (3.33–2536.75) |
| Pre-SBPT ALC (103/μL, median, range) | 1.80 (0.81–3.31) |
| Surgery | |
| No | 41 (83.7) |
| Yes | 8 (16.3) |
| Before SBPT | 6 (12.2) |
| After SBPT | 2 (4.1) |
| RT aim | |
| Definitive (no other previous treatment) | 3 (6.1) |
| Consolidation (after induction chemotherapy) | 38 (77.6) |
| Salvage | 8 (16.3) |
| Progression after induction chemotherapy | 3 (6.1) |
| After induction chemotherapy for recurrence | 3 (6.1) |
| Immediate RT after recurrence | 2 (4.1) |
| Induction chemotherapy (n = 44) | |
| FOLFIRINOX | 31 (70.5) |
| gemcitabine/abraxane | 13 (29.5) |
| Interval induction chemotherapy to SBPT (n = 44) | |
| <4 month | 10 (20.4) |
| ≥4 month | 34 (79.6) |
| Induction chemotherapy response (n = 44) | |
| PR | 16 (32.7) |
| SD | 25 (51.0) |
| PD | 3 (6.1) |
| Chemotherapy after SBPT | |
| No | 9 (18.4) |
| Yes | 40 (81.6) |
| FOLFIRINOX | 23 (46.9) |
| gemcitabine/abraxane | 11 (22.4) |
| Others * | 6 (12.2) |
| RT dose schedule | |
| 50 GyRBE in 5 fractions | 7 (14.3) |
| 60 GyRBE in 5 fractions | 42 (85.7) |
| PTV (cc, median, range) | 79.00 (20.50–291.80) |
| No. (%) | Univariable | Multivariable | |||
|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | ||
| Age | 61 (46–90) * | 1.10 (1.01–1.20) | 0.025 | 1.05 (1.01–1.10) | 0.024 |
| Sex | |||||
| Male | 31 (63.3) | Reference | 0.523 | ||
| Female | 18 (36.7) | 0.59 (0.12–2.94) | |||
| T stage | |||||
| T1–3 | 11 (22.4) | Reference | 0.655 | ||
| T4 | 38 (77.6) | 1.63 (0.19–14.04) | |||
| Lymph node metastases | |||||
| No | 22 (44.9) | Reference | 0.804 | ||
| Yes | 27 (55.1) | 1.22 (0.24–6.13) | |||
| Distant metastases | |||||
| No | 43 (87.8) | Reference | 0.632 | ||
| Yes | 6 (12.2) | 0.04 (0.0–22.061.28) | |||
| Primary site | |||||
| Head | 23 (46.9) | Reference | 0.546 | ||
| Body/Tail | 26 (53.1) | 0.61 (0.12–3.02) | |||
| Induction CT | |||||
| No | 5 (10.2) | Reference | 0.375 | ||
| Yes | 44 (89.8) | 0.04 (0.04–3.32) | |||
| Induction CT regimen | |||||
| FOLFIRINOX | 31 (63.3) | Reference | 0.838 | ||
| gemcitabine/abraxane | 13 (26.5) | 0.00 (0.00–4.199 E) | 0.972 | ||
| No | 5 (10.2) | 1.94 (0.21–17.50) | 0.553 | ||
| CT to RT interval | |||||
| <4 month | 10 (20.4) | Reference | 0.793 | ||
| ≥4 month | 34 (79.6) | 1.34 (0.14–12.30) | |||
| Induction CT response | |||||
| PR | 16 (32.7) | Reference | 0.661 | ||
| SD | 25 (51.0) | 161,339 (0–1.438 E) | 0.960 | ||
| PD | 3 (6.1) | 446,977 (0–3.999 E) | 0.957 | ||
| After CT | |||||
| No | 9 (18.4) | Reference | 0.172 | Reference 3.38 (1.00–11.41) | 0.050 |
| Yes | 40 (81.6) | 0.28 (0.04–1.72) | |||
| After CT regimen | |||||
| FOLFIRINOX | 23 (46.9) | Reference | 0.089 | Reference 2.19 (0.91–5.26) | 0.079 |
| Others/No | 26 (53.1) | 1.99 (0.90–4.41) | |||
| Pre- SBPT CA19-9 | |||||
| <60 U/mL | 24 (49.0) | Reference | 0.112 | Reference 2.06 (0.86–4.87) | 0.101 |
| ≥60 U/mL | 25 (51.0) | 5.71 (0.66–48.89) | |||
| Pre-SBPT ALC (103/μL) | 1.80 (0.81–3.31) * | 1.84 (0.37–9.13) | 0.455 | ||
| No. (%) | Univariable | Multivariable | |||
|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | ||
| Age | 61 (46–90) * | 0.96 (0.88–1.05) | 0.435 | ||
| Sex | |||||
| Male | 31 (63.3) | Reference | 0.219 | ||
| Female | 18 (36.7) | 38.79 (0.11–13,265.15) | |||
| T stage | |||||
| T1–3 | 11 (22.4) | Reference | 0.371 | ||
| T4 | 38 (77.6) | 2.58 (0.32–20.67) | |||
| Lymph node metastases | |||||
| No | 22 (44.9) | Reference | 0.488 | ||
| Yes | 27 (55.1) | 1.60 (0.42–6.06) | |||
| Distant metastases | |||||
| No | 43 (87.8) | Reference | 0.770 | ||
| Yes | 6 (12.2) | 1.36 (0.16–11.24) | |||
| Primary site | |||||
| Head | 23 (46.9) | Reference | 0.049 | Reference | 0.074 |
| Body/Tail | 26 (53.1) | 0.24 (0.05–0.99) | 0.27 (0.06–1.14) | ||
| Induction CT | |||||
| No | 5 (10.2) | Reference | 0.592 | ||
| Yes | 44 (89.8) | 23.11 (0.00–2,212,943.9) | |||
| Induction CT regimen | |||||
| FOLFIRINOX | 31 (63.3) | Reference | 0.989 | ||
| gemcitabine/abraxane | 13 (26.5) | 1.11 (0.27–4.47) | 0.881 | ||
| No | 5 (10.2) | 0.00 (0.00) | 0.988 | ||
| CT to RT interval | |||||
| <4 month | 10 (20.4) | Reference | 0.173 | Reference | 0.296 |
| ≥4 month | 34 (79.6) | 0.40 (0.11–1.49) | 0.49 (0.12–1.86) | ||
| Induction CT response | |||||
| PR | 16 (32.7) | Reference | 0.962 | ||
| SD | 25 (51.0) | 1.21 (0.30–4.86) | 0.782 | ||
| PD | 3 (6.1) | 0.00 (0.0) | 0.991 | ||
| After CT | |||||
| No | 9 (18.4) | Reference | 0.748 | ||
| Yes | 40 (81.6) | 1.41 (0.17–11.42) | |||
| After CT regimen | |||||
| FOLFIRINOX | 23 (46.9) | Reference | 0.331 | ||
| Others/No | 26 (53.1) | 1.99 (−0.69–2.07) | |||
| Pre-SBPT CA19-9 | |||||
| <60 U/mL | 24 (49.0) | Reference | 0.436 | ||
| ≥60 U/mL | 25 (51.0) | 1.73 (0.43–6.94) | |||
| Pre-SBPT ALC (103/μL) | 1.80 (0.81–3.31) * | 0.49 (0.15–1.58) | 0.235 | ||
| No. (%) | Univariable | Multivariable | |||
|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | ||
| Age | 61 (46–90) * | 1.05 (1.01–1.10) | 0.023 | 1.05 (1.01–1.10) | 0.023 |
| Sex | |||||
| Male | 31 (63.3) | Reference | 0.919 | ||
| Female | 18 (36.7) | 1.04 (0.46–2.34) | |||
| T stage | |||||
| T1–3 | 11 (22.4) | Reference | 0.776 | ||
| T4 | 38 (77.6) | 0.88 (0.36–2.11) | |||
| Lymph node metastases | |||||
| No | 22 (44.9) | Reference | 0.331 | ||
| Yes | 27 (55.1) | 1.47 (0.67–3.23) | |||
| Distant metastases | |||||
| No | 43 (87.8) | Reference | 0.637 | ||
| Yes | 6 (12.2) | 1.35 (0.39–4.61) | |||
| Primary site | |||||
| Head | 23 (46.9) | Reference | 0.088 | ||
| Body/Tail | 26 (53.1) | 0.51 (0.23–1.10) | |||
| Induction CT | |||||
| No | 5 (10.2) | Reference | 0.590 | ||
| Yes | 44 (89.8) | 0.71 (0.21–2.41) | |||
| Induction CT regimen | |||||
| FOLFIRINOX | 31 (63.3) | Reference | 0.817 | ||
| gemcitabine/abraxane | 13 (26.5) | 1.16 (0.48–2.84) | 0.732 | ||
| No | 5 (10.2) | 1.45 (0.42–5.03) | 0.551 | ||
| CT to RT interval | |||||
| <4 month | 10 (20.4) | Reference | 0.379 | ||
| ≥4 month | 34 (79.6) | 1634 (0.54–4.83) | |||
| Induction CT response | |||||
| PR | 16 (32.7) | Reference | 0.357 | ||
| SD | 25 (51.0) | 1.99 (0.77–5.15) | 0.155 | ||
| PD | 3 (6.1) | 1.87 (0.37–9.34) | 0.443 | ||
| After CT | |||||
| No | 9 (18.4) | Reference | 0.726 | ||
| Yes | 40 (81.6) | 1.21 (0.41–3.51) | |||
| After CT regimen | |||||
| FOLFIRINOX | 23 (46.9) | Reference | 0.086 | ||
| Others/No | 26 (53.1) | 6.59 (0.77–56.60) | |||
| Pre-SBPT CA19-9 | |||||
| <60 U/mL | 24 (49.0) | Reference | 0.067 | ||
| ≥60 U/mL | 25 (51.0) | 2.13 (0.94–4.79) | |||
| Pre-SBPT ALC (103/μL) | 1.80 (0.81–3.31) * | 0.81 (0.41–1.60) | 0.556 | ||
| Parameter | Cut off Value of EQD2 | HR | 95% CI | p |
|---|---|---|---|---|
| Dmax | ≥57.000 GyRBE | 2.11 | 0.41–10.98 | 0.373 |
| D5cc | ≥10.028 GyRBE | 2.44 | 0.58–10.37 | 0.225 |
| D10cc | ≥5.990 GyRBE | 2.16 | 0.50–9.22 | 0.296 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, H.; Yu, J.I.; Park, H.C.; Yoo, G.S.; Cho, S.; Park, J.O.; Lee, K.T.; Lee, K.H.; Lee, J.K.; Park, J.K.; et al. The Feasibility of Stereotactic Body Proton Beam Therapy for Pancreatic Cancer. Cancers 2022, 14, 4556. https://doi.org/10.3390/cancers14194556
Shin H, Yu JI, Park HC, Yoo GS, Cho S, Park JO, Lee KT, Lee KH, Lee JK, Park JK, et al. The Feasibility of Stereotactic Body Proton Beam Therapy for Pancreatic Cancer. Cancers. 2022; 14(19):4556. https://doi.org/10.3390/cancers14194556
Chicago/Turabian StyleShin, Hyunju, Jeong Il Yu, Hee Chul Park, Gyu Sang Yoo, Sungkoo Cho, Joon Oh Park, Kyu Taek Lee, Kwang Hyuck Lee, Jong Kyun Lee, Joo Kyung Park, and et al. 2022. "The Feasibility of Stereotactic Body Proton Beam Therapy for Pancreatic Cancer" Cancers 14, no. 19: 4556. https://doi.org/10.3390/cancers14194556
APA StyleShin, H., Yu, J. I., Park, H. C., Yoo, G. S., Cho, S., Park, J. O., Lee, K. T., Lee, K. H., Lee, J. K., Park, J. K., Heo, J. S., Han, I. W., & Shin, S. H. (2022). The Feasibility of Stereotactic Body Proton Beam Therapy for Pancreatic Cancer. Cancers, 14(19), 4556. https://doi.org/10.3390/cancers14194556