



Proton Beam Therapy for Treatment-Naïve Hepatocellular Carcinoma and Prognostic Significance of Albumin-Bilirubin (ALBI) Grade
 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Treatment
2.3. Assessments and Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Trevisani, F.; Cantarini, M.C.; Wands, J.R.; Bernardi, M. Recent advances in the natural history of hepatocellular carcinoma. Carcinogenesis 2008, 29, 1299–1305. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed]
- Korean Liver Cancer, A.; National Cancer, C. 2018 Korean Liver Cancer Association-National Cancer Center Korea Practice Guidelines for the Management of Hepatocellular Carcinoma. Gut Liver 2019, 13, 227–299. [Google Scholar] [CrossRef]
- Kudo, M.; Kawamura, Y.; Hasegawa, K.; Tateishi, R.; Kariyama, K.; Shiina, S.; Toyoda, H.; Imai, Y.; Hiraoka, A.; Ikeda, M.; et al. Management of Hepatocellular Carcinoma in Japan: JSH Consensus Statements and Recommendations 2021 Update. Liver Cancer 2021, 10, 181–223. [Google Scholar] [CrossRef] [PubMed]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef]
- Omata, M.; Cheng, A.L.; Kokudo, N.; Kudo, M.; Lee, J.M.; Jia, J.; Tateishi, R.; Han, K.H.; Chawla, Y.K.; Shiina, S.; et al. Asia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: A 2017 update. Hepatol. Int. 2017, 11, 317–370. [Google Scholar] [CrossRef]
- Bush, D.A.; Kayali, Z.; Grove, R.; Slater, J.D. The safety and efficacy of high-dose proton beam radiotherapy for hepatocellular carcinoma: A phase 2 prospective trial. Cancer 2011, 117, 3053–3059. [Google Scholar] [CrossRef]
- Bush, D.A.; Smith, J.C.; Slater, J.D.; Volk, M.L.; Reeves, M.E.; Cheng, J.; Grove, R.; de Vera, M.E. Randomized Clinical Trial Comparing Proton Beam Radiation Therapy with Transarterial Chemoembolization for Hepatocellular Carcinoma: Results of an Interim Analysis. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 477–482. [Google Scholar] [CrossRef]
- Fukuda, K.; Okumura, T.; Abei, M.; Fukumitsu, N.; Ishige, K.; Mizumoto, M.; Hasegawa, N.; Numajiri, H.; Ohnishi, K.; Ishikawa, H.; et al. Long-term outcomes of proton beam therapy in patients with previously untreated hepatocellular carcinoma. Cancer Sci. 2017, 108, 497–503. [Google Scholar] [CrossRef]
- Fukumitsu, N.; Sugahara, S.; Nakayama, H.; Fukuda, K.; Mizumoto, M.; Abei, M.; Shoda, J.; Thono, E.; Tsuboi, K.; Tokuuye, K. A prospective study of hypofractionated proton beam therapy for patients with hepatocellular carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2009, 74, 831–836. [Google Scholar] [CrossRef]
- Hong, T.S.; Wo, J.Y.; Yeap, B.Y.; Ben-Josef, E.; McDonnell, E.I.; Blaszkowsky, L.S.; Kwak, E.L.; Allen, J.N.; Clark, J.W.; Goyal, L.; et al. Multi-Institutional Phase II Study of High-Dose Hypofractionated Proton Beam Therapy in Patients with Localized, Unresectable Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma. J. Clin. Oncol. 2016, 34, 460–468. [Google Scholar] [CrossRef] [PubMed]
- Kawashima, M.; Furuse, J.; Nishio, T.; Konishi, M.; Ishii, H.; Kinoshita, T.; Nagase, M.; Nihei, K.; Ogino, T. Phase II study of radiotherapy employing proton beam for hepatocellular carcinoma. J. Clin. Oncol. 2005, 23, 1839–1846. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.H.; Park, J.W.; Kim, B.H.; Kim, H.; Moon, S.H.; Kim, S.S.; Woo, S.M.; Koh, Y.H.; Lee, W.J.; Kim, D.Y.; et al. Does Risk-Adapted Proton Beam Therapy Have a Role as a Complementary or Alternative Therapeutic Option for Hepatocellular Carcinoma? Cancers 2019, 11, 230. [Google Scholar] [CrossRef]
- Kim, T.H.; Park, J.W.; Kim, B.H.; Oh, E.S.; Youn, S.H.; Moon, S.H.; Kim, S.S.; Woo, S.M.; Koh, Y.H.; Lee, W.J.; et al. Phase II Study of Hypofractionated Proton Beam Therapy for Hepatocellular Carcinoma. Front. Oncol. 2020, 10, 542. [Google Scholar] [CrossRef]
- Kim, T.H.; Park, J.W.; Kim, Y.J.; Kim, B.H.; Woo, S.M.; Moon, S.H.; Kim, S.S.; Koh, Y.H.; Lee, W.J.; Park, S.J.; et al. Phase I dose-escalation study of proton beam therapy for inoperable hepatocellular carcinoma. Cancer Res. Treat. 2015, 47, 34–45. [Google Scholar] [CrossRef]
- Kim, T.H.; Koh, Y.H.; Kim, B.H.; Kim, M.J.; Lee, J.H.; Park, B.; Park, J.W. Proton beam radiotherapy vs. radiofrequency ablation for recurrent hepatocellular carcinoma: A randomized phase III trial. J. Hepatol. 2021, 74, 603–612. [Google Scholar] [CrossRef]
- Child, C.G.; Turcotte, J.G. Surgery and portal hypertension. Major Probl. Clin. Surg. 1964, 1, 1–85. [Google Scholar]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef]
- Amin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K. AJCC Cancer Staging Manual, 8th ed.; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar]
- Kim, D.Y.; Park, J.W.; Kim, T.H.; Kim, B.H.; Moon, S.H.; Kim, S.S.; Woo, S.M.; Koh, Y.H.; Lee, W.J.; Kim, C.M. Risk-adapted simultaneous integrated boost-proton beam therapy (SIB-PBT) for advanced hepatocellular carcinoma with tumour vascular thrombosis. Radiother. Oncol. 2017, 122, 122–129. [Google Scholar] [CrossRef]
- Lee, S.U.; Park, J.W.; Kim, T.H.; Kim, Y.J.; Woo, S.M.; Koh, Y.H.; Lee, W.J.; Park, S.J.; Kim, D.Y.; Kim, C.M. Effectiveness and safety of proton beam therapy for advanced hepatocellular carcinoma with portal vein tumor thrombosis. Strahlenther. Oncol. 2014, 190, 806–814. [Google Scholar] [CrossRef]
- Fowler, J.F. The linear-quadratic formula and progress in fractionated radiotherapy. Br. J. Radiol. 1989, 62, 679–694. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Lencioni, R.; de Baere, T.; Soulen, M.C.; Rilling, W.S.; Geschwind, J.F. Lipiodol transarterial chemoembolization for hepatocellular carcinoma: A systematic review of efficacy and safety data. Hepatology 2016, 64, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.I.; Cho, Y.; Ki, M.; Kim, B.H.; Lee, I.J.; Kim, T.H.; Kim, S.H.; Koh, Y.H.; Kim, H.B.; Hong, E.K.; et al. Better survival of patients with hepatitis B virus-related hepatocellular carcinoma in South Korea: Changes in 16-years cohorts. PLoS ONE 2022, 17, e0265668. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Cheng, A.L.; Meinhardt, G.; Nakajima, K.; De Sanctis, Y.; Llovet, J. Prognostic factors and predictors of sorafenib benefit in patients with hepatocellular carcinoma: Analysis of two phase III studies. J. Hepatol. 2017, 67, 999–1008. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Bustamante, J.; Castells, A.; Vilana, R.; Ayuso Mdel, C.; Sala, M.; Bru, C.; Rodes, J.; Bruix, J. Natural history of untreated nonsurgical hepatocellular carcinoma: Rationale for the design and evaluation of therapeutic trials. Hepatology 1999, 29, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Cabibbo, G.; Enea, M.; Attanasio, M.; Bruix, J.; Craxi, A.; Camma, C. A meta-analysis of survival rates of untreated patients in randomized clinical trials of hepatocellular carcinoma. Hepatology 2010, 51, 1274–1283. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.L.; Kang, Y.K.; Chen, Z.; Tsao, C.J.; Qin, S.; Kim, J.S.; Luo, R.; Feng, J.; Ye, S.; Yang, T.S.; et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009, 10, 25–34. [Google Scholar] [CrossRef]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef]
- Cheng, A.L.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Lim, H.Y.; Kudo, M.; Breder, V.; Merle, P.; et al. Updated efficacy and safety data from IMbrave150: Atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J. Hepatol. 2022, 76, 862–873. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Yoon, S.M.; Ryoo, B.Y.; Lee, S.J.; Kim, J.H.; Shin, J.H.; An, J.H.; Lee, H.C.; Lim, Y.S. Efficacy and Safety of Transarterial Chemoembolization Plus External Beam Radiotherapy vs Sorafenib in Hepatocellular Carcinoma with Macroscopic Vascular Invasion: A Randomized Clinical Trial. JAMA Oncol. 2018, 4, 661–669. [Google Scholar] [CrossRef]
- Sugahara, S.; Nakayama, H.; Fukuda, K.; Mizumoto, M.; Tokita, M.; Abei, M.; Shoda, J.; Matsuzaki, Y.; Thono, E.; Tsuboi, K.; et al. Proton-beam therapy for hepatocellular carcinoma associated with portal vein tumor thrombosis. Strahlenther. Onkol. 2009, 185, 782–788. [Google Scholar] [CrossRef]
- Hiraoka, A.; Michitaka, K.; Kumada, T.; Izumi, N.; Kadoya, M.; Kokudo, N.; Kubo, S.; Matsuyama, Y.; Nakashima, O.; Sakamoto, M.; et al. Validation and Potential of Albumin-Bilirubin Grade and Prognostication in a Nationwide Survey of 46,681 Hepatocellular Carcinoma Patients in Japan: The Need for a More Detailed Evaluation of Hepatic Function. Liver Cancer 2017, 6, 325–336. [Google Scholar] [CrossRef]
- Murray, L.J.; Sykes, J.; Brierley, J.; Kim, J.J.; Wong, R.K.S.; Ringash, J.; Craig, T.; Velec, M.; Lindsay, P.; Knox, J.J.; et al. Baseline Albumin-Bilirubin (ALBI) Score in Western Patients with Hepatocellular Carcinoma Treated with Stereotactic Body Radiation Therapy (SBRT). Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 900–909. [Google Scholar] [CrossRef]
- Su, T.S.; Yang, H.M.; Zhou, Y.; Huang, Y.; Liang, P.; Cheng, T.; Chen, L.; Li, L.Q.; Liang, S.X. Albumin–bilirubin (ALBI) versus Child-Turcotte-Pugh (CTP) in prognosis of HCC after stereotactic body radiation therapy. Radiat. Oncol. 2019, 14, 50. [Google Scholar] [CrossRef]
- Toesca, D.A.S.; Osmundson, E.C.; von Eyben, R.; Shaffer, J.L.; Koong, A.C.; Chang, D.T. Assessment of hepatic function decline after stereotactic body radiation therapy for primary liver cancer. Pract. Radiat. Oncol. 2017, 7, 173–182. [Google Scholar] [CrossRef]
- Cho, I.J.; Jeong, J.U.; Nam, T.K.; Joo, Y.E.; Cho, S.B.; Kim, Y.H.; Song, J.Y.; Yoon, M.S.; Ahn, S.J.; Chung, W.K. PIVKA-II as a surrogate marker for prognosis in patients with localized hepatocellular carcinoma receiving stereotactic body radiotherapy. Radiat. Oncol. J. 2022, 40, 20–28. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristics | n (%) | |
|---|---|---|
| Sex | Male | 35 (76.1) |
| Female | 11 (23.9) | |
| Age, years | Median (range) | 62 (44–81) |
| <65 | 27 (58.7) | |
| ≥65 | 19 (41.3) | |
| ECOG PS | 0 | 44 (95.7) |
| 1 | 2 (4.3) | |
| Etiology of LC | HBV | 29 (63.0) |
| HCV | 6 (13.1) | |
| Alcoholic | 4 (8.7) | |
| Unknown | 7 (15.2) | |
| Child–Pugh score | 5 | 41 (89.1) |
| 6 | 4 (8.7) | |
| 7 | 1 (2.2) | |
| AFP, ng/mL | Median (range) | 10.8 (1.3–294,089.0) |
| <10 | 22 (47.8) | |
| ≥10 | 24 (52.2) | |
| Tumor size, cm | Median (range) | 2.6 (1.0–16.0) |
| ≤3 | 26 (56.5) | |
| >3 | 20 (43.5) | |
| Tumor location | Hilar | 19 (41.3) |
| Non-hilar | 27 (58.7) | |
| Vascular invasion | No | 40 (87.0) |
| Non-major | 1 (2.2) | |
| Major | 5 (10.8) | |
| AJCC stage | I | 37 (80.4) |
| II | 3 (6.5) | |
| III | 5 (10.9) | |
| IV | 1 (2.2) | |
| BCLC stage | 0 | 1 (2.2) |
| A | 36 (78.3) | |
| B | 2 (4,3) | |
| C | 7 (15.2) | |
| Albumin (g/dL) | Median (range) | 42.2 (31–51) |
| Total bilirubin (μmol/L) | Median (range) | 70.0 (35.4–168.0) |
| ALBI score | Median (range) | −2.36 (−3.14–−1.17) |
| ALBI grade | 1 (≤−2.60) | 11 (23.9) |
| 2 (−2.60< and ≥−1.39) | 34 (73.9) | |
| 3 (>−1.39) | 1 (2.2) | |
| Post-Tx | No | 41 (89.1) |
| Yes | 5 (10.9) | |
| Sorafenib | 4 (8.7) | |
| AP | 1 (2.2) | |
| Total dose (EQD2, GyE10) | Median (range) | 95.8 (62.5–102.1) |
| ≤90 | 7 (15.2) | |
| >90 | 39 (84.8) | |
| Planning target volume, cm3 | Median (range) | 20.8 (8.0–627.0) |
| Total liver (TL) volume, mL | Median (range) | 1177.3 (645.8–3211.0) |
| TLV27GyE, % | Median (range) | 12.5 (3.8–65.3) |
| Remaining residual liver (RRL) volume, cm3 | Median (range) | 1049.4 (593.9–2032.4) |
| RRLV27GyE, % | Median (range) | 10.2 (3.0–36.8) |
| StomachD2cc, GyE | Median (range) | 0.0 (0.0–34.0) |
| EsophagusD2cc, GyE | Median (range) | 0.0 (0.0–39.1) |
| DuodenumD2cc, GyE | Median (range) | 0.0 (0.0–34.4) |
| BowelD2cc, GyE | Median (range) | 0.0 (0.0–17.5) |
| CordD2cc, GyE | Median (range) | 0.0 (0.0–34.5) |
| FFLP | PFS | OS | ||||||
|---|---|---|---|---|---|---|---|---|
| Characteristics | N | 5 Year (95% CI), % | p Value * | 5 Year (95% CI), % | p Value * | 5 Year (95% CI), % | p Value * | |
| Sex | Male | 35 | 93.4 (84.5–102.2) | 0.738 | 37.5 (7.4–67.6) | 0.412 | 65.8 (49.2–82.5) | 0.360 |
| Female | 11 | 90.0 (71.4–108.6) | 63.6 (47.7–79.5) | 80.8 (56.9–104.7) | ||||
| Age, years | <65 | 27 | 91.8 (80.8–102.8) | 0.813 | 43.3 (24.3–62.3) | 0.927 | 68.3 (49.7–86.9) | 0.679 |
| ≥65 | 19 | 93.8 (81.8–105.8) | 46.3 (23.4–69.2) | 72.4 (51.6–93.2) | ||||
| Etiology of LC | HBV | 29 | 92.4 (82.2–102.6) | 0.952 | 46.9 (28.3–65.5) | 0.521 | 73.9 (56.8–91.0) | 0.117 |
| Others | 17 | 92.9 (79.4–106.4) | 35.3 (8.6–62.0) | 59.0 (32.3–85.7) | ||||
| Child–Pugh score | 5 | 41 | 91.9 (83.1–100.7) | 0.563 | 47.1 (31.2–63.0) | 0.289 | 73.5 (59.0–88.0) | 0.092 |
| 6–7 | 5 | 100 (–) † | 0.0 (–) † | 30.0 (−16.8–76.8) † | ||||
| AFP, ng/mL | <10 | 22 | 89.5 (75.8–103.2) | 0.507 | 32.1 (10.9–53.3) | 0.507 | 56.7 (32.0–81.4) | 0.119 |
| ≥10 | 24 | 95.7 (87.3–104.1) | 53.6 (33.4–73.8) | 79.2 (62.9–95.5) | ||||
| Tumor size, cm | <3 | 26 | 92.7 (82.7–102.5) | 0.947 | 56.3 (37.7–74.9) | 0.078 | 84.9 (71.2–98.6) | 0.030 |
| ≥3 | 20 | 93.3 (77.7–109.0) | 23.3 (3.1–43.5) | 45.8 (20.9–70.7) | ||||
| Tumor location | Hilar | 19 | 87.4 (70.9–103.9) | 0.261 | 36.1 (14.1–58.1) | 0.333 | 57.4 (34.9–79.9) | 0.155 |
| Non-hilar | 27 | 96.0 (88.4–103.6) | 48.3 (28.1–68.5) | 76.7 (57.9–95.5) | ||||
| Vascular invasion | No/Non-major | 41 | 94.7 (87.4–102.0) | 0.022 | 46.0 (29.9–62.1) | 0.043 | 75.1 (60.6–89.6) | 0.011 |
| Major | 5 | 66.7 (13.4–120.0) | 20.0 (−15.1–55.1) | 20.0 (−15.1–55.1) | ||||
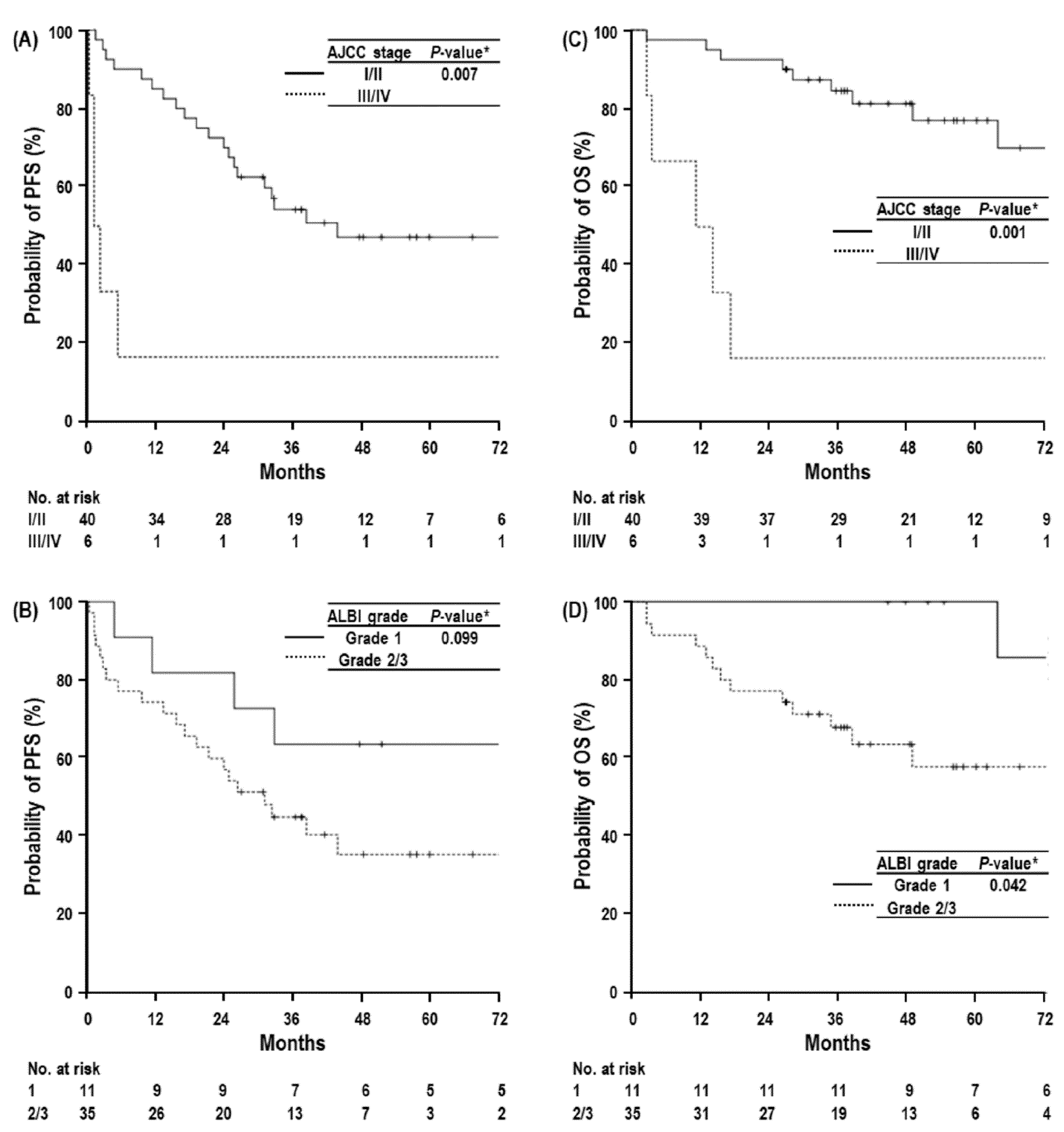
| AJCC stage | I/II | 40 | 94.7 (87.5–102.0) | 0.037 | 47.2 (30.7–63.7) | 0.007 | 77.0 (62.5–91.5) | 0.001 |
| III/IV | 6 | 75.0 (32.5–117.5) | 16.7 (−13.1–46.5) | 16.7 (−13.1–46.5) | ||||
| BCLC stage | 0/A/B | 39 | 94.5 (87.1–102.0) | 0.110 | 46.5 (30.0–63.0) | 0.053 | 76.7 (58.1–95.3) | 0.004 |
| C | 7 | 80.0 (44.9–115.1) | 28.6 (−4.9–62.1) | 28.6 (−4.9–62.1) | ||||
| ALBI grade | 1 | 11 | 100 (–) | 0.284 | 63.6 (35.2–92.0) | 0.099 | 85.7 (59.8–111.6) | 0.042 |
| 2/3 | 35 | 89.9 (79.1–100.7) | 35.4 (17.8–53.0) | 57.8 (39.0–76.6) | ||||
| Total dose | ≤90 | 7 | 83.3 (53.5–113.1) | 0.203 | 14.3 (−11.6–40.2) | 0.037 | 14.3 (−11.6–40.2) | 0.004 |
| (EQD2, GyE10) | >90 | 39 | 94.4 (86.8–102.0) | 48.4 (31.7–65.1) | 76.3 (61.4–91.2) |
| FFLP | PFS | OS | |||||
|---|---|---|---|---|---|---|---|
| Characteristics | Hazard Ratio (95% CI) | p Value * | Hazard Ratio (95% CI) | p Value * | Hazard Ratio (95% CI) | p Value * | |
| AJCC stage | I/II | - | - | 1.000 | 0.002 | 1.000 | 0.001 |
| III/IV | - | 0.162 (0.051–0.511) | 0.101 (0.027–0.384) | ||||
| ALBI grade | 1 | - | - | 1.000 | 0.030 | 1.000 | 0.035 |
| 2/3 | - | 0.282 (0.090–0.882) | 0.098 (0.011–0.847) |
| All Patients (n = 46) | ALBI Grade | ||||||
|---|---|---|---|---|---|---|---|
| CTCAE Grade | Grade 1, n (%) | Grade 2, n (%) | Grade 3, n (%) | Grade 4, n (%) | 1, n (%) | 2/3, n (%) | p Value * |
| Hematologic AEs | 18 (39.1) | 2 (4.3) | 0 (0.0) | 0 (0.0) | 6 (54.5) | 14 (40.0) | 0.494 |
| WBC increase | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |||
| WBC decrease | 5 (10.9) | 2 (4.3) | 0 (0.0) | 0 (0.0)) | |||
| PLT decrease | 7 (15.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |||
| ALT/AST increase | 10 (21.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |||
| Albumin decrease | 1 (2.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |||
| Bilirubin increase | 1 (2.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |||
| Non-hematologic AEs | 16 (38.4) | 2 (4.3) | 0 (0.0) | 0 (0.0) | 4 (36.4) | 14 (40.0) | 1.000 |
| Fever | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |||
| Pain | 1 (2.2) | 1 (2.2) | 0 (0.0) | 0 (0.0) | |||
| Nausea | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |||
| Bleeding | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |||
| Dermatitis | 11 (23.9) | 2 (4.3) | 0 (0.0) | 0 (0.0) | |||
| Radiation pneumonitis | 7 (15.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |||
| Upper gastrointestinal ulcer | 2 (4.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, T.H.; Kim, B.H.; Park, J.-W.; Cho, Y.R.; Koh, Y.-H.; Chun, J.W.; Oh, E.S.; Lee, D.Y.; Lee, S.U.; Suh, Y.-G.; et al. Proton Beam Therapy for Treatment-Naïve Hepatocellular Carcinoma and Prognostic Significance of Albumin-Bilirubin (ALBI) Grade. Cancers 2022, 14, 4445. https://doi.org/10.3390/cancers14184445
Kim TH, Kim BH, Park J-W, Cho YR, Koh Y-H, Chun JW, Oh ES, Lee DY, Lee SU, Suh Y-G, et al. Proton Beam Therapy for Treatment-Naïve Hepatocellular Carcinoma and Prognostic Significance of Albumin-Bilirubin (ALBI) Grade. Cancers. 2022; 14(18):4445. https://doi.org/10.3390/cancers14184445
Chicago/Turabian StyleKim, Tae Hyun, Bo Hyun Kim, Joong-Won Park, Yu Ri Cho, Young-Hwan Koh, Jung Won Chun, Eun Sang Oh, Do Yeul Lee, Sung Uk Lee, Yang-Gun Suh, and et al. 2022. "Proton Beam Therapy for Treatment-Naïve Hepatocellular Carcinoma and Prognostic Significance of Albumin-Bilirubin (ALBI) Grade" Cancers 14, no. 18: 4445. https://doi.org/10.3390/cancers14184445
APA StyleKim, T. H., Kim, B. H., Park, J.-W., Cho, Y. R., Koh, Y.-H., Chun, J. W., Oh, E. S., Lee, D. Y., Lee, S. U., Suh, Y.-G., Woo, S. M., Moon, S. H., Kim, S. S., & Lee, W. J. (2022). Proton Beam Therapy for Treatment-Naïve Hepatocellular Carcinoma and Prognostic Significance of Albumin-Bilirubin (ALBI) Grade. Cancers, 14(18), 4445. https://doi.org/10.3390/cancers14184445