
Endometrial Cancer Detection Using a Cervical DNA Methylation Assay (MPap) in Women with Abnormal Uterine Bleeding: A Multicenter Hospital-Based Validation Study

 , , , ,
, , , ,  , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
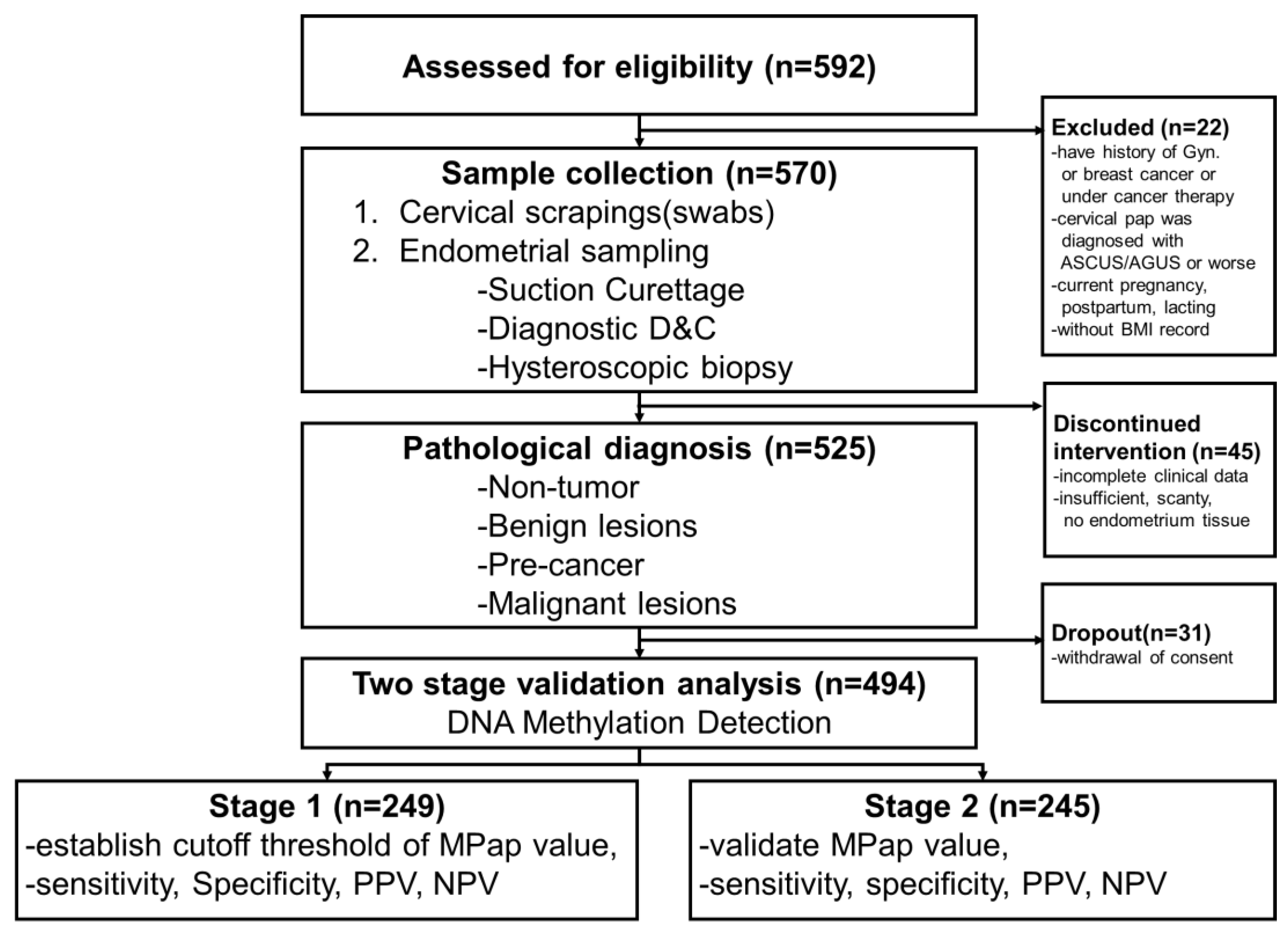
2.1. Study Design
2.2. Patients and Samples
2.3. Data Collection
2.4. Specimen Processing (DNA Extraction, Bisulfite Conversion, and Quantitative Methylation-Specific PCR)
2.5. The Frequency of Diagnosing EC among IVPs from the Taiwan Cancer Registry Database
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
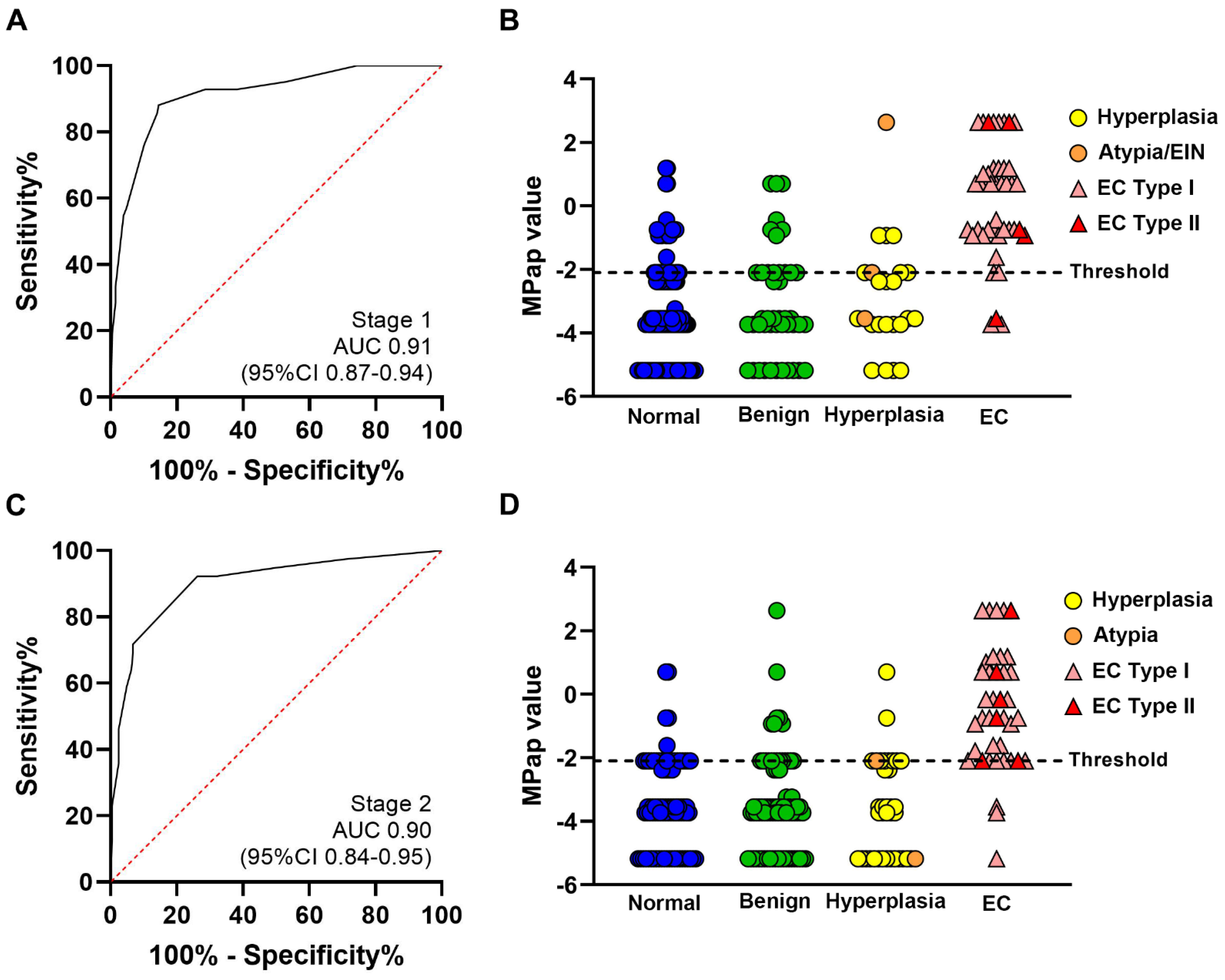
3.2. DNA Methylation Levels and Diagnostic Performance
Where: ϵ = −5.18
3.3. MPap and Endometrial Thickness
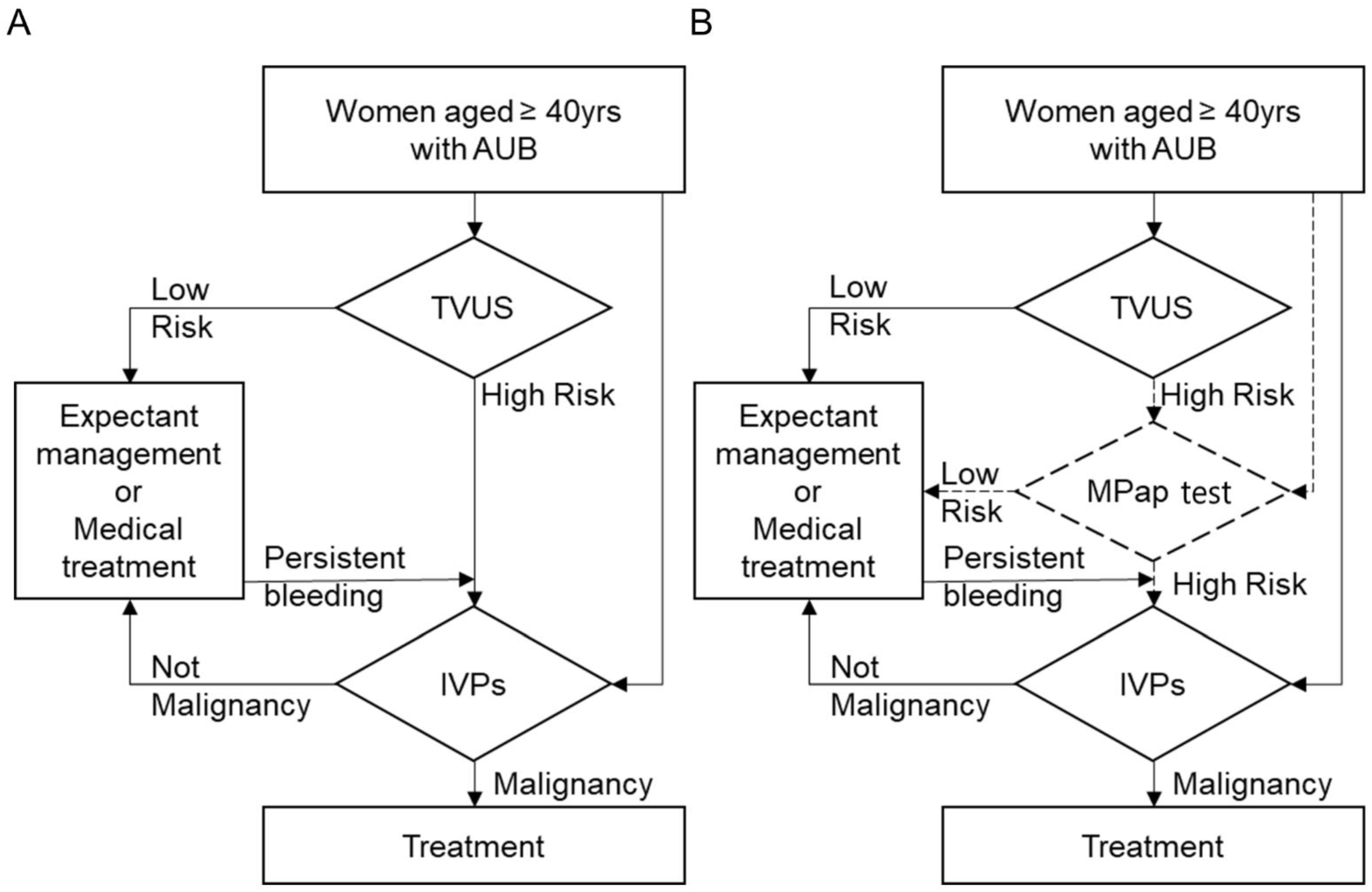
3.4. MPap in Algorism
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Brüggmann, D.; Ouassou, K.; Klingelhöfer, D.; Bohlmann, M.K.; Jaque, J.; Groneberg, D.A. Endometrial cancer: Mapping the global landscape of research. J. Transl. Med. 2020, 18, 386. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today; International Agency for Research on Cancer: Lyon, France, 2020. [Google Scholar]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Mukerji, B.; Baptiste, C.; Chen, L.; Tergas, A.I.; Hou, J.Y.; Ananth, C.V.; Neugut, A.I.; Hershman, D.L.; Wright, J.D. Racial disparities in young women with endometrial cancer. Gynecol. Oncol. 2018, 148, 527–534. [Google Scholar] [CrossRef]
- Scott, O.W.; Tin Tin, S.; Bigby, S.M.; Elwood, J.M. Rapid increase in endometrial cancer incidence and ethnic differences in New Zealand. Cancer Causes Control 2019, 30, 121–127. [Google Scholar] [CrossRef]
- Temkin, S.M.; Kohn, E.C.; Penberthy, L.; Cronin, K.A.; Rubinsak, L.; Dickie, L.A.; Minasian, L.; Noone, A.M. Hysterectomy-corrected rates of endometrial cancer among women younger than age 50 in the United States. Cancer Causes Control 2018, 29, 427–433. [Google Scholar] [CrossRef]
- Smrz, S.A.; Calo, C.; Fisher, J.L.; Salani, R. An ecological evaluation of the increasing incidence of endometrial cancer and the obesity epidemic. Am. J. Obstet. Gynecol. 2021, 224, 506.e501–506.e508. [Google Scholar] [CrossRef]
- Schramm, A.; Ebner, F.; Bauer, E.; Janni, W.; Friebe-Hoffmann, U.; Pellegrino, M.; De Gregorio, N.; Friedl, T.W.P. Value of endometrial thickness assessed by transvaginal ultrasound for the prediction of endometrial cancer in patients with postmenopausal bleeding. Arch. Gynecol. Obstet. 2017, 296, 319–326. [Google Scholar] [CrossRef]
- Smith-Bindman, R.; Weiss, E.; Feldstein, V. How thick is too thick? When endometrial thickness should prompt biopsy in postmenopausal women without vaginal bleeding. Ultrasound Obstet. Gynecol. 2004, 24, 558–565. [Google Scholar] [CrossRef]
- Jansen, F.W.; Vredevoogd, C.B.; Van Ulzen, K.; Hermans, J.; Trimbos, J.B.; Trimbos-Kemper, T.C. Complications of hysteroscopy: A prospective, multicenter study. Obstet. Gynecol. 2000, 96, 266–270. [Google Scholar] [CrossRef]
- Dijkhuizen, F.P.; Mol, B.W.; Brölmann, H.A.; Heintz, A.P. The accuracy of endometrial sampling in the diagnosis of patients with endometrial carcinoma and hyperplasia: A meta-analysis. Cancer 2000, 89, 1765–1772. [Google Scholar] [CrossRef] [PubMed]
- Van Hanegem, N.; Prins, M.M.; Bongers, M.Y.; Opmeer, B.C.; Sahota, D.S.; Mol, B.W.; Timmermans, A. The accuracy of endometrial sampling in women with postmenopausal bleeding: A systematic review and meta-analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 197, 147–155. [Google Scholar] [CrossRef]
- Klutstein, M.; Nejman, D.; Greenfield, R.; Cedar, H. DNA methylation in cancer and aging. Cancer Res. 2016, 76, 3446–3450. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.L.; Su, P.H.; Liao, Y.P.; Wu, T.I.; Hsu, Y.T.; Lin, W.Y.; Wang, H.C.; Weng, Y.C.; Ou, Y.C.; Huang, T.H.; et al. Integrated epigenomics analysis reveals a DNA methylation panel for endometrial cancer detection using cervical scrapings. Clin. Cancer Res. 2017, 23, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Liew, P.L.; Huang, R.L.; Wu, T.I.; Liao, C.C.; Chen, C.W.; Su, P.H.; Wang, H.C.; Weng, Y.C.; Lai, H.C. Combined genetic mutations and DNA-methylated genes as biomarkers for endometrial cancer detection from cervical scrapings. Clin. Epigenet. 2019, 11, 170. [Google Scholar] [CrossRef]
- Hajian-Tilaki, K. Sample size estimation in diagnostic test studies of biomedical informatics. J. Biomed. Inform. 2014, 48, 193–204. [Google Scholar] [CrossRef]
- Clarke, M.A.; Long, B.J.; Del Mar Morillo, A.; Arbyn, M.; Bakkum-Gamez, J.N.; Wentzensen, N. Association of endometrial cancer risk with postmenopausal bleeding in women: A systematic review and meta-analysis. JAMA Intern. Med. 2018, 178, 1210–1222. [Google Scholar] [CrossRef]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef]
- Kolehmainen, A.; Pasanen, A.; Tuomi, T.; Koivisto-Korander, R.; Bützow, R.; Loukovaara, M. Clinical factors as prognostic variables among molecular subgroups of endometrial cancer. PLoS ONE 2020, 11, e0242733. [Google Scholar] [CrossRef]
- Bakkum-Gamez, J.N.; Wentzensen, N.; Maurer, M.J.; Hawthorne, K.M.; Voss, J.S.; Kroneman, T.N.; Famuyide, A.O.; Clayton, A.C.; Halling, K.C.; Kerr, S.E.; et al. Detection of endometrial cancer via molecular analysis of DNA collected with vaginal tampons. Gynecol. Oncol. 2015, 137, 14–22. [Google Scholar] [CrossRef] [Green Version]
- Fiegl, H.; Gattringer, C.; Widschwendter, A.; Schneitter, A.; Ramoni, A.; Sarlay, D.; Gaugg, I.; Goebel, G.; Müller, H.M.; Mueller-Holzner, E.; et al. Methylated DNA collected by tampons—A new tool to detect endometrial cancer. Cancer Epidemiol. Biomark. Prev. 2004, 13, 882–888. [Google Scholar] [CrossRef]
- Wang, Y.; Li, L.; Douville, C.; Cohen, J.D.; Yen, T.T.; Kinde, I.; Sundfelt, K.; Kjær, S.K.; Hruban, R.H.; Shih, I.M.; et al. Evaluation of liquid from the Papanicolaou test and other liquid biopsies for the detection of endometrial and ovarian cancers. Sci. Transl. Med. 2018, 10, eaap8793. [Google Scholar] [CrossRef] [PubMed]
- Wentzensen, N.; Bakkum-Gamez, J.N.; Killian, J.K.; Sampson, J.; Guido, R.; Glass, A.; Adams, L.; Luhn, P.; Brinton, L.A.; Rush, B.; et al. Discovery and validation of methylation markers for endometrial cancer. Int. J. Cancer 2014, 135, 1860–1868. [Google Scholar] [CrossRef] [PubMed]
- Le Lous, M.; De Chanaud, N.; Bourret, A.; Senat, M.V.; Colmant, C.; Jaury, P.; Tesnière, A.; Tsatsaris, V. Improving the quality of transvaginal ultrasound scan by simulation training for general practice residents. Adv. Simul. 2017, 2, 24. [Google Scholar] [CrossRef]
- Maritschnegg, E.; Wang, Y.; Pecha, N.; Horvat, R.; Van Nieuwenhuysen, E.; Vergote, I.; Heitz, F.; Sehouli, J.; Kinde, I.; Diaz, L.A.; et al. Lavage of the uterine cavity for molecular detection of müllerian duct carcinomas: A proof-of-concept study. J. Clin. Oncol. 2015, 33, 4293–4300. [Google Scholar] [CrossRef]
- Krimmel, J.D.; Schmitt, M.W.; Harrell, M.I.; Agnew, K.J.; Kennedy, S.R.; Emond, M.J.; Loeb, L.A.; Swisher, E.M.; Risques, R.A. Ultra-deep sequencing detects ovarian cancer cells in peritoneal fluid and reveals somatic TP53 mutations in noncancerous tissues. Proc. Natl. Acad. Sci. USA 2016, 113, 6005–6010. [Google Scholar] [CrossRef]
- Anglesio, M.S.; Papadopoulos, N.; Ayhan, A.; Nazeran, T.M.; Noë, M.; Horlings, H.M.; Lum, A.; Jones, S.; Senz, J.; Seckin, T.; et al. Cancer-associated mutations in endometriosis without cancer. N. Engl. J. Med. 2017, 376, 1835–1848. [Google Scholar] [CrossRef]
- Nair, N.; Camacho-Vanegas, O.; Rykunov, D.; Dashkoff, M.; Camacho, S.C.; Schumacher, C.A.; Irish, J.C.; Harkins, T.T.; Freeman, E.; Garcia, I.; et al. Genomic analysis of uterine lavage fluid detects early endometrial cancers and reveals a prevalent landscape of driver mutations in women without histopathologic evidence of cancer: A prospective cross-sectional study. PLoS Med. 2016, 13, e1002206. [Google Scholar] [CrossRef]
- Gemer, O.; Segev, Y.; Helpman, L.; Hag-Yahia, N.; Eitan, R.; Raban, O.; Vaknin, Z.; Leytes, S.; Ben Arie, A.; Amit, A.; et al. Is there a survival advantage in diagnosing endometrial cancer in asymptomatic postmenopausal patients? An Israeli gynecology oncology group study. Am. J. Obstet. Gynecol. 2018, 219, 181.e181–181.e186. [Google Scholar] [CrossRef]
- Gull, B.; Karlsson, B.; Milsom, I.; Granberg, S. Can ultrasound replace dilation and curettage? A longitudinal evaluation of postmenopausal bleeding and transvaginal sonographic measurement of the endometrium as predictors of endometrial cancer. Am. J. Obstet. Gynecol. 2003, 188, 401–408. [Google Scholar] [CrossRef]
- Jacobs, I.; Gentry-Maharaj, A.; Burnell, M.; Manchanda, R.; Singh, N.; Sharma, A.; Ryan, A.; Seif, M.W.; Amso, N.N.; Turner, G.; et al. Sensitivity of transvaginal ultrasound screening for endometrial cancer in postmenopausal women: A case-control study within the UKCTOCS cohort. Lancet Oncol. 2011, 12, 38–48. [Google Scholar] [CrossRef]
- Duffy, S.; Jackson, T.L.; Lansdown, M.; Philips, K.; Wells, M.; Pollard, S.; Clack, G.; Cuzick, J.; Coibion, M.; Bianco, A.R. The ATAC adjuvant breast cancer trial in postmenopausal women: Baseline endometrial subprotocol data. BJOG 2003, 110, 1099–1106. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Cohort | Normal | Benign | Precancerous | EC | p-Value | |
|---|---|---|---|---|---|---|
| Stage 1 | n | 138 | 45 | 24 | 42 | |
| Age, mean (SD) | 49.3 (7.2) | 51.0 (9.2) | 48.0 (6.2) | 56.7 (8.5) | <0.0001 | |
| BMI, mean (SD) | 24.0 (4.2) | 25.1 (5.4) | 25.6 (5.8) | 25.7 (4.8) | 0.0966 | |
| ET, mean (SD) | 11.6 (9.2) | 13.8 (6.9) | 11.8 (7.0) | 16.4 (8.8) | 0.0223 | |
| BHLHE22 (Ct) | 49.7 (1.8) | 49.8 (1.4) | 49.6 (2.2) | 45.6 (6.4) | <0.0001 | |
| CDO1 (Ct) | 46.0 (5.0) | 46.2 (4.2) | 45.2 (5.4) | 38.4 (5.1) | <0.0001 | |
| Stage 2 | n | 86 | 83 | 37 | 39 | |
| Age, mean (SD) | 49.4 (6.7) | 49.0 (6.9) | 48.3 (5.0) | 59.9 (11.0) | <0.0001 | |
| BMI, mean (SD) | 24.1 (4.6) | 24.0 (3.7) | 24.1 (3.6) | 27.1 (6.2) | 0.0019 | |
| ET, mean (SD) | 11.4 (13.6) | 13.8 (18.6) | 11.7 (4.7) | 16.4 (8.1) | 0.2957 | |
| BHLHE22 (Ct) | 50.0 (0.0) | 49.9 (1.4) | 50.0 (0.0) | 46.1 (6.2) | <0.0001 | |
| CDO1 (Ct) | 48.0 (3.4) | 47.6 (4.1) | 47.8 (3.6) | 42.4 (6.2) | <0.0001 |
| Composition of Different Combined Variables | AUC (95% CI) |
|---|---|
| BHLHE22 + CDO1 | 0.86 (0.82 to 0.90) |
| BHLHE22 + CDO1 + Age | 0.89 (0.84 to 0.92) |
| BHLHE22 + CDO1 + BMI | 0.88 (0.83 to 0.92) |
| BHLHE22 + CDO1 + Age + BMI | 0.91 (0.87 to 0.94) |
| MPap-Value | TVUS | p-Value | ||
|---|---|---|---|---|
| ≥Cutoff Threshold | ET | |||
| Stage 1 | Sen | 92.9 (80.5–98.5) | 50.0 (32.9–67.1) | <0.0001 |
| Spe | 71.5 (64.8–77.5) | 77.7 (71.2–83.3) | 0.1190 | |
| PPV | 39.8 (34.4–45.5) | 29.0 (21.1–38.3) | 0.0128 | |
| NPV | 98.0 (94.3–99.3) | 89.5 (85.9–92.2) | 0.0001 | |
| Stage 2 | Sen | 92.5 (82.9–100.0) | 55.6 (38.1–72.1) | <0.0001 |
| Spe | 73.8 (67.6–79.4) | 82.2 (76.2–87.3) | 0.0271 | |
| PPV | 40.2 (30.8–50.5) | 36.4 (27.3–46.5) | 0.3936 | |
| NPV | 98.1 (95.8–100.0) | 91.0 (87.5–93.6) | 0.0006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wen, K.-C.; Huang, R.-L.; Chen, L.-Y.; Wu, T.-I.; Lu, C.-H.; Chu, T.-Y.; Ou, Y.-C.; Wu, C.-H.; Hsu, S.-T.; Ding, D.-C.; et al. Endometrial Cancer Detection Using a Cervical DNA Methylation Assay (MPap) in Women with Abnormal Uterine Bleeding: A Multicenter Hospital-Based Validation Study. Cancers 2022, 14, 4343. https://doi.org/10.3390/cancers14174343
Wen K-C, Huang R-L, Chen L-Y, Wu T-I, Lu C-H, Chu T-Y, Ou Y-C, Wu C-H, Hsu S-T, Ding D-C, et al. Endometrial Cancer Detection Using a Cervical DNA Methylation Assay (MPap) in Women with Abnormal Uterine Bleeding: A Multicenter Hospital-Based Validation Study. Cancers. 2022; 14(17):4343. https://doi.org/10.3390/cancers14174343
Chicago/Turabian StyleWen, Kuo-Chang, Rui-Lan Huang, Lin-Yu Chen, Tzu-I Wu, Chien-Hsing Lu, Tang-Yuan Chu, Yu-Che Ou, Chen-Hsuan Wu, Shih-Tien Hsu, Dah-Ching Ding, and et al. 2022. "Endometrial Cancer Detection Using a Cervical DNA Methylation Assay (MPap) in Women with Abnormal Uterine Bleeding: A Multicenter Hospital-Based Validation Study" Cancers 14, no. 17: 4343. https://doi.org/10.3390/cancers14174343
APA StyleWen, K.-C., Huang, R.-L., Chen, L.-Y., Wu, T.-I., Lu, C.-H., Chu, T.-Y., Ou, Y.-C., Wu, C.-H., Hsu, S.-T., Ding, D.-C., Chu, L.-H., Chen, C.-W., Chang, H.-C., Liu, Y.-S., Wang, H.-C., Weng, Y.-C., Su, P.-H., Lin, H., & Lai, H.-C. (2022). Endometrial Cancer Detection Using a Cervical DNA Methylation Assay (MPap) in Women with Abnormal Uterine Bleeding: A Multicenter Hospital-Based Validation Study. Cancers, 14(17), 4343. https://doi.org/10.3390/cancers14174343