
Demographics, Outcomes, and Risk Factors for Patients with Sarcoma and COVID-19: A CCC19-Registry Based Retrospective Cohort Study


 , ,
, ,  , , , , , , , , , ,
, , , , , , , , , ,  , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
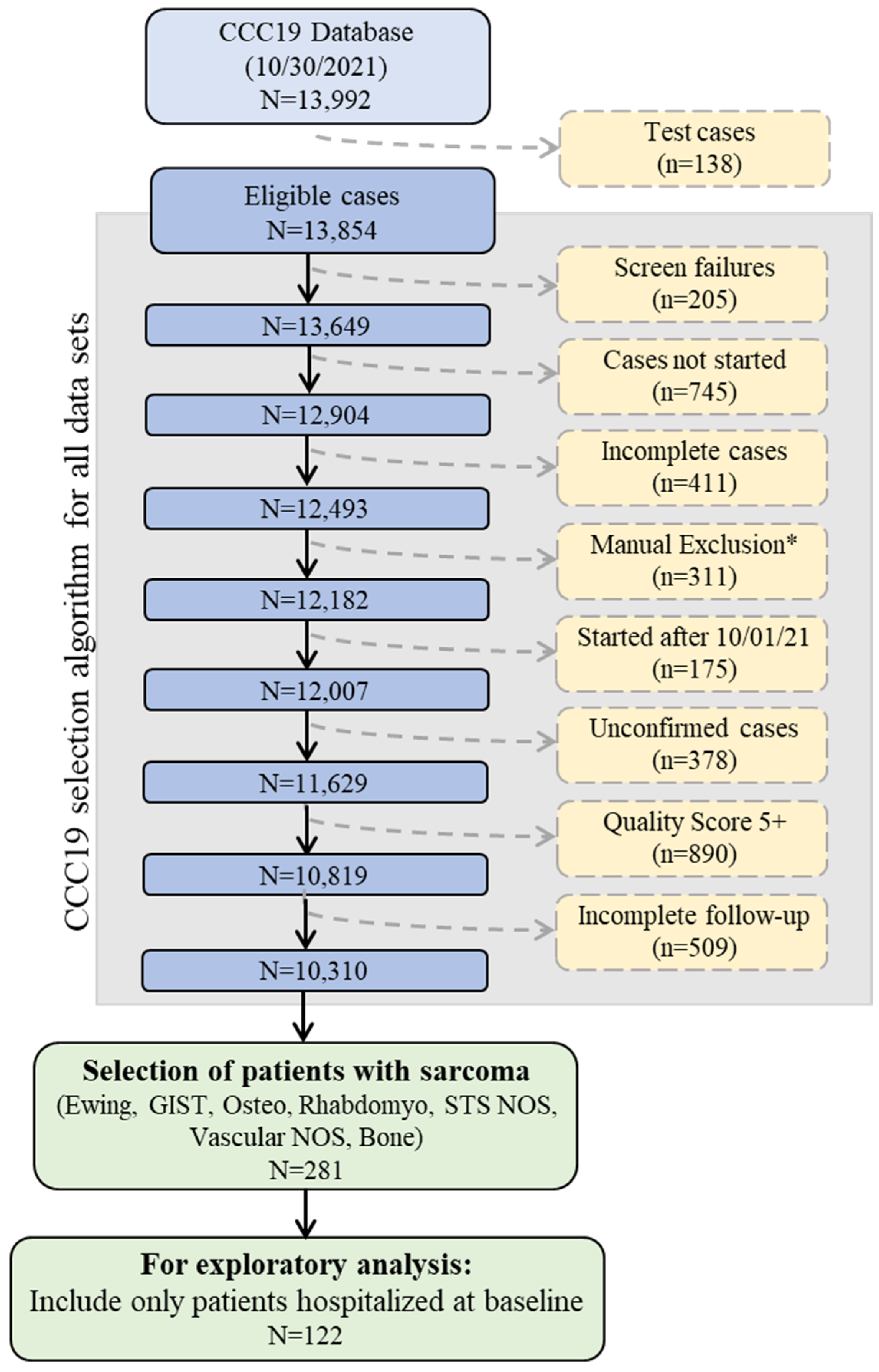
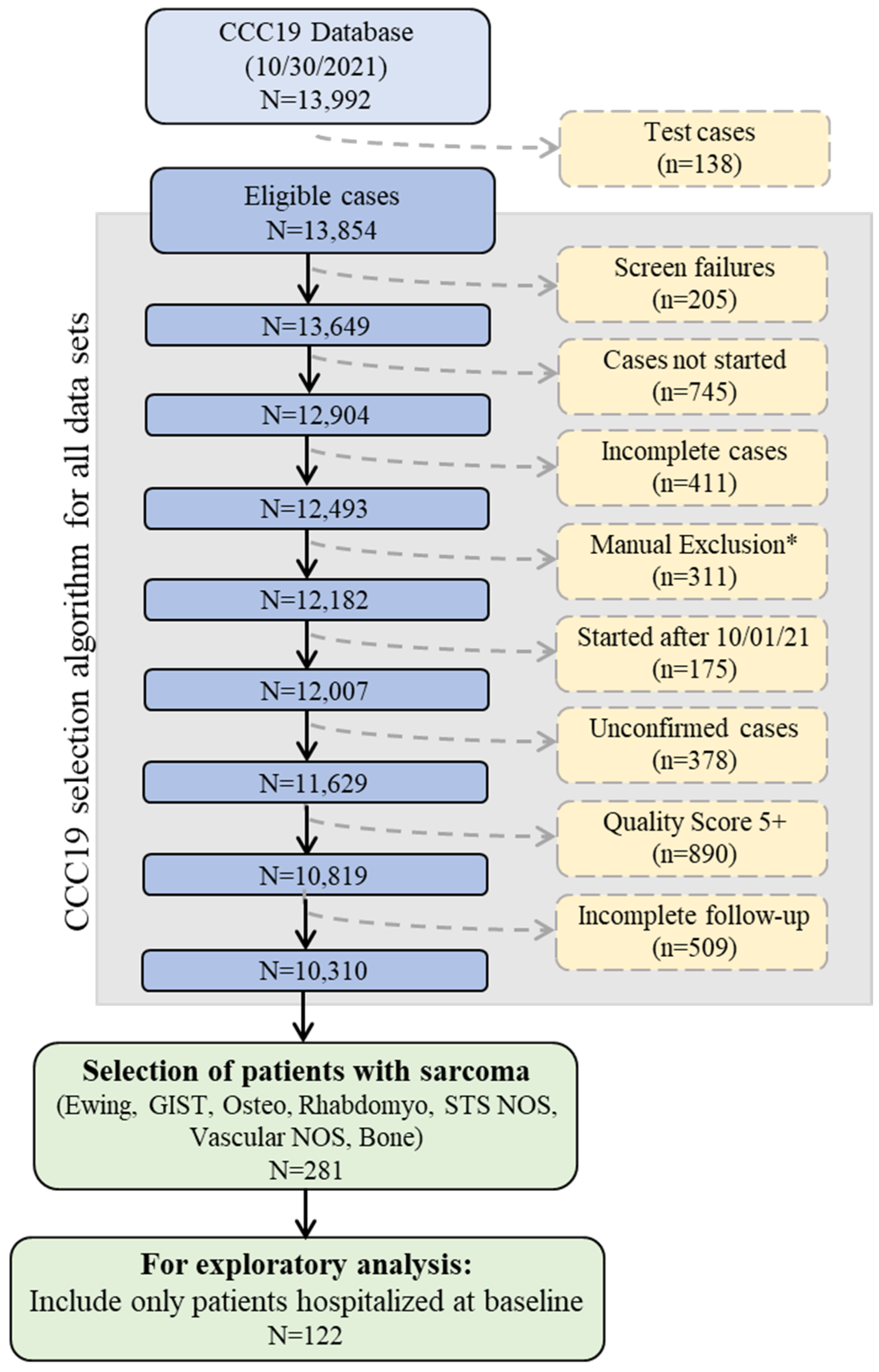
2.1. Study Design and Patient Population
2.2. Data Elements
2.3. Statistical Analysis
2.4. Comparison to SEER Data
3. Results
3.1. Clinical Characteristics of Sarcoma Patients Infected with SARS-CoV-2
3.2. Clinical Outcomes Stratified by Sarcoma Subgroup
3.3. Clinical Risk Factors for COVID-19 Severity
3.4. Comparison to Matched SEER Cohort
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The COVID-19 and Cancer Consortium. A Systematic Framework to Rapidly Obtain Data on Patients with Cancer and COVID-19: CCC19 Governance, Protocol, and Quality Assurance. Cancer Cell 2020, 38, 761–766. [Google Scholar] [CrossRef] [PubMed]
- Mehta, V.; Goel, S.; Kabarriti, R.; Cole, D.; Goldfinger, M.; Acuna-Villaorduna, A.; Pradhan, K.; Thota, R.; Reissman, S.; Sparano, J.A.; et al. Case Fatality Rate of Cancer Patients with COVID-19 in a New York Hospital System. Cancer Discov. 2020, 10, 935–941. [Google Scholar] [CrossRef]
- Saini, K.S.; Tagliamento, M.; Lambertini, M.; McNally, R.; Romano, M.; Leone, M.; Curigliano, G.; de Azambuja, E. Mortality in patients with cancer and coronavirus disease 2019: A systematic review and pooled analysis of 52 studies. Eur. J. Cancer 2020, 139, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Dai, M.; Liu, D.; Liu, M.; Zhou, F.; Li, G.; Chen, Z.; Zhang, Z.; You, H.; Wu, M.; Zheng, Q.; et al. Patients with Cancer Appear More Vulnerable to SARS-CoV-2: A Multicenter Study during the COVID-19 Outbreak. Cancer Discov. 2020, 10, 783–791. [Google Scholar] [CrossRef]
- Giannakoulis, V.G.; Papoutsi, E.; Siempos, I.I. Effect of Cancer on Clinical Outcomes of Patients With COVID-19: A Meta-Analysis of Patient Data. JCO Glob. Oncol. 2020, 6, 799–808. [Google Scholar] [CrossRef]
- Kuderer, N.M.; Choueiri, T.K.; Shah, D.P.; Shyr, Y.; Rubinstein, S.M.; Rivera, D.R.; Shete, S.; Hsu, C.Y.; Desai, A.; de Lima Lopes, G., Jr.; et al. Clinical impact of COVID-19 on patients with cancer (CCC19): A cohort study. Lancet 2020, 395, 1907–1918. [Google Scholar] [CrossRef]
- Grivas, P.; Khaki, A.R.; Wise-Draper, T.M.; French, B.; Hennessy, C.; Hsu, C.Y.; Shyr, Y.; Li, X.; Choueiri, T.K.; Painter, C.A.; et al. Association of clinical factors and recent anticancer therapy with COVID-19 severity among patients with cancer: A report from the COVID-19 and Cancer Consortium. Ann. Oncol. 2021, 32, 787–800. [Google Scholar] [CrossRef] [PubMed]
- Doyle, L.A. Sarcoma classification: An update based on the 2013 World Health Organization Classification of Tumors of Soft Tissue and Bone. Cancer 2014, 120, 1763–1774. [Google Scholar] [CrossRef]
- Crago, A.M.; Brennan, M.F. Principles in Management of Soft Tissue Sarcoma. Adv. Surg. 2015, 49, 107–122. [Google Scholar] [CrossRef]
- Onega, T.; Duell, E.J.; Shi, X.; Wang, D.; Demidenko, E.; Goodman, D. Geographic access to cancer care in the U.S. Cancer 2008, 112, 909–918. [Google Scholar] [CrossRef]
- Seynaeve, C.; Verweij, J. High-dose chemotherapy in adult sarcomas: No standard yet. Semin. Oncol. 1999, 26, 119–133. [Google Scholar] [PubMed]
- Demetri, G.D. High-dose ifosfamide in the treatment of sarcomas of soft tissues and bone. Semin. Oncol. 1996, 23, 22–26. [Google Scholar] [PubMed]
- Verma, S.; Bramwell, V. Dose-intensive chemotherapy in advanced adult soft tissue sarcoma. Expert Rev. Anticancer Ther. 2002, 2, 201–215. [Google Scholar] [CrossRef] [PubMed]
- Wagner, M.J.; Pollack, S.M.; Cranmer, L.D.; Thompson, M.J.; Maxwell, S.; Wright, S.; Khaki, A.R.; Madeleine, M.M.; Grivas, P.; Kuderer, N.M.; et al. Outcomes of Patients with Sarcoma and COVID-19 Infection: A Single Institution Cohort Analysis. Cancer Investig. 2021, 39, 315–320. [Google Scholar] [CrossRef]
- French, B.; Shotwell, M.S. Regression Models for Ordinal Outcomes. JAMA 2022, 328, 772–773. [Google Scholar] [CrossRef]
- Elo, I.T.; Luck, A.; Stokes, A.C.; Hempstead, K.; Xie, W.; Preston, S.H. Evaluation of Age Patterns of COVID-19 Mortality by Race and Ethnicity from March 2020 to October 2021 in the US. JAMA Netw. Open 2022, 5, e2212686. [Google Scholar] [CrossRef]
- Wagner, M.J.; Livingston, J.A.; Patel, S.R.; Benjamin, R.S. Chemotherapy for Bone Sarcoma in Adults. J. Oncol. Pract. 2016, 12, 208–216. [Google Scholar] [CrossRef]
- Picci, P. Osteosarcoma (osteogenic sarcoma). Orphanet J. Rare Dis. 2007, 2, 6. [Google Scholar] [CrossRef]
- Harder, T.; Kulper-Schiek, W.; Reda, S.; Treskova-Schwarzbach, M.; Koch, J.; Vygen-Bonnet, S.; Wichmann, O. Effectiveness of COVID-19 vaccines against SARS-CoV-2 infection with the Delta (B.1.617.2) variant: Second interim results of a living systematic review and meta-analysis, 1 January to 25 August 2021. Eurosurveillance 2021, 26, 2100920. [Google Scholar] [CrossRef]
- Liu, Q.; Qin, C.; Liu, M.; Liu, J. Effectiveness and safety of SARS-CoV-2 vaccine in real-world studies: A systematic review and meta-analysis. Infect. Dis. Poverty 2021, 10, 132. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Perez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.; Shao, W.; Chen, X.; Zhang, B.; Wang, G.; Zhang, W. Real-world effectiveness of COVID-19 vaccines: A literature review and meta-analysis. Int. J. Infect. Dis. 2022, 114, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Seneviratne, S.L.; Yasawardene, P.; Wijerathne, W.; Somawardana, B. COVID-19 vaccination in cancer patients: A narrative review. J. Int. Med. Res. 2022, 50, 3000605221086155. [Google Scholar] [CrossRef] [PubMed]
- Magesh, S.; John, D.; Li, W.T.; Li, Y.; Mattingly-app, A.; Jain, S.; Chang, E.Y.; Ongkeko, W.M. Disparities in COVID-19 Outcomes by Race, Ethnicity, and Socioeconomic Status: A Systematic Review and Meta-analysis. JAMA Netw. Open 2021, 4, e2134147. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.; Reid, S.A.; French, B.; Hennessy, C.; Hwang, C.; Gatson, N.T.; Duma, N.; Mishra, S.; Nguyen, R.; Hawley, J.E.; et al. Racial Disparities in COVID-19 Outcomes Among Black and White Patients with Cancer. JAMA Netw. Open 2022, 5, e224304. [Google Scholar] [CrossRef] [PubMed]
- Wagner, M.J.; Chalian, M.; Ricciotti, R.; Roberts, J.L.; Thompson, M.J.; Schaub, S. Sarcoma Care Collaborations: Models for patient centered sub-specialty oncology care in the COVID-19 era and beyond. IJCCD 2022, 2. [Google Scholar] [CrossRef]
- Tevaarwerk, A.J.; Chandereng, T.; Osterman, T.; Arafat, W.; Smerage, J.; Polubriaginof, F.C.G.; Heinrichs, T.; Sugalski, J.; Martin, D.B. Oncologist Perspectives on Telemedicine for Patients with Cancer: A National Comprehensive Cancer Network Survey. JCO Oncol. Pract. 2021, 17, e1318–e1326. [Google Scholar] [CrossRef]

{kind=link}
| Characteristics | All Patients | STS | Bone | GIST | Other/Indolent |
|---|---|---|---|---|---|
| N = 281 | N = 153 | N = 48 | N = 45 | N = 35 | |
| Age, years [Median (IQR)] | 56 (41–66) | 56 (43–64) | 36 (22–56) | 65 (60–72) | 56 (38–68) |
| Sex | |||||
| Female | 132 (47%) | 80 (52%) | 20 (42%) | 23 (51%) | 9 (26%) |
| Male | 149 (53%) | 73 (48%) | 28 (58%) | 22 (49%) | 26 (74%) |
| Race/ethnicity | |||||
| Non-Hispanic White | 133 (47%) | 73 (48%) | 24 (50%) | 25 (56%) | 11 (31%) |
| Other 1 | 145 (52%) | 77 (50%) | 24 (50%) | 20 (44%) | 24 (69%) |
| Missing/Unknown | 3 (1%) | 3 (2%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Obesity | |||||
| Not Obese | 167 (59%) | 81 (53%) | 29 (60%) | 30 (67%) | 27 (77%) |
| Obese | 111 (40%) | 71 (46%) | 18 (38%) | 14 (31%) | 8 (23%) |
| Missing/Unknown | 3 (1%) | 1 (1%) | 1 (2%) | 1 (2%) | 0 (0%) |
| Comorbidities | |||||
| Cardiovascular | 51 (18%) | 29 (19%) | 9 (19%) | 10 (22%) | 3 (9%) |
| Pulmonary | 40 (14%) | 19 (12%) | 7 (15%) | 11 (24%) | 3 (9%) |
| Renal disease | 14 (5%) | 7 (5%) | 1 (2%) | 3 (7%) | 3 (9%) |
| Diabetes Mellitus | 54 (19%) | 27 (18%) | 11 (23%) | 9 (20%) | 7 (20%) |
| Missing/Unknown | 4 (1%) | 2 (1%) | 1 (2%) | 1 (2%) | 0 (0%) |
| ECOG performance status | |||||
| 0 | 78 (28%) | 50 (33%) | 7 (15%) | 15 (33%) | 6 (17%) |
| 1 | 86 (31%) | 53 (35%) | 9 (19%) | 10 (22%) | 14 (40%) |
| 2+ | 42 (15%) | 21 (14%) | 9 (19%) | 7 (16%) | 5 (14%) |
| Unknown | 75 (27%) | 29 (19%) | 23 (48%) | 13 (29%) | 10 (29%) |
| Cancer Status | |||||
| Remission/NED | 105 (37%) | 45 (29%) | 18 (38%) | 23 (51%) | 19 (54%) |
| Active, stable/responding | 79 (28%) | 42 (27%) | 12 (25%) | 14 (31%) | 11 (31%) |
| Active, progressing | 73 (26%) | 50 (33%) | 14 (29%) | 7 (16%) | 2 (6%) |
| Unknown | 24 (9%) | 16 (10%) | 4 (8%) | 1 (2%) | 3 (9%) |
| Metastasis and lung status | |||||
| No metastatic cancer | 172 (61%) | 85 (56%) | 25 (52%) | 33 (73%) | 29 (83%) |
| Metastatic cancer to the lung | 53 (19%) | 38 (25%) | 12 (25%) | 3 (7%) | 0 (0%) |
| Metastatic cancer—other sites | 37 (13%) | 19 (12%) | 8 (17%) | 5 (11%) | 5 (14%) |
| Missing/Unknown | 19 (7%) | 11 (7%) | 3 (6%) | 4 (9%) | 1 (3%) |
| Modality of Recent Anti-cancer Therapy (within 3 months prior to COVID-19 diagnosis) | |||||
| None within 3 months of COVID-19 | 137 (49%) | 72 (47%) | 21 (44%) | 19 (42%) | 25 (71%) |
| Cytotoxic Therapy | 82 (29%) | 53 (35%) | 22 (46%) | 3 (7%) | 4 (11%) |
| Anthracycline 2 | 16 (6%) | 9 (6%) | 4 (8%) | 1 (2%) | 2 (6%) |
| Targeted Therapy | 44 (16%) | 13 (8%) | 6 (12%) | 22 (49%) | 3 (9%) |
| TKI | 31 (11%) | 10 (7%) | 4 (8%) | 17 (38%) | 0 (0%) |
| VEGF Inhibitor | 13 (5%) | 8 (5%) | 2 (4%) | 3 (7%) | 0 (0%) |
| Endocrine Therapy | 4 (1%) | 2 (1%) | 1 (2%) | 1 (2%) | 0 (0%) |
| Immunotherapy | 10 (4%) | 8 (5%) | 1 (2%) | 1 (2%) | 0 (0%) |
| Local | 41 (15%) | 27 (18%) | 7 (15%) | 4 (9%) | 3 (9%) |
| Other | 2 (1%) | 0 (0%) | 1 (2%) | 1 (2%) | 0 (0%) |
| Missing/Unknown | 2 (1%) | 1 (1%) | 1 (2%) | 0 (0%) | 0 (0%) |
| Timing of anti-cancer therapy | |||||
| Never or after COVID-19 diagnosis | 24 (9%) | 14 (9%) | 6 (12%) | 3 (7%) | 1 (3%) |
| 0–4 weeks before COVID-19 diagnosis | 113 (40%) | 60 (39%) | 23 (48%) | 21 (47%) | 9 (26%) |
| 1–3 months before COVID-19 diagnosis | 29 (10%) | 20 (13%) | 3 (6%) | 5 (11%) | 1 (3%) |
| More than 3 months before COVID-19 diagnosis | 106 (38%) | 52 (34%) | 15 (31%) | 16 (36%) | 23 (66%) |
| Missing/Unknown | 9 (3%) | 7 (5%) | 1 (2%) | 0 (0%) | 1 (3%) |
| Date of COVID-19 Diagnosis | |||||
| January–April 2020 | 44 (16%) | 21 (14%) | 5 (10%) | 9 (20%) | 9 (26%) |
| May–August 2020 | 125 (44%) | 72 (47%) | 28 (58%) | 16 (36%) | 9 (26%) |
| September–December 2020 | 65 (23%) | 37 (24%) | 8 (17%) | 9 (20%) | 11 (31%) |
| January–April 2021 | 43 (15%) | 22 (14%) | 7 (15%) | 8 (18%) | 6 (17%) |
| May–September 2021 | 4 (1%) | 1 (1%) | 0 (0%) | 3 (6%) | 0 (0%) |
| Outcomes | All Patients | STS | Bone | GIST | Other/Indolent |
|---|---|---|---|---|---|
| N = 281 | N = 153 | N = 48 | N = 45 | N = 35 | |
| Hospitalization | 139 (49%) | 79 (52%) | 24 (50%) | 20 (44%) | 16 (46%) |
| Without supplemental O2 | 43 (15%) | 27 (18%) | 7 (15%) | 3 (7%) | 6 (17%) |
| With Supplemental O2 1 | 93 (33%) | 50 (33%) | 16 (33%) | 17 (38%) | 10 (29%) |
| Intensive care unit admission | 31 (11%) | 19 (12%) | 4 (8%) | 5 (11%) | 3 (9%) |
| Received mechanical ventilation | 16 (6%) | 8 (5%) | 4 (8%) | 3 (7%) | 1 (3%) |
| Death due to any cause | |||||
| Within 30 days | 23 (8%) | 13 (8%) | 7 (15%) | 2 (4%) | 1 (3%) |
| Ever during follow-up | 44 (16%) | 30 (20%) | 9 (19%) | 4 (9%) | 1 (3%) |
| Follow up time, days [Median (IQR)] | 90 (30–180) | 90 (30–180) | 63 (29–180) | 90 (30–180) | 180 (36–225) |
| With Sarcoma Subtypes | With Anti-Cancer Modalities | |||
|---|---|---|---|---|
| Odds Ratios | 95% CI | Odds Ratios | 95% CI | |
| Sarcoma subtype | ||||
| Bone vs. STS | 0.68 | 0.29–1.57 | ||
| GIST vs. STS | 0.37 | 0.16–0.82 | ||
| Other/Indolent histologies vs STS | 0.34 | 0.14–0.83 | ||
| Timing of any anti-cancer therapy | ||||
| 0–3 months vs. >3 months before COVID-19 diagnosis | 1.59 | 0.81–3.14 | ||
| Never or after COVID diagnosis vs. >3 months before COVID-19 diagnosis | 1.08 | 0.38–3.08 | ||
| Modality of recent anti-cancer therapy | ||||
| Cytotoxic therapy (yes vs. no) | 1.97 | 0.99–3.93 | ||
| Targeted therapy (yes vs. no) | 0.97 | 0.46–2.03 | ||
| Immunotherapy (yes vs. no) | 2.03 | 0.46–8.99 | ||
| Locoregional therapy (yes vs. no) | 1.56 | 0.73–3.32 | ||
| No therapy, ever vs. >3 months before COVID-19 diagnosis | 1.34 | 0.50–3.59 | ||
| Age, per decade | ||||
| <40 years | 0.87 | 0.48–1.59 | 0.97 | 0.54–1.74 |
| >40 years | 1.50 | 1.17–1.93 | 1.43 | 1.11–1.83 |
| Sex (Male vs. Female) | 1.71 | 0.98–2.99 | 1.51 | 0.87–2.60 |
| Renal disease (yes vs. no) | 3.69 | 1.25–10.9 | 2.92 | 0.94–9.03 |
| ECOG performance status | ||||
| 1 vs. 0 | 2.01 | 0.97–4.16 | 1.74 | 0.85-3.58 |
| 2+ vs. 0 | 20.7 | 8.24–52.0 | 17.4 | 7.01–43.2 |
| Unknown vs. 0 | 2.98 | 1.35–6.54 | 2.60 | 1.22–5.55 |
| Metastasis | ||||
| To lung vs. none | 5.69 | 2.46–13.2 | 6.47 | 2.80–15.0 |
| To other sites vs. none | 2.94 | 1.29–6.70 | 2.80 | 1.19–6.60 |
| Date of COVID-19 Diagnosis | ||||
| May–August 2020 vs. January–April 2020 | 0.41 | 0.19–0.90 | 0.41 | 0.19–0.89 |
| September–December 2020 vs. January–April 2020 | 0.14 | 0.06–0.33 | 0.14 | 0.06–0.33 |
| January–September 2021 vs. January–April 2020 | 0.31 | 0.12–0.78 | 0.27 | 0.11–0.69 |
| 30 Day Mortality | CCC19 | SEER | |||||
|---|---|---|---|---|---|---|---|
| N Cases | n Deaths | Mortality Rate (%) | N Cases | n Deaths | Mortality Rate (%) | p-Value 1 | |
| Overall | 255 | 20 | 7.8% | 16582 | 1223 | 7.4% | 0.718 |
| Sarcoma Subtype | |||||||
| Bone | 37 | 5 | 13.5% | 608 | 27 | 4.4% | 0.030 |
| GIST | 43 | 2 | 4.7% | 1408 | 52 | 3.7% | 0.673 |
| STS | 144 | 12 | 8.3% | 13,689 | 1123 | 8.2% | 0.879 |
| Other | 31 | 1 | 3.2% | 877 | 21 | 2.4% | 0.539 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wagner, M.J.; Hennessy, C.; Beeghly, A.; French, B.; Shah, D.P.; Croessmann, S.; Vilar-Compte, D.; Ruiz-Garcia, E.; Ingham, M.; Schwartz, G.K.; et al. Demographics, Outcomes, and Risk Factors for Patients with Sarcoma and COVID-19: A CCC19-Registry Based Retrospective Cohort Study. Cancers 2022, 14, 4334. https://doi.org/10.3390/cancers14174334
Wagner MJ, Hennessy C, Beeghly A, French B, Shah DP, Croessmann S, Vilar-Compte D, Ruiz-Garcia E, Ingham M, Schwartz GK, et al. Demographics, Outcomes, and Risk Factors for Patients with Sarcoma and COVID-19: A CCC19-Registry Based Retrospective Cohort Study. Cancers. 2022; 14(17):4334. https://doi.org/10.3390/cancers14174334
Chicago/Turabian StyleWagner, Michael J., Cassandra Hennessy, Alicia Beeghly, Benjamin French, Dimpy P. Shah, Sarah Croessmann, Diana Vilar-Compte, Erika Ruiz-Garcia, Matthew Ingham, Gary K. Schwartz, and et al. 2022. "Demographics, Outcomes, and Risk Factors for Patients with Sarcoma and COVID-19: A CCC19-Registry Based Retrospective Cohort Study" Cancers 14, no. 17: 4334. https://doi.org/10.3390/cancers14174334
APA StyleWagner, M. J., Hennessy, C., Beeghly, A., French, B., Shah, D. P., Croessmann, S., Vilar-Compte, D., Ruiz-Garcia, E., Ingham, M., Schwartz, G. K., Painter, C. A., Chugh, R., Fecher, L., Park, C., Zamulko, O., Trent, J. C., Subbiah, V., Khaki, A. R., Tachiki, L., ... Davis, E. J., on behalf of the COVID-19 and Cancer Consortium. (2022). Demographics, Outcomes, and Risk Factors for Patients with Sarcoma and COVID-19: A CCC19-Registry Based Retrospective Cohort Study. Cancers, 14(17), 4334. https://doi.org/10.3390/cancers14174334