

Preoperative Multiparametric Quantitative Magnetic Resonance Imaging Correlates with Prognosis and Recurrence Patterns in Pancreatic Ductal Adenocarcinoma


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
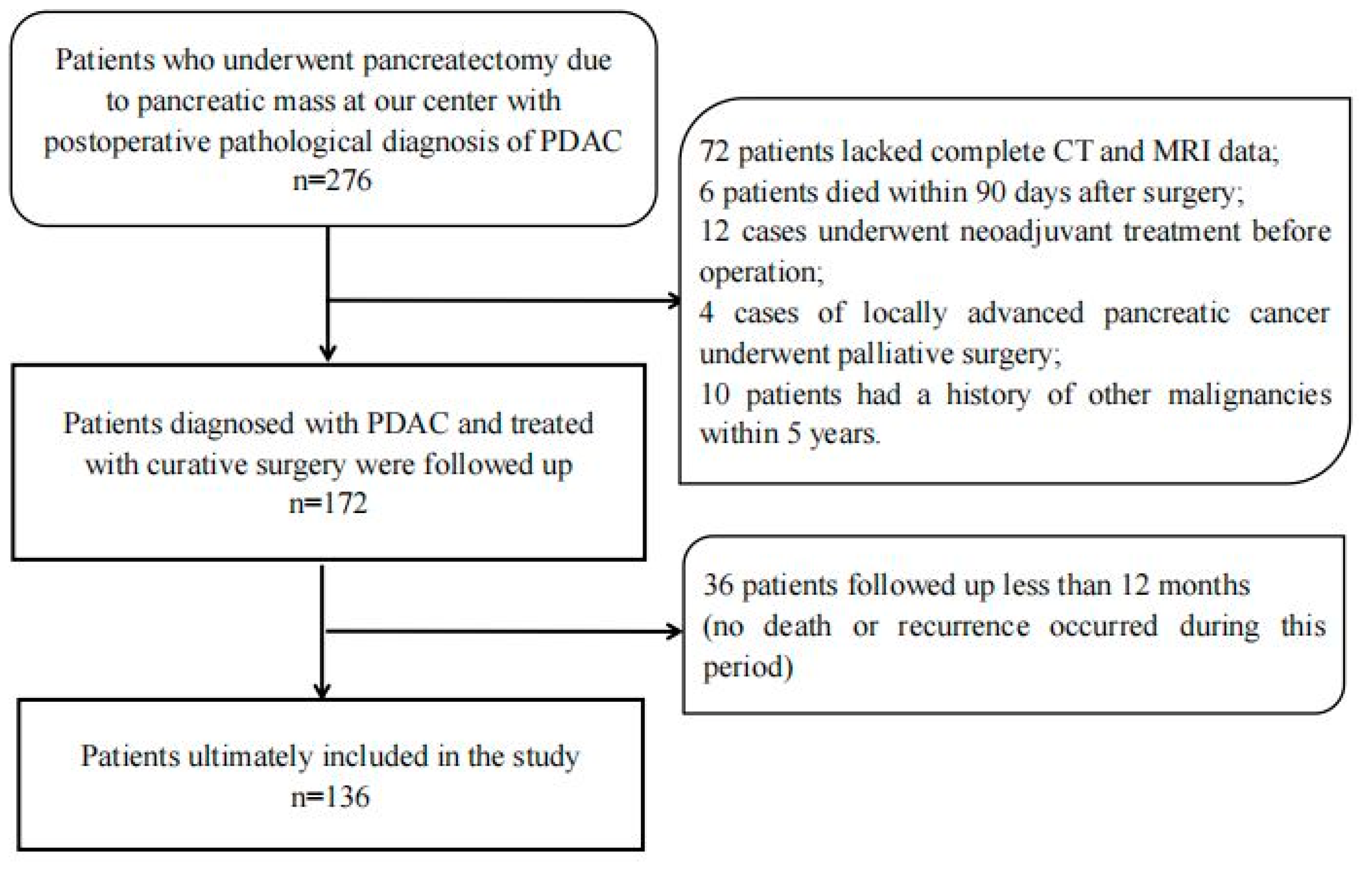
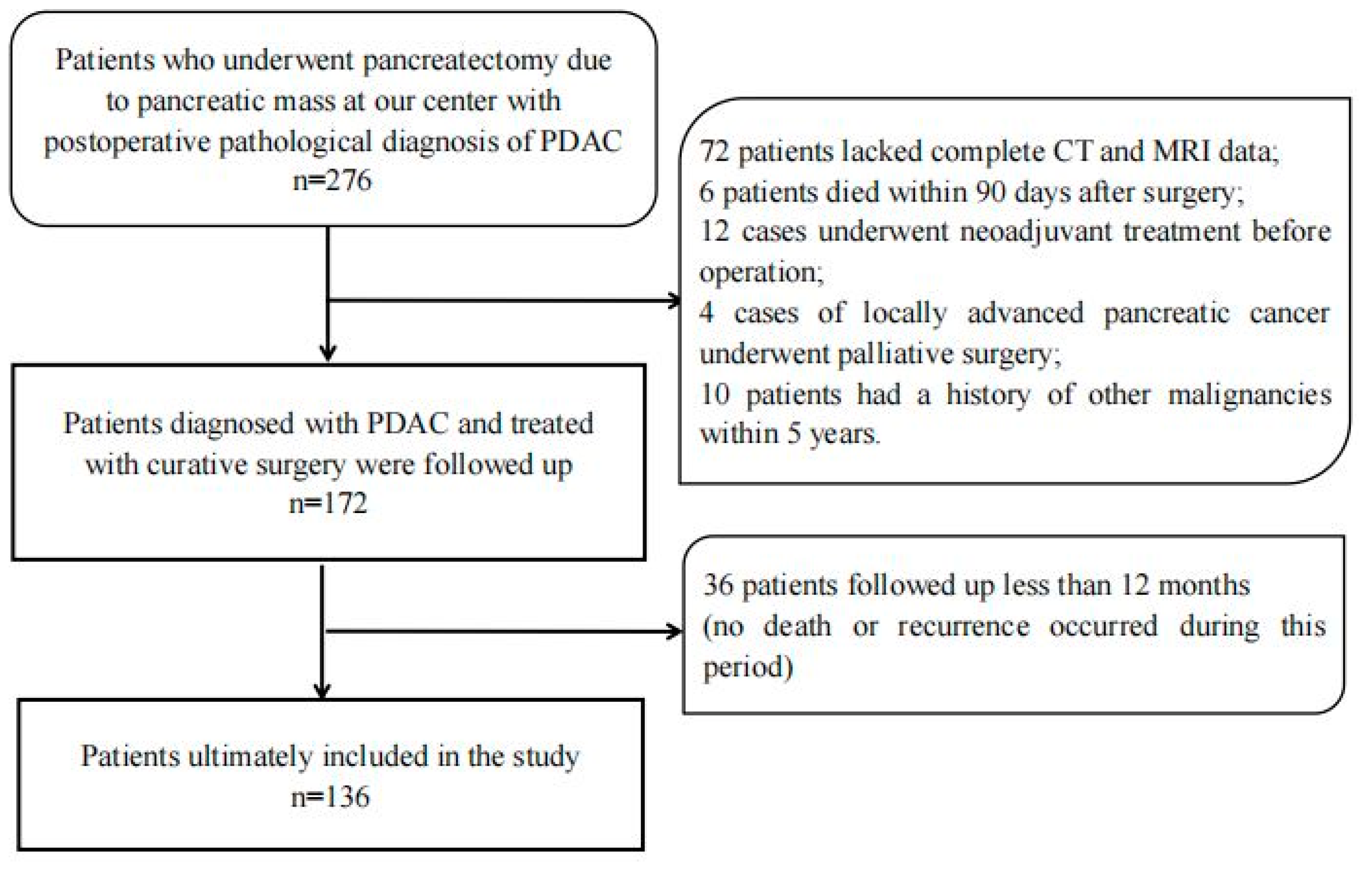
2.1. Patients
2.2. Magnetic Resonance Imaging Techniques
2.3. DWI Analysis
2.4. Clinicopathological Findings
2.5. Follow Up
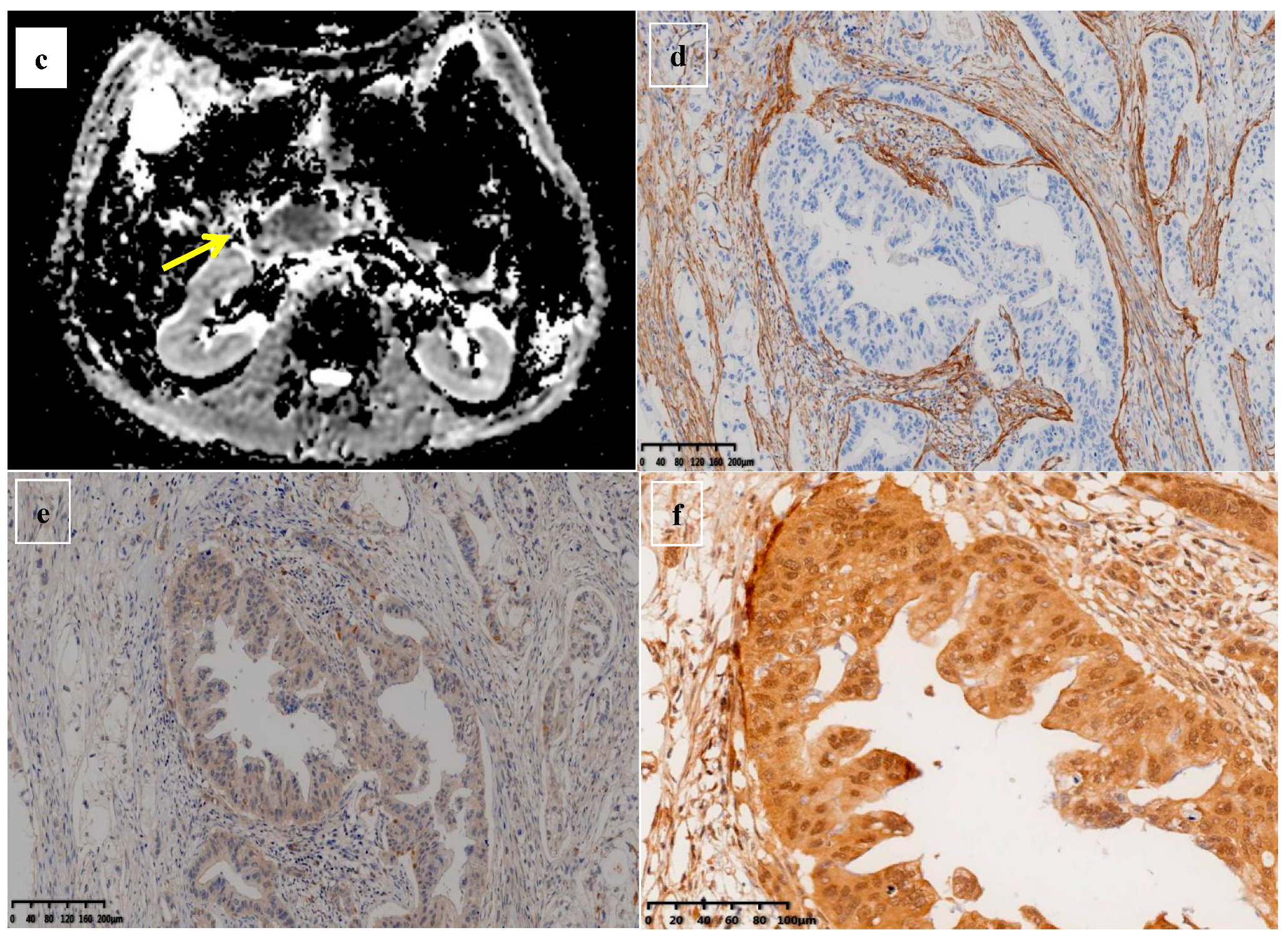
2.6. Immunohistochemical Staining and Quantification
2.7. Statistical Analysis
3. Results
3.1. Demographic and Clinicopathological Characteristics
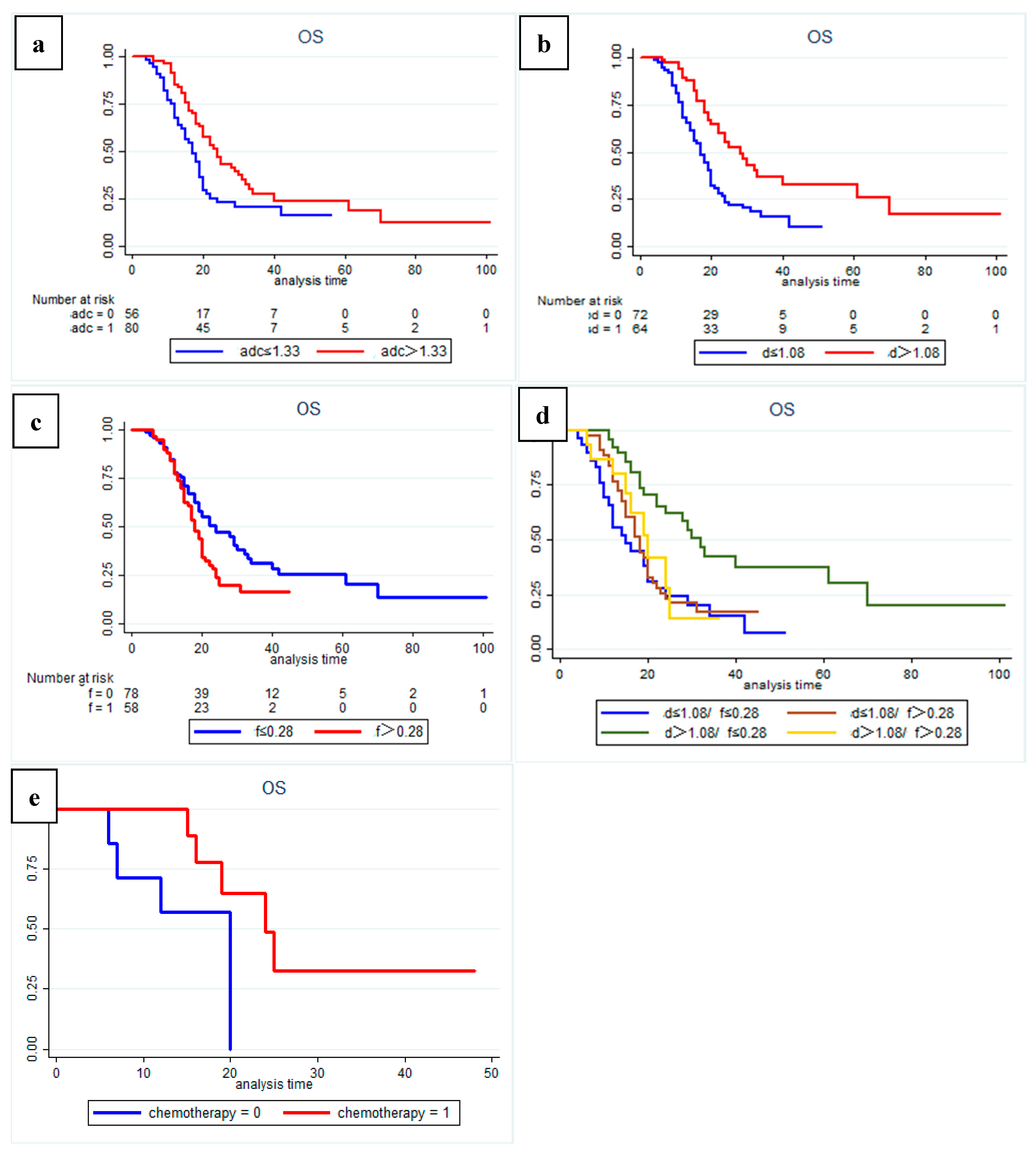
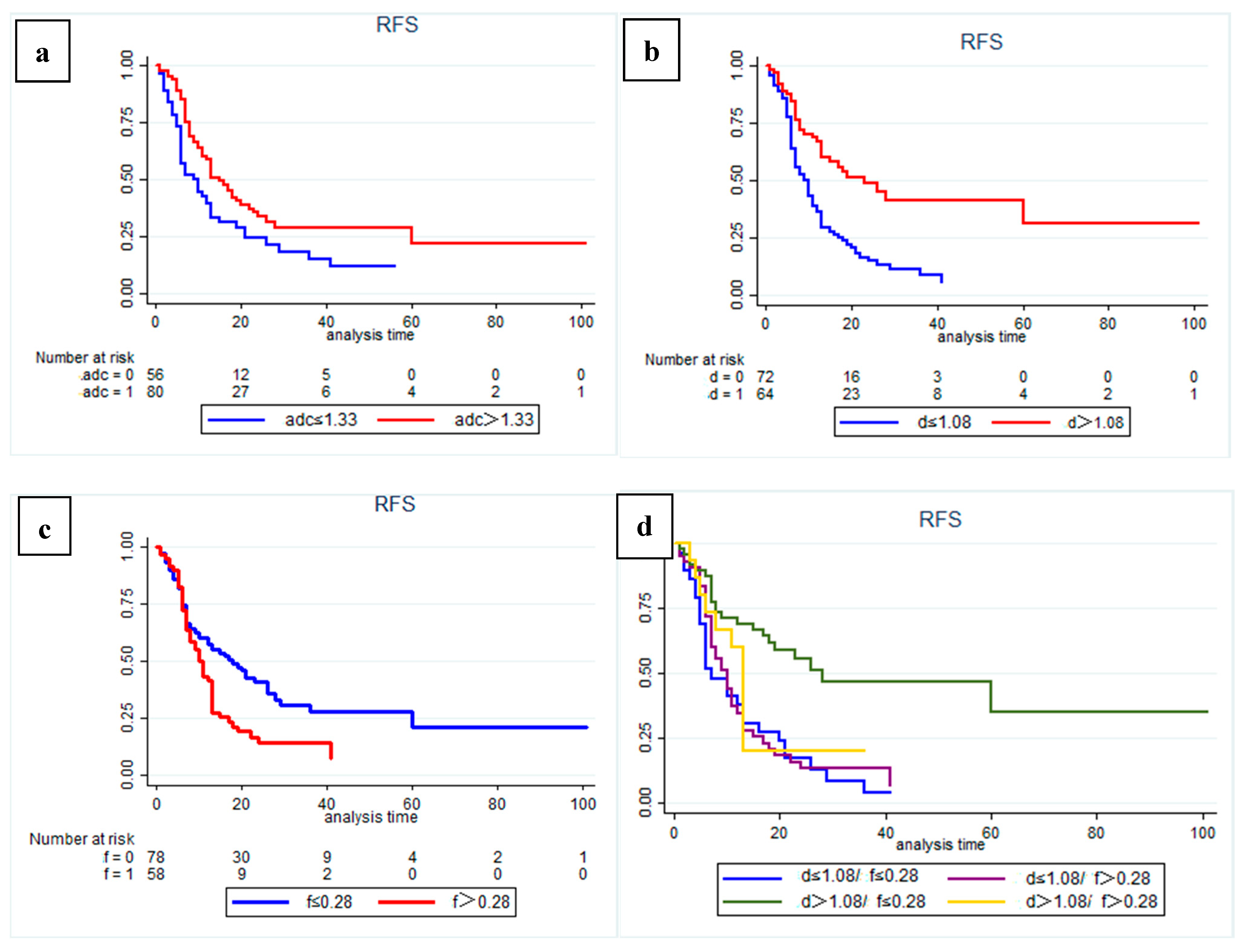
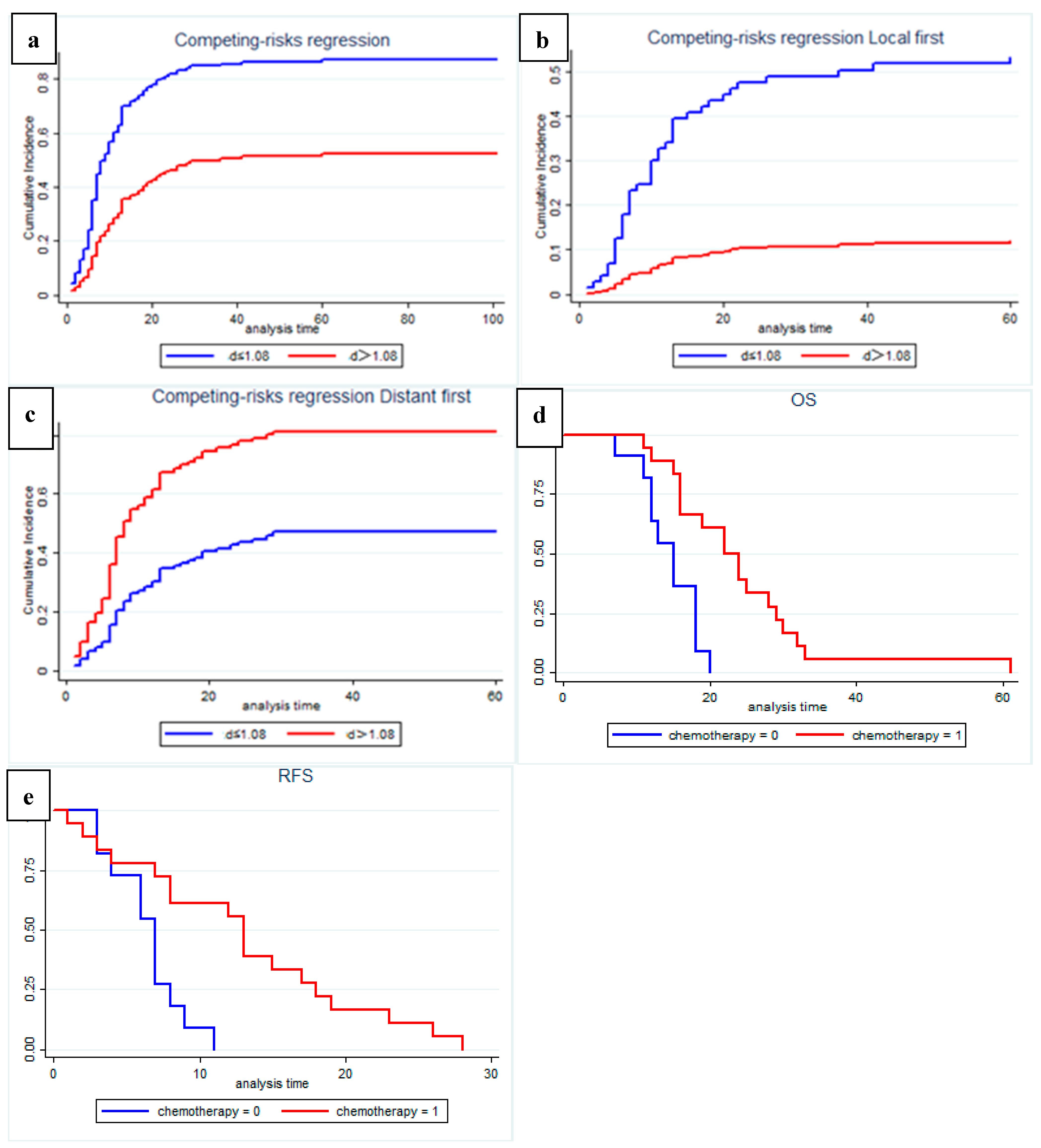
3.2. Quantitative MRI Correlates with Survival Outcomes
3.3. Quantitative MRI Correlates with Recurrence Pattern
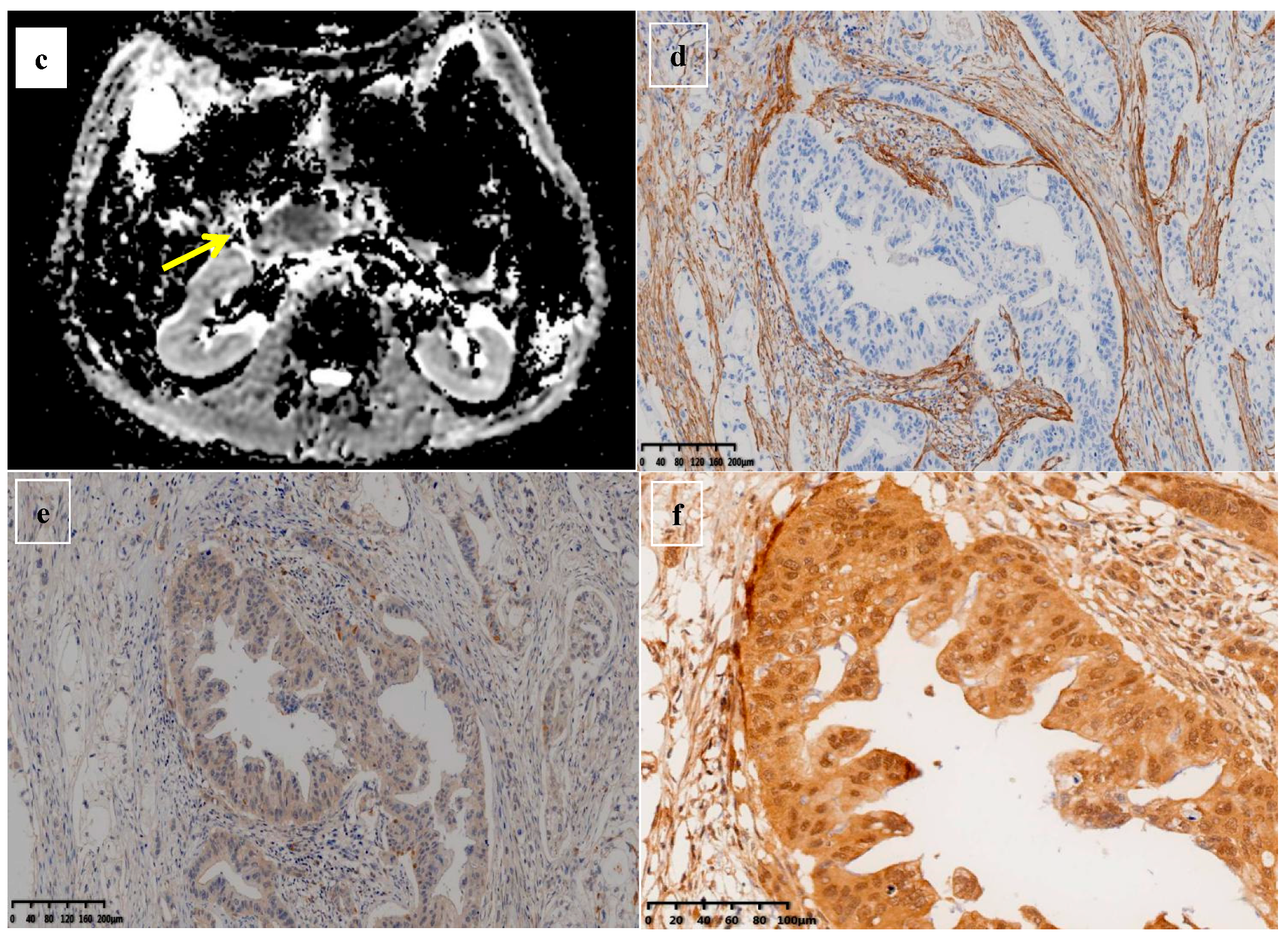
3.4. Quantitative MRI Correlates with Histopathology
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA A Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA A Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Winter, J.M.; Cameron, J.L.; Campbell, K.A.; Arnold, M.A.; Chang, D.C.; Coleman, J.; Hodgin, M.B.; Sauter, P.K.; Hruban, R.H.; Riall, T.S.; et al. 1423 pancreaticoduodenectomies for pancreatic cancer: A single-institution experience. J. Gastrointest. Surg. 2006, 10, 1199–1210, discussion 1210–1211. [Google Scholar] [CrossRef] [PubMed]
- Garcea, G.; Dennison, A.R.; Pattenden, C.J.; Neal, C.P.; Sutton, C.D.; Berry, D.P. Survival following curative resection for pancreatic ductal adenocarcinoma. A systematic review of the literature. JOP 2008, 9, 99–132. [Google Scholar]
- Ge, J.; Tao, M.; Li, L.; Ma, Z.; Jiang, B.; Yuan, C.; Wang, H.; Peng, Y.; Xiu, D. Nomogram and competing risk model to predict recurrence after curative surgical resection of PDAC. Pancreatology 2021, 21, 1102–1111. [Google Scholar] [CrossRef]
- Parikh, T.; Drew, S.J.; Lee, V.S.; Wong, S.; Hecht, E.M.; Babb, J.S.; Taouli, B. Focal liver lesion detection and characterization with diffusion-weighted MR imaging: Comparison with standard breath-hold T2-weighted imaging. Radiology 2008, 246, 812–822. [Google Scholar] [CrossRef]
- Chen, C.Y.; Li, C.W.; Kuo, Y.T.; Jaw, T.S.; Wu, D.K.; Jao, J.C.; Hsu, J.S.; Liu, G.C. Early response of hepatocellular carcinoma to transcatheter arterial chemoembolization: Choline levels and MR diffusion constants--initial experience. Radiology 2006, 239, 448–456. [Google Scholar] [CrossRef]
- Tahmassebi, A.; Wengert, G.J.; Helbich, T.H.; Bago-Horvath, Z.; Alaei, S.; Bartsch, R.; Dubsky, P.; Baltzer, P.; Clauser, P.; Kapetas, P.; et al. Impact of Machine Learning With Multiparametric Magnetic Resonance Imaging of the Breast for Early Prediction of Response to Neoadjuvant Chemotherapy and Survival Outcomes in Breast Cancer Patients. Investig. Radiol. 2019, 54, 110–117. [Google Scholar] [CrossRef]
- Qu, C.; Zeng, P.E.; Wang, H.Y.; Yuan, C.H.; Yuan, H.S.; Xiu, D.R. Application of Magnetic Resonance Imaging in Neoadjuvant Treatment of Pancreatic Ductal Adenocarcinoma. J. Magn. Reson. Imaging 2022, 55, 1625–1632. [Google Scholar] [CrossRef]
- Higano, S.; Yun, X.; Kumabe, T.; Watanabe, M.; Mugikura, S.; Umetsu, A.; Sato, A.; Yamada, T.; Takahashi, S. Malignant astrocytic tumors: Clinical importance of apparent diffusion coefficient in prediction of grade and prognosis. Radiology 2006, 241, 839–846. [Google Scholar] [CrossRef]
- Groot, V.P.; Rezaee, N.; Wu, W.; Cameron, J.L.; Fishman, E.K.; Hruban, R.H.; Weiss, M.J.; Zheng, L.; Wolfgang, C.L.; He, J. Patterns, Timing, and Predictors of Recurrence Following Pancreatectomy for Pancreatic Ductal Adenocarcinoma. Ann. Surg. 2018, 267, 936–945. [Google Scholar] [CrossRef] [PubMed]
- Hecht, E.M.; Liu, M.Z.; Prince, M.R.; Jambawalikar, S.; Remotti, H.E.; Weisberg, S.W.; Garmon, D.; Lopez-Pintado, S.; Woo, Y.; Kluger, M.D.; et al. Can diffusion-weighted imaging serve as a biomarker of fibrosis in pancreatic adenocarcinoma? J. Magn. Reson. Imaging 2017, 46, 393–402. [Google Scholar] [CrossRef]
- Mizutani, Y.; Kobayashi, H.; Iida, T.; Asai, N.; Masamune, A.; Hara, A.; Esaki, N.; Ushida, K.; Mii, S.; Shiraki, Y.; et al. Meflin-Positive Cancer-Associated Fibroblasts Inhibit Pancreatic Carcinogenesis. Cancer Res. 2019, 79, 5367–5381. [Google Scholar] [CrossRef] [PubMed]
- Sipos, B.; Weber, D.; Ungefroren, H.; Kalthoff, H.; Zühlsdorff, A.; Luther, C.; Török, V.; Klöppel, G. Vascular endothelial growth factor mediated angiogenic potential of pancreatic ductal carcinomas enhanced by hypoxia: Anin vitro andin vivo study. Int. J. Cancer 2002, 102, 592–600. [Google Scholar] [CrossRef]
- Yankeelov, T.E.; Arlinghaus, L.R.; Li, X.; Gore, J.C. The role of magnetic resonance imaging biomarkers in clinical trials of treatment response in cancer. Semin. Oncol. 2011, 38, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Padhani, A.R. Diffusion magnetic resonance imaging in cancer patient management. Semin. Radiat. Oncol. 2011, 21, 119–140. [Google Scholar] [CrossRef]
- Muraoka, N.; Uematsu, H.; Kimura, H.; Imamura, Y.; Fujiwara, Y.; Murakami, M.; Yamaguchi, A.; Itoh, H. Apparent diffusion coefficient in pancreatic cancer: Characterization and histopathological correlations. J. Magn. Reson. Imaging 2008, 27, 1302–1308. [Google Scholar] [CrossRef]
- Hayano, K.; Miura, F.; Amano, H.; Toyota, N.; Wada, K.; Kato, K.; Sano, K.; Takeshita, K.; Aoyagi, T.; Shuto, K.; et al. Correlation of apparent diffusion coefficient measured by diffusion-weighted MRI and clinicopathologic features in pancreatic cancer patients. J. Hepato-Biliary-Pancreat. Sci. 2013, 20, 243–248. [Google Scholar] [CrossRef]
- Padhani, A.R.; Liu, G.; Koh, D.M.; Chenevert, T.L.; Thoeny, H.C.; Takahara, T.; Dzik-Jurasz, A.; Ross, B.D.; Van Cauteren, M.; Collins, D.; et al. Diffusion-weighted magnetic resonance imaging as a cancer biomarker: Consensus and recommendations. Neoplasia 2009, 11, 102–125. [Google Scholar] [CrossRef]
- Ma, W.; Li, N.; Zhao, W.; Ren, J.; Wei, M.; Yang, Y.; Wang, Y.; Fu, X.; Zhang, Z.; Larson, A.C.; et al. Apparent Diffusion Coefficient and Dynamic Contrast-Enhanced Magnetic Resonance Imaging in Pancreatic Cancer. J. Comput. Assist. Tomogr. 2016, 40, 709–716. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Chen, Z.E.; Nikolaidis, P.; McCarthy, R.J.; Merrick, L.; Sternick, L.A.; Horowitz, J.M.; Yaghmai, V.; Miller, F.H. Diffusion-weighted magnetic resonance imaging of pancreatic adenocarcinomas: Association with histopathology and tumor grade. J. Magn. Reson. Imaging 2011, 33, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Lyng, H.; Haraldseth, O.; Rofstad, E.K. Measurement of cell density and necrotic fraction in human melanoma xenografts by diffusion weighted magnetic resonance imaging. Magn. Reson. Med. 2000, 43, 828–836. [Google Scholar] [CrossRef]
- Harimoto, N.; Araki, K.; Hoshino, K.; Muranushi, R.; Hagiwara, K.; Ishii, N.; Tsukagoshi, M.; Igarashi, T.; Watanabe, A.; Kubo, N.; et al. Diffusion-Weighted MRI Predicts Lymph Node Metastasis and Tumor Aggressiveness in Resectable Pancreatic Neuroendocrine Tumors. World J. Surg. 2020, 44, 4136–4141. [Google Scholar] [CrossRef]
- Micco, M.; Vargas, H.A.; Burger, I.A.; Kollmeier, M.A.; Goldman, D.A.; Park, K.J.; Abu-Rustum, N.R.; Hricak, H.; Sala, E. Combined pre-treatment MRI and 18F-FDG PET/CT parameters as prognostic biomarkers in patients with cervical cancer. Eur. J. Radiol. 2014, 83, 1169–1176. [Google Scholar] [CrossRef]
- Pope, W.B.; Qiao, X.J.; Kim, H.J.; Lai, A.; Nghiemphu, P.; Xue, X.; Ellingson, B.M.; Schiff, D.; Aregawi, D.; Cha, S.; et al. Apparent diffusion coefficient histogram analysis stratifies progression-free and overall survival in patients with recurrent GBM treated with bevacizumab: A multi-center study. J. Neurooncol. 2012, 108, 491–498. [Google Scholar] [CrossRef]
- Kurosawa, J.; Tawada, K.; Mikata, R.; Ishihara, T.; Tsuyuguchi, T.; Saito, M.; Shimofusa, R.; Yoshitomi, H.; Ohtsuka, M.; Miyazaki, M.; et al. Prognostic relevance of apparent diffusion coefficient obtained by diffusion-weighted MRI in pancreatic cancer. J. Magn. Reson. Imaging 2015, 42, 1532–1537. [Google Scholar] [CrossRef]
- Fukukura, Y.; Takumi, K.; Higashi, M.; Shinchi, H.; Kamimura, K.; Yoneyama, T.; Tateyama, A. Contrast-enhanced CT and diffusion-weighted MR imaging: Performance as a prognostic factor in patients with pancreatic ductal adenocarcinoma. Eur. J. Radiol. 2014, 83, 612–619. [Google Scholar] [CrossRef]
- Garces-Descovich, A.; Morrison, T.C.; Beker, K.; Jaramillo-Cardoso, A.; Moser, A.J.; Mortele, K.J. DWI of Pancreatic Ductal Adenocarcinoma: A Pilot Study to Estimate the Correlation With Metastatic Disease Potential and Overall Survival. Am. J. Roentgenol. (1976) 2019, 212, 323. [Google Scholar] [CrossRef]
- Nishiofuku, H.; Tanaka, T.; Marugami, N.; Sho, M.; Akahori, T.; Nakajima, Y.; Kichikawa, K. Increased tumour ADC value during chemotherapy predicts improved survival in unresectable pancreatic cancer. Eur. Radiol. 2016, 26, 1835–1842. [Google Scholar] [CrossRef]
- Senthebane, D.A.; Rowe, A.; Thomford, N.E.; Shipanga, H.; Munro, D.; Mazeedi, M.; Almazyadi, H.; Kallmeyer, K.; Dandara, C.; Pepper, M.S.; et al. The Role of Tumor Microenvironment in Chemoresistance: To Survive, Keep Your Enemies Closer. Int. J. Mol. Sci. 2017, 18, 1586. [Google Scholar] [CrossRef] [Green Version]
- Yuen, A.; Diaz, B. The impact of hypoxia in pancreatic cancer invasion and metastasis. Hypoxia 2014, 2, 91–106. [Google Scholar] [PubMed]
- Mayer, P.; Kraft, A.; Witzel, H.R.; Marnet, N.; Hörner, N.; Roth, W.; Heinrich, S.; Hackert, T.; Bergmann, F.; Kauczor, H.; et al. Restricted Water Diffusion in Diffusion-Weighted Magnetic Resonance Imaging in Pancreatic Cancer is Associated with Tumor Hypoxia. Cancers 2021, 13, 89. [Google Scholar] [CrossRef] [PubMed]
- Iima, M.; Le Bihan, D. Clinical Intravoxel Incoherent Motion and Diffusion MR Imaging: Past, Present, and Future. Radiology 2016, 278, 13–32. [Google Scholar] [CrossRef] [PubMed]
- Koh, D.M.; Collins, D.J.; Orton, M.R. Intravoxel incoherent motion in body diffusion-weighted MRI: Reality and challenges. AJR Am. J. Roentgenol. 2011, 196, 1351–1361. [Google Scholar] [CrossRef]
- Klaassen, R.; Steins, A.; Gurney Champion, O.J.; Bijlsma, M.F.; Tienhoven, G.; Engelbrecht, M.R.W.; Eijck, C.H.J.; Suker, M.; Wilmink, J.W.; Besselink, M.G.; et al. Pathological validation and prognostic potential of quantitative MRI in the characterization of pancreas cancer: Preliminary experience. Mol. Oncol. 2020, 14, 2176–2189. [Google Scholar] [CrossRef]
- Rong, D.; Mao, Y.; Hu, W.; Xu, S.; Wang, J.; He, H.; Li, S.; Zhang, R. Intravoxel incoherent motion magnetic resonance imaging for differentiating metastatic and non-metastatic lymph nodes in pancreatic ductal adenocarcinoma. Eur Radiol 2018, 28, 2781–2789. [Google Scholar] [CrossRef]
- Korc, M. Pancreatic cancer–associated stroma production. Am. J. Surg. 2007, 194, S84–S86. [Google Scholar] [CrossRef]
- Northey, J.J.; Przybyla, L.; Weaver, V.M. Tissue Force Programs Cell Fate and Tumor Aggression. Cancer Discov. 2017, 7, 1224–1237. [Google Scholar] [CrossRef]
- Neesse, A.; Bauer, C.A.; Ohlund, D.; Lauth, M.; Buchholz, M.; Michl, P.; Tuveson, D.A.; Gress, T.M. Stromal biology and therapy in pancreatic cancer: Ready for clinical translation? Gut 2019, 68, 159–171. [Google Scholar] [CrossRef]
- Mayer, P.; Fritz, F.; Koell, M.; Skornitzke, S.; Bergmann, F.; Gaida, M.M.; Hackert, T.; Maier-Hein, K.; Laun, F.B.; Kauczor, H.; et al. Assessment of tissue perfusion of pancreatic cancer as potential imaging biomarker by means of Intravoxel incoherent motion MRI and CT perfusion: Correlation with histological microvessel density as ground truth. Cancer Imaging 2021, 21, 13. [Google Scholar] [CrossRef]
- Lewin, M.; Fartoux, L.; Vignaud, A.; Arrivé, L.; Menu, Y.; Rosmorduc, O. The diffusion-weighted imaging perfusion fraction f is a potential marker of sorafenib treatment in advanced hepatocellular carcinoma: A pilot study. Eur. Radiol. 2011, 21, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Klau, M.; Mayer, P.; Bergmann, F.; Maier-Hein, K.; Hase, J.; Hackert, T.; Kauczor, H.U.; Grenacher, L.; Stieltjes, B. Correlation of Histological Vessel Characteristics and Diffusion-Weighted Imaging Intravoxel Incoherent Motion-Derived Parameters in Pancreatic Ductal Adenocarcinomas and Pancreatic Neuroendocrine Tumors. Investig. Radiol. 2015, 50, 792–797. [Google Scholar] [CrossRef] [PubMed]
- Fujioka, S.; Yoshida, K.; Yanagisawa, S.; Kawakami, M.; Aoki, T.; Yamazaki, Y. Angiogenesis in pancreatic carcinoma: Thymidine phosphorylase expression in stromal cells and intratumoral microvessel density as independent predictors of overall and relapse-free survival. Cancer-Am. Cancer Soc. 2001, 92, 1788–1797. [Google Scholar] [CrossRef]
- Benckert, C.; Thelen, A.; Cramer, T.; Weichert, W.; Gaebelein, G.; Gessner, R.; Jonas, S. Impact of microvessel density on lymph node metastasis and survival after curative resection of pancreatic cancer. Surg. Today 2012, 42, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Lemke, A.; Stieltjes, B.; Schad, L.R.; Laun, F.B. Toward an optimal distribution of b values for intravoxel incoherent motion imaging. Magn. Reson. Imaging 2011, 29, 766–776. [Google Scholar] [CrossRef] [PubMed]
- Barral, M.; Taouli, B.; Guiu, B.; Koh, D.M.; Luciani, A.; Manfredi, R.; Vilgrain, V.; Hoeffel, C.; Kanematsu, M.; Soyer, P. Diffusion-weighted MR imaging of the pancreas: Current status and recommendations. Radiology 2015, 274, 45–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | No. of Patients (%) (n = 136) |
|---|---|
| Age (years) | 65 ± 9.1 |
| Sex | |
| Male | 74 (54.4%) |
| Female | 62 (45.5%) |
| CEA (ng/mL) | |
| Normal (≤5) | 97 (71.3%) |
| Elevated (>5) | 39 (28.7%) |
| CA19-9 (U/mL) | |
| Normal (≤39) | 22 (16.2%) |
| Elevated (>39) | 114 (83.8%) |
| After surgery CA19-9 (U/mL) | |
| Normal (≤39) | 69 (50.7%) |
| Elevated (>39) | 67 (49.3%) |
| Type of surgery | |
| TP | 8 (5.9%) |
| PD | 86 (63.2%) |
| DP | 42 (30.9%) |
| Tumor location | |
| Head | 90 (66.2%) |
| Body | 8 (5.9%) |
| Tail | 38 (27.9%) |
| Tumor size (cm) | |
| ≤2 | 22 (16.2%) |
| 2–4 | 86 (63.2%) |
| >4 | 28 (20.6%) |
| N stage | |
| N0 | 76 (55.9%) |
| N1 | 48 (35.3%) |
| N2 | 12 (8.8%) |
| AJCC stage, 8th | |
| IA | 15 (11.0%) |
| IB | 50 (36.8%) |
| IIA | 10 (7.4%) |
| IIB | 48 (35.3%) |
| III | 13 (9.6%) |
| Baseline resectability | |
| Resectable | 91 (66.9%) |
| Borderline resectable | 45 (33.1%) |
| Margin | |
| R0 | 94 (69.1%) |
| R1 | 42 (30.9%) |
| Nerve invasion | |
| (+) | 17 (12.5%) |
| (−) | 119 (87.5%) |
| Adjuvant Chemotherapy | |
| Yes | 82 (60.3%) |
| No | 54 (41.9%) |
| Recurrence | |
| Distant first | 59 (43.4%) |
| Local first | 39 (28.7%) |
| ADC (×10−3 mm2 /s) | |
| ≤1.33 | 56 (41.2%) |
| >1.33 | 80 (58.8%) |
| D (×10−3 mm2 /s) | |
| ≤1.08 | 72 (52.9%) |
| >1.08 | 64 (47.1%) |
| D* (×10−3 mm2 /s) | |
| ≤7.94 | 40 (29.4%) |
| >7.94 | 96 (70.6%) |
| f | |
| ≤0.28 | 78 (57.4%) |
| >0.28 | 58 (42.6%) |
| DDC | |
| ≤1.5 | 90 (66.2%) |
| >1.5 | 46 (33.8%) |
| α | |
| ≤0.86 | 105 (77.2%) |
| >0.86 | 31 (22.8%) |
| Variables | Category | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | ||
| Age (years) | <65 vs. ≥65 | 0.777 (0.514, 1.176) | 0.234 | ||
| Sex | Male vs. Female | 1.167 (0.772, 1.765) | 0.463 | ||
| CEA (ng/mL) | ≤5 vs. >5 | 1.271 (0.715, 2.260) | 0.415 | ||
| CA19-9 (U/mL) | ≤39 vs. >39 | 1.068 (0.622, 1.835) | 0.810 | ||
| After surgery CA19-9 (U/mL) | ≤39 vs. >39 | 1.425 (0.941, 2.151) | 0.094 | - | |
| Type of surgery | PD | Ref | |||
| DP | 1.197 (0.764, 1.875) | 0.434 | |||
| TP | 1.060 (0.457, 2.460) | 0.892 | |||
| Tumor location | Head | Ref | |||
| Body | 0.637 (0.231, 1.758) | 0.384 | |||
| Tail | 1.209 (0.767, 1.907) | 0.414 | |||
| Tumor size (cm) | ≤2 | Ref | Ref | ||
| 2–4 | 1.947 (0.994, 3.812) | 0.052 | 1.845 (0.937, 3.630) | 0.076 | |
| >4 | 3.296 (1.551, 7.003) | 0.002 | 2.559 (1.185, 5.524) | 0.017 | |
| N stage | N0 | Ref | |||
| N1 | 1.452 (0.945, 2.230) | 0.088 | |||
| N2 | 1.383 (0.674, 2.837) | 0.377 | |||
| AJCC stage, 8th | IA | Ref | |||
| IB | 1.986 (0.829, 4.761) | 0.124 | |||
| IIA | 2.715 (0.824, 8.944) | 0.101 | |||
| IIB | 2.625 (1.123, 6.263) | 0.026 | |||
| III | 2.726 (0.989, 7.517) | 0.053 | |||
| Baseline resectability | Resectable vs. Borderline | 1.321 (0.869, 2.614) | 0.231 | ||
| Margin | R0 vs. R1 | 1.594 (1.034, 2.457) | 0.035 | 1.515 (0.970, 2.365) | 0.068 |
| Nerve invasion | (+) vs. (−) | 1.057 (0.587, 1.905) | 0.853 | ||
| Adjuvant Chemotherapy | Yes vs. No | 0.686 (0.451, 1.043) | 0.078 | ||
| ADC (×10−3 mm2/s) | >1.33 vs. ≤1.33 | 1.701 (1.123, 2.577) | 0.012 | 1.336 (0.831, 2.149) | 0.232 |
| D (×10−3 mm2/s) | >1.08 vs. ≤1.08 | 2.189 (1.417, 3.381) | 0.001 | 1.696 (1.003, 2.869) | 0.049 |
| D* (×10−3 mm2/s) | >7.94 vs. ≤7.94 | 1.070 (0.681, 1.682) | 0.768 | ||
| f | >0.28 vs. ≤0.28 | 0.642 (0.424, 0.973) | 0.037 | 0.859 (0.530, 1.393) | 0.538 |
| DDC | >1.5 vs. ≤1.5 | 1.299 (0.839, 2.010) | 0.240 | ||
| α | >0.86 vs. ≤0.86 | 1.566 (0.922, 2.659) | 0.097 | ||
| α-SMA | VEGF | HIF-1α | ADC | D | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| r | p | r | p | r | p | r | p | r | p | |
| VEGF | 0.017 | 0.849 | ||||||||
| HIF-1α | 0.207 | 0.018 | −0.060 | 0.501 | ||||||
| ADC | −0.208 | 0.019 | 0.149 | 0.096 | −0.320 | 0.002 | ||||
| D | −0.475 | 0.000 | −0.078 | 0.380 | −0.304 | 0.000 | 0.512 | 0.000 | ||
| f | 0.341 | 0.001 | 0.206 | 0.020 | −0.096 | 0.282 | 0.129 | 0.147 | −0.464 | 0.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qu, C.; Zeng, P.; Wang, H.; Guo, L.; Zhang, L.; Yuan, C.; Yuan, H.; Xiu, D. Preoperative Multiparametric Quantitative Magnetic Resonance Imaging Correlates with Prognosis and Recurrence Patterns in Pancreatic Ductal Adenocarcinoma. Cancers 2022, 14, 4243. https://doi.org/10.3390/cancers14174243
Qu C, Zeng P, Wang H, Guo L, Zhang L, Yuan C, Yuan H, Xiu D. Preoperative Multiparametric Quantitative Magnetic Resonance Imaging Correlates with Prognosis and Recurrence Patterns in Pancreatic Ductal Adenocarcinoma. Cancers. 2022; 14(17):4243. https://doi.org/10.3390/cancers14174243
Chicago/Turabian StyleQu, Chao, Piaoe Zeng, Hangyan Wang, Limei Guo, Lingfu Zhang, Chunhui Yuan, Huishu Yuan, and Dianrong Xiu. 2022. "Preoperative Multiparametric Quantitative Magnetic Resonance Imaging Correlates with Prognosis and Recurrence Patterns in Pancreatic Ductal Adenocarcinoma" Cancers 14, no. 17: 4243. https://doi.org/10.3390/cancers14174243
APA StyleQu, C., Zeng, P., Wang, H., Guo, L., Zhang, L., Yuan, C., Yuan, H., & Xiu, D. (2022). Preoperative Multiparametric Quantitative Magnetic Resonance Imaging Correlates with Prognosis and Recurrence Patterns in Pancreatic Ductal Adenocarcinoma. Cancers, 14(17), 4243. https://doi.org/10.3390/cancers14174243