
Impressive Results after “Metabolism-Guided” Lattice Irradiation in Patients Submitted to Palliative Radiation Therapy: Preliminary Results of LATTICE_01 Multicenter Study

 ,
,  , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Eligibility Criteria and Pretreatment Evaluation
2.2. Treatment
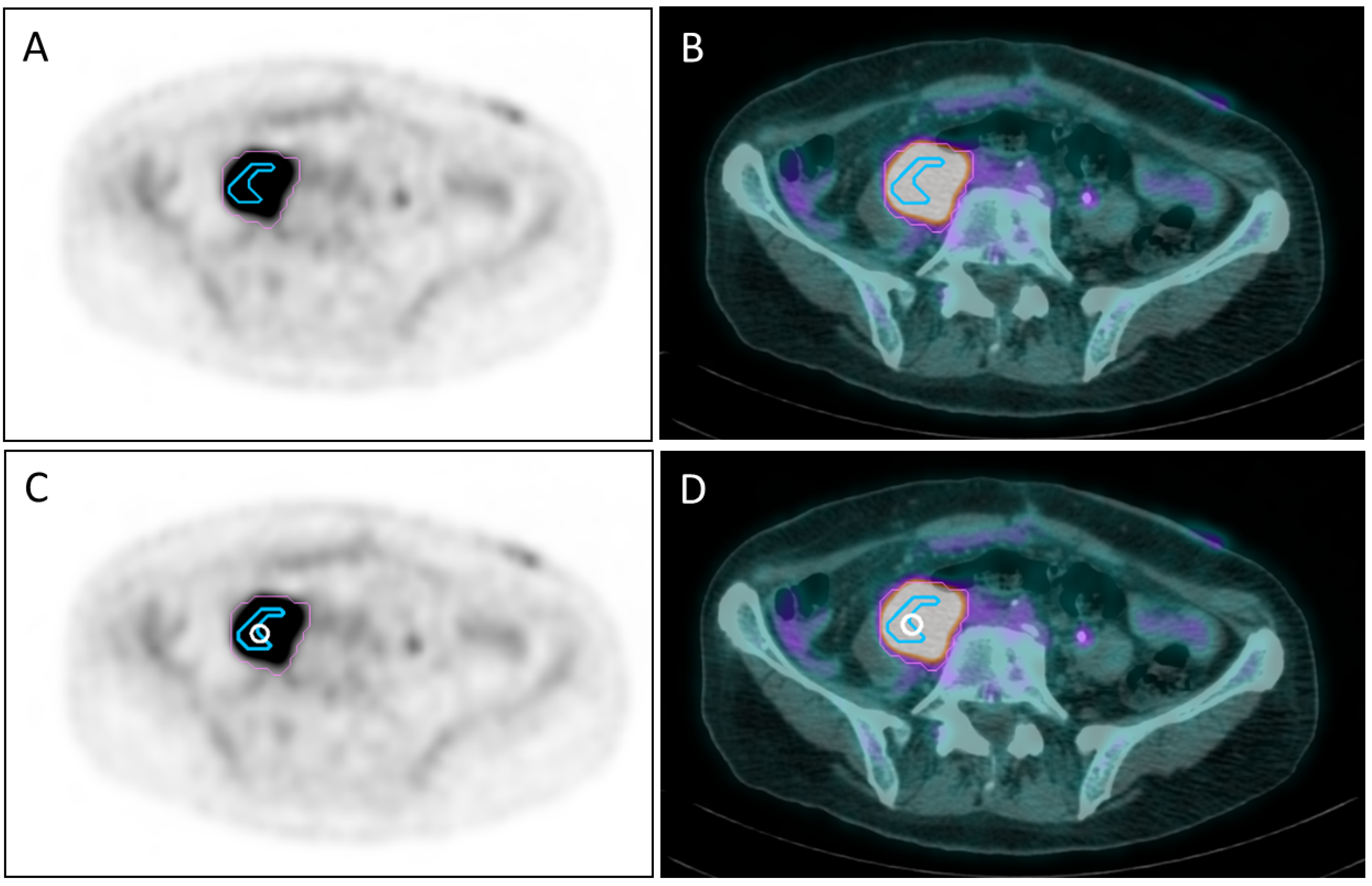
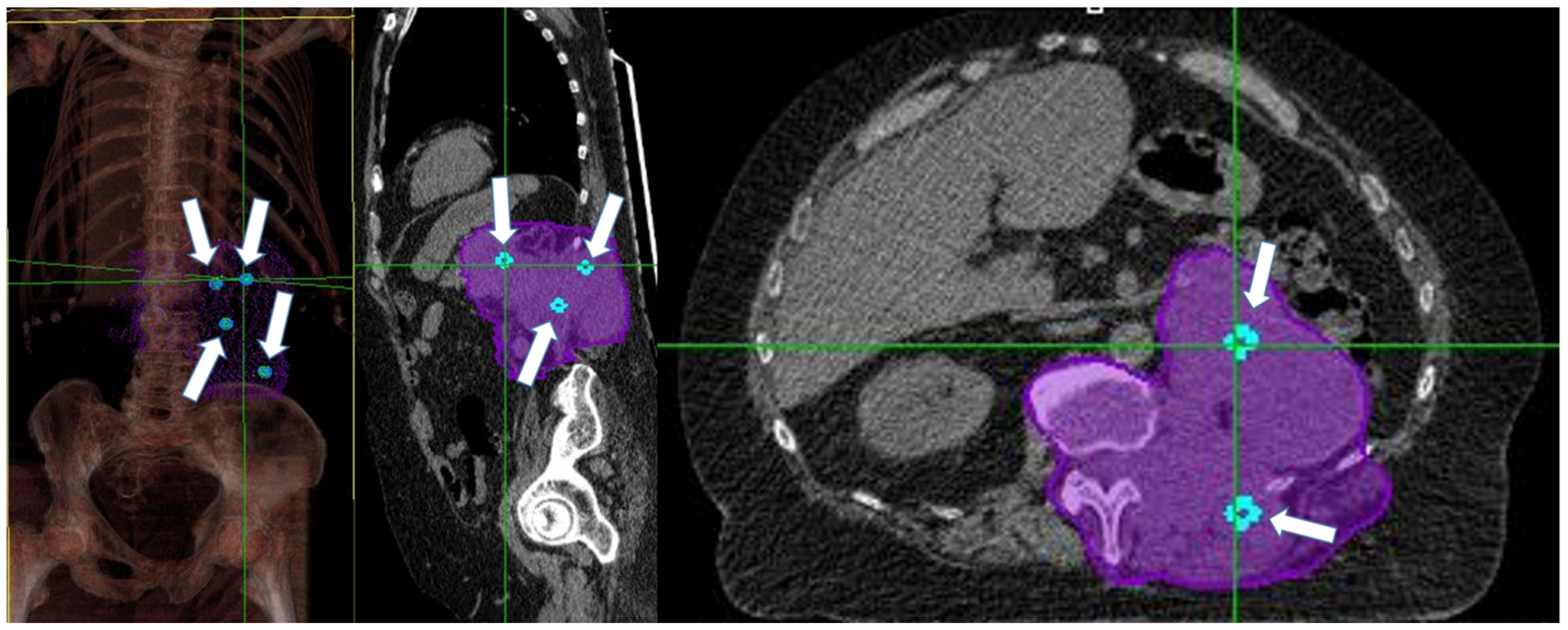
2.2.1. Vertex Positioning and Treatment Planning for Bulky Disease
2.2.2. Treatment Scheme
2.3. Endpoints
Evaluation of Toxicities and Response Assessment
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Spencer, K.; Parrish, R.; Barton, R.; Henry, A. Palliative radiotherapy. BMJ 2018, 360, k821. [Google Scholar] [CrossRef] [PubMed]
- Griffin, R.J.; Ahmed, M.M.; Amendola, B.; Belyakov, O.; Bentzen, S.M.; Butterworth, K.T.; Chang, S.; Coleman, C.N.; Djonov, V.; Formenti, S.C.; et al. Understanding High-Dose, Ultra-High Dose Rate, and Spatially Fractionated Radiation Therapy. Int. J. Radiat. Oncol. 2020, 107, 766–778. [Google Scholar] [CrossRef] [PubMed]
- Mohiuddin, M.; Fujita, M.; Regine, W.F.; Megooni, A.S.; Ibbott, G.S.; Ahmed, M.M. High-dose spatially-fractionated radiation (GRID): A new paradigm in the management of advanced cancers. Int. J. Radiat. Oncol. Biol. Phys. 1999, 45, 721–727. [Google Scholar] [CrossRef]
- Amendola, B.E.; Perez, N.C.; Mayr, N.A.; Wu, X.; Amendola, M. Spatially fractionated radiation therapy using lattice radiation in far-advanced bulky cervical cancer: A clinical and molecular imaging and outcome study. Radiat. Res. 2020, 194, 724–736. [Google Scholar] [CrossRef]
- Duriseti, S.; Kavanaugh, J.A.; Szymanski, J.; Huang, Y.; Basarabescu, F.; Chaudhuri, A.; Henke, L.; Samson, P.; Lin, A.; Robinson, C.; et al. LITE SABR M1: A phase I trial of Lattice stereotactic body radiotherapy for large tumors. Radiother. Oncol. 2021, 167, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Neuner, G.; Mohiuddin, M.M.; Walde, N.V.; Goloubeva, O.; Ha, J.; Yu, C.X.; Regine, W.F. High-Dose Spatially Fractionated GRID Radiation Therapy (SFGRT): A Comparison of Treatment Outcomes With Cerrobend vs. MLC SFGRT. Int. J. Radiat. Oncol. 2012, 82, 1642–1649. [Google Scholar] [CrossRef]
- Eapen, L. Radiovaccination Hypothesis. Cureus 2017, 9, e1135. [Google Scholar] [CrossRef]
- Welz, S.; Paulsen, F.; Pfannenberg, C.; Reimold, M.; Reischl, G.; Nikolaou, K.; La Fougère, C.; Alber, M.; Belka, C.; Zips, D.; et al. Dose escalation to hypoxic subvolumes in head and neck cancer: A randomized phase II study using dynamic [18F]FMISO PET/CT. Radiother. Oncol. 2022, 171, 30–36. [Google Scholar] [CrossRef]
- Castorina, P.; Castorina, L.; Ferini, G. Non-homogeneous tumor growth and its implications for radiotherapy: A phenomenological approach. J. Pers. Med. 2021, 11, 527. [Google Scholar] [CrossRef]
- Ferini, G.; Valenti, V.; Tripoli, A.; Illari, S.; Molino, L.; Parisi, S.; Cacciola, A.; Lillo, S.; Giuffrida, D.; Pergolizzi, S. Lattice or Oxygen-Guided Radiotherapy: What If They Converge? Possible Future Directions in the Era of Immunotherapy. Cancers 2021, 13, 3290. [Google Scholar] [CrossRef]
- Busk, M.; Horsman, M.R.; Jakobsen, S.; Bussink, J.; van der Kogel, A.; Overgaard, J. Cellular uptake of PET tracers of glucose metabolism and hypoxia and their linkage. Eur. J. Nucl. Med. Mol. Imaging 2008, 35, 2294–2303. [Google Scholar] [CrossRef] [PubMed]
- Li, X.-F.; Du, Y.; Ma, Y.; Postel, G.C.; Civelek, A.C. 18F-Fluorodeoxyglucose uptake and tumor hypoxia: Re-visit 18F-fluorodeoxyglucose in oncology application. Translat. Oncol. 2014, 7, 240–247. [Google Scholar] [CrossRef] [PubMed]
- Herrera, F.G.; Bourhis, J.; Coukos, G. Radiotherapy combination opportunities leveraging immunity for the next oncology practice. CA Cancer J. Clin. 2016, 67, 65–85. [Google Scholar] [CrossRef] [PubMed]
- Portella, L.; Scala, S. Ionizing radiation effects on the tumor microenvironment. Semin. Oncol. 2019, 46, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Parisi, S.; Napoli, I.; Lillo, S.; Cacciola, A.; Ferini, G.; Iatì, G.; Pontoriero, A.; Tamburella, C.; Davì, V.; Pergolizzi, S. Spine eburnation in a metastatic lung cancer patient treated with immunotherapy and radiotherapy. The first case report of bystander effect on bone. J. Oncol. Pharm. Pr. 2021, 28, 237–241. [Google Scholar] [CrossRef]
- Tubin, S.; Popper, H.H.; Brcic, L. Novel stereotactic body radiation therapy (SBRT)-based partial tumor irradiation targeting hypoxic segment of bulky tumors (SBRT-PATHY): Improvement of the radiotherapy outcome by exploiting the bystander and abscopal effects. Radiat. Oncol. 2019, 14, 21. [Google Scholar] [CrossRef]
- Hanna, G.; Murray, L.; Patel, R.; Jain, S.; Aitken, K.; Franks, K.; van As, N.; Tree, A.; Hatfield, P.; Harrow, S.; et al. UK consensus on normal tissue dose constraints for stereotactic radiotherapy. Clin. Oncol. 2018, 30, 5–14. [Google Scholar] [CrossRef]
- Wu, X.; Perez, N.C.; Zheng, Y.; Li, X.; Jiang, L.; Amendola, B.E.; Xu, B.; Mayr, N.A.; Lu, J.J.; Hatoum, G.F.; et al. The Technical and Clinical Implementation of LATTICE Radiation Therapy (LRT). Radiat. Res. 2020, 194, 737–746. [Google Scholar] [CrossRef]
- Dincer, N.; Ugurluer, G.; Korkmaz, L.; Serkizyan, A.; Atalar, B.; Gungor, G.; Ozyar, E. Magnetic Resonance Imaging-Guided Online Adaptive Lattice Stereotactic Body Radiotherapy in Voluminous Liver Metastasis: Two Case Reports. Cureus 2022, 14, e23980. [Google Scholar] [CrossRef]
- Ferini, G.; Castorina, P.; Valenti, V.; Illari, S.I.; Sachpazidis, I.; Castorina, L.; Marrale, M.; Pergolizzi, S. A novel radiotherapeutic approach to treat bulky metastases even from cutaneous squamous cell carcinoma: Its rationale and a look at the reliability of the linear-quadratic model to explain its radiobiological effects. Front. Oncol. 2022, 12, 809279. [Google Scholar] [CrossRef]
- Jiang, L.; Li, X.; Zhang, J.; Li, W.; Dong, F.; Chen, C.; Lin, Q.; Zhang, C.; Zheng, F.; Yan, W.; et al. Combined high-dose LATTICE radiation therapy and immune checkpoint blockade for advanced bulky tumors: The concept and a case report. Front. Oncol. 2021, 10, 548132. [Google Scholar] [CrossRef] [PubMed]
- Parisi, S.; Ferini, G.; Pontoriero, A.; Viola, A.; Cacciola, A.; Lillo, S.; Ferrantelli, G.; Tamburella, C.; Giudice, G.L.; Valenti, V.; et al. PO-1462 High radiation dose delivery by lattice-rt to hypoxic areas in bulky tumours: A multicentric study. Radiother. Oncol. 2022, 170, S1241–S1242. [Google Scholar] [CrossRef]
- McDonald, R.; Chow, E.; Rowbottom, L.; DeAngelis, C.; Soliman, H. Incidence of pain flare in radiation treatment of bone metastases: A literature review. J. Bone Oncol. 2014, 3, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Amendola, B.E.; Perez, N.C.; Wu, X.; Amendola, M.A.; Qureshi, I.Z. Safety and efficacy of lattice radiotherapy in voluminous non-small cell lung cancer. Cureus 2019, 11, e4263. [Google Scholar] [CrossRef] [PubMed]
- Suarez, J.M.B.; E Amendola, B.; Perez, N.; Amendola, M.; Wu, X. The Use of Lattice Radiation Therapy (LRT) in the Treatment of Bulky Tumors: A Case Report of a Large Metastatic Mixed Mullerian Ovarian Tumor. Cureus 2015, 7, e389. [Google Scholar] [CrossRef]
- Collier, R. From bedside to bench and back again. Can. Med Assoc. J. 2011, 183, E323–E324. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Age (years) | |
|---|---|
| Median | 74.5 |
| Range | 42–91 |
| ECOG Status | |
| Median | 2 |
| Range | 0–2 |
| Sex | |
| Female | 10 |
| Male | 20 |
| Tumor-Related Symptoms | |
| Pain | 24 |
| Neuropathic pain | 3 |
| Palpable mass | 5 |
| No pain | 3 |
| VAS Score | |
| Median | 5 |
| Range | 0–10 |
| Histology | |
| Adenocarcinoma | 8 |
| Squamous cell carcinoma | 7 |
| Urothelial carcinoma | 5 |
| Soft tissue sarcoma | 5 |
| Ductal carcinoma | 2 |
| Malignant melanoma | 3 |
| Bulky Disease Location in 31 Sites/30 Patients | |
| Head and neck | 4 |
| Trunk | |
| - Intrathoracic | 5 |
| - Abdomen–pelvis | 15 |
| - Breast | 2 |
| - Soft tissue | 4 |
| Lower extremities | 1 |
| Tumor size in 31 Sites/30 Patients | |
| 5–10 cm | 25 |
| >10 cm | 6 |
| Gross Tumor Volume, cc | |
| Median | 146,8 |
| Range | 50.9–2039.7 |
| Systemic Therapy Immediately Preceding Irradiation | |
|---|---|
| Chemotherapy | 17 |
| Immunotherapy | 3 |
| Chemo-Immunotherapy | 6 |
| None | 4 |
| Dose Fraction to Vertices in 31 Sites/30 Patients | |
| Median | 15 Gy/1 fx |
| 10 Gy/1 fx | 12 |
| 15 Gy/1 fx | 13 |
| 18 Gy/1 fx | 1 |
| 21 Gy/3 fx | 1 |
| 24 Gy/3 Fx | 1 |
| 27 Gy/3 Fx | 3 |
| Dose-Fraction Schemes to GTV in 31 Sites/30 Patients | |
| Median | 20 Gy/4 fx |
| 18 Gy/3 fx | 1 |
| 20 Gy/4 fx | 17 |
| 22.4 Gy/4 fx | 1 |
| 30 Gy/3 fx | 10 |
| 30 Gy/5 fx | 1 |
| 40.5 Gy/15 fx | 1 |
| Symptomatic Benefit after Irradiation | |
|---|---|
| Yes | 30 |
| No | 0 |
| VAS Score | |
| Median | 1.5 |
| Range | 0–4 |
| Acute Toxicity | |
| None | 21 |
| G2 mucositis | 1 |
| G1 dysphagia | 2 |
| G1 skin | 5 |
| G1 diarrhea | 1 |
| Late Toxicity | |
| None | 29 |
| Skin | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferini, G.; Parisi, S.; Lillo, S.; Viola, A.; Minutoli, F.; Critelli, P.; Valenti, V.; Illari, S.I.; Brogna, A.; Umana, G.E.; et al. Impressive Results after “Metabolism-Guided” Lattice Irradiation in Patients Submitted to Palliative Radiation Therapy: Preliminary Results of LATTICE_01 Multicenter Study. Cancers 2022, 14, 3909. https://doi.org/10.3390/cancers14163909
Ferini G, Parisi S, Lillo S, Viola A, Minutoli F, Critelli P, Valenti V, Illari SI, Brogna A, Umana GE, et al. Impressive Results after “Metabolism-Guided” Lattice Irradiation in Patients Submitted to Palliative Radiation Therapy: Preliminary Results of LATTICE_01 Multicenter Study. Cancers. 2022; 14(16):3909. https://doi.org/10.3390/cancers14163909
Chicago/Turabian StyleFerini, Gianluca, Silvana Parisi, Sara Lillo, Anna Viola, Fabio Minutoli, Paola Critelli, Vito Valenti, Salvatore Ivan Illari, Anna Brogna, Giuseppe Emmanuele Umana, and et al. 2022. "Impressive Results after “Metabolism-Guided” Lattice Irradiation in Patients Submitted to Palliative Radiation Therapy: Preliminary Results of LATTICE_01 Multicenter Study" Cancers 14, no. 16: 3909. https://doi.org/10.3390/cancers14163909
APA StyleFerini, G., Parisi, S., Lillo, S., Viola, A., Minutoli, F., Critelli, P., Valenti, V., Illari, S. I., Brogna, A., Umana, G. E., Ferrantelli, G., Lo Giudice, G., Carrubba, C., Zagardo, V., Santacaterina, A., Leotta, S., Cacciola, A., Pontoriero, A., & Pergolizzi, S. (2022). Impressive Results after “Metabolism-Guided” Lattice Irradiation in Patients Submitted to Palliative Radiation Therapy: Preliminary Results of LATTICE_01 Multicenter Study. Cancers, 14(16), 3909. https://doi.org/10.3390/cancers14163909