
Challenges in Glioblastoma Radiomics and the Path to Clinical Implementation


Abstract
:Simple Summary
Abstract
1. Introduction
2. Literature Selection Methodology
3. Radiomics
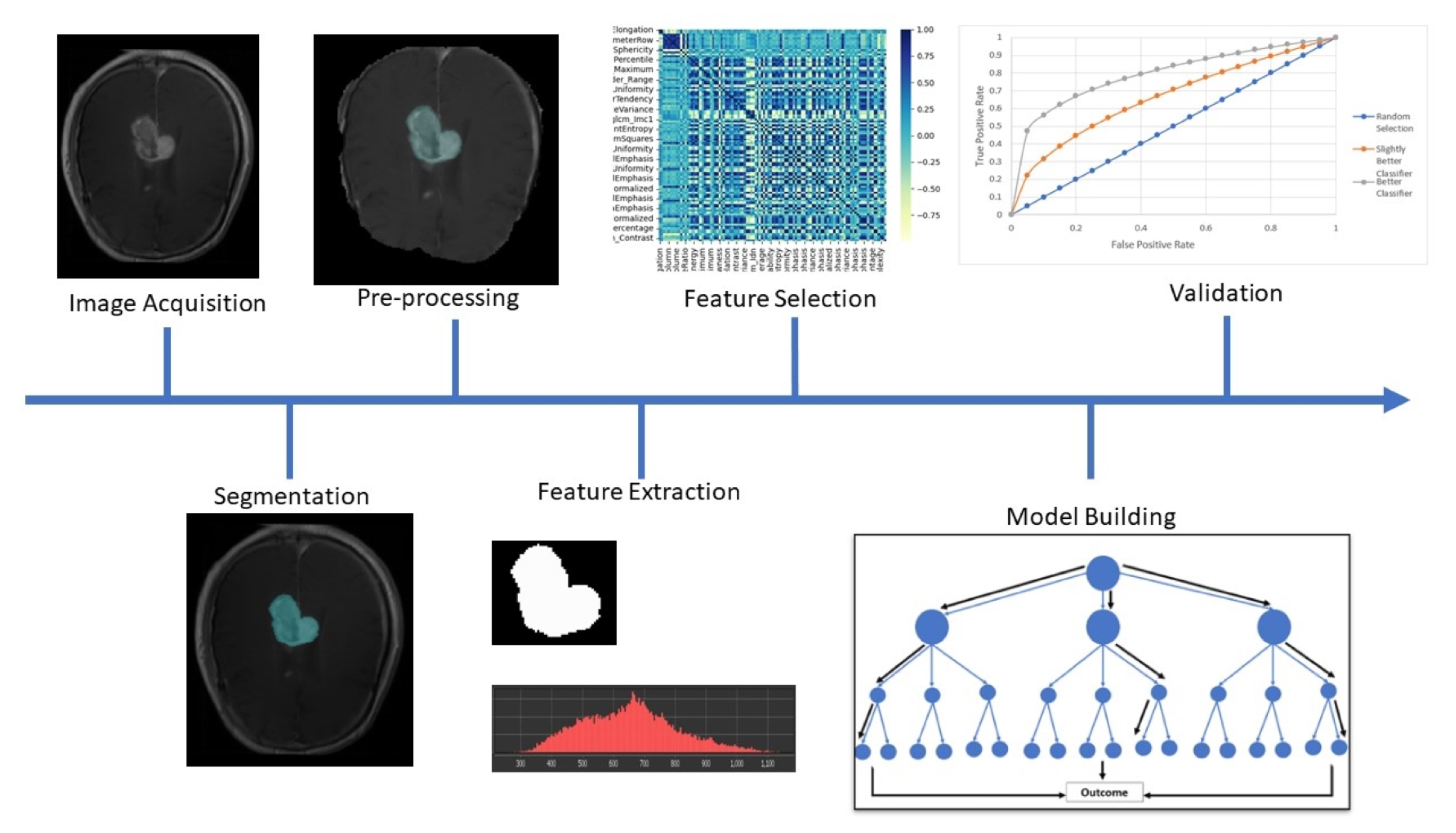
3.1. Radiomics Methodology
3.2. Radiomic Features
3.3. Artificial Intelligence and Radiomics
3.4. Implementation of Standardisation Methods
4. Current State of Research in GBM Radiomics
4.1. Potential Applications of Radiomics in GBM Patient Management
4.2. Existing Models in GBM Radiomics
4.3. Challenges of Developing a Radiomics Model for Brain Cancer
5. Improvements Required to Build Confidence in GBM Radiomics
5.1. Multi-Parametric Radiomics Models
- Diffusion weighted imaging (DWI)—MRI sequences which quantify diffusion of water molecules [19];
- Perfusion weighted imaging (PWI)—Group of MRI sequences which quantify perfusion parameters [19];
- Magnetic Resonance Spectroscopy (MRS)—MRI spectroscopy sequence to identify the presence of certain metabolites [73].
5.2. A Roadmap for the Implementation of Radiomics in Clinical Practice
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Maher, E.A.; Bachoo, R.M. Glioblastoma. In Rosenberg’s Molecular and Genetic Basis of Neurological and Psychiatric Disease, 5th ed.; Academic Press: Cambridge, MA, USA, 2015; pp. 909–917. ISBN 9780124105294. [Google Scholar] [CrossRef]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Brain and Other Central Nervous System Cancers; Australian Institute of Health and Welfare: Canberra, Australia, 2017; p. 108. [Google Scholar]
- Fernandes, C.; Costa, A.; Osório, L.; Lago, R.C.; Linhares, P.; Carvalho, B.; Caeiro, C. Current Standards of Care in Glioblastoma Therapy. Glioblastoma 2017, 197–241. [Google Scholar] [CrossRef]
- Roa, W.; Brasher, P.M.; Bauman, G.; Anthes, M.; Bruera, E.; Chan, A.; Fisher, B.; Fulton, D.; Gulavita, S.; Hao, C.; et al. Abbreviated course of radiation therapy in older patients with glioblastoma multiforme: A prospective randomized clinical trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2004, 22, 1583–1588. [Google Scholar] [CrossRef]
- Ou, A.; Yung, W.A.; Majd, N. Molecular mechanisms of drug resistance in glioblastoma. Int. J. Mol. Sci. 2021, 22, 6385. [Google Scholar] [CrossRef]
- Bergmann, N.; Delbridge, C.; Gempt, J.; Feuchtinger, A.; Walch, A.; Schirmer, L.; Bunk, W.; Aschenbrenner, T.; Liesche-Starnecker, F.; Schlegel, J. The Intratumoral Heterogeneity Reflects the Intertumoral Subtypes of Glioblastoma Multiforme: A Regional Immunohistochemistry Analysis. Front. Oncol. 2020, 10, 494. [Google Scholar] [CrossRef]
- Beig, N.; Patel, J.; Prasanna, P.; Hill, V.; Gupta, A.; Correa, R.; Bera, K.; Singh, S.; Partovi, S.; Varadan, V.; et al. Radiogenomic analysis of hypoxia pathway is predictive of overall survival in Glioblastoma. Sci. Rep. 2018, 8, 7. [Google Scholar] [CrossRef]
- Yan, J.L.; Li, C.; Boonzaier, N.R.; Fountain, D.M.; Larkin, T.J.; Matys, T.; van der Hoorn, A.; Price, S.J. Multimodal MRI characteristics of the glioblastoma infiltration beyond contrast enhancement. Ther. Adv. Neurol. Disord. 2019, 12, 1756286419844664. [Google Scholar] [CrossRef]
- Shukla, G.; Alexander, G.S.; Bakas, S.; Nikam, R.; Talekar, K.; Palmer, J.D.; Shi, W. Advanced magnetic resonance imaging in glioblastoma: A review. Chin. Clin. Oncol. 2017, 6, 40. [Google Scholar] [CrossRef]
- Menze, B.H.; Jakab, A.; Bauer, S.; Kalpathy-cramer, J.; Farahani, K.; Kirby, J.; Burren, Y.; Porz, N.; Slotboom, J.; Wiest, R.; et al. The multimodal brain tumor image segmentation benchmark (BRATS). IEEE Trans. Med. Imaging 2015, 34, 1993–2024. [Google Scholar] [CrossRef]
- Yan, J.L.; Li, C.; Hoorn, A.v.d.; Boonzaier, N.R.; Matys, T.; Price, S.J. A Neural Network Approach to Identify the Peritumoral Invasive Areas in Glioblastoma Patients by Using MR Radiomics. Sci. Rep. 2020, 10, 9748. [Google Scholar] [CrossRef]
- Garrett, M.D.; Yanagihara, T.K.; Yeh, R.; McKhann, G.M.; Sisti, M.B.; Bruce, J.N.; Sheth, S.A.; Sonabend, A.M.; Wang, T.J. Monitoring Radiation Treatment Effects in Glioblastoma: FLAIR Volume as Significant Predictor of Survival. Tomography 2017, 3, 131. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; Wang, G.; Feng, Y.; Yu, T.; Guo, Y.; Bai, X.; Ye, Z. Diffusion and perfusion weighted magnetic resonance imaging for tumor volume definition in radiotherapy of brain tumors. Radiat. Oncol. 2016, 11, 123. [Google Scholar] [CrossRef] [PubMed]
- Gardin, I.; Grégoire, V.; Gibon, D.; Kirisli, H.; Pasquier, D.; Thariat, J.; Vera, P. Radiomics: Principles and radiotherapy applications. Crit. Rev. Oncol./Hematol. 2019, 138, 44–50. [Google Scholar] [CrossRef]
- Shaikh, F.; Dupont-Roettger, D.; Dehmeshki, J.; Awan, O.; Kubassova, O.; Bisdas, S. The Role of Imaging Biomarkers Derived From Advanced Imaging and Radiomics in the Management of Brain Tumors. Front. Oncol. 2020, 10, 1–6. [Google Scholar] [CrossRef]
- Caruso, D.; Polici, M.; Zerunian, M.; Pucciarelli, F.; Guido, G.; Polidori, T.; Landolfi, F.; Nicolai, M.; Lucertini, E.; Tarallo, M.; et al. Radiomics in Oncology, Part 1: Technical Principles and Gastrointestinal Application in CT and MRI. Cancers 2021, 13, 2522. [Google Scholar] [CrossRef]
- Caruso, D.; Polici, M.; Zerunian, M.; Pucciarelli, F.; Guido, G.; Polidori, T.; Landolfi, F.; Nicolai, M.; Lucertini, E.; Tarallo, M.; et al. Radiomics in Oncology, Part 2: Thoracic, Genito-Urinary, Breast, Neurological, Hematologic and Musculoskeletal Applications. Cancers 2021, 13, 2681. [Google Scholar] [CrossRef]
- Park, J.E.; Kim, H.S.; Jo, Y.; Yoo, R.E.; Choi, S.H.; Nam, S.J.; Kim, J.H. Radiomics prognostication model in glioblastoma using diffusion- and perfusion-weighted MRI. Sci. Rep. 2020, 10, 4250. [Google Scholar] [CrossRef]
- Patel, M.; Zhan, J.; Natarajan, K.; Flintham, R.; Davies, N.; Sanghera, P.; Grist, J.; Duddalwar, V.; Peet, A.; Sawlani, V. Machine learning-based radiomic evaluation of treatment response prediction in glioblastoma. Clin. Radiol. 2021, 76, 17–628. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.L.; Toh, C.H.; Ko, L.; Wei, K.C.; Chen, P.Y. A Neural Network Approach to Identify Glioblastoma Progression Phenotype from Multimodal MRI. Cancers 2021, 13, 2006. [Google Scholar] [CrossRef]
- Shim, K.Y.; Chung, S.W.; Jeong, J.H.; Hwang, I.; Park, C.K.; Kim, T.M.; Park, S.H.; Won, J.K.; Lee, J.H.; Lee, S.T.; et al. Radiomics-based neural network predicts recurrence patterns in glioblastoma using dynamic susceptibility contrast-enhanced MRI. Sci. Rep. 2021, 11, 9974. [Google Scholar] [CrossRef]
- Shboul, Z.A.; Alam, M.; Vidyaratne, L.; Pei, L.; Elbakary, M.I.; Iftekharuddin, K.M. Feature-Guided Deep Radiomics for Glioblastoma Patient Survival Prediction. Front. Neurosci. 2019, 13, 966. [Google Scholar] [CrossRef]
- O’Connor, J.P.; Aboagye, E.O.; Adams, J.E.; Aerts, H.J.; Barrington, S.F.; Beer, A.J.; Boellaard, R.; Bohndiek, S.E.; Brady, M.; Brown, G.; et al. Imaging biomarker roadmap for cancer studies. Nat. Rev. Clin. Oncol. 2017, 14, 169. [Google Scholar] [CrossRef]
- Hu, L.S.; Swanson, K.R. Roadmap for the clinical integration of radiomics in neuro-oncology. Neuro-Oncology 2020, 22, 743–745. [Google Scholar] [CrossRef] [PubMed]
- Carles, M.; Popp, I.; Starke, M.M.; Mix, M.; Urbach, H.; Schimek-Jasch, T.; Eckert, F.; Niyazi, M.; Baltas, D.; Grosu, A.L. FET-PET radiomics in recurrent glioblastoma: Prognostic value for outcome after re-irradiation? Radiat. Oncol. 2021, 16, 46. [Google Scholar] [CrossRef]
- Lohmann, P.; Elahmadawy, M.A.; Gutsche, R.; Werner, J.M.; Bauer, E.K.; Ceccon, G.; Kocher, M.; Lerche, C.W.; Rapp, M.; Fink, G.R.; et al. FET PET Radiomics for Differentiating Pseudoprogression from Early Tumor Progression in Glioma Patients Post-Chemoradiation. Cancers 2020, 12, 3835. [Google Scholar] [CrossRef]
- Fournier, L.; Costaridou, L.; Bidaut, L.; Michoux, N.; Lecouvet, F.E.; de Geus-Oei, L.F.; Boellaard, R.; Oprea-Lager, D.E.; Obuchowski, N.A.; Caroli, A.; et al. Incorporating radiomics into clinical trials: Expert consensus endorsed by the European Society of Radiology on considerations for data-driven compared to biologically driven quantitative biomarkers. Eur. Radiol. 2021, 31, 6001–6012. [Google Scholar] [CrossRef]
- van Timmeren, J.E.; Cester, D.; Tanadini-Lang, S.; Alkadhi, H.; Baessler, B. Radiomics in medical imaging—“How-to” guide and critical reflection. Insights Imaging 2020, 11, 91. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Steinmann, A.; Ding, Y.; Lee, H.; Owens, C.; Wang, J.; Yang, J.; Followill, D.; Ger, R.; MacKin, D.; et al. Radiomics feature robustness as measured using an MRI phantom. Sci. Rep. 2021, 11, 3973. [Google Scholar] [CrossRef] [PubMed]
- Haarburger, C.; Müller-Franzes, G.; Weninger, L.; Kuhl, C.; Truhn, D.; Merhof, D. Radiomics feature reproducibility under inter-rater variability in segmentations of CT images. Sci. Rep. 2020, 10, 12688. [Google Scholar] [CrossRef]
- Hoebel, K.V.; Patel, J.B.; Beers, A.L.; Chang, K.; Singh, P.; Brown, J.M.; Pinho, M.C.; Batchelor, T.T.; Gerstner, E.R.; Rosen, B.R.; et al. Radiomics repeatability pitfalls in a scan-rescan mri study of glioblastoma. Radiol. Artif. Intell. 2021, 3, e190199. [Google Scholar] [CrossRef]
- Koçak, B.; Durmaz, E.Ş.; Ateş, E.; Kılıçkesmez, Ö. Radiomics with artificial intelligence: A practical guide for beginners. Diagn. Interv. Radiol. 2019, 25, 485–495. [Google Scholar] [CrossRef]
- Papanikolaou, N.; Matos, C.; Koh, D.M. How to develop a meaningful radiomic signature for clinical use in oncologic patients. Cancer Imaging 2020, 20, 33. [Google Scholar] [CrossRef]
- Kim, D.W.; Jang, H.Y.; Kim, K.W.; Shin, Y.; Park, S.H. Design Characteristics of Studies Reporting the Performance of Artificial Intelligence Algorithms for Diagnostic Analysis of Medical Images: Results from Recently Published Papers. Korean J. Radiol. 2019, 20, 405. [Google Scholar] [CrossRef]
- Suter, Y.; Knecht, U.; Alão, M.; Valenzuela, W.; Hewer, E.; Schucht, P.; Wiest, R.; Reyes, M. Radiomics for glioblastoma survival analysis in pre-operative MRI: Exploring feature robustness, class boundaries, and machine learning techniques. Cancer Imaging 2020, 20, 55. [Google Scholar] [CrossRef]
- Chaddad, A.; Kucharczyk, M.J.; Daniel, P.; Sabri, S.; Jean-Claude, B.J.; Niazi, T.; Abdulkarim, B. Radiomics in Glioblastoma: Current Status and Challenges Facing Clinical Implementation. Front. Oncol. 2019, 9, 374. [Google Scholar] [CrossRef]
- Lao, J.; Chen, Y.; Li, Z.C.; Li, Q.; Zhang, J.; Liu, J.; Zhai, G. A Deep Learning-Based Radiomics Model for Prediction of Survival in Glioblastoma Multiforme. Sci. Rep. 2017, 7, 10353. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, K.; Miyake, M.; Takahashi, M.; Hamamoto, R. Observing deep radiomics for the classification of glioma grades. Sci. Rep. 2021, 11, 10942. [Google Scholar] [CrossRef]
- Court, L.E.; Fave, X.; Mackin, D.; Lee, J.; Yang, J.; Zhang, L. Computational resources for radiomics. Transl. Cancer Res. 2016, 5, 340–348. [Google Scholar] [CrossRef]
- Korte, J.C.; Cardenas, C.; Hardcastle, N.; Kron, T.; Wang, J.; Bahig, H.; Elgohari, B.; Ger, R.; Court, L.; Fuller, C.D.; et al. Radiomics feature stability of open-source software evaluated on apparent diffusion coefficient maps in head and neck cancer. Sci. Rep. 2021, 11, 17633. [Google Scholar] [CrossRef]
- Sotoudeh, H.; Shafaat, O.; Bernstock, J.D.; Brooks, M.D.; Elsayed, G.A.; Chen, J.A.; Szerip, P.; Chagoya, G.; Gessler, F.; Sotoudeh, E.; et al. Artificial intelligence in the management of glioma: Era of personalized medicine. Front. Oncol. 2019, 9, 768. [Google Scholar] [CrossRef] [PubMed]
- Qian, Z.; Zhang, L.; Hu, J.; Chen, S.; Chen, H.; Shen, H.; Zheng, F.; Zang, Y.; Chen, X. Machine Learning-Based Analysis of Magnetic Resonance Radiomics for the Classification of Gliosarcoma and Glioblastoma. Front. Oncol. 2021, 11, 3296. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.; Tustison, N.J.; Patel, S.H.; Meyer, C.H. Brain Tumor Segmentation Using an Ensemble of 3D U-Nets and Overall Survival Prediction Using Radiomic Features. Front. Comput. Neurosci. 2020, 14, 25. [Google Scholar] [CrossRef]
- Bakas, S.; Reyes, M.; Jakab, A.; Bauer, S.; Rempfler, M.; Crimi, A.; Shinohara, R.T.; Berger, C.; Ha, S.M.; Rozycki, M.; et al. Identifying the best machine learning algorithms for brain tumor segmentation, progression assessment, and overall survival prediction in the BRATS challenge. arXiv 2018, arXiv:1811.02629. [Google Scholar]
- Bae, S.; Choi, Y.S.; Ahn, S.S.; Chang, J.H.; Kang, S.G.; Kim, E.H.; Kim, S.H.; Lee, S.K. Radiomic MRI phenotyping of glioblastoma: Improving survival prediction. Radiology 2018, 289, 797–806. [Google Scholar] [CrossRef]
- Cho, H.H.; Lee, S.H.; Kim, J.; Park, H. Classification of the glioma grading using radiomics analysis. PeerJ 2018, 2018, e5982. [Google Scholar] [CrossRef]
- Barnhart, H.X.; Barboriak, D.P. Applications of the Repeatability of Quantitative Imaging Biomarkers: A Review of Statistical Analysis of Repeat Data Sets. Transl. Oncol. 2009, 2, 231. [Google Scholar] [CrossRef]
- Shukla-Dave, A.; Obuchowski, N.A.; Chenevert, T.L.; Jambawalikar, S.; Schwartz, L.H.; Malyarenko, D.; Huang, W.; Noworolski, S.M.; Young, R.J.; Shiroishi, M.S.; et al. Quantitative Imaging Biomarkers Alliance (QIBA) Recommendations for Improved Precision of DWI and DCE-MRI Derived Biomarkers in Multicenter Oncology Trials. J. Magn. Reson. Imaging JMRI 2019, 49, e101. [Google Scholar] [CrossRef]
- Raunig, D.L.; McShane, L.M.; Pennello, G.; Gatsonis, C.; Carson, P.L.; Voyvodic, J.T.; Wahl, R.L.; Kurland, B.F.; Schwarz, A.J.; Gönen, M.; et al. Quantitative imaging biomarkers: A review of statistical methods for technical performance assessment. Stat. Methods Med. Res. 2015, 24, 27–67. [Google Scholar] [CrossRef] [PubMed]
- Carré, A.; Klausner, G.; Edjlali, M.; Lerousseau, M.; Briend-Diop, J.; Sun, R.; Ammari, S.; Reuzé, S.; Alvarez Andres, E.; Estienne, T.; et al. Standardization of brain MR images across machines and protocols: Bridging the gap for MRI-based radiomics. Sci. Rep. 2020, 10, 12340. [Google Scholar] [CrossRef]
- H, M.; SMR, A.; R, G. Impact of image preprocessing methods on reproducibility of radiomic features in multimodal magnetic resonance imaging in glioblastoma. J. Appl. Clin. Med. Phys. 2020, 21, 179–190. [Google Scholar] [CrossRef]
- Nyú, L.G.; Udupa, J.K. On Standardizing the MR Image Intensity Scale. Magn. Reson. Med. 1999, 42, 1072–1081. [Google Scholar] [CrossRef]
- Gispert, J.D.; Reig, S.; Pascau, J.; Vaquero, J.J.; García-Barreno, P.; Desco, M. Method for bias field correction of brain T1-weighted magnetic resonance images minimizing segmentation error. Hum. Brain Mapp. 2004, 22, 133. [Google Scholar] [CrossRef]
- Choi, S.W.; Cho, H.H.; Koo, H.; Cho, K.R.; Nenning, K.H.; Langs, G.; Furtner, J.; Baumann, B.; Woehrer, A.; Cho, H.J.; et al. Multi-Habitat Radiomics Unravels Distinct Phenotypic Subtypes of Glioblastoma with Clinical and Genomic Significance. Cancers 2020, 12, 1707. [Google Scholar] [CrossRef]
- Komori, T. Grading of adult diffuse gliomas according to the 2021 WHO Classification of Tumors of the Central Nervous System. Lab. Investig. 2021, 102, 126–133. [Google Scholar] [CrossRef]
- Bakas, S.; Akbari, H.; Sotiras, A.; Bilello, M.; Rozycki, M.; Kirby, J.S.; Freymann, J.B.; Farahani, K.; Davatzikos, C. Advancing The Cancer Genome Atlas glioma MRI collections with expert segmentation labels and radiomic features. Sci. Data 2017, 4, 170117. [Google Scholar] [CrossRef]
- Rivera, A.L.; Pelloski, C.E.; Gilbert, M.R.; Colman, H.; De La Cruz, C.; Sulman, E.P.; Bekele, B.N.; Aldape, K.D. MGMT promoter methylation is predictive of response to radiotherapy and prognostic in the absence of adjuvant alkylating chemotherapy for glioblastoma. Neuro-Oncology 2010, 12, 116. [Google Scholar] [CrossRef]
- Hegi, M.E.; Diserens, A.C.; Gorlia, T.; Hamou, M.F.; de Tribolet, N.; Weller, M.; Kros, J.M.; Hainfellner, J.A.; Mason, W.; Mariani, L.; et al. MGMT Gene Silencing and Benefit from Temozolomide in Glioblastoma. N. Engl. J. Med. 2005, 352, 997–1003. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, T.; Kinoshita, M.; Fujita, K.; Fukai, J.; Hayashi, N.; Uematsu, Y.; Okita, Y.; Nonaka, M.; Moriuchi, S.; Uda, T.; et al. Radiomics and MGMT promoter methylation for prognostication of newly diagnosed glioblastoma. Sci. Rep. 2019, 9, 14435. [Google Scholar] [CrossRef]
- Vils, A.; Bogowicz, M.; Tanadini-Lang, S.; Vuong, D.; Saltybaeva, N.; Kraft, J.; Wirsching, H.G.; Gramatzki, D.; Wick, W.; Rushing, E.; et al. Radiomic Analysis to Predict Outcome in Recurrent Glioblastoma Based on Multi-Center MR Imaging from the Prospective DIRECTOR Trial. Front. Oncol. 2021, 11, 636672. [Google Scholar] [CrossRef] [PubMed]
- Kickingereder, P.; Götz, M.; Muschelli, J.; Wick, A.; Neuberger, U.; Shinohara, R.T.; Sill, M.; Nowosielski, M.; Schlemmer, H.P.; Radbruch, A.; et al. Large-scale Radiomic Profiling of Recurrent Glioblastoma Identifies an Imaging Predictor for Stratifying Anti-Angiogenic Treatment Response. Clin. Cancer Res. 2016, 22, 5765–5771. [Google Scholar] [CrossRef]
- Wen, P.Y.; Chang, S.M.; Van Den Bent, M.J.; Vogelbaum, M.A.; Macdonald, D.R.; Lee, E.Q. Response assessment in neuro-oncology clinical trials. J. Clin. Oncol. 2017, 35, 2439–2449. [Google Scholar] [CrossRef]
- Hamstra, D.A.; Galbán, C.J.; Meyer, C.R.; Johnson, T.D.; Sundgren, P.C.; Tsien, C.; Lawrence, T.S.; Junck, L.; Ross, D.J.; Rehemtulla, A.; et al. Functional diffusion map as an early imaging biomarker for high-grade glioma: Correlation with conventional radiologic response and overall survival. J. Clin. Oncol. 2008, 26, 3387–3394. [Google Scholar] [CrossRef]
- Qiu, Q.; Duan, J.; Yin, Y. Radiomics in radiotherapy: Applications and future challenges. Precis. Radiat. Oncol. 2020, 4, 29–33. [Google Scholar] [CrossRef]
- Sloan, A.E.; Shukla, G.; Rathore, S.; Akbari, H.; Gondi, V.; Davatzikos, C. Radiomics-based identification of peritumoral infiltration in de novo glioblastoma imaging presents targets amenable for potential targeted extended resection: A neurosurgical survey. J. Clin. Oncol. 2019, 37, e13573. [Google Scholar] [CrossRef]
- Forghani, R.; Gupta, R.; Maleki, F.; Chiu, Y.; Yen, Y. Efficient Radiomics-Based Classification of Multi-Parametric MR Images to Identify Volumetric Habitats and Signatures in Glioblastoma: A Machine Learning Approach. Cancers 2022, 14, 1475. [Google Scholar] [CrossRef]
- Um, H.; Tixier, F.; Bermudez, D.; Deasy, J.O.; Young, R.J.; Veeraraghavan, H. Impact of image preprocessing on the scanner dependence of multi-parametric MRI radiomic features and covariate shift in multi-institutional glioblastoma datasets. Phys. Med. Biol. 2019, 64, 165011. [Google Scholar] [CrossRef]
- Park, J.E.; Kim, H.S.; Kim, D.; Park, S.Y.; Kim, J.Y.; Cho, S.J.; Kim, J.H. A systematic review reporting quality of radiomics research in neuro-oncology: Toward clinical utility and quality improvement using high-dimensional imaging features. BMC Cancer 2020, 20, 29. [Google Scholar] [CrossRef] [PubMed]
- Riley, R.D.; Snell, K.I.; Ensor, J.; Burke, D.L.; Harrell, F.E.; Moons, K.G.; Collins, G.S. Minimum sample size for developing a multivariable prediction model: PART II—Binary and time-to-event outcomes. Stat. Med. 2019, 38, 1276–1296. [Google Scholar] [CrossRef] [PubMed]
- Mohyeldin, A.; Lonser, R.R.; Elder, J.B. Real-time magnetic resonance imaging-guided frameless stereotactic brain biopsy: Technical note. J. Neurosurg. 2016, 124, 1039–1046. [Google Scholar] [CrossRef] [PubMed]
- Rathore, S.; Akbari, H.; Doshi, J. Radiomic signature of infiltration in peritumoral edema predicts subsequent recurrence in glioblastoma: Implications for personalized radiotherapy planning. J. Med. Imaging 2018, 5, 1. [Google Scholar] [CrossRef]
- Park, J.E.; Kim, H.S.; Park, K.J.; Kim, S.J.; Kim, J.H.; Smith, S.A. Pre-and posttreatment glioma: Comparison of amide proton transfer imaging with MR spectroscopy for biomarkers of tumor proliferation. Radiology 2016, 278, 514–523. [Google Scholar] [CrossRef] [PubMed]
- Kong, Z.; Jiang, C.; Zhu, R.; Feng, S.; Wang, Y.; Li, J.; Chen, W.; Liu, P.; Zhao, D.; Ma, W.; et al. 18F-FDG-PET-based radiomics features to distinguish primary central nervous system lymphoma from glioblastoma. Neuroimage Clin. 2019, 23, 101912. [Google Scholar] [CrossRef] [PubMed]
- Gao, M.; Huang, S.; Pan, X.; Liao, X.; Yang, R.; Liu, J. Machine Learning-Based Radiomics Predicting Tumor Grades and Expression of Multiple Pathologic Biomarkers in Gliomas. Front. Oncol. 2020, 10, 1676. [Google Scholar] [CrossRef]
- Kumar, V.; Gu, Y.; Basu, S.; Berglund, A.; Eschrich, S.A.; Schabath, M.B.; Forster, K.; Aerts, H.J.; Dekker, A.; Fenstermacher, D.; et al. QIN “Radiomics: The Process and the Challenges”. Magn. Reson. Imaging 2012, 30, 1234. [Google Scholar] [CrossRef] [PubMed]
- Clark, K.; Vendt, B.; Smith, K.; Freymann, J.; Kirby, J.; Koppel, P.; Moore, S.; Phillips, S.; Maffitt, D.; Pringle, M.; et al. The cancer imaging archive (TCIA): Maintaining and operating a public information repository. J. Digit. Imaging 2013, 26, 1045–1057. [Google Scholar] [CrossRef] [PubMed]
- Lord, S.J.; St John, A.; Bossuyt, P.M.; Sandberg, S.; Monaghan, P.J.; O’Kane, M.; Cobbaert, C.M.; Röddiger, R.; Lennartz, L.; Gelfi, C.; et al. Setting clinical performance specifications to develop and evaluate biomarkers for clinical use. Ann. Clin. Biochem. 2019, 56, 527–535. [Google Scholar] [CrossRef]

{kind=link}
| Algorithm | Description | Application in Radiomics |
|---|---|---|
| Support Vector Machine | A support vector machine aims to perform binary classification on multidimensional data by finding the ideal hyperplane to separate the two classifications | Support vector machines can be used on a voxel-by-voxel basis to predict tissue biological parameters or in conjunction with radiomic features to make a binary prediction (for example distinguishing between high and low grade glioma) based on multiple feature values. This was implemented in a study by Qian et al. [43] to differentiate between Glioblastoma and Gliosarcoma. |
| Neural Network | A neural network performs mathematical operations on input data through a series of interconnected layers to produce a prediction. Deep Learning is a subset of Machine Learning based on neural networks using two or more ‘hidden layers’ and has received much attention in recent years for image and data processing. | Neural networks can be used in place of a regression algorithm to generate predictions based on the values of radiomic features [12]. In the case of deep learning, a class of radiomic features known as deep features that are derived using convolutional neural networks. In addition to this, deep learning has been implemented in automated segmentation of brain tumours [44,45]. |
| Random Forest | A random forest is an ensemble of decision trees with a final prediction created by the results of all the trees. The final decision is created by a ‘vote’ of all these trees. | A model aiming to produce a binary prediction based on multiple factors could benefit from the implementation of random forests. Tasks related to GBM patient management suited for including differentiation between pseudo- and true- tumour progression, stratification of patients into high or low risk categories [46] and a grading of gliomas [47]. |
| Author | Model Description | Conclusions | Clinical Application | Performance | Patient Numbers |
|---|---|---|---|---|---|
| Kickingereder et al., 2016 [62] | Stratification of patients into groups who were likely or not likely to benefit from anti-angiogenic therapies | A radiomics model based on supervised principal component analysis is effective at stratifying patients into groups that can benefit from the addition of anti-angiogenic therapy | Identification of which patients may benefit from certain therapies provides clinicians a convenient to tailor treatment regimens to individuals | AUC = 0.792 | 172 |
| Lao et al., 2017 [38] | Deep features were extracted using transfer learning and implemented into a survival prediction model. This model utilised learned features, handcrafted radiomics features and clinical factors to produce a prediction of overall patient survival. | Implementing learned features into a predictive radiomics model can improve the performance of a predictive model. | A survival prediction model can be used to determine if a patient would benefit from a more aggressive treatment regimen. Improving performance by implementing learned features and clinical factors can build confidence in the model. | AUC = 0.739 | 112 |
| Shboul et al., 2019 [23] | A fully automated segmentation pipeline using Deep Neural Networks was developed using the BraTS challenge dataset. Survival prediction was then performed using radiomic features extracted from this dataset. | A fully automated framework for the delineation of GBM and patient survival prediction can be useful to reduce clinical workload and bias in the tasks of segmentation and survival prediction. | A framework such as this can be used to provide a perform a tumour segmentation for the purpose of radiotherapy treatment planning. Survival predictions can be used to recommend a more or less aggressive treatment regimen as required | Leave one out cross validation accuracy = 0.73 | 396 total |
| Park et al., 2020 [19] | Survival Prediction based on T1 Post Contrast, T2 FLAIR and DSC MRI as well as clinical factors. | By incorporating mpMRI as well as clinical factors, it is possible to achieve a high performing survival prediction model | An accurate prediction of survival period can provide a quantitative measure of the severity of the disease. | AUC = 0.74 | 216 |
| Yan et al., 2020 [12] | Identification of peritumoural invasive regions in GBM based on Structural, Perfusion-weighted and Diffusion-weighted MRI. Convolutional Neural Network was used along with radiomics to identify regions of peritumoural infiltration | Lower intensity on Diffusion-weighted MRI and higher intensity on T1, FLAIR and Perfusion-weighted MRI was observed in peritumoural invasion areas. | Identification of regions of peritumoural invasion will allow treatment plans to accurately target whole tumour volumes and improve local control. | Accuracy = 78.5% | 57 |
| Suter et al., 2020 [36] | Feature robustness was tested and models developed on single centre data were applied to multicentre data. In addition to this, a model developed using robust features on single centre data was tested on multicentre data. | A large performance drop was found when models trained on single centre data were applied to multicentre data. This performance drop could be reduced when the model was restricted to robust features. | Model transferability is an important factor in radiomic research. To develop transferable radiomics models, it will be necessary to develop models on multi-centre data and identify reproducible radiomic features. | AUC reduced by 0.56 for single centre model tested on multicentre data | 63 single centre patients, 76 multicentre data |
| Shim et al., 2021 [22] | Prediction of recurrence pattern based on DSC MRI radiomics and neural networks, model produced to predict local and distant recurrence | Quantitative measures of tumour perfusion can accurately predict recurrence patterns of tumour recurrence | Identifying the likely course of tumour progression could enable early intervention or treatment plan adaptation. | AUC = 0.969; AUC = 0.864 (local and distant) | 192 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martin, P.; Holloway, L.; Metcalfe, P.; Koh, E.-S.; Brighi, C. Challenges in Glioblastoma Radiomics and the Path to Clinical Implementation. Cancers 2022, 14, 3897. https://doi.org/10.3390/cancers14163897
Martin P, Holloway L, Metcalfe P, Koh E-S, Brighi C. Challenges in Glioblastoma Radiomics and the Path to Clinical Implementation. Cancers. 2022; 14(16):3897. https://doi.org/10.3390/cancers14163897
Chicago/Turabian StyleMartin, Philip, Lois Holloway, Peter Metcalfe, Eng-Siew Koh, and Caterina Brighi. 2022. "Challenges in Glioblastoma Radiomics and the Path to Clinical Implementation" Cancers 14, no. 16: 3897. https://doi.org/10.3390/cancers14163897
APA StyleMartin, P., Holloway, L., Metcalfe, P., Koh, E.-S., & Brighi, C. (2022). Challenges in Glioblastoma Radiomics and the Path to Clinical Implementation. Cancers, 14(16), 3897. https://doi.org/10.3390/cancers14163897