
Neither Tumor-Infiltrating Lymphocytes nor Cytotoxic T Cells Predict Enhanced Benefit from Chemotherapy in the DBCG77B Phase III Clinical Trial

 , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
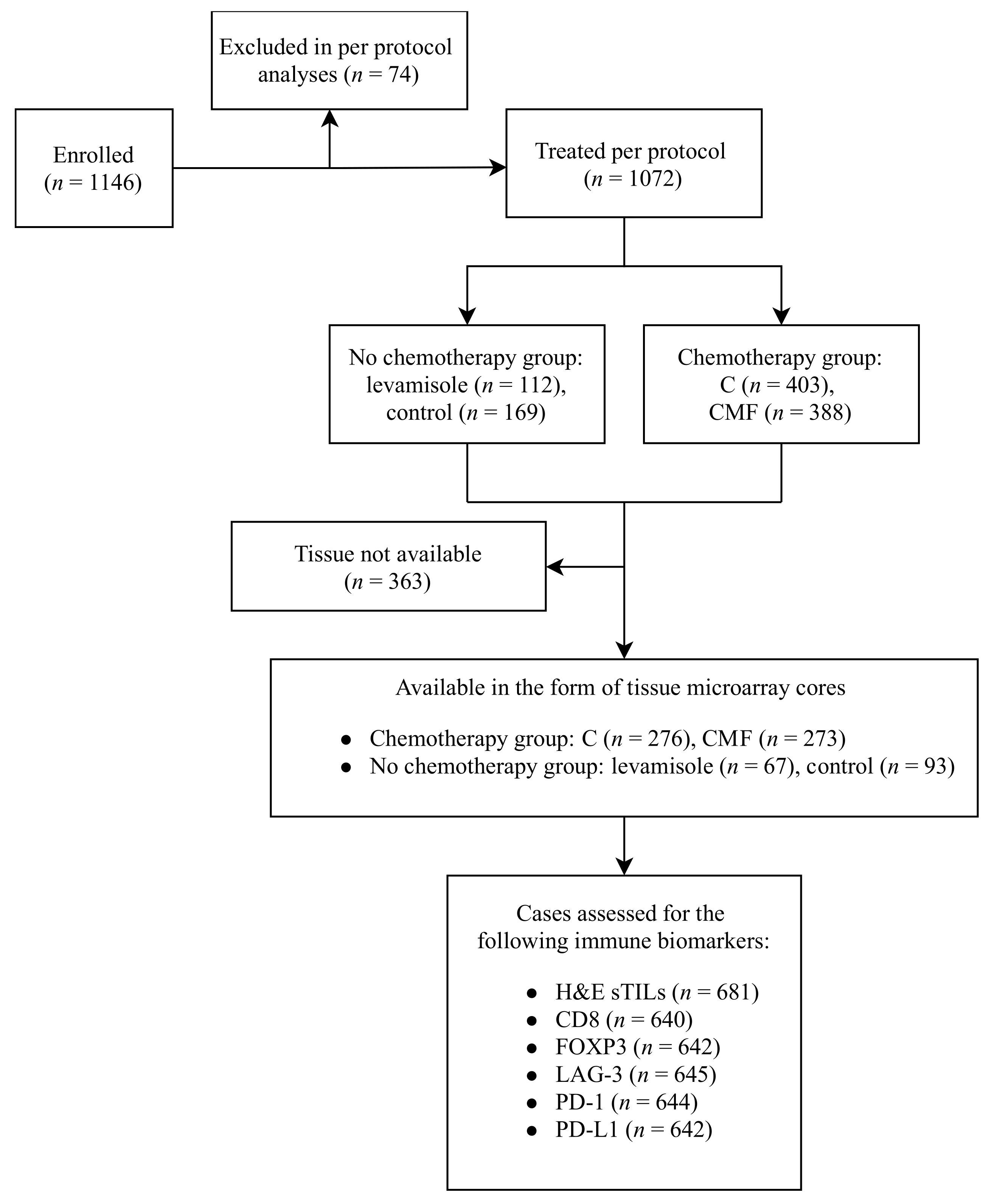
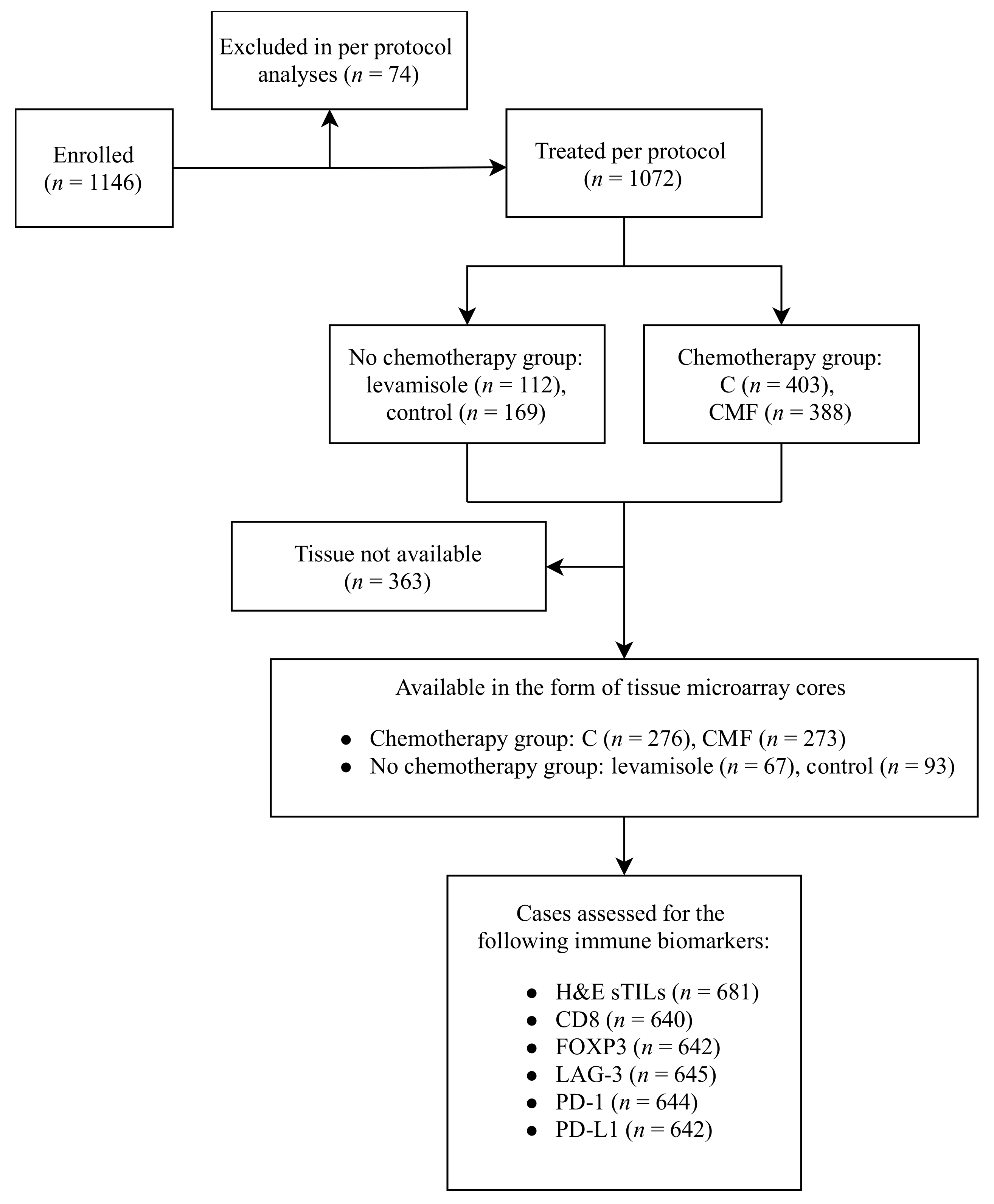
2.1. Study Cohort
2.2. Immunohistochemical Staining and Assessment
2.3. Statistical Analysis
3. Results
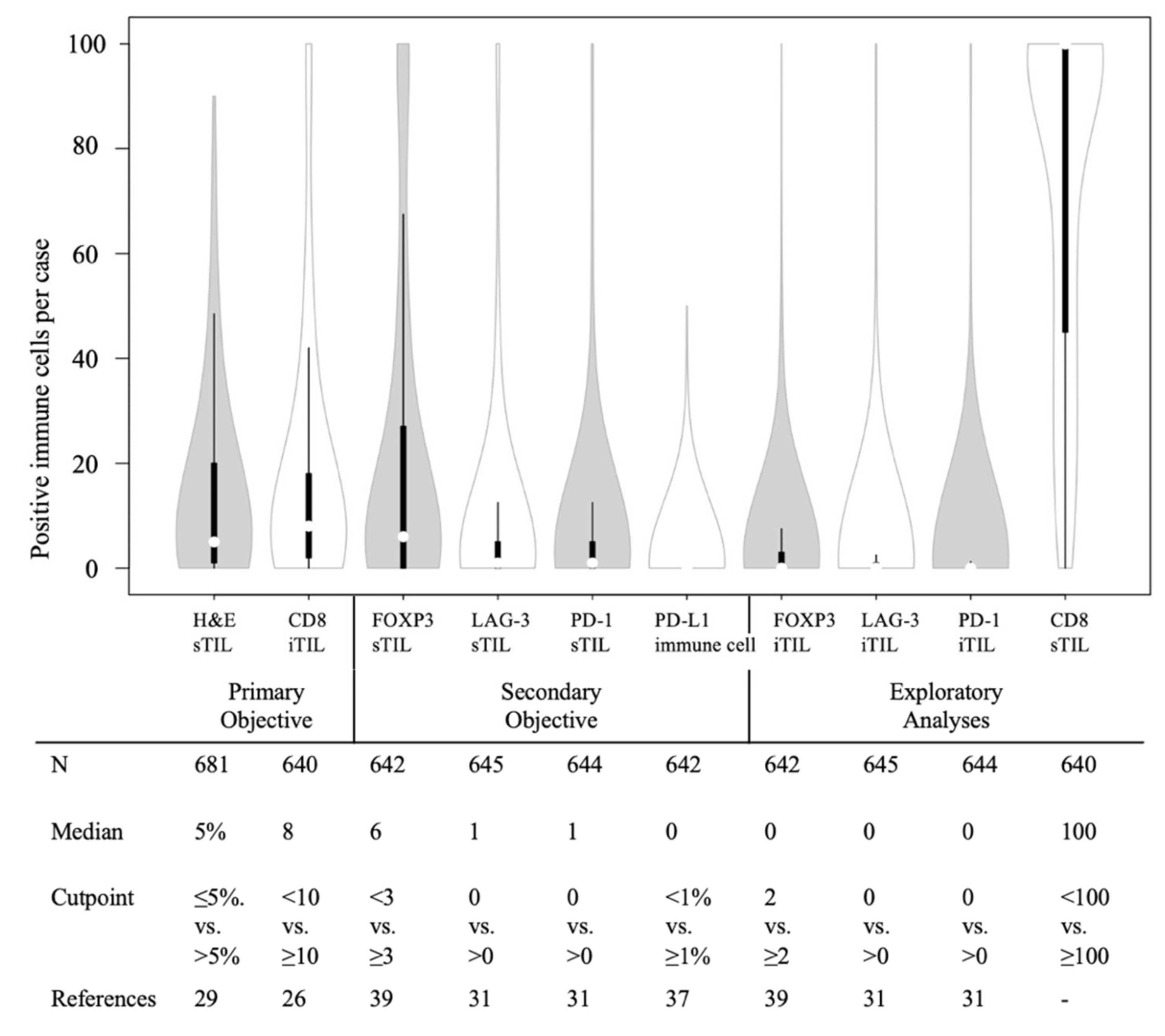
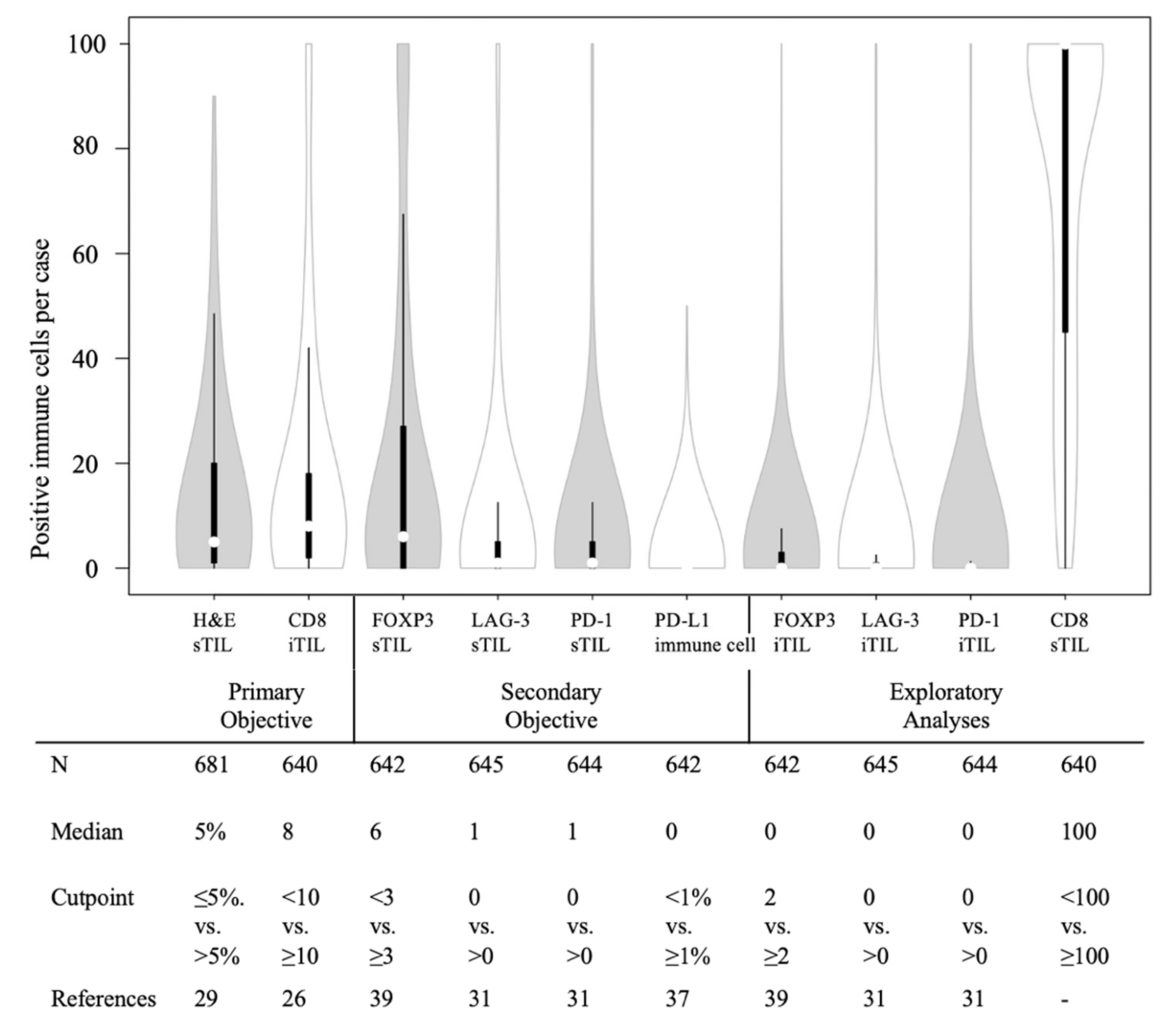
3.1. Biomarker Distribution and Clinicopathological Factors
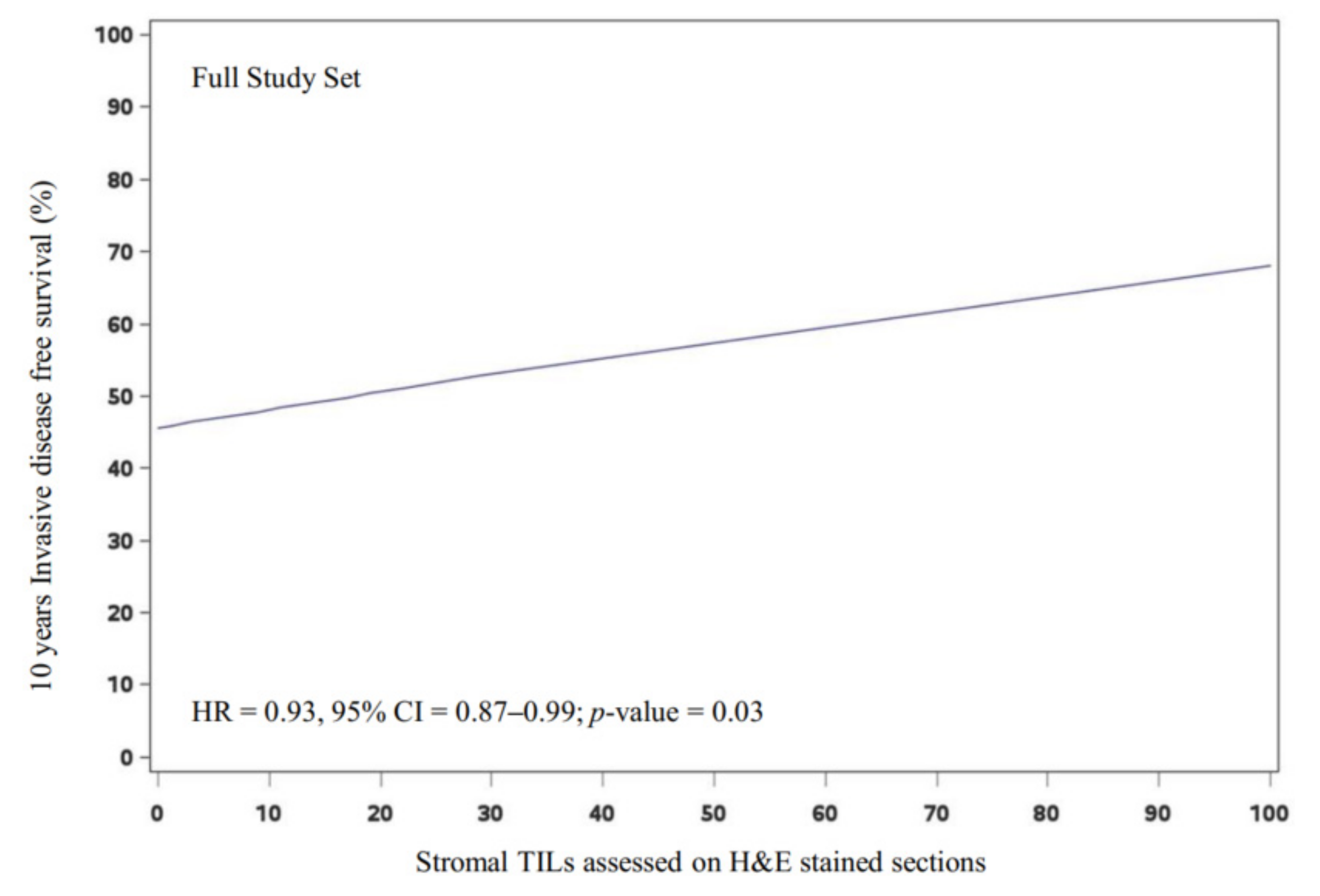
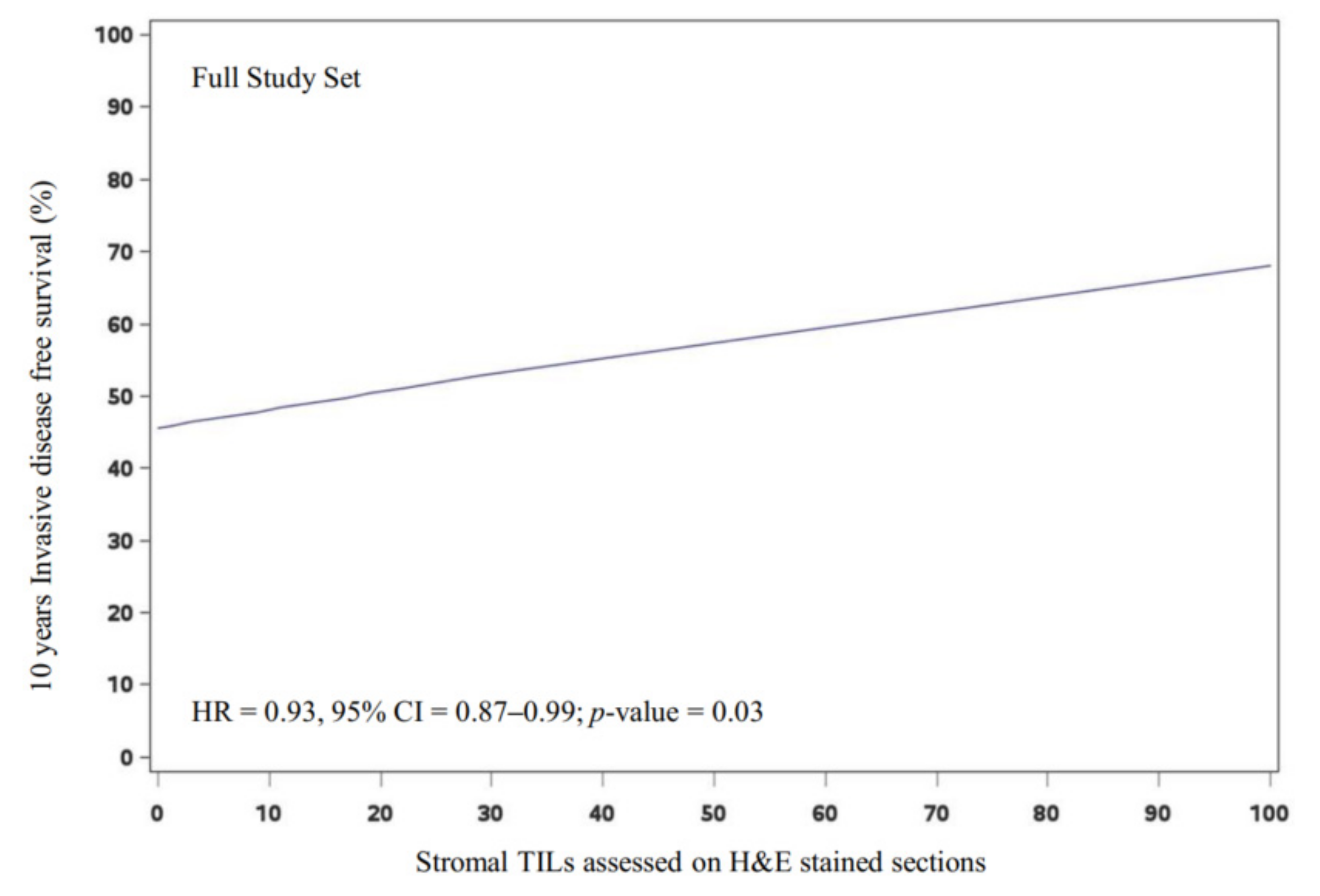
3.2. Prognostic Value of the Primary Immune Biomarkers in the Full Study Set
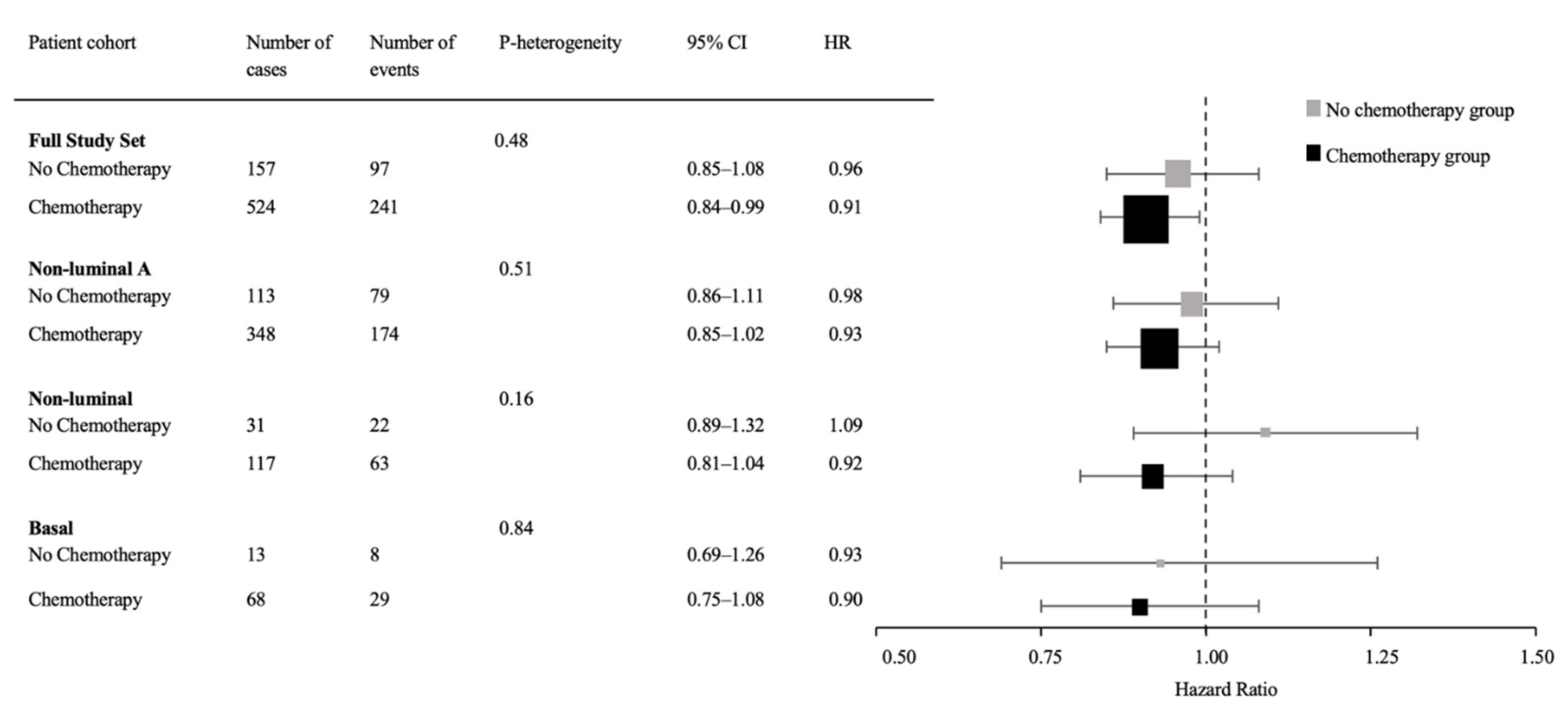
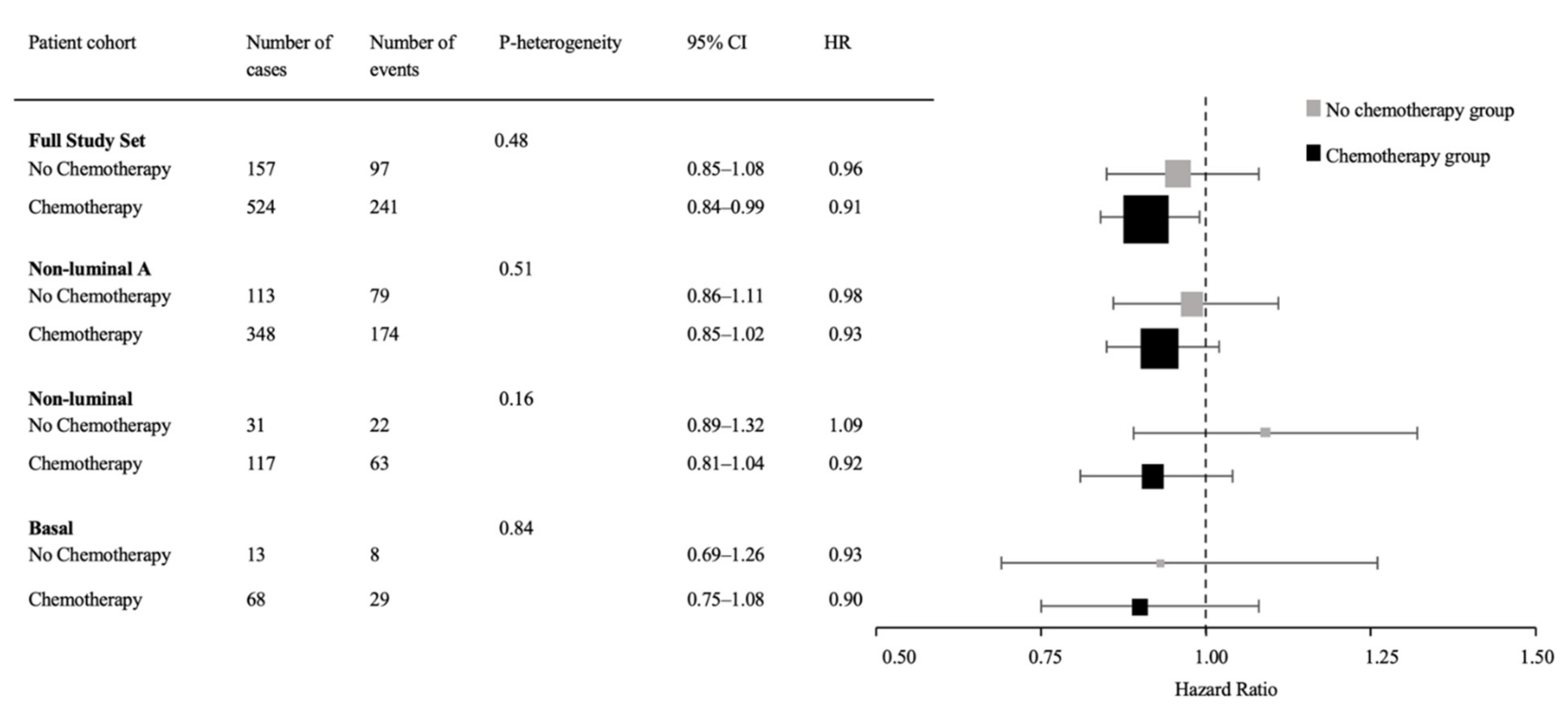
3.3. Predictive Value of Immune Biomarkers for Chemotherapy Benefit
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Anampa, J.; Makower, D.; Sparano, J.A. Progress in Adjuvant Chemotherapy for Breast Cancer: An Overview. BMC Med. 2015, 13, 195. [Google Scholar] [CrossRef] [Green Version]
- Galluzzi, L.; Humeau, J.; Buqué, A.; Zitvogel, L.; Kroemer, G. Immunostimulation with Chemotherapy in the Era of Immune Checkpoint Inhibitors. Nat. Rev. Clin. Oncol. 2020, 17, 725–741. [Google Scholar] [CrossRef]
- Buccione, C.; Fragale, A.; Polverino, F.; Ziccheddu, G.; Aricò, E.; Belardelli, F.; Proietti, E.; Battistini, A.; Moschella, F. Role of Interferon Regulatory Factor 1 in Governing Treg Depletion, Th1 Polarization, Inflammasome Activation and Antitumor Efficacy of Cyclophosphamide. Int. J. Cancer 2018, 142, 976–987. [Google Scholar] [CrossRef] [Green Version]
- North, R.J. Cyclophosphamide-Facilitated Adoptive Immunotherapy of an Established Tumor Depends on Elimination of Tumor-Induced Suppressor T Cells. J. Exp. Med. 1982, 155, 1063. [Google Scholar] [CrossRef] [Green Version]
- Ghiringhelli, F.; Larmonier, N.; Schmitt, E.; Parcellier, A.; Cathelin, D.; Garrido, C.; Chauffert, B.; Solary, E.; Bonnotte, B.; Martin, F. CD4+CD25+ Regulatory T Cells Suppress Tumor Immunity but Are Sensitive to Cyclophosphamide Which Allows Immunotherapy of Established Tumors to Be Curative. Eur. J. Immunol. 2004, 34, 336–344. [Google Scholar] [CrossRef]
- Schiavoni, G.; Sistigu, A.; Valentini, M.; Mattei, F.; Sestili, P.; Spadaro, F.; Sanchez, M.; Lorenzi, S.; D’Urso, M.T.; Belardelli, F.; et al. Cyclophosphamide Synergizes with Type I Interferons through Systemic Dendritic Cell Reactivation and Induction of Immunogenic Tumor Apoptosis. Cancer Res. 2011, 71, 768–778. [Google Scholar] [CrossRef] [Green Version]
- Ge, Y.; Domschke, C.; Stoiber, N.; Schott, S.; Heil, J.; Rom, J.; Blumenstein, M.; Thum, J.; Sohn, C.; Schneeweiss, A.; et al. Metronomic Cyclophosphamide Treatment in Metastasized Breast Cancer Patients: Immunological Effects and Clinical Outcome. Cancer Immunol. Immunother. 2012, 61, 353–362. [Google Scholar] [CrossRef]
- Ghiringhelli, F.; Menard, C.; Puig, P.E.; Ladoire, S.; Roux, S.; Martin, F.; Solary, E.; le Cesne, A.; Zitvogel, L.; Chauffert, B. Metronomic Cyclophosphamide Regimen Selectively Depletes CD4 +CD25+ Regulatory T Cells and Restores T and NK Effector Functions in End Stage Cancer Patients. Cancer Immunol. Immunother. 2007, 56, 641–648. [Google Scholar] [CrossRef]
- Moschella, F.; Torelli, G.F.; Valentini, M.; Urbani, F.; Buccione, C.; Petrucci, M.T.; Natalino, F.; Belardelli, F.; Foá, R.; Proietti, E. Cyclophosphamide Induces a Type I Interferon–Associated Sterile Inflammatory Response Signature in Cancer Patients’ Blood Cells: Implications for Cancer Chemoimmunotherapy. Clin. Cancer Res. 2013, 19, 4249–4261. [Google Scholar] [CrossRef] [Green Version]
- Schmid, P.; Cortes, J.; Pusztai, L.; McArthur, H.; Kümmel, S.; Bergh, J.; Denkert, C.; Park, Y.H.; Hui, R.; Harbeck, N.; et al. Pembrolizumab for Early Triple-Negative Breast Cancer. N. Engl. J. Med. 2020, 382, 810–821. [Google Scholar] [CrossRef]
- Mittendorf, E.A.; Zhang, H.; Barrios, C.H.; Saji, S.; Jung, K.H.; Hegg, R.; Koehler, A.; Sohn, J.; Iwata, H.; Telli, M.L.; et al. Neoadjuvant Atezolizumab in Combination with Sequential Nab-Paclitaxel and Anthracycline-Based Chemotherapy versus Placebo and Chemotherapy in Patients with Early-Stage Triple-Negative Breast Cancer (IMpassion031): A Randomised, Double-Blind, Phase 3 Trial. Lancet 2020, 396, 1090–1100. [Google Scholar] [CrossRef]
- Tolaney, S.M.; Kalinsky, K.; Kaklamani, V.G.; D’Adamo, D.R.; Aktan, G.; Tsai, M.L.; O’Regan, R.M.; Kaufman, P.A.; Wilks, S.T.; Andreopoulou, E.; et al. Eribulin Plus Pembrolizumab in Patients with Metastatic Triple-Negative Breast Cancer (ENHANCE 1): A Phase Ib/II Study. Clin. Cancer Res. 2021, 27, 3061–3068. [Google Scholar] [CrossRef]
- Foldi, J.; Silber, A.; Reisenbichler, E.; Singh, K.; Fischbach, N.; Persico, J.; Adelson, K.; Katoch, A.; Horowitz, N.; Lannin, D.; et al. Neoadjuvant Durvalumab plus Weekly Nab-Paclitaxel and Dose-Dense Doxorubicin/Cyclophosphamide in Triple-Negative Breast Cancer. NPJ Breast Cancer 2021, 7, 9. [Google Scholar] [CrossRef]
- Jin, M.Z.; Jin, W.L. The Updated Landscape of Tumor Microenvironment and Drug Repurposing. Signal Transduct. Target. Ther. 2020, 5, 1–16. [Google Scholar] [CrossRef]
- Loi, S.; Drubay, D.; Adams, S.; Pruneri, G.; Francis, P.A.; Lacroix-Triki, M.; Joensuu, H.; Dieci, M.V.; Badve, S.; Demaria, S.; et al. Tumor-Infiltrating Lymphocytes and Prognosis: A Pooled Individual Patient Analysis of Early-Stage Triple-Negative Breast Cancers. J. Clin. Oncol. 2019, 37, 559–569. [Google Scholar] [CrossRef]
- Denkert, C.; von Minckwitz, G.; Darb-Esfahani, S.; Lederer, B.; Heppner, B.I.; Weber, K.E.; Budczies, J.; Huober, J.; Klauschen, F.; Furlanetto, J.; et al. Tumour-Infiltrating Lymphocytes and Prognosis in Different Subtypes of Breast Cancer: A Pooled Analysis of 3771 Patients Treated with Neoadjuvant Therapy. Lancet Oncol. 2018, 19, 40–50. [Google Scholar] [CrossRef]
- Heppner, B.I.; Untch, M.; Denkert, C.; Pfitzner, B.M.; Lederer, B.; Schmitt, W.; Eidtmann, H.; Fasching, P.A.; Tesch, H.; Solbach, C.; et al. Tumor-Infiltrating Lymphocytes: A Predictive and Prognostic Biomarker in Neoadjuvant-Treated HER2-Positive Breast Cancer. Clin. Cancer Res. 2016, 22, 5747–5754. [Google Scholar] [CrossRef] [Green Version]
- Denkert, C.; Loibl, S.; Noske, A.; Roller, M.; Müller, B.M.; Komor, M.; Budczies, J.; Darb-Esfahani, S.; Kronenwett, R.; Hanusch, C.; et al. Tumor-Associated Lymphocytes as an Independent Predictor of Response to Neoadjuvant Chemotherapy in Breast Cancer. J. Clin. Oncol. 2010, 28, 105–113. [Google Scholar] [CrossRef]
- Lundgren, C.; Bendahl, P.O.; Ekholm, M.; Fernö, M.; Forsare, C.; Krüger, U.; Nordenskjöld, B.; Stål, O.; Rydén, L. Tumour-Infiltrating Lymphocytes as a Prognostic and Tamoxifen Predictive Marker in Premenopausal Breast Cancer: Data from a Randomised Trial with Long-Term Follow-Up. Breast Cancer Res. 2020, 22, 140. [Google Scholar] [CrossRef]
- El Bairi, K.; Haynes, H.R.; Blackley, E.; Fineberg, S.; Shear, J.; Turner, S.; de Freitas, J.R.; Sur, D.; Amendola, L.C.; Gharib, M.; et al. The Tale of TILs in Breast Cancer: A Report from The International Immuno-Oncology Biomarker Working Group. Npj Breast Cancer 2021, 7, 1–17. [Google Scholar] [CrossRef]
- Goldberg, J.; Pastorello, R.G.; Vallius, T.; Davis, J.; Cui, Y.X.; Agudo, J.; Waks, A.G.; Keenan, T.; McAllister, S.S.; Tolaney, S.M.; et al. The Immunology of Hormone Receptor Positive Breast Cancer. Front. Immunol. 2021, 12, 674192. [Google Scholar] [CrossRef]
- Griguolo, G.; Dieci, M.V.; Paré, L.; Miglietta, F.; Generali, D.G.; Frassoldati, A.; Cavanna, L.; Bisagni, G.; Piacentini, F.; Tagliafico, E.; et al. Immune Microenvironment and Intrinsic Subtyping in Hormone Receptor-Positive/HER2-Negative Breast Cancer. Npj Breast Cancer 2021, 7, 1–5. [Google Scholar] [CrossRef]
- Burugu, S.; Asleh-Aburaya, K.; Nielsen, T.O. Immune Infiltrates in the Breast Cancer Microenvironment: Detection, Characterization and Clinical Implication. Breast Cancer 2017, 24, 3–15. [Google Scholar] [CrossRef]
- Shou, J.; Zhang, Z.; Lai, Y.; Chen, Z.; Huang, J. Worse Outcome in Breast Cancer with Higher Tumor-Infiltrating FOXP3+ Tregs: A Systematic Review and Meta-Analysis. BMC Cancer 2016, 16, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Lachapelle, J.; Leung, S.; Gao, D.; Foulkes, W.D.; Nielsen, T.O. CD8 +lymphocyte Infiltration Is an Independent Favorable Prognostic Indicator in Basal-like Breast Cancer. Breast Cancer Res. 2012, 14, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Ali, H.R.; Provenzano, E.; Dawson, S.J.; Blows, F.M.; Liu, B.; Shah, M.; Earl, H.M.; Poole, C.J.; Hiller, L.; Dunn, J.A.; et al. Association between CD8+ T-Cell Infiltration and Breast Cancer Survival in 12 439 Patients. Ann. Oncol. 2014, 25, 1536–1543. [Google Scholar] [CrossRef]
- Baker, K.; Lachapelle, J.; Zlobec, I.; Bismar, T.A.; Terracciano, L.; Foulkes, W.D. Prognostic Significance of CD8+ T Lymphocytes in Breast Cancer Depends upon Both Oestrogen Receptor Status and Histological Grade. Histopathology 2011, 58, 1107–1116. [Google Scholar] [CrossRef]
- Liu, S.; Chen, B.; Burugu, S.; Leung, S.; Gao, D.; Virk, S.; Kos, Z.; Parulekar, W.R.; Shepherd, L.; Gelmon, K.A.; et al. Role of Cytotoxic Tumor-Infiltrating Lymphocytes in Predicting Outcomes in Metastatic HER2-Positive Breast Cancer: A Secondary Analysis of a Randomized Clinical Trial. JAMA Oncol. 2017, 3, e172085. [Google Scholar] [CrossRef]
- Litvin, I.E.; Paganella, M.P.; Wendland, E.M.; Roehe, A.V. Prognosis of PD-L1 in Human Breast Cancer: Protocol for a Systematic Review and Meta-Analysis. Syst. Rev. 2020, 9, 1–7. [Google Scholar] [CrossRef]
- Burugu, S.; Gao, D.; Leung, S.; Chia, S.K.; Nielsen, T.O. LAG-3+ Tumor Infiltrating Lymphocytes in Breast Cancer: Clinical Correlates and Association with PD-1/PD-L1+ Tumors. Ann. Oncol. 2017, 28, 2977–2984. [Google Scholar] [CrossRef]
- Chic, N.; Brasó-Maristany, F.; Prat, A. Biomarkers of Immunotherapy Response in Breast Cancer beyond PD-L1. Breast Cancer Res. Treat. 2021, 191, 39–49. [Google Scholar] [CrossRef]
- Ejlertsen, B.; Mouridsen, H.T.; Jensen, M.B.; Andersen, J.; Andersson, M.; Kamby, C.; Knoop, A.S. Cyclophosphamide, Methotrexate, and Fluorouracil; Oral Cyclophosphamide; Levamisole; or No Adjuvant Therapy for Patients with High-Risk, Premenopausal Breast Cancer. Cancer 2010, 116, 2081–2089. [Google Scholar] [CrossRef] [Green Version]
- Increased Breast-Cancer Recurrence Rate after Adjuvant Therapy with Levamisole. A Preliminary Report. Executive Committee of the Danish Breast Cancer Cooperative Group. Lancet 1980, 2, 824–927. [Google Scholar]
- Sauerbrei, W.; Taube, S.E.; McShane, L.M.; Cavenagh, M.M.; Altman, D.G. Reporting Recommendations for Tumor Marker Prognostic Studies (REMARK): An Abridged Explanation and Elaboration. J. Natl. Cancer Inst. 2018, 110, 803–811. [Google Scholar] [CrossRef]
- Stovgaard, E.S.; Asleh, K.; Riaz, N.; Leung, S.; Gao, D.; Nielsen, L.B.; Lænkholm, A.V.; Balslev, E.; Jensen, M.B.; Nielsen, D.; et al. The Immune Microenvironment and Relation to Outcome in Patients with Advanced Breast Cancer Treated with Docetaxel with or without Gemcitabine. OncoImmunology 2021, 10, 1924492. [Google Scholar] [CrossRef]
- Stovgaard, E.S.; Bokharaey, M.; List-Jensen, K.; Roslind, A.; Kümler, I.; Høgdall, E.; Nielsen, D.; Balslev, E. PD-L1 Diagnostics in the Neoadjuvant Setting: Implications of Intratumoral Heterogeneity of PD-L1 Expression in Triple Negative Breast Cancer for Assessment in Small Biopsies. Breast Cancer Res. Treat. 2020, 181, 553–560. [Google Scholar] [CrossRef]
- Salgado, R.; Denkert, C.; Demaria, S.; Sirtaine, N.; Klauschen, F.; Pruneri, G.; Wienert, S.; van den Eynden, G.; Baehner, F.L.; Penault-Llorca, F.; et al. The Evaluation of Tumor-Infiltrating Lymphocytes (TILs) in Breast Cancer: Recommendations by an International TILs Working Group 2014. Ann. Oncol. 2015, 26, 259–271. [Google Scholar] [CrossRef]
- Liu, S.; Foulkes, W.D.; Leung, S.; Gao, D.; Lau, S.; Kos, Z.; Nielsen, T.O. Prognostic Significance of FOXP3+ Tumor-Infiltrating Lymphocytes in Breast Cancer Depends on Estrogen Receptor and Human Epidermal Growth Factor Receptor-2 Expression Status and Concurrent Cytotoxic T-Cell Infiltration. Breast Cancer Res. 2014, 16, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, T.O.; Jensen, M.B.; Burugu, S.; Gao, D.; Tykjaer Jørgensen, C.L.; Balslev, E.; Ejlertsen, B. High-Risk Premenopausal Luminal A Breast Cancer Patients Derive No Benefit from Adjuvant Cyclophosphamide-Based Chemotherapy: Results from the DBCG77B Clinical Trial. Clin. Cancer Res. 2017, 23, 946–953. [Google Scholar] [CrossRef] [Green Version]
- Oner, G.; Altintas, S.; Canturk, Z.; Tjalma, W.; Verhoeven, Y.; van Berckelaer, C.; Berneman, Z.; Peeters, M.; Pauwels, P.; van Dam, P.A. Triple-Negative Breast Cancer-Role of Immunology: A Systemic Review. Breast J. 2020, 26, 995–999. [Google Scholar] [CrossRef] [PubMed]
- Dieci, M.V.; Mathieu, M.C.; Guarneri, V.; Conte, P.; Delaloge, S.; Andre, F.; Goubar, A. Editor’s Choice: Prognostic and Predictive Value of Tumor-Infiltrating Lymphocytes in Two Phase III Randomized Adjuvant Breast Cancer Trials. Ann. Oncol. 2015, 26, 1698. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.B.; Lænkholm, A.V.; Nielsen, T.O.; Eriksen, J.O.; Wehn, P.; Hood, T.; Ram, N.; Buckingham, W.; Ferree, S.; Ejlertsen, B. The Prosigna Gene Expression Assay and Responsiveness to Adjuvant Cyclophosphamide-Based Chemotherapy in Premenopausal High-Risk Patients with Breast Cancer. Breast Cancer Res. 2018, 20, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emens, L.A.; Middleton, G. The Interplay of Immunotherapy and Chemotherapy: Harnessing Potential Synergies. Cancer Immunol. Res. 2015, 3, 436–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbon, C.M.; Yang, M.; Wands, G.D.; Ramesh, R.; Slusher, B.S.; Hedley, M.L.; Luby, T.M. Consecutive Low Doses of Cyclophosphamide Preferentially Target Tregs and Potentiate T Cell Responses Induced by DNA PLG Microparticle Immunization. Cell Immunol. 2010, 262, 150–161. [Google Scholar] [CrossRef]
- Marinelli, D.; Mazzotta, M.; Pizzuti, L.; Krasniqi, E.; Gamucci, T.; Natoli, C.; Grassadonia, A.; Tinari, N.; Tomao, S.; Sperduti, I.; et al. Neoadjuvant Immune-Checkpoint Blockade in Triple-Negative Breast Cancer: Current Evidence and Literature-Based Meta-Analysis of Randomized Trials. Cancers 2020, 12, 1–13. [Google Scholar] [CrossRef]
- Axelrod, M.L.; Nixon, M.J.; Gonzalez-Ericsson, P.I.; Bergman, R.E.; Pilkinton, M.A.; McDonnell, W.J.; Sanchez, V.; Opalenik, S.R.; Loi, S.; Zhou, J.; et al. Changes in Peripheral and Local Tumor Immunity after Neoadjuvant Chemotherapy Reshape Clinical Outcomes in Patients with Breast Cancer. Clin. Cancer Res. 2020, 26, 5668–5681. [Google Scholar] [CrossRef]
- Voorwerk, L.; Slagter, M.; Horlings, H.M.; Sikorska, K.; van de Vijver, K.K.; de Maaker, M.; Nederlof, I.; Kluin, R.J.C.; Warren, S.; Ong, S.F.; et al. Immune Induction Strategies in Metastatic Triple-Negative Breast Cancer to Enhance the Sensitivity to PD-1 Blockade: The TONIC Trial. Nat. Med. 2019, 25, 920–928. [Google Scholar] [CrossRef]
- Behling, F.; Schittenhelm, J. Tissue Microarrays—Translational Biomarker Research in the Fast Lane. Expert Rev. Mol. Diagn. 2018, 18, 833–835. [Google Scholar] [CrossRef]
- Tan, W.C.C.; Nerurkar, S.N.; Cai, H.Y.; Ng, H.H.M.; Wu, D.; Wee, Y.T.F.; Lim, J.C.T.; Yeong, J.; Lim, T.K.H. Overview of Multiplex Immunohistochemistry/Immunofluorescence Techniques in the Era of Cancer Immunotherapy. Cancer Commun. 2020, 40, 135–153. [Google Scholar] [CrossRef] [Green Version]
- Buhtoiarov, I.N.; Sondel, P.M.; Wigginton, J.M.; Buhtoiarova, T.N.; Yanke, E.M.; Mahvi, D.A.; Rakhmilevich, A.L. Anti-Tumour Synergy of Cytotoxic Chemotherapy and Anti-CD40 plus CpG-ODN Immunotherapy through Repolarization of Tumour-Associated Macrophages. Immunology 2011, 132, 226–239. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Jaffar, J.; Hellstrom, I.; Hellstrom, K.E. Administration of Cyclophosphamide Changes the Immune Profile of Tumor-Bearing Mice. J. Immunother. 2010, 33, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| H&E sTIL | CD8 iTIL | FOXP3 sTIL | LAG-3 sTIL | PD-1 sTIL | PD-L1 Immune Cell | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Low ≤5% n = 361 (%) | High >5% n = 320 (%) | Low <10 n = 355 (%) | High ≥10 n = 285 (%) | Low <3 n = 253 (%) | High ≥3 n = 389 (%) | Negative 0 n = 314 (%) | Positive >0 n = 331 (%) | Negative 0 n = 307 (%) | Positive >0 n = 337 (%) | Negative <1% n = 512 (%) | Positive ≥1% n = 130 (%) | |
| Age (years) | ||||||||||||
| ≤50 | 266 (52) | 245 (48) | 273 (56) | 211 (44) | 185 (38) | 299 (62) | 246 (51) | 241 (49) | 217 (45) | 268 (55) | 389 (81) | 94 (19%) |
| >50 | 95 (56) | 75 (44) | 82 (53) | 74 (47) | 68 (43) | 90 (57) | 68 (43) | 90 (57) | 90 (57) | 69 (43) | 123 (77) | 36 (23%) |
| p-value | 0.386 | 0.401 | 0.282 | 0.102 | 0.009 | 0.387 | ||||||
| Tumor size (mm) | ||||||||||||
| 0–20 | 110 (52) | 101 (48) | 123 (65) | 67 (35) | 81 (42) | 111 (58) | 110 (58) | 80 (42) | 92 (48) | 101 (52) | 158 (82) | 34 (18) |
| 21–50 | 184 (53) | 160 (47) | 168 (52) | 158 (48) | 110 (34) | 216 (66) | 149 (45) | 182 (55) | 159 (48) | 170 (52) | 253 (78) | 73 (22) |
| >50 | 67 (55) | 54 (45) | 63 (53) | 56 (47) | 61 (51) | 58 (49) | 54 (45) | 65 (55) | 55 (47) | 62 (53) | 98 (82) | 21 (18) |
| p-value | 0.850 | 0.011 | 0.002 | 0.013 | 0.968 | 0.333 | ||||||
| Histological type | ||||||||||||
| Ductal | 310 (52) | 281 (48) | 306 (55) | 252 (45) | 214 (38) | 345 (62) | 267 (47) | 297 (53) | 264 (47) | 298 (53) | 441 (79) | 119 (21) |
| Lobular | 24 (60) | 16 (40) | 27 (73) | 10 (27) | 20 (54) | 17 (46) | 24 (67) | 12 (33) | 19 (53) | 17 (47) | 35 (92) | 3 (8) |
| Medullary | 4 (36) | 7 (64) | 2 (22) | 7 (78) | 6 (67) | 3 (33) | 2 (22) | 7 (78) | 2 (22) | 7 (78) | 5 (63) | 3 (37) |
| Other | 18 (58) | 13 (42) | 16 (57) | 12 (43) | 10 (34) | 19 (66) | 17 (61) | 11 (39) | 18 (62) | 11 (38) | 25 (89) | 3 (11) |
| p-value | 0.494 | 0.033 | 0.082 | 0.027 | 0.156 | 0.072 | ||||||
| Grade | ||||||||||||
| 1 | 67 (57) | 50 (43) | 72 (67) | 35 (33) | 45 (42) | 61 (58) | 69 (65) | 37 (35) | 59 (56) | 47 (44) | 93 (87) | 14 (13) |
| 2 | 195 (55) | 162 (45) | 187 (55) | 152 (45) | 137 (40) | 204 (60) | 171 (50) | 174 (50) | 166 (49) | 175 (51) | 278 (81) | 66 (19) |
| 3 | 48 (41) | 69 (59) | 46 (41) | 65 (59) | 31 (28) | 80 (72) | 27 (24) | 86 (76) | 38 (33) | 76 (67) | 69 (64) | 39 (36) |
| p-value | 0.019 | 0.0006 | 0.042 | <0.0001 | 0.002 | <0.0001 | ||||||
| ER status | ||||||||||||
| <1% | 62 (37) | 107 (63) | 67 (42) | 92 (58) | 54 (35) | 102 (65) | 41 (26) | 119 (74) | 61 (38) | 98 (62) | 93 (61) | 60 (39) |
| ≥1% | 295 (59) | 207 (41) | 288 (59) | 203 (41) | 196 (39) | 302 (61) | 273 (55) | 221 (45) | 250 (50) | 246 (50) | 423 (86) | 71 (14) |
| p-value | <0.0001 | 0.0003 | 0.288 | <0.0001 | 0.008 | <0.0001 | ||||||
| HER2 status | ||||||||||||
| 0, 1+, 2+ | 307 (57) | 231 (43) | 291 (56) | 226 (44) | 213 (41) | 310 (59) | 275 (53) | 245 (47) | 252 (48) | 271 (52) | 435 (84) | 80 (16) |
| 3+ | 50 (36) | 87 (64) | 63 (47) | 71 (53) | 40 (30) | 92 (70) | 39 (29) | 96 (71) | 60 (45) | 74 (55) | 84 (63) | 50 (37) |
| p-value | <0.0001 | 0.055 | 0.279 | <0.0001 | 0.481 | <0.0001 | ||||||
| Marker | HR | 95% CI | P-Heterogeneity | HR | 95% CI | P-Heterogeneity | |
|---|---|---|---|---|---|---|---|
| Full Study Set | Non Luminal A | ||||||
| Primary objective | Secondary objective | ||||||
| CD8 iTILs | Low <10 | 0.50 | 0.36–0.70 | 0.54 | 0.46 | 0.31–0.68 | 0.68 |
| High ≥10 | 0.59 | 0.41–0.85 | 0.51 | 0.35–0.76 | |||
| Secondary objective | |||||||
| FOXP3 sTIL | Low <3 | 0.49 | 0.33–0.72 | 0.48 | 0.39 | 0.25–0.62 | 0.22 |
| High ≥3 | 0.58 | 0.42–0.80 | 0.56 | 0.40–0.79 | |||
| LAG-3 sTIL | Negative 0 | 0.53 | 0.36–0.78 | 0.68 | 0.47 | 0.30–0.76 | 0.65 |
| Positive >0 | 0.59 | 0.43–0.81 | 0.54 | 0.39–0.76 | |||
| PD-1 sTIL | Negative 0 | 0.71 | 0.49–1.03 | 0.04 | 0.53 | 0.35–0.81 | 0.75 |
| Positive >0 | 0.42 | 0.30–0.59 | 0.49 | 0.34–0.70 | |||
| PD-L1 | Negative <1% | 0.58 | 0.43–0.77 | 0.30 | 0.52 | 0.38–0.72 | 0.48 |
| Positive ≥1% | 0.43 | 0.26–0.71 | 0.42 | 0.25–0.71 | |||
| Exploratory analyses | |||||||
| H&E (categorical) | Low ≤5% | 0.54 | 0.40–0.75 | 0.95 | 0.49 | 0.34–0.71 | 0.65 |
| High >5% | 0.55 | 0.38–0.79 | 0.55 | 0.37–0.82 | |||
| FOXP3 iTIL | Low <2 | 0.50 | 0.37–0.68 | 0.32 | 0.44 | 0.31–0.62 | 0.26 |
| High ≥2 | 0.64 | 0.42–0.97 | 0.60 | 0.39–0.94 | |||
| LAG-3 iTIL | Negative 0 | 0.62 | 0.45–0.84 | 0.27 | 0.56 | 0.39–0.79 | 0.41 |
| Positive >0 | 0.46 | 0.31–0.70 | 0.44 | 0.28–0.68 | |||
| PD-1 iTIL | Negative 0 | 0.62 | 0.46–0.83 | 0.11 | 0.55 | 0.39–0.77 | 0.37 |
| Positive >0 | 0.40 | 0.25–0.62 | 0.42 | 0.26–0.69 | |||
| CD8 sTIL | Low <100 | 0.47 | 0.33–0.67 | 0.36 | 0.42 | 0.28–0.63 | 0.40 |
| High ≥100 | 0.59 | 0.41–0.83 | 0.53 | 0.36–0.77 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shenasa, E.; Stovgaard, E.S.; Jensen, M.-B.; Asleh, K.; Riaz, N.; Gao, D.; Leung, S.; Ejlertsen, B.; Laenkholm, A.-V.; Nielsen, T.O. Neither Tumor-Infiltrating Lymphocytes nor Cytotoxic T Cells Predict Enhanced Benefit from Chemotherapy in the DBCG77B Phase III Clinical Trial. Cancers 2022, 14, 3808. https://doi.org/10.3390/cancers14153808
Shenasa E, Stovgaard ES, Jensen M-B, Asleh K, Riaz N, Gao D, Leung S, Ejlertsen B, Laenkholm A-V, Nielsen TO. Neither Tumor-Infiltrating Lymphocytes nor Cytotoxic T Cells Predict Enhanced Benefit from Chemotherapy in the DBCG77B Phase III Clinical Trial. Cancers. 2022; 14(15):3808. https://doi.org/10.3390/cancers14153808
Chicago/Turabian StyleShenasa, Elahe, Elisabeth Specht Stovgaard, Maj-Britt Jensen, Karama Asleh, Nazia Riaz, Dongxia Gao, Samuel Leung, Bent Ejlertsen, Anne-Vibeke Laenkholm, and Torsten O. Nielsen. 2022. "Neither Tumor-Infiltrating Lymphocytes nor Cytotoxic T Cells Predict Enhanced Benefit from Chemotherapy in the DBCG77B Phase III Clinical Trial" Cancers 14, no. 15: 3808. https://doi.org/10.3390/cancers14153808
APA StyleShenasa, E., Stovgaard, E. S., Jensen, M.-B., Asleh, K., Riaz, N., Gao, D., Leung, S., Ejlertsen, B., Laenkholm, A.-V., & Nielsen, T. O. (2022). Neither Tumor-Infiltrating Lymphocytes nor Cytotoxic T Cells Predict Enhanced Benefit from Chemotherapy in the DBCG77B Phase III Clinical Trial. Cancers, 14(15), 3808. https://doi.org/10.3390/cancers14153808