
Proton Beam Therapy versus Photon Radiotherapy for Stage I Non-Small Cell Lung Cancer

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Statistical Analysis
2.3. Propensity Score-Matched Analysis
3. Results
3.1. Patients and Treatment
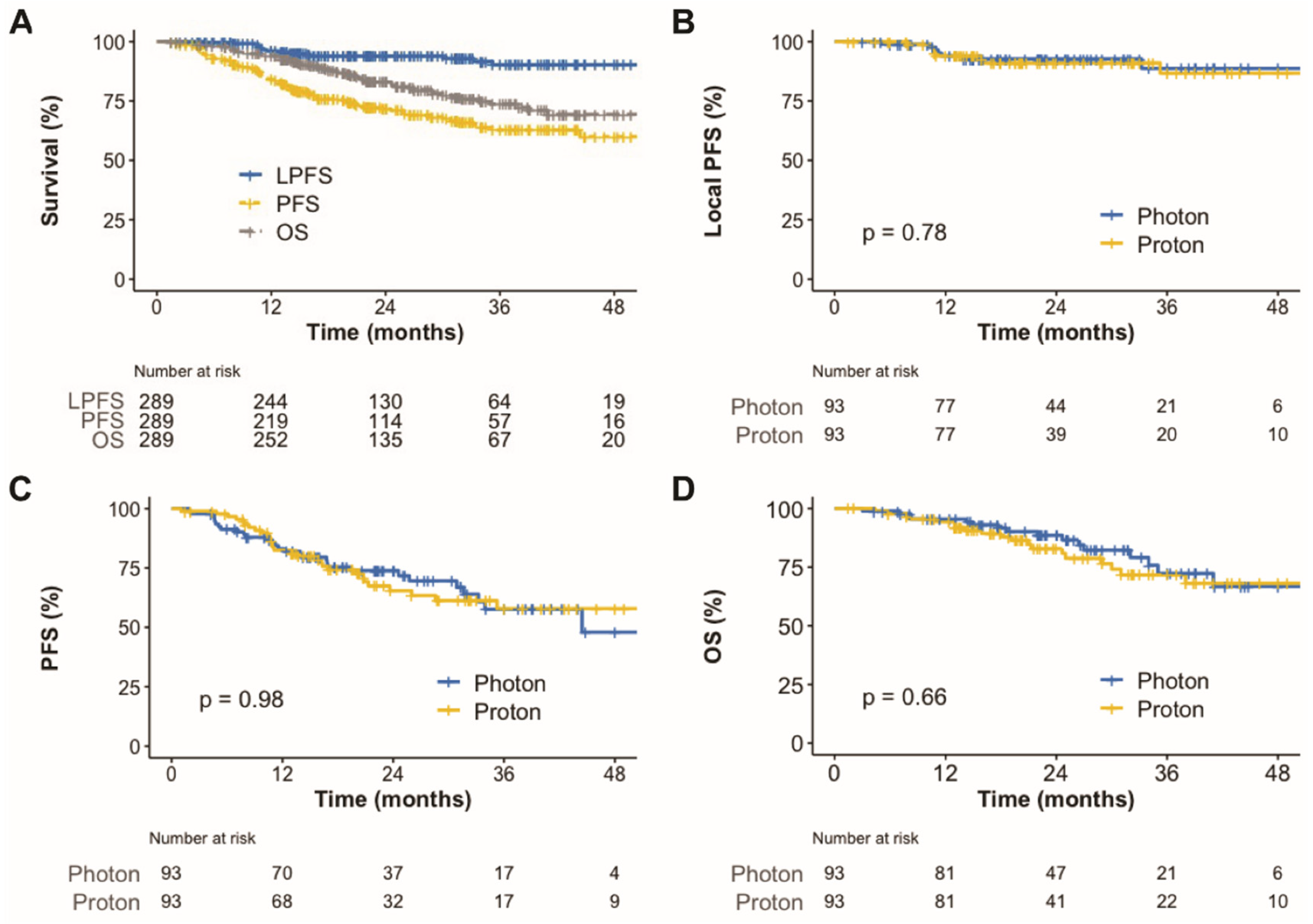
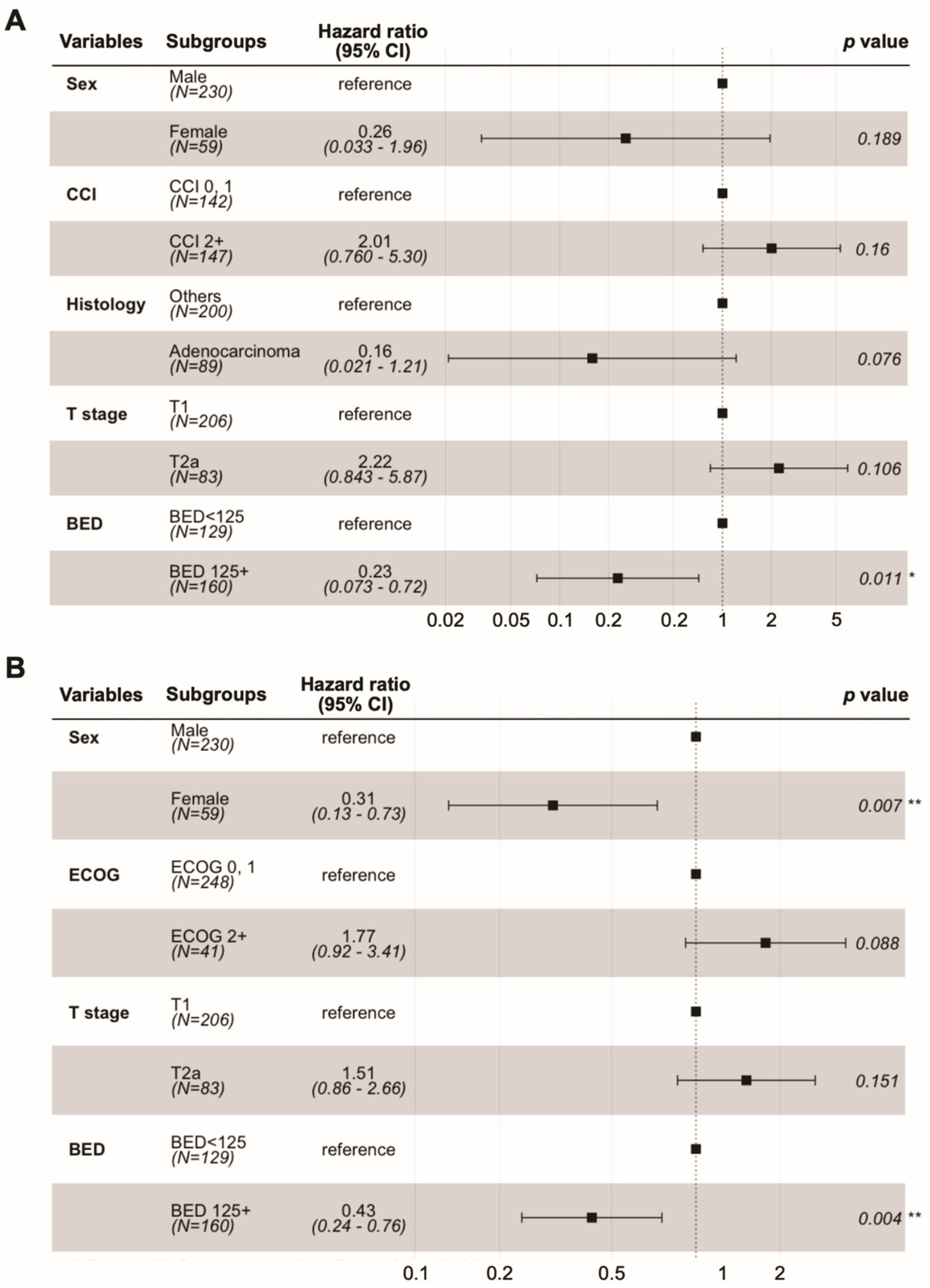
3.2. Survival
3.3. Propensity Score-Matched Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baumann, P.; Nyman, J.; Hoyer, M.; Wennberg, B.; Gagliardi, G.; Lax, I.; Drugge, N.; Ekberg, L.; Friesland, S.; Johansson, K.-A.; et al. Outcome in a Prospective Phase II Trial of Medically Inoperable Stage I Non–Small-Cell Lung Cancer Patients Treated With Stereotactic Body Radiotherapy. J. Clin. Oncol. 2009, 27, 3290–3296. [Google Scholar] [CrossRef]
- Timmerman, R.; Paulus, R.; Galvin, J.; Michalski, J.; Straube, W.; Bradley, J.; Fakiris, A.; Bezjak, A.; Videtic, G.; Johnstone, D.; et al. Stereotactic Body Radiation Therapy for Inoperable Early Stage Lung Cancer. JAMA 2010, 303, 1070–1076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Videtic, G.M.; Hu, C.; Singh, A.K.; Chang, J.Y.; Parker, W.; Olivier, K.R.; Schild, S.E.; Komaki, R.; Urbanic, J.J.; Timmerman, R.D.; et al. A Randomized Phase 2 Study Comparing 2 Stereotactic Body Radiation Therapy Schedules for Medically Inoperable Patients With Stage I Peripheral Non-Small Cell Lung Cancer: NRG Oncology RTOG 0915 (NCCTG N0927). Int. J. Radiat. Oncol. Biol. Phys. 2015, 93, 757–764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Timmerman, R.; McGarry, R.; Yiannoutsos, C.; Papiez, L.; Tudor, K.; DeLuca, J.; Ewing, M.; Abdulrahman, R.; DesRosiers, C.; Williams, M.; et al. Excessive Toxicity When Treating Central Tumors in a phase II Study of Stereotactic Body Radiation Therapy for Medically Inoperable Early-Stage Lung Cancer. J. Clin. Oncol. 2006, 24, 4833–4839. [Google Scholar] [CrossRef] [PubMed]
- Lindberg, K.; Grozman, V.; Karlsson, K.; Lindberg, S.; Lax, I.; Wersäll, P.; Persson, G.F.; Josipovic, M.; Khalil, A.A.; Moeller, D.S.; et al. The HILUS-Trial-A Prospective Nordic Multicenter Phase 2 Study of Ultracentral Lung Tumors Treated With Ste-reotactic Body Radiotherapy. J. Thorac. Oncol. 2021, 16, 1200–1210. [Google Scholar] [CrossRef] [PubMed]
- Haasbeek, C.J.; Lagerwaard, F.J.; Slotman, B.J.; Senan, S. Outcomes of Stereotactic Ablative Radiotherapy for Centrally Lo-cated Early-Stage Lung Cancer. J. Thorac. Oncol. 2011, 6, 2036–2043. [Google Scholar] [CrossRef] [Green Version]
- Chang, J.Y.; Li, Q.-Q.; Xu, Q.-Y.; Allen, P.K.; Rebueno, N.; Gomez, D.R.; Balter, P.; Komaki, R.; Mehran, R.; Swisher, S.G.; et al. Stereotactic Ablative Radiation Therapy for Centrally Located Early Stage or Isolated Parenchymal Recurrences of Non-Small Cell Lung Cancer: How to Fly in a “No Fly Zone”. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 1120–1128. [Google Scholar] [CrossRef]
- Voroney, J.-P.J.; Hope, A.; Dahele, M.R.; Purdy, T.; Franks, K.N.; Pearson, S.; Cho, J.B.; Sun, A.; Payne, D.G.; Bissonnette, J.-P.; et al. Chest Wall Pain and Rib Fracture after Stereotactic Radiotherapy for Peripheral Non-small Cell Lung Cancer. J. Thorac. Oncol. 2009, 4, 1035–1037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunlap, N.E.; Cai, J.; Biedermann, G.B.; Yang, W.; Benedict, S.H.; Sheng, K.; Schefter, T.E.; Kavanagh, B.D.; Larner, J.M. Chest Wall Volume Receiving >30 Gy Predicts Risk of Severe Pain and/or Rib Fracture After Lung Stereotactic Body Radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, 796–801. [Google Scholar] [CrossRef]
- Lee, S.U.; Moon, S.H.; Cho, K.H.; Pyo, H.R.; Kim, J.Y.; Kim, D.Y.; Kim, T.H.; Suh, Y.G.; Kim, Y.J. Ablative Dose Proton Beam Therapy for Stage I and Recurrent Non-Small Cell Lung Carcinomas. Strahlenther. Onkol. 2016, 192, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Kadoya, N.; Obata, Y.; Kato, T.; Kagiya, M.; Nakamura, T.; Tomoda, T.; Takada, A.; Takayama, K.; Fuwa, N. Dose-Volume Comparison of Proton Radiotherapy and Stereotactic Body Radiotherapy for Non-Small-Cell Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 1225–1231. [Google Scholar] [CrossRef] [PubMed]
- Bayasgalan, U.; Moon, S.H.; Jeong, J.H.; Kim, T.H.; Cho, K.H.; Suh, Y.G. Treatment Outcomes of Passive Scattering Proton Beam Therapy for Stage I Non-Small Cell Lung Cancer. Radiat. Oncol. 2021, 16, 155. [Google Scholar] [CrossRef] [PubMed]
- Bayasgalan, U.; Moon, S.H.; Kim, T.H.; Kim, T.Y.; Lee, S.H.; Suh, Y.G. Dosimetric Comparisons Between Proton Beam Therapy and Modern Photon Radiation Techniques for Stage I Non-Small Cell Lung Cancer According to Tumor Location. Cancers 2021, 13, 6356. [Google Scholar] [CrossRef]
- Bert, C.; Grözinger, S.O.; Rietzel, E. Quantification of Interplay Effects of Scanned Particle Beams and Moving Targets. Phys. Med. Biol. 2008, 53, 2253–2265. [Google Scholar] [CrossRef] [PubMed]
- Paganetti, H. Range Uncertainties in Proton Therapy and the Role of Monte Carlo Simulations. Phys. Med. Biol. 2012, 57, R99–R117. [Google Scholar] [CrossRef] [PubMed]
- Baumann, K.S.; Flatten, V.; Weber, U.; Lautenschläger, S.; Eberle, F.; Zink, K.; Engenhart-Cabillic, R. Effects of the Bragg Peak Degradation Due to Lung Tissue in Proton Therapy of Lung Cancer Patients. Radiat. Oncol. 2019, 14, 183. [Google Scholar] [CrossRef]
- Casares-Magaz, O.; Toftegaard, J.; Muren, L.P.; Kallehauge, J.F.; Bassler, N.; Poulsen, P.R.; Petersen, J.B. A Method for Selection of Beam Angles Robust to Intra-Fractional Motion in Proton Therapy of Lung Cancer. Acta Oncol. 2014, 53, 1058–1063. [Google Scholar] [CrossRef]
- Yeo, C.D.; Lee, M.K.; Lee, S.H.; Kim, E.Y.; Lee, I.J.; Park, H.S.; Chang, Y.S. Indicators and Qualitative Assessment of Lung Cancer Management by Health Insurance Review and Assessment Service (HIRA) of Korea in 2015. Tuberc. Respir. Dis. 2018, 81, 19–28. [Google Scholar] [CrossRef]
- Kim, H.; Pyo, H.; Noh, J.M.; Lee, W.; Park, B.; Park, H.Y.; Yoo, H. Preliminary Result of Definitive Radiotherapy in Patients With Non-Small Cell Lung Cancer Who Have Underlying Idiopathic Pulmonary Fibrosis: Comparison Between X-ray and Proton Therapy. Radiat. Oncol. 2019, 14, 19. [Google Scholar] [CrossRef]
- Liao, Z.; Lee, J.J.; Komaki, R.; Gomez, D.R.; O’Reilly, M.S.; Fossella, F.V.; Blumenschein, G.R., Jr.; Heymach, J.V.; Vaporciyan, A.A.; Swisher, S.G.; et al. Bayesian Adaptive Randomization Trial of Passive Scattering Proton Therapy and Intensi-ty-Modulated Photon Radiotherapy for Locally Advanced Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2018, 36, 1813–1822. [Google Scholar] [CrossRef]
- Darby, S.C.; Ewertz, M.; McGale, P.; Bennet, A.M.; Blom-Goldman, U.; Brønnum, D.; Correa, C.; Cutter, D.; Gagliardi, G.; Gigante, B.; et al. Risk of Ischemic Heart Disease in Women After Radiotherapy for Breast Cancer. N. Engl. J. Med. 2013, 368, 987–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bongers, E.M.; Haasbeek, C.J.; Lagerwaard, F.J.; Slotman, B.J.; Senan, S. Incidence and Risk Factors for Chest Wall Toxicity After Risk-Adapted Stereotactic Radiotherapy for Early-Stage Lung Cancer. J. Thorac. Oncol. 2011, 6, 2052–2057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Creach, K.M.; El Naqa, I.; Bradley, J.D.; Olsen, J.R.; Parikh, P.J.; Drzymala, R.E.; Bloch, C.; Robinson, C.G. Dosimetric Predictors of Chest Wall Pain After Lung Stereotactic Body Radiotherapy. Radiother. Oncol. 2012, 104, 23–27. [Google Scholar] [CrossRef]
- Mutter, R.W.; Liu, F.; Abreu, A.; Yorke, E.; Jackson, A.; Rosenzweig, K.E. Dose-Volume Parameters Predict for the Devel-opment of Chest Wall Pain After Stereotactic Body Radiation for Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 1783–1790. [Google Scholar] [CrossRef] [Green Version]
- Moreno, A.C.; Fellman, B.; Hobbs, B.P.; Liao, Z.; Gomez, D.R.; Chen, A.; Hahn, S.M.; Chang, J.Y.; Lin, S.H. Biologically Effective Dose in Stereotactic Body Radiotherapy and Survival for Patients With Early-Stage NSCLC. J. Thorac. Oncol. 2020, 15, 101–109. [Google Scholar] [CrossRef]
- Koshy, M.; Malik, R.; Weichselbaum, R.R.; Sher, D.J. Increasing Radiation Therapy Dose Is Associated With Improved Survival in Patients Undergoing Stereotactic Body Radiation Therapy for Stage I Non-Small-Cell Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2015, 91, 344–350. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | All, No. (%) (n = 289) | Photon, No. (%) (n = 177) | Proton, No. (%) (n = 112) | p-Value |
|---|---|---|---|---|
| Age, years * | 76 (72–80) | 77 (72–81) | 75 (70–80) | 0.235 |
| Sex | ||||
| Male | 230 (79.6) | 139 (78.5) | 91 (81.2) | 0.683 |
| Female | 59 (20.4) | 38 (21.5) | 21 (18.8) | |
| Smoking history | ||||
| Never | 65 (22.5) | 42 (23.7) | 23 (20.5) | 0.052 |
| Former | 182 (63.0) | 103 (58.2) | 79 (70.5) | |
| Current | 42 (14.5) | 32 (18.1) | 10 (8.9) | |
| ECOG performance status | ||||
| 0 | 35 (12.1) | 21 (11.9) | 14 (12.5) | 0.004 |
| 1 | 213 (73.7) | 121 (68.4) | 92 (82.1) | |
| 2 | 37 (12.8) | 31 (17.5) | 6 (5.4) | |
| 3 | 4 (1.4) | 4 (2.3) | 0 | |
| Charlson comorbidity index | ||||
| 0 | 56 (19.4) | 32 (18.1) | 24 (21.4) | 0.494 |
| 1 | 86 (29.8) | 58 (32.8) | 28 (25.0) | |
| 2 | 63 (21.8) | 39 (22.0) | 24 (21.4) | |
| 3+ | 84 (29.1) | 48 (27.1) | 36 (32.1) | |
| Chronic lung disease | 0.119 | |||
| No | 113 (39.1) | 76 (42.9) | 37 (33.0) | |
| Yes | 176 (60.9) | 101 (57.1) | 75 (67.0) | |
| Baseline FEV1, % predicted * | 78.0 (59.0–96.0) | 78.5 (62.0–97.0) | 76 (55.0–92.0) | 0.324 |
| Baseline DLCO, % predicted † | 65.0 (21.2) | 68.3 (20.7) | 64.3 (21.9) | 0.137 |
| Characteristics | All, No. (%) (n = 289) | Photon, No. (%) (n = 177) | Proton, No. (%) (n = 112) | p-Value |
|---|---|---|---|---|
| Tumor histologic type | ||||
| Squamous cell carcinoma | 89 (30.8) | 53 (29.9) | 36 (32.1) | 0.263 |
| Adenocarcinoma | 88 (30.5) | 48 (27.1) | 40 (35.7) | |
| Others | 11 (3.8) | 7 (4.0) | 4 (3.6) | |
| Unproven | 101 (34.9) | 69 (39.0) | 32 (28.6) | |
| Tumor location | ||||
| Peripheral | 56 (19.4) | 36 (20.3) | 20 (17.9) | 0.454 |
| Close to chest wall | 157 (54.3) | 99 (55.9) | 58 (51.8) | |
| Central | 76 (26.3) | 42 (23.7) | 34 (30.4) | |
| Tumor lobar location | 0.033 | |||
| Left upper lobe | 67 (23.2) | 44 (24.9) | 23 (20.5) | |
| Left lower lobe | 74 (25.6) | 36 (20.3) | 38 (33.9) | |
| Right upper lobe | 87 (30.1) | 61 (34.5) | 26 (23.2) | |
| Right middle lobe | 14 (4.8) | 6 (3.4) | 8 (7.1) | |
| Right lower lobe | 47 (16.3) | 30 (16.9%) | 17 (15.2) | |
| T stage * | ||||
| T1a | 21 (7.3) | 11 (6.2) | 10 (8.9) | 0.802 |
| T1b | 94 (32.5) | 60 (33.9) | 34 (30.4) | |
| T1c | 91 (31.5) | 56 (31.6) | 35 (31.2) | |
| T2a | 83 (28.7) | 50 (28.2) | 33 (29.5) | |
| Total radiation dose, BED10 † (CGE) | ||||
| 75–100 | 60 (20.8) | 36 (20.3) | 24 (21.4) | <0.001 |
| 100–125 | 69 (23.9) | 24 (13.6) | 45 (40.2) | |
| 125–150 | 160 (55.4) | 117 (66.1) | 43 (38.4) | |
| Volume of ITV (cm3) ‡ | 29.3 (14.5–54.3) | 29.9 (15.6–54.4) | 28.4 (12.9–52.9) | 0.612 |
| Photon, No. (%) (n = 93) | Proton, No. (%) (n = 93) | p-Value | |
|---|---|---|---|
| Radiation pneumonitis | |||
| Grade 0 | 9 (9.7) | 12 (12.9) | 0.280 |
| Grade 1 | 73 (78.5) | 74 (79.6) | |
| Grade 2 | 10 (10.8) | 4 (4.3) | |
| Grade 3 | 1 (1.1) | 3 (3.2) | |
| Non-cardiac chest pain and chest wall pain | |||
| Grade 0 | 70 (75.3) | 79 (84.9) | 0.240 |
| Grade 1 | 20 (21.5) | 12 (12.9) | |
| Grade 2 | 3 (3.2) | 2 (2.2) | |
| Rib fracture | |||
| Grade 0 | 78 (83.9%) | 89 (95.7%) | 0.014 |
| Grade 1 | 14 (15.1%) | 4 (4.3) | |
| Grade 2 | 1 (1.1) | 0 (0.0) | |
| Aggravation of symptoms after treatment * | 53 (57.0) | 40 (39.3) | 0.078 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suh, Y.-G.; Noh, J.M.; Lee, D.Y.; Kim, T.H.; Bayasgalan, U.; Pyo, H.; Moon, S.H. Proton Beam Therapy versus Photon Radiotherapy for Stage I Non-Small Cell Lung Cancer. Cancers 2022, 14, 3627. https://doi.org/10.3390/cancers14153627
Suh Y-G, Noh JM, Lee DY, Kim TH, Bayasgalan U, Pyo H, Moon SH. Proton Beam Therapy versus Photon Radiotherapy for Stage I Non-Small Cell Lung Cancer. Cancers. 2022; 14(15):3627. https://doi.org/10.3390/cancers14153627
Chicago/Turabian StyleSuh, Yang-Gun, Jae Myoung Noh, Doo Yeul Lee, Tae Hyun Kim, Unurjargal Bayasgalan, Hongryull Pyo, and Sung Ho Moon. 2022. "Proton Beam Therapy versus Photon Radiotherapy for Stage I Non-Small Cell Lung Cancer" Cancers 14, no. 15: 3627. https://doi.org/10.3390/cancers14153627
APA StyleSuh, Y.-G., Noh, J. M., Lee, D. Y., Kim, T. H., Bayasgalan, U., Pyo, H., & Moon, S. H. (2022). Proton Beam Therapy versus Photon Radiotherapy for Stage I Non-Small Cell Lung Cancer. Cancers, 14(15), 3627. https://doi.org/10.3390/cancers14153627