
SMARCB1 (INI-1)-Deficient Sinonasal Carcinoma: A Systematic Review and Pooled Analysis of Treatment Outcomes

 , , , , ,
, , , , ,
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
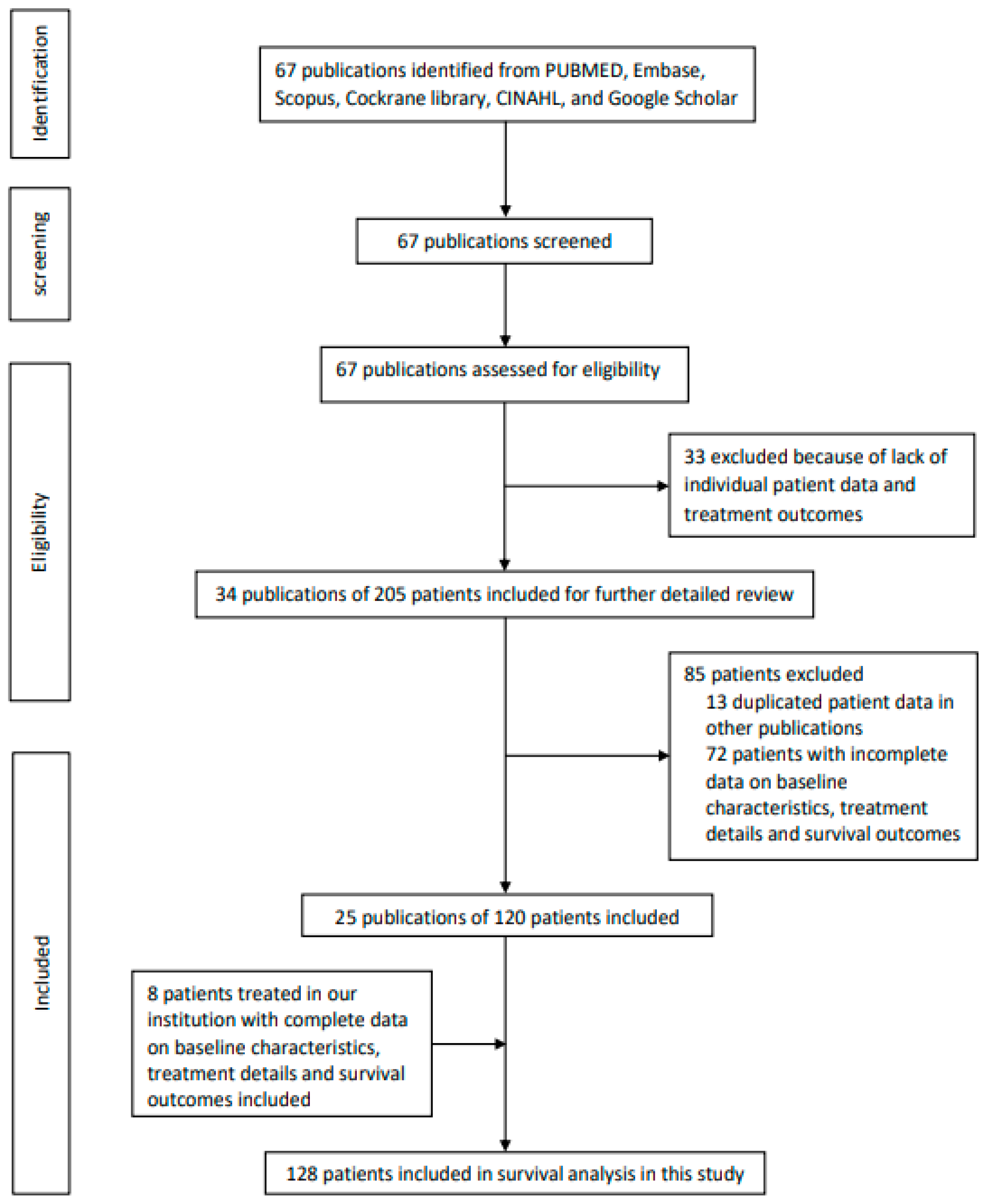
2.1. Search Strategy and Selection Criteria
2.2. Survival Analysis
3. Results
3.1. Search Strategy Results
3.2. Histology and Cytomorphology of Tumor Samples
3.3. Deletional Status of SMARCB1 by Further Molecular and Genetic/Genomic Diagnostics
3.4. Treatment Outcomes of Patients in Our Institution
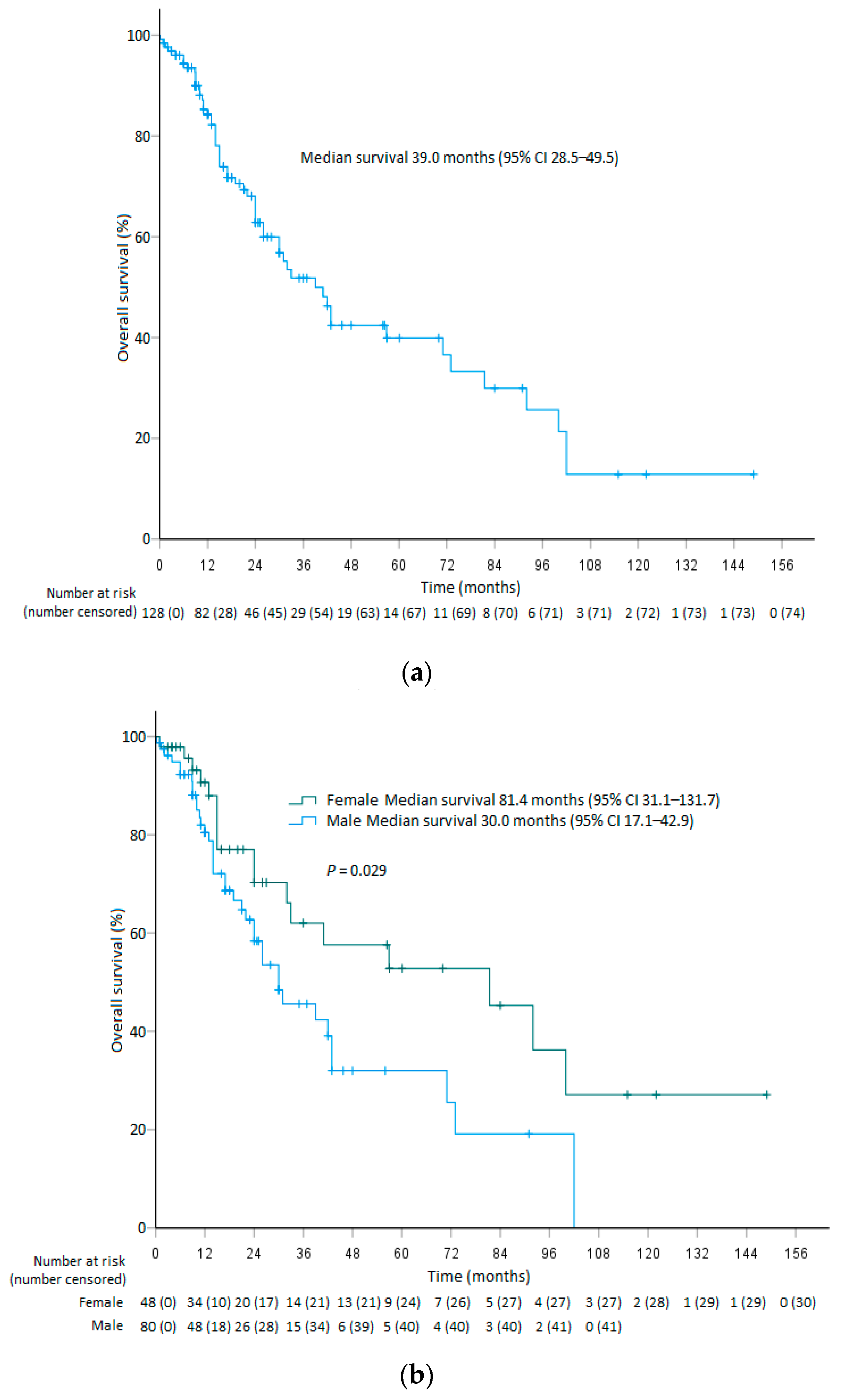
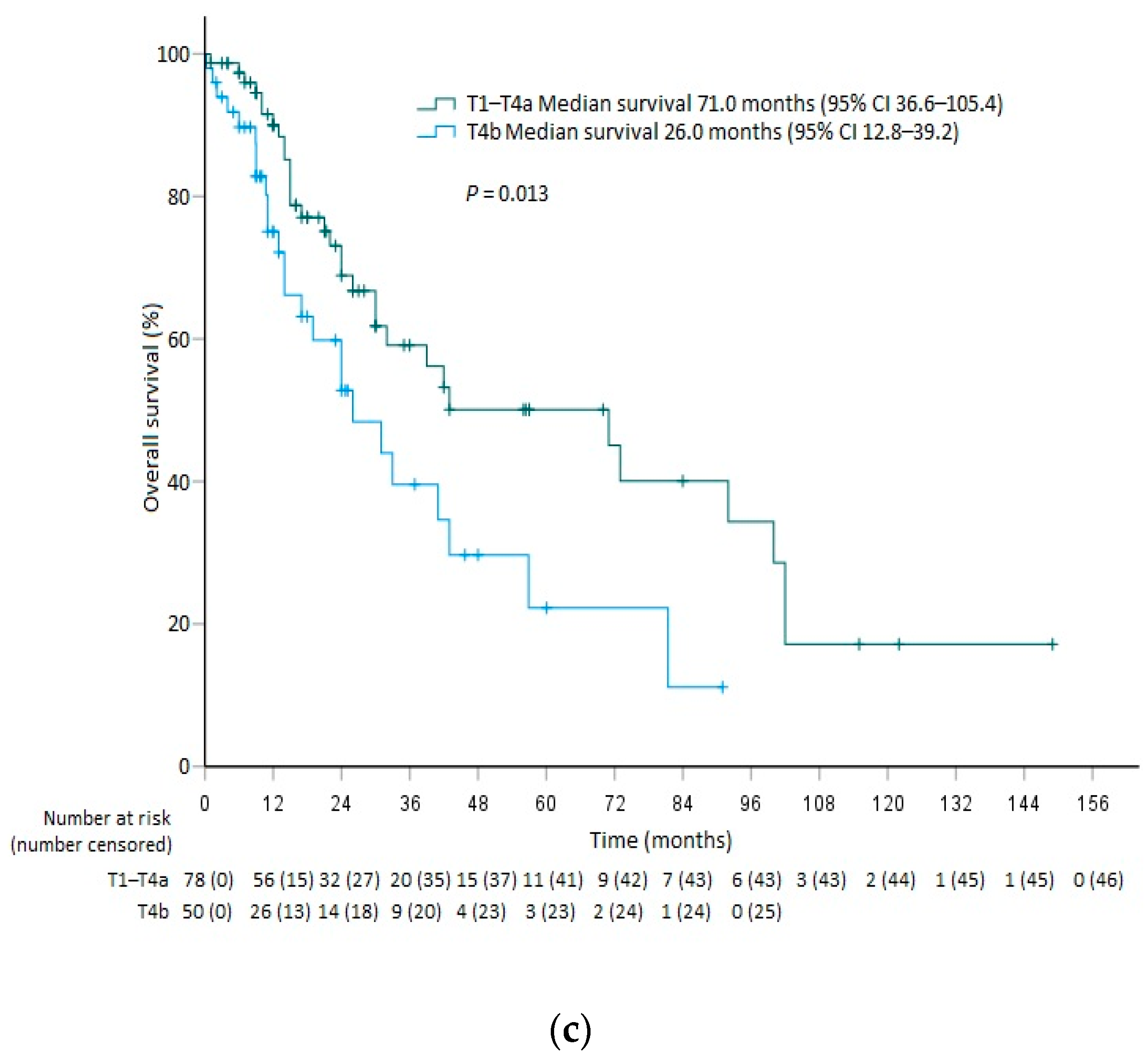
3.5. Survival Analysis
3.6. Prognostic Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Agaimy, A.; Koch, M.; Lell, M.; Semrau, S.; Dudek, W.; Wachter, D.L.; Knöll, A.; Iro, H.; Haller, F.; Hartmann, A. SMARCB1(INI1)-deficient sinonasal basaloid carcinoma: A novel member of the expanding family of SMARCB1-deficient neoplasms. Am. J. Surg. Pathol. 2014, 38, 1274–1281. [Google Scholar] [CrossRef] [PubMed]
- Bishop, J.A.; Antonescu, C.R.; Westra, W.H. SMARCB1 (INI-1)-deficient carcinomas of the sinonasal tract. Am. J. Surg. Pathol. 2014, 38, 1282–1289. [Google Scholar] [CrossRef] [PubMed]
- Judkins, A.R. Immunohistochemistry of INI1 expression: A new tool for old challenges in CNS and soft tissue pathology. Adv. Anat. Pathol. 2007, 14, 335–339. [Google Scholar] [CrossRef]
- El-Naggar, A.K.; Chan, J.K.C.; Grandis, J.R.; Takata, T.; Slootweg, P.J. WHO Classification of Head and Neck Tumours, 4th eds.; International Agency for Research on Cancer: Lyon, France, 2017. [Google Scholar]
- Morand, G.B.; Anderegg, N.; Vital, D.; Ikenberg, K.; Huber, G.F.; Soyka, M.B.; Egger, M.; Holzmann, D. Outcome by treatment modality in sinonasal undifferentiated carcinoma (SNUC): A case-series, systematic review and meta-analysis. Oral Oncol. 2017, 75, 28–34. [Google Scholar] [CrossRef]
- Reiersen, D.A.; Pahilan, M.E.; Devaiah, A.K. Meta-analysis of treatment outcomes for sinonasal undifferentiated carcinoma. Otolaryngol. Head Neck Surg. 2012, 147, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Kuo, P.; Manes, R.P.; Schwam, Z.G.; Judson, B.J. Survival outcomes for combined modality therapy for sinonasal undifferentiated carcinoma. Otolaryngol. Head Neck Surg. 2017, 156, 132–136. [Google Scholar] [CrossRef]
- Bhasker, S.; Mallick, S.; Benson, R.; Bhanuprasad, V.; Sharma, A.; Thakar, A. A multimodality approach to sinonasal undifferentiated carcinoma: A single institute experience. J. Laryngol. Otol. 2017, 131, 19–25. [Google Scholar] [CrossRef]
- Amit, M.; Abdelmeguid, A.S.; Watcherporn, T.; Takahashi, H.; Tam, S.; Bell, D.; Ferrarotto, R.; Glisson, B.; Kupferman, M.E.; Roberts, D.M.; et al. Induction chemotherapy response as a guide for treatment optimization in sinonasal undifferentiated carcinoma. J. Clin. Oncol. 2019, 37, 504–512. [Google Scholar] [CrossRef]
- ECOG-ACRIN Cancer Research Group; National Cancer Institute (NCI). Chemotherapy Before Surgery and Radiation Therapy or Surgery and Radiation Therapy Alone in Treating Patients with Nasal and Paranasal Sinus Cancer That Can Be Removed by Surgery. Available online: https://clinicaltrials.gov/ct2/show/NCT03493425 (accessed on 15 May 2022).
- Jamshidi, F.; Pleasance, E.; Li, Y.; Shen, Y.; Kasaian, K.; Corbett, R.; Eirew, P.; Lum, A.; Pandoh, P.; Zhao, Y.; et al. Diagnostic value of next-generation sequencing in an unusual sphenoid tumor. Oncologist 2014, 19, 623–630. [Google Scholar] [CrossRef]
- Bell, D.; Hanna, E.Y.; Agaimy, A.; Weissferdt, A. Reappraisal of sinonasal undifferentiated carcinoma: SMARCB1 (INI1)-deficient sinonasal carcinoma: A single-institution experience. Virchows Arch. 2015, 467, 649–656. [Google Scholar] [CrossRef]
- Allison, D.B.; Bishop, J.A.; Ali, S.Z. Cytopathologic characteristics of SMARCB1 (INI-1) deficient sinonasal carcinoma: A potential diagnostic pitfall. Diagn. Cytopathol. 2016, 44, 700–703. [Google Scholar] [CrossRef] [PubMed]
- Zeng, M.; Chen, C.; Yang, S.; Chen, X. SMARCB1 (INI1)-deficient sinonasal carcinoma: A newly described entity. Int. J. Clin. Exp. Pathol. 2016, 9, 3454–3458. [Google Scholar]
- Shatzkes, D.R.; Ginsberg, L.E.; Wong, M.; Aiken, A.H.; Branstetter, B.F., IV; Michel, M.A.; Aygun, N. Imaging appearance of SMARCB1 (INI1)-deficient sinonasal carcinoma: A newly described sinonasal malignancy. AJNR Am. J. Neuroradiol. 2016, 37, 1925–1929. [Google Scholar] [CrossRef] [PubMed]
- Agaimy, A.; Hartmann, A.; Antonescu, C.R.; Chiosea, S.I.; El-Mofty, S.K.; Geddert, H.; Iro, H.; Lewis, J.S., Jr.; Märkl, B.; Mills, S.E.; et al. SMARCB1 (INI-1)-deficient Sinonasal Carcinoma: A series of 39 cases expanding the morphologic and clinicopathologic spectrum of a recently described entity. Am. J. Surg. Pathol. 2017, 41, 458–471. [Google Scholar] [CrossRef] [PubMed]
- Wasserman, J.K.; Dickson, B.C.; Perez-Ordonez, B.; de Almeida, J.R.; Irish, J.C.; Weinreb, I. INI1 (SMARCB1)-deficient sinonasal carcinoma: A clinicopathologic report of 2 cases. Head Neck Pathol. 2017, 11, 256–261. [Google Scholar] [CrossRef]
- Laco, J.; Chmelařová, M.; Vošmiková, H.; Sieglová, K.; Bubancová, I.; Dundr, P.; Němejcová, K.; Michálek, J.; Čelakovský, P.; Mottl, R.; et al. SMARCB1/INI1-deficient sinonasal carcinoma shows methylation of RASSF1 gene: A clinicopathological, immunohistochemical and molecular genetic study of a recently described entity. Pathol. Res. Pract. 2017, 213, 133–342. [Google Scholar] [CrossRef]
- Dogan, S.; Chute, D.J.; Xu, B.; Ptashkin, R.N.; Chandramohan, R.; Casanova-Murphy, J.; Nafa, K.; Bishop, J.A.; Chiosea, S.I.; Stelow, E.B.; et al. Frequent IDH2 R172 mutations in undifferentiated and poorly-differentiated sinonasal carcinomas. J. Pathol. 2017, 242, 400–408. [Google Scholar] [CrossRef]
- Zamecnik, M.; Rychnovsky, J.; Syrovatka, J. Sinonasal SMARCB1 (INI1) deficient carcinoma with yolk sac tumor differentiation: Report of a case and comparison with INI1 expression in gonadal germ cell tumors. Int. J. Surg. Pathol. 2018, 26, 245–249. [Google Scholar] [CrossRef]
- Laco, J.; Kovaříková, H.; Chmelařová, M.; Vošmiková, H.; Sieglová, K.; Baranová, I.; Dundr, P.; Němejcová, K.; Michálek, J.; Šatanková, J.; et al. MicroRNA expression in SMARCB1/INI1-deficient sinonasal carcinoma: A clinicopathological and molecular genetic study. Virchows Arch. 2018, 472, 871–875. [Google Scholar] [CrossRef]
- Allard, F.D.; Bell, D.; Stelow, E. Cytopathologic features of SMARCB1 (INI-1)-deficient sinonasal carcinoma. Cancer Cytopathol. 2018, 126, 567–574. [Google Scholar] [CrossRef]
- Kakkar, A.; Antony, V.M.; Pramanik, R.; Sakthivel, P.; Singh, C.A.; Jain, D. SMARCB1 (INI1)-deficient sinonasal carcinoma: A series of 13 cases with assessment of histologic patterns. Hum. Pathol. 2019, 83, 59–67. [Google Scholar] [CrossRef] [PubMed]
- McHugh, K.E.; Policarpio-Nicolas, M.L.C. Metastatic SMARCB1 (INI-1)-deficient sinonasal carcinoma diagnosed by endobronchial ultrasound-guided fine-needle aspiration (EBUS-FNA): A potential diagnostic pitfall and review of the literature. Acta Cytol. 2019, 63, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Acevedo, H.; Patterson, J.D.; Sardar, S.; Gokden, M.; Das, B.C.; Ussery, D.W.; Rodriguez, A. SMARC-B1 deficient sinonasal carcinoma metastasis to the brain with next generation sequencing data: A case report of perineural invasion progressing to leptomeningeal invasion. BMC Cancer 2019, 19, 827. [Google Scholar] [CrossRef] [PubMed]
- Trieu, V.; Aulet, R.M.; Ciolino, A.; Rimash, T. SMARCB1-deficient sinonasal carcinoma: A case report and discussion of the clinical implications. Ann. Otol. Rhinol. Laryngol. 2019, 128, 676–680. [Google Scholar] [CrossRef] [PubMed]
- Vaziri Fard, E.; Zhang, S.; Cai, Z.; Ding, J.; Sun, Q.; Saluja, K.; Zhu, H. Sinonasal undifferentiated carcinoma: Clinicopathological spectrums and diagnosis reappraisal. Hum. Pathol. 2019, 89, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Dogan, S.; Vasudevaraja, V.; Xu, B.; Serrano, J.; Ptashkin, R.N.; Jung, H.J.; Chang, S.; Jungbluth, A.A.; Cohen, M.A.; Ganly, I.; et al. DNA methylation-based classification of sinonasal undifferentiated carcinoma. Mod. Pathol. 2019, 32, 1447–1459. [Google Scholar] [CrossRef]
- Parsel, S.M.; Jawad, B.A.; McCoul, E.D. SMARCB1-deficient sinonasal carcinoma: Systematic review and case report. World Neurosurg. 2020, 136, 305–310. [Google Scholar] [CrossRef]
- Shah, A.A.; Jain, D.; Ababneh, E.; Agaimy, A.; Hoschar, A.P.; Grifth, C.C. SMARCB1 (INI–1)–deficient adenocarcinoma of the sinonasal tract: A potentially under–recognized form of sinonasal adenocarcinoma with occasional yolk sac tumor–like features. Head Neck Pathol. 2020, 14, 465–472. [Google Scholar] [CrossRef]
- Levitan, I.; Fichman, S.; Laviv, Y. Fulminant presentation of a SMARCB1-deficient, anterior cranial fossa tumor in adult. Surg. Neurol. Int. 2020, 11, 195. [Google Scholar] [CrossRef]
- Shanti, R.M.; Farahi, A.; Curry, J.M.; Alawi, F. SMARCB1 (Integrase Interactor 1)-deficient sinonasal carcinoma of the maxillary sinus: A newly described sinonasal neoplasm. J. Oral Maxillofac. Surg. 2020, 78, 1870.e1–1870.e6. [Google Scholar] [CrossRef]
- Chitguppi, C.; Rabinowitz, M.R.; Johnson, J.; Bar-Ad, V.; Fastenberg, J.H.; Molligan, J.; Berman, E.; Nyquist, G.G.; Rosen, M.R.; Evans, J.E.; et al. Loss of SMARCB1 expression confers poor prognosis to sinonasal undifferentiated carcinoma. J. Neurol. Surg. B Skull Base 2020, 81, 610–619. [Google Scholar] [CrossRef] [PubMed]
- Dogan, S.; Cotzia, P.; Ptashkin, R.N.; Nanjangud, G.J.; Xu, B.; Boroujeni, A.M.; Cohen, M.A.; Pfister, D.G.; Prasad, M.L.; Antonescu, C.R.; et al. Genetic basis of SMARCB1 protein loss in 22 sinonasal carcinomas. Hum. Pathol. 2020, 104, 105–116. [Google Scholar] [CrossRef]
- Shaverdashvili, K.; Azimi-Nekoo, E.; Cohen, P.; Akbar, N.; Ow, T.J.; Halmos, B.; Castellucci, E. INI-1 (SMARCB1)-deficient undifferentiated sinonasal carcinoma: Novel paradigm of molecular testing in the diagnosis and management of sinonasal malignancies. Oncologist 2020, 25, 738–744. [Google Scholar] [CrossRef] [PubMed]
- Libera, L.; Ottini, G.; Sahnane, N.; Pettenon, F.; Turri-Zanoni, M.; Lambertoni, A.; Chiaravalli, A.M.; Leone, F.; Battaglia, P.; Castelnuovo, P.; et al. Methylation drivers and prognostic implications in sinonasal poorly differentiated carcinomas. Cancers 2021, 13, 5030. [Google Scholar] [CrossRef] [PubMed]
- Li, C.Y.; Han, Y.M.; Xu, K.; Wu, S.Y.; Lin, X.Y.; Cao, H.Y. Case Report: SMARCB1 (INI-1)-Deficient Carcinoma of the Nasal Cavity with Pure Yolk Sac Tumor Differentiation and Elevated Serum AFP Levels. Onco. Targets Ther. 2021, 14, 2227–2233. [Google Scholar] [CrossRef] [PubMed]
- Yanagawa, N.; Suzuki, M.; Sugimoto, R.; Osakabe, M.; Uesugi, N.; Shiga, K.; Sugai, T. SMARCB1-deficient sinonasal carcinoma: A case report and literature review. J. Surg. Case Rep. 2021, 2021, rjab161. [Google Scholar] [CrossRef]
- Ayyanar, P.; Mishra, P.; Preetam, C.; Adhya, A.K. SMARCB1/INI1 deficient sino-nasal carcinoma: Extending the histomorphological features. Head Neck Pathol. 2021, 15, 555–565. [Google Scholar] [CrossRef]
- Hazir, B.; Şímșek, B.; Erdemír, A.; Gürler, F.; Yazici, O.; Kizil, Y.; Aydíl, U. Sinonasal SMARCB1 (INI1) deficient carcinoma with yolk sac tumor differentiation: A case report and treatment options. Head Neck Pathol. 2022, 16, 596–601. [Google Scholar] [CrossRef]
- Su, Y.J.; Lee, Y.H.; Hsieh, M.S. SMARCB1(INI1)-deficient sinonasal adenocarcinoma: Report of a case previously diagnosed as high-grade non-intestinal-type sinonasal adenocarcinoma. Pathol. Int. 2022, 72, 53–58. [Google Scholar] [CrossRef]
- Wang, R.; Wang, L.; Fang, J.; Zhong, Q.; Hou, L.; Ma, H.; Feng, L.; He, S.; Wang, C.; Zhang, L. Clinical diagnosis and treatment analyses on SMARCB1 (INI-1)-deficient sinonasal carcinoma: Case series with systematic review of the literature. World Neurosurg. 2022, 161, e229–e243. [Google Scholar] [CrossRef]
- Agaimy, A.; Bishop, J.A. SWI/SNF-deficient head and neck neoplasms: An overview. Semin. Diagn. Pathol. 2021, 38, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Glöss, S.; Jurmeister, P.; Thieme, A.; Schmid, S.; Cai, W.Y.; Serrette, R.N.; Perner, S.; Ribbat-Idel, J.; Pagenstecher, A.; Bläker, H.; et al. IDH2 R172 mutations across poorly differentiated sinonasal tract malignancies: Forty molecularly homogeneous and histologically variable cases with favorable outcome. Am. J. Surg. Pathol. 2021, 45, 1190–1204. [Google Scholar] [CrossRef]
- Chen, A.M.; Daly, M.E.; El-Sayed, I.; Garcia, J.; Lee, N.Y.; Bucci, M.K.; Kaplan, M.J. Patterns of failure after combined-modality approaches incorporating radiotherapy for sinonasal undifferentiated carcinoma of the head and neck. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Mourad, W.F.; Hauerstock, D.; Shourbaji, R.A.; Hu, K.S.; Culliney, B.; Li, Z.; Jacobson, A.; Tran, T.; Manolidis, S.; Schantz, S.; et al. Trimodality management of sinonasal undifferentiated carcinoma and review of the literature. Am. J. Clin. Oncol. 2013, 36, 584–588. [Google Scholar] [CrossRef] [PubMed]
- Al-Mamgani, A.; van Rooij, P.; Mehilal, R.; Tans, L.; Levendag, P.C. Combined-modality treatment improved outcome in sinonasal undifferentiated carcinoma: Single-institutional experience of 21 patients and review of the literature. Eur. Arch. Otorhinolaryngol. 2013, 270, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulières, D.; Tahara, M.; de Castro, G., Jr.; Psyrri, M.; Basté, N.; Neupane, P.; Bratland, A.; et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): A randomised, open-label, phase 3 study. Lancet 2019, 394, 1915–1928. [Google Scholar] [CrossRef]
- National Cancer Institute (NCI). Nivolumab and Ipilimumab in Treating Patients with Rare Tumors. Available online: https://clinicaltrials.gov/ct2/show/NCT02834013 (accessed on 15 May 2022).
- H. Lee Moffitt Cancer Center and Research Institute; James and Esther King Biomedical Research Program; Eli Lilly and Company; Bristol-Myers Squibb. Cetuximab & Nivolumab in Patients with Recurrent/Metastatic Head & Neck Squamous Cell Carcinoma. Available online: https://clinicaltrials.gov/ct2/show/NCT03370276 (accessed on 15 May 2022).
- Pasini, D.; Di Croce, L. Emerging roles for Polycomb proteins in cancer. Curr. Opin. Genet. Dev. 2016, 36, 50–58. [Google Scholar] [CrossRef]
- Knutson, S.K.; Warholic, N.M.; Wigle, T.J.; Klaus, C.R.; Allain, C.J.; Raimondi, A.; Scott, M.P.; Chesworth, R.; Moyer, M.P.; Copeland, R.A.; et al. Durable tumor regression in genetically altered malignant rhabdoid tumors by inhibition of methyltransferase EZH2. Proc. Natl. Acad. Sci. USA 2013, 110, 7922–7927. [Google Scholar] [CrossRef]
- Yamaguchi, H.; Hung, M.C. Regulation and Role of EZH2 in Cancer. Cancer Res. Treat. 2014, 46, 209–222. [Google Scholar] [CrossRef]
- Burmeister, T. EZH2: A pleiotropic protein. Blood 2016, 128, 888–889. [Google Scholar] [CrossRef]
- Italiano, A.; Soria, J.C.; Toulmonde, M.; Michot, J.M.; Lucchesi, C.; Varga, A.; Coindre, J.M.; Blakemore, S.J.; Clawson, A.; Suttle, B.; et al. Tazemetostat, an EZH2 inhibitor, in relapsed or refractory B-cell non-Hodgkin lymphoma and advanced solid tumours: A first-in-human, open-label, phase 1 study. Lancet Oncol. 2018, 19, 649–659. [Google Scholar] [CrossRef]
- Morschhauser, F.; Tilly, H.; Chaidos, A.; McKay, P.; Philips, T.; Assouline, S.; Batlevi, C.L.; Campbell, P.; Ribrag, V.; Damaj, G.L.; et al. Tazemetostat for patients with relapsed or refractory follicular lymphoma: An open-label, single-arm, multicentre, phase 2 trial. Lancet Oncol. 2020, 21, 1433–1442. [Google Scholar] [CrossRef]
- Gounder, M.; Schöffski, P.; Jones, R.L.; Agulnik, M.; Cote, G.M.; Villalobos, V.M.; Attia, S.; Chugh, R.; Chen, T.W.W.; Jahan, T.; et al. Tazemetostat in advanced epithelioid sarcoma with loss of INI1/SMARCB1: An international, open-label, phase 2 basket study. Lancet Oncol. 2020, 21, 1423–1432. [Google Scholar] [CrossRef]
- Epizyme, Inc. A Phase I Study of the EZH2 Inhibitor Tazemetostat in Pediatric Subjects with Relapsed or Refractory INI1-Negative Tumors or Synovial Sarcoma. Available online: https://clinicaltrials.gov/ct2/show/NCT02601937 (accessed on 15 May 2022).
- National Cancer Institute (NCI). Tazemetostat in Treating Patients with Relapsed or Refractory Advanced Solid Tumors, Non-Hodgkin Lymphoma, or Histiocytic Disorders with EZH2, SMARCB1, or SMARCA4 Gene Mutations (A Pediatric MATCH Treatment Trial). Available online: https://clinicaltrials.gov/ct2/show/NCT03213665 (accessed on 15 May 2022).
- Epizyme, Inc. Tazemeostat in Malignant Peripheral Nerve Sheath Tumors. Available online: https://clinicaltrials.gov/ct2/show/NCT04917042 (accessed on 15 May 2022).
- Lee, V.H.F. Induction Chemotherapy and Tazemetostat for Locally Advanced SMARCB1-Deficient Sinonasal Carcinoma. Available online: https://clinicaltrials.gov/ct2/show/NCT05151588 (accessed on 15 May 2022).
- Russo, A.L.; Adams, J.A.; Weyman, E.A.; Busse, P.M.; Goldberg, S.I.; Varvares, M.; Deschler, D.D.; Lin, D.T.; Delaney, T.F.; Chan, A.W. Long-term outcomes after proton beam therapy for sinonasal squamous cell carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 368–376. [Google Scholar] [CrossRef]
- Dagan, R.; Bryant, C.; Li, Z.; Yeung, D.; Justice, J.; Dzieglewiski, P.; Werning, J.; Fernandes, R.; Pirgousis, P.; Lanza, D.C.; et al. Outcomes of sinonasal cancer treated with proton therapy. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 377–385. [Google Scholar] [CrossRef]
- Pasalic, D.; Ludmir, E.B.; Allen, P.K.; Thaker, N.J.; Chapman, B.V.; Hanna, E.Y.; Su, S.Y.; Ferrarotto, R.; Glisson, B.S.; Reddy, J.P.; et al. Patient-reported outcomes, physician-reported toxicities, and treatment outcomes in a modern cohort of patients with sinonasal cancer treated using proton beam therapy. Radiother. Oncol. 2020, 148, 258–266. [Google Scholar] [CrossRef]
- Yu, N.Y.; Gamez, M.E.; Hartsell, W.F.; Tsai, H.K.; Laramore, G.E.; Larson, G.L.; Simone, C.B., II; Rossi, C.; Katz, S.R.; Buras, M.R.; et al. A multi-Institutional experience of proton beam therapy for sinonasal tumors. Adv. Radiat. Oncol. 2019, 4, 689–698. [Google Scholar] [CrossRef]
- Hu, W.; Hu, J.; Huang, Q.; Gao, J.; Yang, J.; Qiu, X.; Kong, L.; Lu, J.J. Particle beam radiation therapy for sinonasal malignancies: Single institutional experience at the Shanghai Proton and Heavy Ion Center. Cancer Med. 2020, 9, 7914–7924. [Google Scholar] [CrossRef]
- Zhang, W.; Hu, W.; Hu, J.; Gao, J.; Yang, J.; Kong, L.; Lu, J.J. Carbon ion radiation therapy for sinonasal malignancies: Promising results from 2282 cases from the real world. Cancer Sci. 2020, 111, 4465–4479. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | No. of Patients (%) Total (n = 128) |
|---|---|
| Median age, years (range) | 53 (20–89) |
| Sex | |
| Male | 80 (62.5) |
| Female | 48 (37.5) |
| T category (Supplementary Table S1 for definition) | |
| T1 | 5 (3.9) |
| T2 | 6 (4.7) |
| T3 | 14 (10.9) |
| T4a | 53 (41.4) |
| T4b | 50 (39.1) |
| N category (Supplementary Table S1 for definition) | |
| N0 | 104 (81.3) |
| N1 | 4 (3.1) |
| N2 | 4 (3.1) |
| Undetermined | 16 (12.5) |
| M category | |
| M0 (no distant metastasis) | 105 (82.0) |
| M1 (distant metastasis) | 7 (5.5) |
| Undetermined | 16 (12.5) |
| Radical resection performed | 79 (63.3) |
| Induction treatment received | |
| Yes | 26 (20.3) |
| No | 87 (68.0) |
| Undetermined | 15 (11.7) |
| Adjuvant treatment received | |
| Yes | 72 (56.3) |
| No | 41 (32.0) |
| Undetermined | 15 (11.7) |
| Multimodality treatment received | |
| Yes | 96 (75.0) |
| No | 17 (13.3) |
| Undetermined | 15 (11.7) |
| Only best supportive care received | 1 (0.8) |
| Predominant Microscopic Morphological Features | No. of Patients (%) Total (n = 192) |
|---|---|
| Basaloid ± other features | |
| Basaloid only | 60 (31.3) |
| Basaloid, spindled and adenoid | 1 (0.5) |
| Basaloid and focal clear cells | 1 (0.5) |
| Basaloid and squamoid | 2 (1.0) |
| Basaloid and rhabdoid | 4 (2.1) |
| Plasmacytoid/rhabdoid ± other features | |
| Plasmacytoid/rhabdoid | 32 (16.7) |
| Plasmacytoid/rhabdoid and squamoid | 1 (0.5) |
| Plasmacytoid/rhabdoid and adenoid | 1 (0.5) |
| Plasmacytoid/rhabdoid and glandular differentiation | 1 (0.5) |
| Plasmacytoid/rhabdoid and focal clear cells | 1 (0.5) |
| Plasmacytoid/rhabdoid and oncocytoid | 1 (0.5) |
| Undifferentiated carcinoma | 15 (7.8) |
| Squamous cell carcinoma | 7 (3.6) |
| Adenocarcinoma | 6 (3.1) |
| Pseudoglandular differentiation | 4 (2.1) |
| Squamoid differentiation | 3 (1.6) |
| Small cell carcinoma | 1 (0.5) |
| Poorly differentiated carcinoma | 1 (0.5) |
| Sarcomatoid differentiation | 1 (0.5) |
| High-grade mixed germ cell tumor | 1 (0.5) |
| Yolk sac differentiation | 1 (0.5) |
| Pseudoalveolar and pseudoglandular differentiation | 1 (0.5) |
| Undetermined | 46 (24.0) |
| Covariate | Univariable Analysis | Multivariable Analysis * | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | |
| Age (every 1-year increment) | 1.012 | 0.995–1.030 | 0.180 | - | - | - |
| Sex (female as reference) | 1.856 | 1.051–3.276 | 0.029 | 1.808 | 0.981–3.302 | 0.061 |
| T category (T1 as reference) | ||||||
| T2 | 1.001 | 0.008–12.879 | 0.968 | - | - | - |
| T3 | 2.012 | 0.604–6.711 | 0.255 | - | - | - |
| T4a | 1.706 | 0.696–4.184 | 0.243 | - | - | - |
| T4b | 1.869 | 1.030–3.390 | 0.013 | 1.952 | 1.134–3.358 | 0.017 |
| N category (N0 as reference) | ||||||
| N1 | 1.553 | 0.371–6.503 | 0.547 | - | - | - |
| N2 | 1.439 | 0.240–8.614 | 0.690 | - | - | - |
| M1 disease (M0 as reference) | 2.018 | 0.277–14.717 | 0.489 | - | - | - |
| Induction treatment | 0.925 | 0.464–1.842 | 0.824 | - | - | - |
| Adjuvant treatment | 0.946 | 0.498–1.797 | 0.866 | - | - | - |
| Multimodality treatment | 1.260 | 0.530–2.994 | 0.601 | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, V.H.-F.; Tsang, R.K.-Y.; Lo, A.W.I.; Chan, S.-Y.; Chung, J.C.-K.; Tong, C.-C.; Leung, T.-W.; Kwong, D.L.-W. SMARCB1 (INI-1)-Deficient Sinonasal Carcinoma: A Systematic Review and Pooled Analysis of Treatment Outcomes. Cancers 2022, 14, 3285. https://doi.org/10.3390/cancers14133285
Lee VH-F, Tsang RK-Y, Lo AWI, Chan S-Y, Chung JC-K, Tong C-C, Leung T-W, Kwong DL-W. SMARCB1 (INI-1)-Deficient Sinonasal Carcinoma: A Systematic Review and Pooled Analysis of Treatment Outcomes. Cancers. 2022; 14(13):3285. https://doi.org/10.3390/cancers14133285
Chicago/Turabian StyleLee, Victor Ho-Fun, Raymond King-Yin Tsang, Anthony Wing Ip Lo, Sum-Yin Chan, Joseph Chun-Kit Chung, Chi-Chung Tong, To-Wai Leung, and Dora Lai-Wan Kwong. 2022. "SMARCB1 (INI-1)-Deficient Sinonasal Carcinoma: A Systematic Review and Pooled Analysis of Treatment Outcomes" Cancers 14, no. 13: 3285. https://doi.org/10.3390/cancers14133285
APA StyleLee, V. H.-F., Tsang, R. K.-Y., Lo, A. W. I., Chan, S.-Y., Chung, J. C.-K., Tong, C.-C., Leung, T.-W., & Kwong, D. L.-W. (2022). SMARCB1 (INI-1)-Deficient Sinonasal Carcinoma: A Systematic Review and Pooled Analysis of Treatment Outcomes. Cancers, 14(13), 3285. https://doi.org/10.3390/cancers14133285