
Intratumoral Switch of Molecular Phenotype and Overall Survival in Muscle Invasive Bladder Cancer

 , ,
, , 
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Case Selection
2.2. Pathological and Immunohistochemical Evaluation
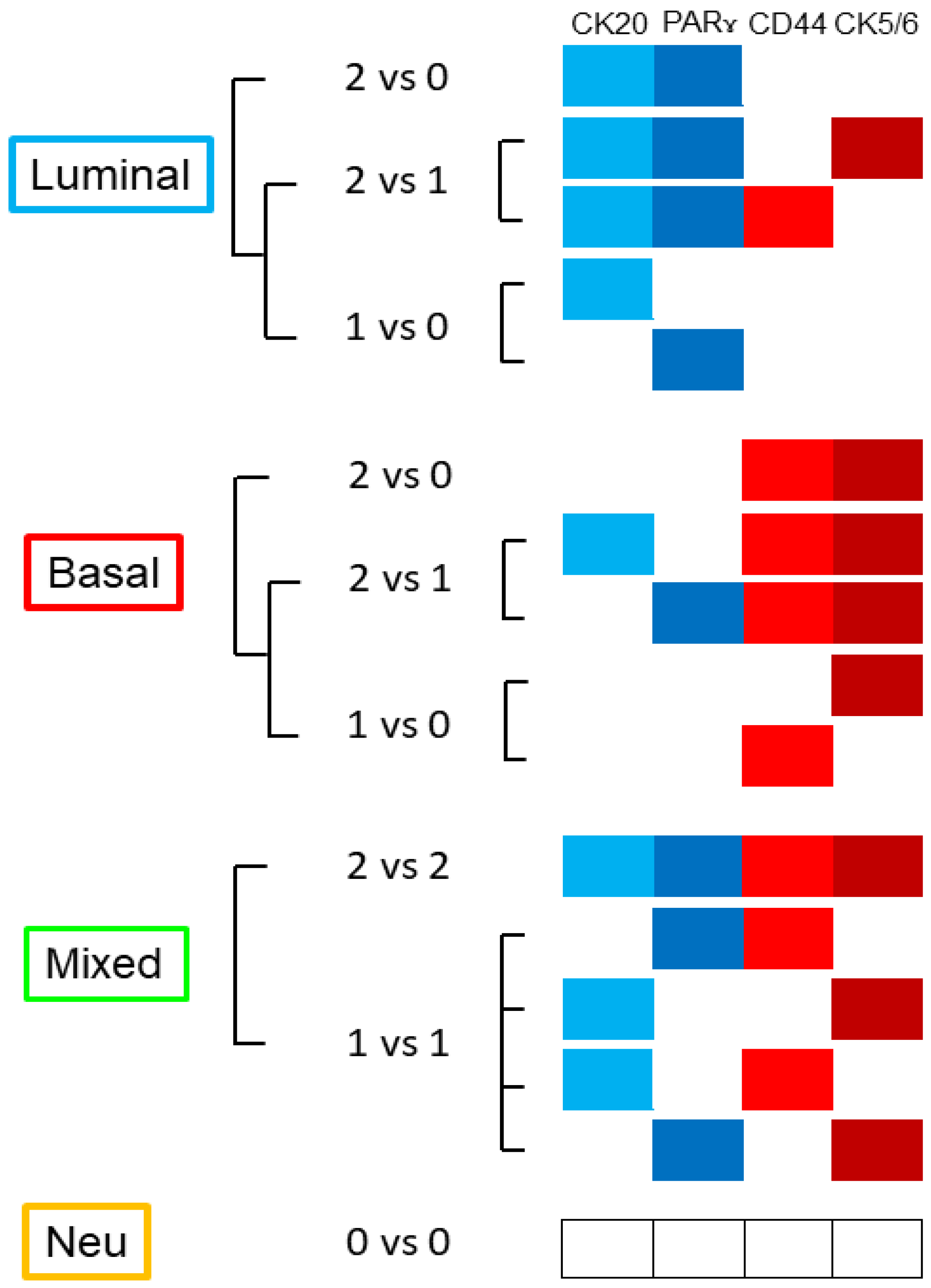
2.3. Identification of Luminal, Basal, Mixed, or Neu-Like Phenotype in pT2 Carcinoma
2.4. Molecular Identification of CD44, CK5/6, CK20, and pPARγ through qRT-PCR Assay
2.5. Statistical Analysis
3. Results
3.1. Clinical and Pathological Characteristics of Patients and Definition of the Different Molecular Groups
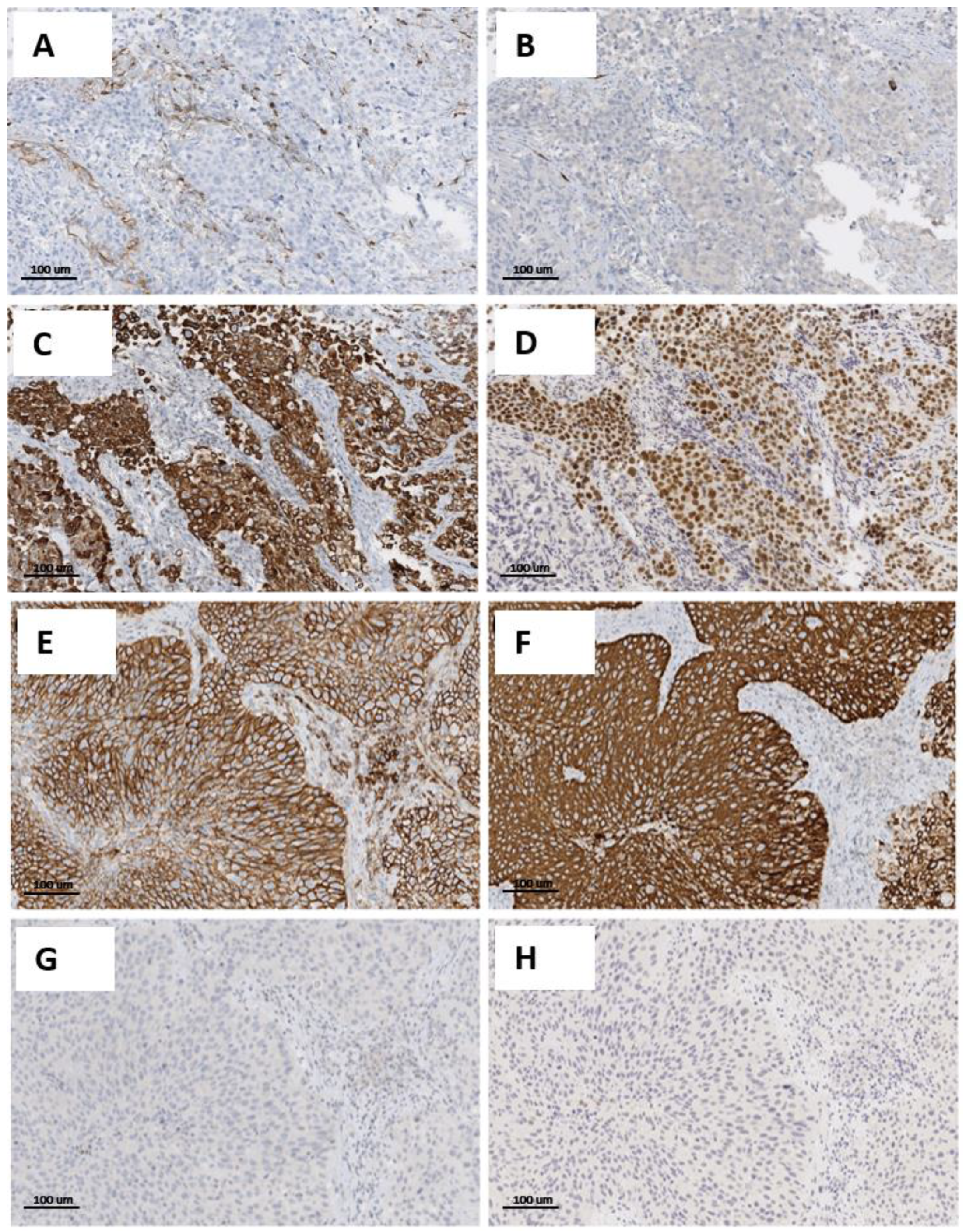
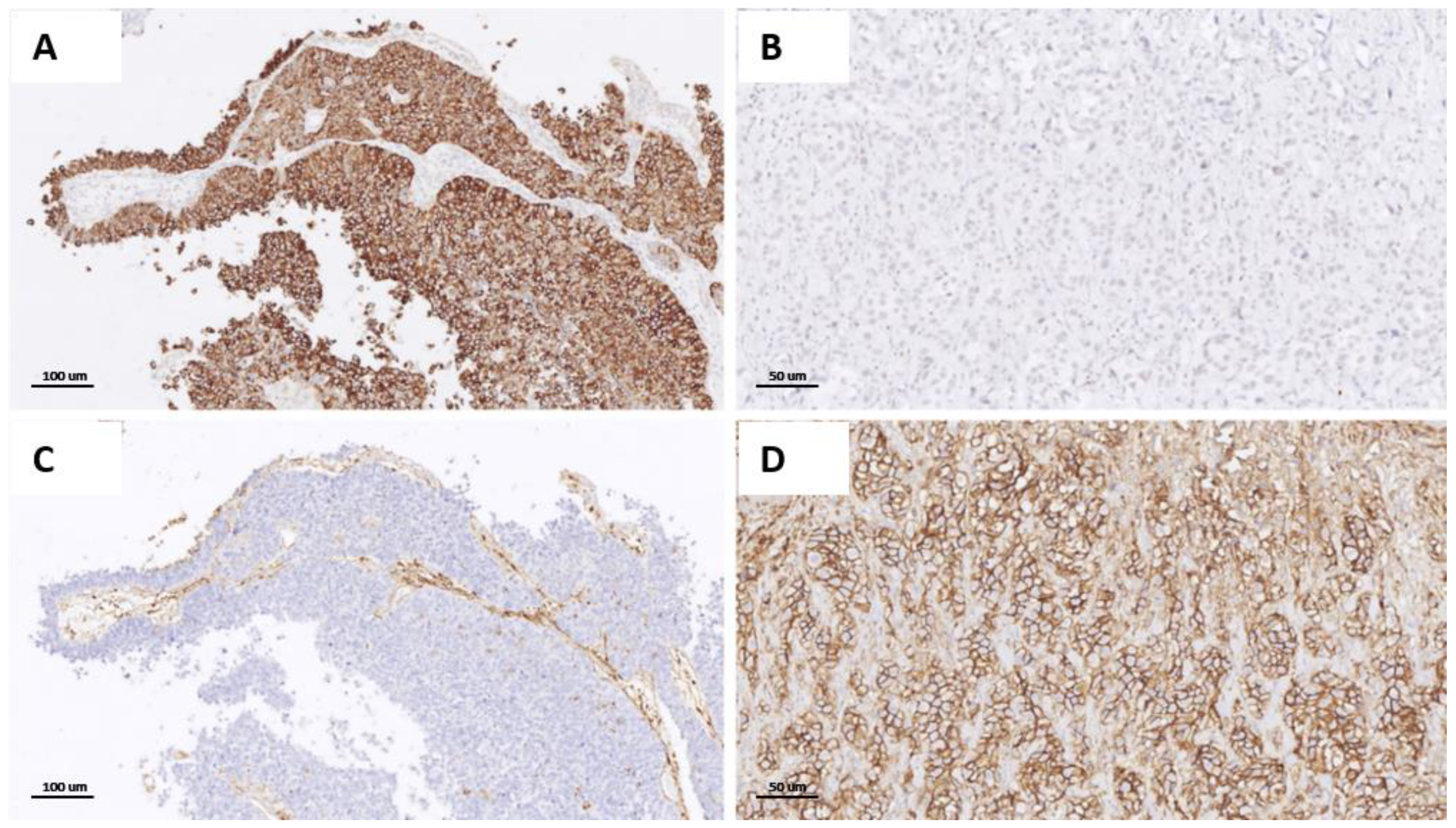
3.2. Immunohistochemical Expression of CD44, CK5/6, CK20, and pPARγ and Identification of the Different Categories
3.3. Phenotypical Switch from Superficial to Muscle-Invasive Component of UC
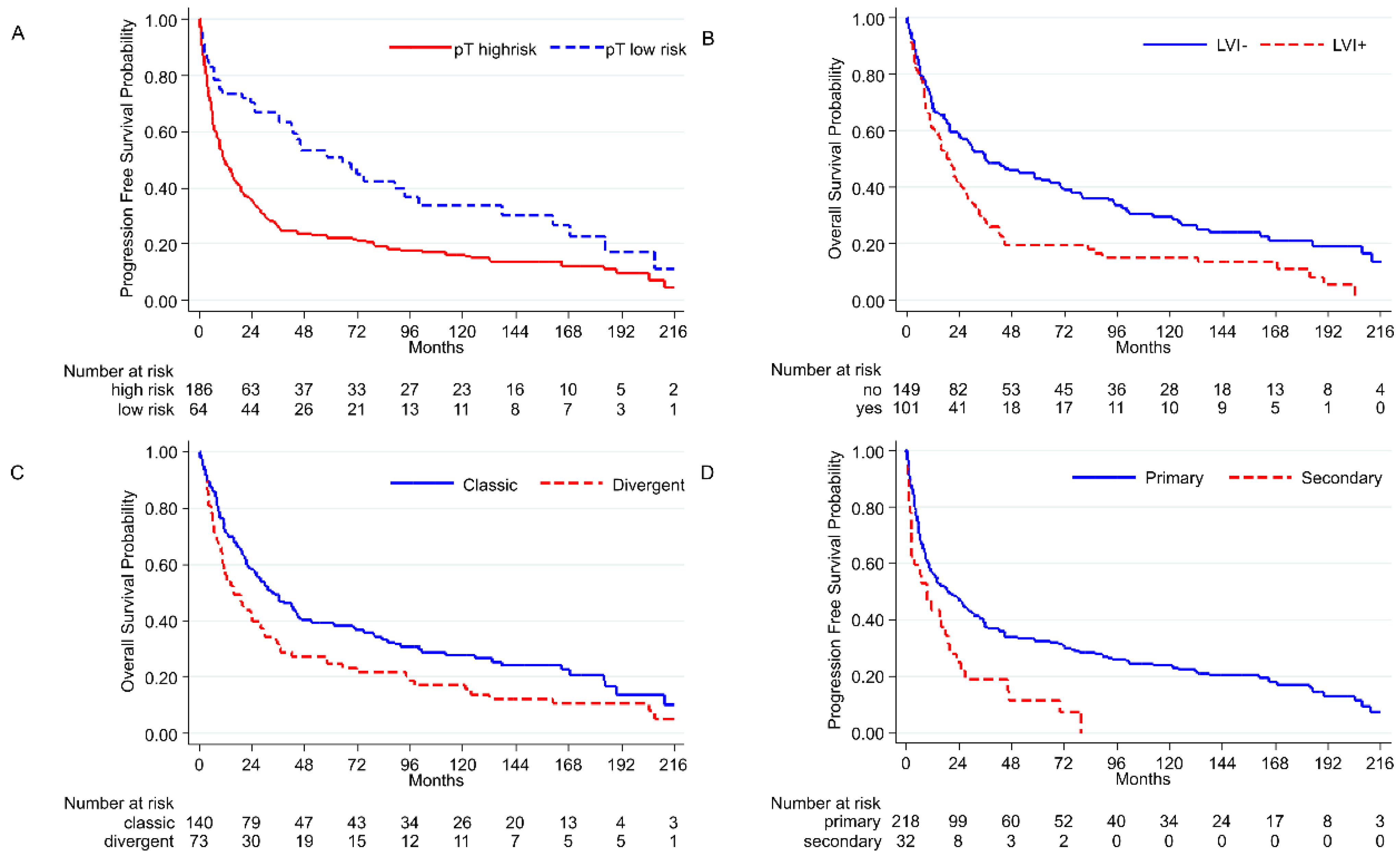
3.4. Histopathological Parameters and Outcome
3.5. Intratumoral Molecular Switch, Phenotypes, and Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Greiman, A.K.; Rosoff, J.S.; Prasad, S.M. Association of Human Development Index with global bladder, kidney, prostate and testis cancer incidence and mortality. Br. J. Urol. 2017, 120, 799–807. [Google Scholar] [CrossRef] [PubMed]
- Dy, G.W.; Gore, J.L.; Forouzanfar, M.H.; Naghavi, M.; Fitzmaurice, C. Global Burden of Urologic Cancers, 1990–2013. Eur. Urol. 2017, 71, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Prasad, S.M.; Decastro, G.J.; Steinberg, G.D. Urothelial carcinoma of the bladder: Definition, treatment and future efforts. Nat. Rev. Urol. 2011, 8, 631–642. [Google Scholar] [CrossRef] [PubMed]
- Dall’Era, M.A.; Cheng, L.; Pan, C.-X. Contemporary management of muscle-invasive bladder cancer. Expert Rev. Anticancer Ther. 2012, 12, 941–950. [Google Scholar] [CrossRef]
- Chang, S.S.; Bochner, B.H.; Chou, R.; Dreicer, R.; Kamat, A.M.; Lerner, S.P.; Lotan, Y.; Meeks, J.J.; Michalski, J.M.; Morgan, T.M.; et al. Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline. J. Urol. 2017, 198, 552–559. [Google Scholar] [CrossRef]
- Rizzo, A.; Mollica, V.; Santoni, M.; Palmiotti, G.; Massari, F. Pathologic Complete Response in Urothelial Carcinoma Patients Receiving Neoadjuvant Immune Checkpoint Inhibitors: A Meta-Analysis. J. Clin. Med. 2022, 11, 1038. [Google Scholar] [CrossRef]
- Tan, W.S.; Lamb, B.; Kelly, J.D. Complications of Radical Cystectomy and Orthotopic Reconstruction. Adv. Urol. 2015, 2015, 323157. [Google Scholar] [CrossRef]
- Burger, M.; Catto, J.W.; Dalbagni, G.; Grossman, H.B.; Herr, H.; Karakiewicz, P.; Kassouf, W.; Kiemeney, L.A.; La Vecchia, C.; Shariat, S.; et al. Epidemiology and risk factors of urothelial bladder cancer. Eur. Urol. 2013, 63, 234–241. [Google Scholar] [CrossRef]
- Mollica, V.; Rizzo, A.; Montironi, R.; Cheng, L.; Giunchi, F.; Schiavina, R.; Santoni, M.; Fiorentino, M.; Lopez-Beltran, A.; Brunocilla, E.; et al. Current Strategies and Novel Therapeutic Approaches for Metastatic Urothelial Carcinoma. Cancers 2020, 12, 1449. [Google Scholar] [CrossRef]
- Knowles, M.A. Molecular genetics of bladder cancer. Br. J. Urol. 1995, 75 (Suppl. S1), 57–66. [Google Scholar] [PubMed]
- Cheng, L.; Zhang, S.; MacLennan, G.T.; Williamson, S.R.; Lopez-Beltran, A.; Montironi, R. Bladder cancer: Translating molecular genetic insights into clinical practice. Hum. Pathol. 2011, 42, 455–481. [Google Scholar] [CrossRef] [PubMed]
- McConkey, D.J.; Choi, W.; Dinney, C.P. Genetic subtypes of invasive bladder cancer. Curr. Opin. Urol. 2015, 25, 449–458. [Google Scholar] [CrossRef]
- Rebola, J.; Aguiar, P.; Blanca, A.; Montironi, R.; Cimadamore, A.; Cheng, L.; Henriques, V.; Lobato-Faria, P.; Lopez-Beltran, A. Predicting outcomes in non-muscle invasive (Ta/T1) bladder cancer: The role of molecular grade based on luminal/basal phenotype. Virchows Arch. 2019, 475, 445–455. [Google Scholar] [CrossRef]
- Choi, W.; Porten, S.; Kim, S.; Willis, D.; Plimack, E.R.; Hoffman-Censits, J.; Roth, B.; Cheng, T.; Tran, M.; Lee, I.-L.; et al. Identification of Distinct Basal and Luminal Subtypes of Muscle-Invasive Bladder Cancer with Different Sensitivities to Frontline Chemotherapy. Cancer Cell 2014, 25, 152–165. [Google Scholar] [CrossRef]
- Kamoun, A.; de Reyniès, A.; Allory, Y.; Sjödahl, G.; Robertson, A.G.; Seiler, R.; Hoadley, K.A.; Groeneveld, C.S.; Al-Ahmadie, H.; Choi, W.; et al. A Consensus Molecular Classification of Muscle-invasive Bladder Cancer. Eur. Urol. 2020, 77, 420–433. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Zhang, Y.; Gao, J.; Lian, X.; Wang, Y. The clinicopathological and prognostic value of CD44 expression in bladder cancer: A study based on meta-analysis and TCGA data. Bioengineered 2020, 11, 572–581. [Google Scholar] [CrossRef] [PubMed]
- Peng, T.; Wang, G.; Cheng, S.; Xiong, Y.; Cao, R.; Qian, K.; Ju, L.; Wang, X.; Xiao, Y. The role and function of PPARγ in bladder cancer. J. Cancer 2020, 11, 3965–3975. [Google Scholar] [CrossRef]
- Wang, C.-C.; Tsai, Y.-C.; Jeng, Y.-M. Biological significance of GATA3, cytokeratin 20, cytokeratin 5/6 and p53 expression in muscle-invasive bladder cancer. PLoS ONE 2019, 14, e0221785. [Google Scholar] [CrossRef]
- Pena, M.D.C.R.; Chaux, A.; Eich, M.-L.; Tregnago, A.C.; Taheri, D.; Borhan, W.; Sharma, R.; Rezaei, M.K.; Netto, G.J. Immunohistochemical assessment of basal and luminal markers in non-muscle invasive urothelial carcinoma of bladder. Virchows Arch. 2019, 475, 349–356. [Google Scholar] [CrossRef]
- Spagnuolo, R.; Corada, M.; Orsenigo, F.; Zanetta, L.; Deuschle, U.; Sandy, P.; Schneider, C.; Drake, C.J.; Breviario, F.; Dejana, E. Gas1 is induced by VE-cadherin and vascular endothelial growth factor and inhibits endothelial cell apoptosis. Blood 2004, 103, 3005–3012. [Google Scholar] [CrossRef] [PubMed]
- Marzouka, N.A.D.; Eriksson, P.; Rovira, C.; Liedberg, F.; Sjödahl, G.; Höglund, M. A validation and extended description of the Lund taxonomy for urothelial carcinoma using the TCGA cohort. Sci. Rep. 2018, 8, 3737. [Google Scholar] [CrossRef]
- Lotan, Y.; Boorjian, S.A.; Zhang, J.; Bivalacqua, T.J.; Porten, S.P.; Wheeler, T.; Lerner, S.P.; Hutchinson, R.; Francis, F.; Davicioni, E.; et al. Molecular Subtyping of Clinically Localized Urothelial Carcinoma Reveals Lower Rates of Pathological Upstaging at Radical Cystectomy Among Luminal Tumors. Eur. Urol. 2019, 76, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Vlachostergios, P.J.; Faltas, B.M. The molecular limitations of biomarker research in bladder cancer. World J. Urol. 2019, 37, 837–848. [Google Scholar] [CrossRef] [PubMed]
- Da Costa, J.B.; Gibb, E.A.; Bivalacqua, T.J.; Liu, Y.; Oo, H.Z.; Miyamoto, D.T.; Alshalalfa, M.; Davicioni, E.; Wright, J.L.; Dall’Era, M.A.; et al. Molecular Characterization of Neuroendocrine-like Bladder Cancer. Clin. Cancer Res. 2019, 25, 3908–3920. [Google Scholar] [CrossRef] [PubMed]
- Han, L.; Gallan, A.J.; Steinberg, G.D.; Sweis, R.F.; Paner, G.P. Morphological correlation of urinary bladder cancer molecular subtypes in radical cystectomies. Hum. Pathol. 2020, 106, 54–61. [Google Scholar] [CrossRef]
- Kollberg, P.; Chebil, G.; Eriksson, P.; Sjödahl, G.; Liedberg, F. Molecular subtypes applied to a population-based modern cystectomy series do not predict cancer-specific survival. Urol. Oncol. Semin. Orig. Investig. 2019, 37, 791–799. [Google Scholar] [CrossRef]
- Desai, S.; Lim, S.D.; Jimenez, R.E.; Chun, T.; Keane, T.E.; McKenney, J.K.; Zavala-Pompa, A.; Cohen, C.; Young, R.H.; Amin, M.B. Relationship of Cytokeratin 20 and CD44 Protein Expression with WHO/ISUP Grade in pTa and pT1 Papillary Urothelial Neoplasia. Mod. Pathol. 2000, 13, 1315–1323. [Google Scholar] [CrossRef]
- Verma, A.; Kapoor, R.; Mittal, R.D. Cluster of Differentiation 44 (CD44) Gene Variants: A Putative Cancer Stem Cell Marker in Risk Prediction of Bladder Cancer in North Indian Population. Indian J. Clin. Biochem. 2017, 32, 74–83. [Google Scholar] [CrossRef]
- Barth, I.; Schneider, U.; Grimm, T.; Karl, A.; Horst, D.; Gaisa, N.T.; Knüchel, R.; Garczyk, S. Progression of urothelial carcinoma in situ of the urinary bladder: A switch from luminal to basal phenotype and related therapeutic implications. Virchows Arch. 2018, 472, 749–758. [Google Scholar] [CrossRef]
- Lee, S.H.; Hu, W.; Matulay, J.T.; Silva, M.V.; Owczarek, T.B.; Kim, K.; Chua, C.W.; Barlow, L.M.J.; Kandoth, C.; Williams, A.B.; et al. Tumor Evolution and Drug Response in Patient-Derived Organoid Models of Bladder. Cancer Cell 2018, 173, 515–528.e17. [Google Scholar] [CrossRef] [PubMed]
- Heide, T.; Maurer, A.; Eipel, M.; Knoll, K.; Geelvink, M.; Veeck, J.; Knuechel, R.; Van Essen, J.; Stoehr, R.; Hartmann, A.; et al. Multiregion human bladder cancer sequencing reveals tumour evolution, bladder cancer phenotypes and implications for targeted therapy. J. Pathol. 2019, 248, 230–242. [Google Scholar] [CrossRef] [PubMed]
- Del Alba, A.G.; Arranz, J.; Puente, J.; Méndez-Vidal, M.J.; Gallardo, E.; Grande, E.; Pérez-Valderrama, B.; González-Billalabeitia, E.; Lázaro-Quintela, M.; Pinto, A.; et al. Recent advances in genitourinary tumors: A review focused on biology and systemic treatment. Crit. Rev. Oncol. 2017, 113, 171–190. [Google Scholar] [CrossRef] [PubMed]
- Warrick, J.I.; Sjödahl, G.; Kaag, M.; Raman, J.D.; Merrill, S.; Shuman, L.; Chen, G.; Walter, V.; DeGraff, D.J. Intratumoral Heterogeneity of Bladder Cancer by Molecular Subtypes and Histologic Variants. Eur. Urol. 2019, 75, 18–22. [Google Scholar] [CrossRef]
- Paciotti, M.; Casale, P.; Colombo, P.; Fasulo, V.; Saita, A.; Lughezzani, G.; Contieri, R.; Buffi, N.M.; Lazzeri, M.; Guazzoni, G.; et al. Long-term Follow-up After En Bloc Transurethral Resection of Non–muscle-invasive Bladder Cancer: Results from a Single-center Experience. Eur. Urol. Open Sci. 2021, 26, 64–71. [Google Scholar] [CrossRef]
- Colombo, R.; Hurle, R.; Moschini, M.; Freschi, M.; Colombo, P.; Colecchia, M.; Ferrari, L.; Lucianò, R.; Conti, G.; Magnani, T.; et al. Feasibility and Clinical Roles of Different Substaging Systems at First and Second Transurethral Resection in Patients with T1 High-Grade Bladder Cancer. Eur. Urol. Focus 2018, 4, 87–93. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Luminal N (%) | Basal N (%) | Mixed N (%) | Neu-like N (%) | |
|---|---|---|---|---|---|
| Patients (%) | 251 (100) | 73 (29.08) | 107 (42.63) | 21 (8.37) | 50 (19.92) |
| Age | |||||
| Median | 70.13 | 69.31 | 70.26 | 65.54 | 73.16 |
| Gender | |||||
| Male | 205 (81.67) | 64 (31.22) | 82 (40.00) | 18 (8.80) | 41 (20.00) |
| Female | 46 (18.32) | 9 (19.56) | 25 (54.35) | 3 (6.52) | 9 (19.56) |
| Smoking | |||||
| Yes | 121 (48.21) | 44 (36.36) | 45 (37.19) | 11 (9.09) | 21 (17.35) |
| Ex | 26 (10.36) | 6 (23.08) | 17 (65.38) | 0 | 3 (11.54) |
| No | 58 (23.11) | 12 (20.70) | 26 (44.83) | 7 (12.07) | 13 (22.41) |
| n.a. | 46 (18.33) | 11 (23.91) | 19 (41.30) | 3 (6.52) | 13 (28.26) |
| Tumor history (TURBT) | |||||
| Primary | 219 (87.25) | 60 (27.40) | 97 (44.29) | 20 (9.13) | 42 (19.18) |
| Secondary | 32 (12.75) | 13 (40.62) | 10 (31.25) | 1 (3.12) | 8 (25.00) |
| CIS (TURBT) | |||||
| Yes | 38 (15.14) | 15 (39.47) | 14 (36.84) | 4 (10.53) | 5 (13.16) |
| No | 213 (84.86) | 58 (27.23) | 93 (42.86) | 17 (7.98) | 45 (21.13) |
| CIS (cystectomy) | |||||
| Yes | 5 (1.99) | 2 (40.00) | 1 (20.00) | 0 | 2 (40.00) |
| No | 246 (98.01) | 71 (28.86) | 106 (43.08) | 21 (8.54) | 48 (19.51) |
| pT (cystectomy) | |||||
| pT0 | 24 (9.56) | 4 (16.67) | 8 (33.33) | 3 (12.5) | 9 (37.5) |
| pTis/Ta | 8 (3.19) | 2 (25.00) | 4 (50.00) | 0 | 2 (25.00) |
| pT1 | 9 (3.58) | 4 (44.44) | 4 (44.44) | 1 (11.11) | 0 |
| pT2 | 29 (11.55) | 11 (37.93) | 11 (37.93) | 3 (10.34) | 4 (13.79) |
| pT3 | 139 (55.38) | 37 (26.62) | 67 (48.20) | 8 (5.75) | 27 (19.42) |
| pT4 | 42 (16.73) | 15 (35.71) | 13 (30.95) | 6 (14.28) | 8 (19.05) |
| pN-M (cystectomy) | |||||
| pN0 | 104 (41.43) | 26 (25.00) | 50 (48.08) | 11 (10.58) | 17 (16.34) |
| pN1-3 | 58 (23.11) | 22 (37.93) | 19 (32.76) | 5 (8.62) | 12 (20.69) |
| pM1 | 5 (1.99) | 2 (40.00) | 2 (40.00) | 0 | 1 (20.00) |
| LVI | |||||
| Yes | 102 (40.64) | 41 (40.20) | 26 (25.49) | 8 (7.84) | 27 (26.48) |
| No | 149 (59.36) | 32 (21.48) | 81 (54.36) | 13 (8.72) | 23 (15.43) |
| Necrosis | |||||
| Yes | 96 (38.25) | 24 (25.00) | 49 (51.04) | 6 (6.25) | 17 (17.71) |
| No | 155 (61.75) | 49 (31.61) | 58 (37.42) | 15 (9.68) | 33 (21.29) |
| CT | |||||
| Yes | 63 (25.1) | 18 (28.58) | 23 (36.51) | 9 (14.28) | 13 (20.63) |
| No | 188 (74.9) | 55 (29.25) | 84 (44.68) | 12 (6.38) | 37 (19.68) |
| Histological Category in pT2 UC at TUR and Markers | ||||||||
|---|---|---|---|---|---|---|---|---|
| Architecture | Histological Subtype/Variant | |||||||
| Phenotype | Papillary 139 (%) | Not Papillary 112 (%) | Classic 157 | Divergent 71 | Sarcomatoid 5 | Nested 5 | Micropap/Plasmacytoid 2/3 | Neuroend 8 |
| Basal Markers+ | ||||||||
| CD44 | 60 (43.16) | 51 (45.53) | 55 (35.03) | 49 (69.01) | 4 (80) | 2 (40) | 0/0 | 1 (12.5) |
| CK 5/6 | 58 (41.73) | 42 (37.5) | 45 (28.67) | 50 (69.44) | 2 (40) | 3 (60) | 0/0 | 0 |
| Luminal Markers+ | ||||||||
| CK20 | 26 (18.70) | 29 (25.89) | 43 (27.39) | 9 (12.5) | 0 | 2 (40) | 1 (50)/0 | 0 |
| pPARg | 27 (19.42) | 35 (31.25) | 43 (27.39) | 13 (18.05) | 0 | 3 (60) | 2 (100)/0 | 1 (12.5) |
| Basal type 107 pts | 63 (45.32) | 44 (39.28) | 51 (32.48) | 49 (69.01) | 5 (100) | 2 (40) | 0/0 | 0 |
| Luminal type 73 pts | 36 (25.90) | 37 (33.03) | 59 (37.58) | 11 (15.28) | 0 | 1 (20) | 2 (100)/0 | 0 |
| Mixed type 21 pts | 12 (8.63) | 9 (8.03) | 15 (9.55) | 4 (5.55) | 0 | 1 (20) | 0/0 | 1 (12.5) |
| Neu-like type 50 pts | 28 (20.14) | 22 (19.64) | 32 (20.38) | 7 (9.86) | 0 | 1 (20) | 0/3 (100) | 7 (87.5) |
| Switched cases | ||||||||
| Yes 96 pts | 64 (46.04) | 32 (28.57) | 63 (40.13) | 23 (32.4) | 3 (60) | 2 (40) | 0/3 (100) | 2 (25) |
| No 155 pts | 75 (53.96) | 80 (71.43) | 94 (59.87) | 48 (67.6) | 2 (40) | 3 (60) | 2 (100)/0 | 6 (75) |
| Pts 251 (100) | 139 (100) | 112 (100) | 157 (100) | 71 (100) | 5 (100) | 5 (100) | 5 (100) | 8 (100) |
| Phenotypes | Marker Combinations | Tot (%) | |||
|---|---|---|---|---|---|
| CD44 | CK5/6 | CK20 | pPARγ | ||
| Basal (107) | + | + | - | - | 74 (69.16) |
| + | + | - | + | 10 (9.3) | |
| + | + | + | - | 2 (1.87) | |
| + | - | - | - | 13 (12.15) | |
| - | + | - | - | 8 (7.5) | |
| Luminal (73) | - | - | + | + | 30 (41.1) |
| + | - | + | + | 4 (5.5) | |
| - | + | + | + | 3 (4.1) | |
| - | - | - | + | 15 (20.5) | |
| - | - | + | - | 21 (28.8) | |
| Mixed (21) | + | + | + | + | 4 (19.05) |
| + | - | - | + | 4 (19,05) | |
| - | + | + | - | 0 (0) | |
| + | - | + | - | 5 (23.8) | |
| - | + | - | + | 8 (38.1) | |
| Neu-like (50) | - | - | - | - | 50 (100) |
| Cases Switch | n | p (t Test) |
|---|---|---|
| Yes No | 96 155 | - |
| Luminal vs. basal Yes No | 53 vs. 8 68 vs. 63 | <0.00001 |
| Luminal vs. mixed Yes No | 53 vs. 30 68 vs. 9 | 0.000318 |
| Luminal vs. neu Yes No | 53 vs. 5 68 vs. 15 | ns |
| Basal vs. mixed Yes No | 8 vs. 30 63 vs. 9 | <0.00001 |
| Basal vs. neu Yes No | 8 vs. 5 63 vs. 15 | ns |
| Mixed vs. neu Yes No | 30 vs. 5 9 vs. 15 | 0.000121 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Carlo, C.; Valeri, M.; Rudini, N.; Zucali, P.A.; Cieri, M.; Elefante, G.M.; D’antonio, F.; Hurle, R.; Giordano, L.; Bressan, A.; et al. Intratumoral Switch of Molecular Phenotype and Overall Survival in Muscle Invasive Bladder Cancer. Cancers 2022, 14, 3256. https://doi.org/10.3390/cancers14133256
De Carlo C, Valeri M, Rudini N, Zucali PA, Cieri M, Elefante GM, D’antonio F, Hurle R, Giordano L, Bressan A, et al. Intratumoral Switch of Molecular Phenotype and Overall Survival in Muscle Invasive Bladder Cancer. Cancers. 2022; 14(13):3256. https://doi.org/10.3390/cancers14133256
Chicago/Turabian StyleDe Carlo, Camilla, Marina Valeri, Noemi Rudini, Paolo Andrea Zucali, Miriam Cieri, Grazia Maria Elefante, Federica D’antonio, Rodolfo Hurle, Laura Giordano, Alessandra Bressan, and et al. 2022. "Intratumoral Switch of Molecular Phenotype and Overall Survival in Muscle Invasive Bladder Cancer" Cancers 14, no. 13: 3256. https://doi.org/10.3390/cancers14133256
APA StyleDe Carlo, C., Valeri, M., Rudini, N., Zucali, P. A., Cieri, M., Elefante, G. M., D’antonio, F., Hurle, R., Giordano, L., Bressan, A., Lazzeri, M., Perrino, M., Guazzoni, G., Terracciano, L. M., & Colombo, P. (2022). Intratumoral Switch of Molecular Phenotype and Overall Survival in Muscle Invasive Bladder Cancer. Cancers, 14(13), 3256. https://doi.org/10.3390/cancers14133256