
No Impact of Seasonality of Diagnoses on Baseline Tumor Immune Infiltration, Response to Treatment, and Prognosis in BC Patients Treated with NAC


 , , ,
, , ,  ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Tumors
2.2. Tumor Samples and BC Subtype
2.3. Tumor-Infiltrating Lymphocytes
2.4. Response to Treatment
2.5. Date and Season of BC Diagnosis
2.6. Survival Endpoints
2.7. Statistical Analysis
3. Results
3.1. Study Population and Tumors Characteristics
3.2. Seasonality of BC Diagnosis
3.3. Response to Treatment and Post-NAC TIL Levels
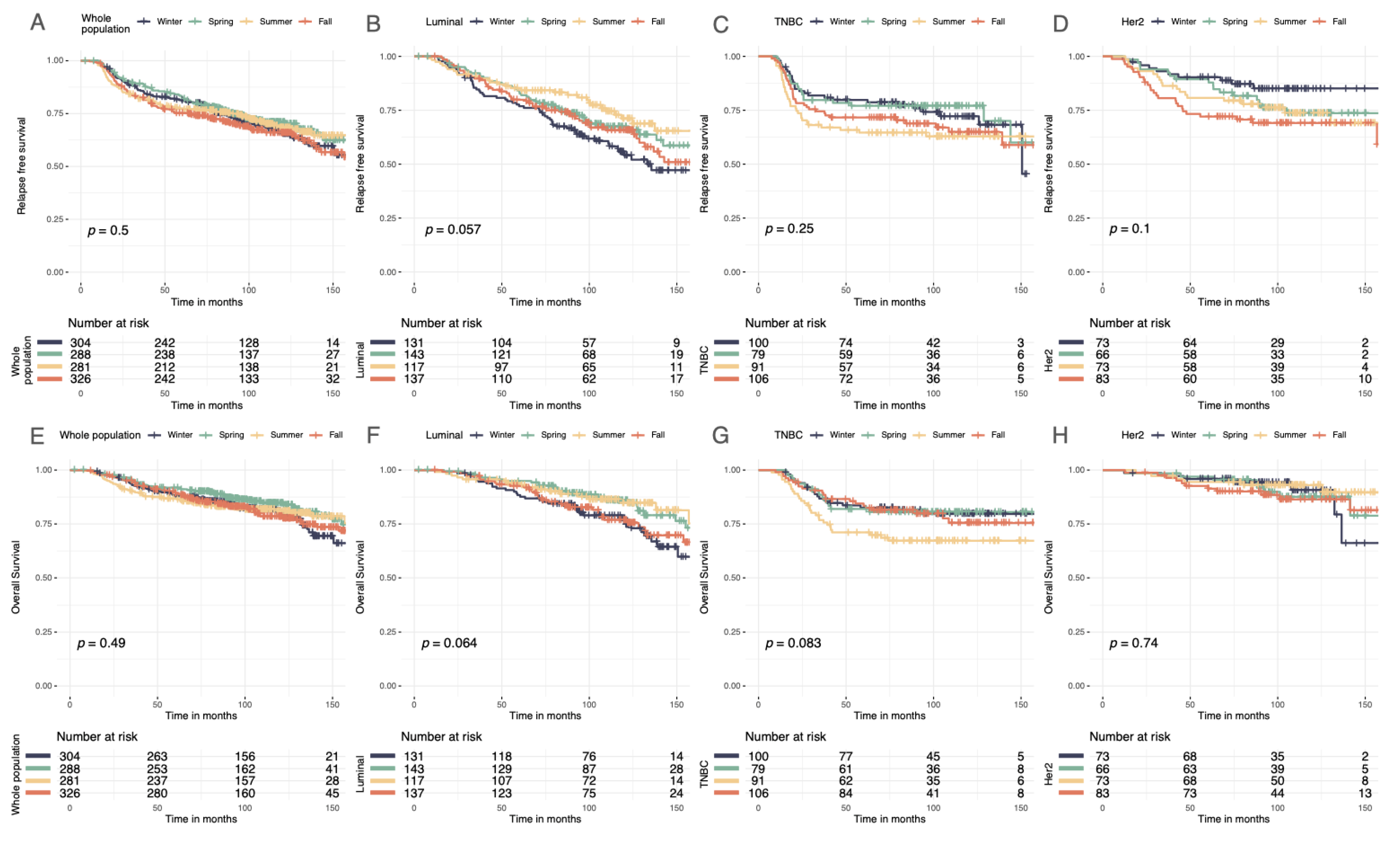
3.4. Survival Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Key, T.J.; Verkasalo, P.K.; Banks, E. Epidemiology of Breast Cancer. Lancet Oncol. 2001, 2, 133–140. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Rastogi, P.; Anderson, S.J.; Bear, H.D.; Geyer, C.E.; Kahlenberg, M.S.; Robidoux, A.; Margolese, R.G.; Hoehn, J.L.; Vogel, V.G.; Dakhil, S.R.; et al. Preoperative Chemotherapy: Updates of National Surgical Adjuvant Breast and Bowel Project Protocols B-18 and B-27. J. Clin. Oncol. 2008, 26, 778–785. [Google Scholar] [CrossRef]
- Reyal, F.; Hamy, A.S.; Piccart, M.J. Neoadjuvant Treatment: The Future of Patients with Breast Cancer. ESMO Open 2018, 3, e000371. [Google Scholar] [CrossRef] [PubMed]
- Luangdilok, S.; Samarnthai, N.; Korphaisarn, K. Association between Pathological Complete Response and Outcome Following Neoadjuvant Chemotherapy in Locally Advanced Breast Cancer Patients. J. Breast Cancer 2014, 17, 376–385. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Balko, J.M.; Giltnane, J.M.; Wang, K.; Schwarz, L.J.; Young, C.D.; Cook, R.S.; Owens, P.; Sanders, M.E.; Kuba, M.G.; Sánchez, V.; et al. Molecular Profiling of the Residual Disease of Triple-Negative Breast Cancers after Neoadjuvant Chemotherapy Identifies Actionable Therapeutic Targets. Cancer Discov. 2014, 4, 232–245. [Google Scholar] [CrossRef] [PubMed]
- Cortazar, P.; Zhang, L.; Untch, M.; Mehta, K.; Costantino, J.P.; Wolmark, N.; Bonnefoi, H.; Cameron, D.; Gianni, L.; Valagussa, P.; et al. Pathological Complete Response and Long-Term Clinical Benefit in Breast Cancer: The CTNeoBC Pooled Analysis. Lancet 2014, 384, 164–172. [Google Scholar] [CrossRef]
- Dieci, M.V.; Radosevic-Robin, N.; Fineberg, S.; van den Eynden, G.; Ternes, N.; Penault-Llorca, F.; Pruneri, G.; D’Alfonso, T.M.; Demaria, S.; Castaneda, C.; et al. Update on Tumor-Infiltrating Lymphocytes (TILs) in Breast Cancer, Including Recommendations to Assess TILs in Residual Disease after Neoadjuvant Therapy and in Carcinoma in Situ: A Report of the International Immuno-Oncology Biomarker Working Group on Breast Cancer. Semin. Cancer Biol. 2018, 52, 16–25. [Google Scholar] [CrossRef]
- El Bairi, K.; Haynes, H.R.; Blackley, E.; Fineberg, S.; Shear, J.; Turner, S.; de Freitas, J.R.; Sur, D.; Amendola, L.C.; Gharib, M.; et al. The Tale of TILs in Breast Cancer: A Report from The International Immuno-Oncology Biomarker Working Group. npj Breast Cancer 2021, 7, 150. [Google Scholar] [CrossRef]
- Denkert, C.; Loibl, S.; Noske, A.; Roller, M.; Müller, B.M.; Komor, M.; Budczies, J.; Darb-Esfahani, S.; Kronenwett, R.; Hanusch, C.; et al. Tumor-Associated Lymphocytes as an Independent Predictor of Response to Neoadjuvant Chemotherapy in Breast Cancer. J. Clin. Oncol. 2010, 28, 105–113. [Google Scholar] [CrossRef]
- Salgado, R.; Denkert, C.; Demaria, S.; Sirtaine, N.; Klauschen, F.; Pruneri, G.; Wienert, S.; Van den Eynden, G.; Baehner, F.L.; Penault-Llorca, F.; et al. The Evaluation of Tumor-Infiltrating Lymphocytes (TILs) in Breast Cancer: Recommendations by an International TILs Working Group 2014. Ann. Oncol. 2015, 26, 259–271. [Google Scholar] [CrossRef] [PubMed]
- Denkert, C.; von Minckwitz, G.; Brase, J.C.; Sinn, B.V.; Gade, S.; Kronenwett, R.; Pfitzner, B.M.; Salat, C.; Loi, S.; Schmitt, W.D.; et al. Tumor-Infiltrating Lymphocytes and Response to Neoadjuvant Chemotherapy With or Without Carboplatin in Human Epidermal Growth Factor Receptor 2–Positive and Triple-Negative Primary Breast Cancers. JCO 2015, 33, 983–991. [Google Scholar] [CrossRef] [PubMed]
- Loi, S.; Drubay, D.; Adams, S.; Pruneri, G.; Francis, P.A.; Lacroix-Triki, M.; Joensuu, H.; Dieci, M.V.; Badve, S.; Demaria, S.; et al. Tumor-Infiltrating Lymphocytes and Prognosis: A Pooled Individual Patient Analysis of Early-Stage Triple-Negative Breast Cancers. JCO 2019, 37, 559–569. [Google Scholar] [CrossRef] [PubMed]
- Denkert, C.; von Minckwitz, G.; Darb-Esfahani, S.; Lederer, B.; Heppner, B.I.; Weber, K.E.; Budczies, J.; Huober, J.; Klauschen, F.; Furlanetto, J.; et al. Tumour-Infiltrating Lymphocytes and Prognosis in Different Subtypes of Breast Cancer: A Pooled Analysis of 3771 Patients Treated with Neoadjuvant Therapy. Lancet Oncol. 2018, 19, 40–50. [Google Scholar] [CrossRef]
- Hamy, A.-S.; Bonsang-Kitzis, H.; Croze, D.D.; Laas, E.; Darrigues, L.; Topciu, L.; Menet, E.; Vincent-Salomon, A.; Lerebours, F.; Pierga, J.-Y.; et al. Interaction between Molecular Subtypes, Stromal Immune Infiltration before and after Treatment in Breast Cancer Patients Treated with Neoadjuvant Chemotherapy. Clin. Cancer Res. 2019, 25, 6731–6741. [Google Scholar] [CrossRef]
- Nixon, A.J.; Neuberg, D.; Hayes, D.F.; Gelman, R.; Connolly, J.L.; Schnitt, S.; Abner, A.; Recht, A.; Vicini, F.; Harris, J.R. Relationship of Patient Age to Pathologic Features of the Tumor and Prognosis for Patients with Stage I or II Breast Cancer. J. Clin. Oncol. 1994, 12, 888–894. [Google Scholar] [CrossRef]
- de la Rochefordière, A.; Campana, F.; Fenton, J.; Vilcoq, J.R.; Fourquet, A.; Asselain, B.; Scholl, S.M.; Pouillart, P.; Durand, J.-C.; Magdelenat, H. Age as Prognostic Factor in Premenopausal Breast Carcinoma. Lancet 1993, 341, 1039–1043. [Google Scholar] [CrossRef]
- Sun, L.; Zhu, Y.; Qian, Q.; Tang, L. Body Mass Index and Prognosis of Breast Cancer. Medicine 2018, 907, e11220. [Google Scholar] [CrossRef]
- Marret, H.; Perrotin, F.; Bougnoux, P.; Descamps, P.; Hubert, B.; Lefranc, T.; Floch, O.L.; Lansac, J.; Body, G. Low Body Mass Index Is an Independent Predictive Factor of Local Recurrence after Conservative Treatment for Breast Cancer. Breast Cancer Res. Treat 2001, 66, 17–23. [Google Scholar] [CrossRef]
- Karatas, F. Obesity Is an Independent Prognostic Factor of Decreased Pathological Complete Response to Neoadjuvant Chemotherapy in Breast Cancer Patients. Breast 2017, 32, 237–244. [Google Scholar] [CrossRef]
- Collaborative Group on Hormonal Factors in Breast Cancer. Alcohol, Tobacco and Breast Cancer—Collaborative Reanalysis of Individual Data from 53 Epidemiological Studies, Including 58,515 Women with Breast Cancer and 95,067 Women without the Disease. Br. J. Cancer 2002, 87, 1234–1245. [Google Scholar] [CrossRef] [PubMed]
- Passarelli, M.N.; Newcomb, P.A.; Hampton, J.M.; Trentham-Dietz, A.; Titus, L.J.; Egan, K.M.; Baron, J.A.; Willett, W.C. Cigarette Smoking Before and After Breast Cancer Diagnosis: Mortality From Breast Cancer and Smoking-Related Diseases. J. Clin. Oncol. 2016, 34, 1315. [Google Scholar] [CrossRef] [PubMed]
- Pushpakom, S.; Iorio, F.; Eyers, P.A.; Escott, K.J.; Hopper, S.; Wells, A.; Doig, A.; Guilliams, T.; Latimer, J.; McNamee, C.; et al. Drug Repurposing: Progress, Challenges and Recommendations. Nat. Rev. Drug Discov. 2019, 18, 41–58. [Google Scholar] [CrossRef] [PubMed]
- Hamy, A.-S.; Derosa, L.; Valdelièvre, C.; Yonekura, S.; Opolon, P.; Priour, M.; Guerin, J.; Pierga, J.-Y.; Asselain, B.; De Croze, D.; et al. Comedications Influence Immune Infiltration and Pathological Response to Neoadjuvant Chemotherapy in Breast Cancer. OncoImmunology 2019, 9, 1677427. [Google Scholar] [CrossRef] [PubMed]
- Lofterød, T.; Frydenberg, H.; Flote, V.; Eggen, A.E.; McTiernan, A.; Mortensen, E.S.; Akslen, L.A.; Reitan, J.B.; Wilsgaard, T.; Thune, I. Exploring the Effects of Lifestyle on Breast Cancer Risk, Age at Diagnosis, and Survival: The EBBA-Life Study. Breast Cancer Res. Treat. 2020, 182, 215–227. [Google Scholar] [CrossRef]
- Verkasalo, P.K.; Lillberg, K.; Stevens, R.G.; Hublin, C.; Partinen, M.; Koskenvuo, M.; Kaprio, J. Sleep Duration and Breast Cancer: A Prospective Cohort Study. Cancer Res. 2005, 65, 9595–9600. [Google Scholar] [CrossRef]
- White, A.J.; Bradshaw, P.T.; Hamra, G.B. Air Pollution and Breast Cancer: A Review. Curr. Epidemiol. Rep. 2018, 5, 92–100. [Google Scholar] [CrossRef]
- Hiller, T.W.R.; O’Sullivan, D.E.; Brenner, D.R.; Peters, C.E.; King, W.D. Solar Ultraviolet Radiation and Breast Cancer Risk: A Systematic Review and Meta-Analysis. Environ. Health Perspect. 2020, 128, 016002. [Google Scholar] [CrossRef]
- Lim, H.-S.; Roychoudhuri, R.; Peto, J.; Schwartz, G.; Baade, P.; Møller, H. Cancer Survival Is Dependent on Season of Diagnosis and Sunlight Exposure. Int. J. Cancer 2006, 119, 1530–1536. [Google Scholar] [CrossRef]
- Wu, S.; Powers, S.; Zhu, W.; Hannun, Y.A. Substantial Contribution of Extrinsic Risk Factors to Cancer Development. Nature 2016, 529, 43–47. [Google Scholar] [CrossRef]
- Song, M.; Giovannucci, E. Preventable Incidence and Mortality of Carcinoma Associated With Lifestyle Factors Among White Adults in the United States. JAMA Oncol. 2016, 2, 1154. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Zhu, W.; Thompson, P.; Hannun, Y.A. Evaluating Intrinsic and Non-Intrinsic Cancer Risk Factors. Nat. Commun. 2018, 9, 3490. [Google Scholar] [CrossRef] [PubMed]
- Gray, J.; Evans, N.; Taylor, B.; Rn, J.R.; Walker, M. State of the Evidence: The Connection Between Breast Cancer and the Environment. Int. J. Occup. Environ. Health 2009, 15, 36. [Google Scholar] [CrossRef]
- Gray, J.M.; Rasanayagam, S.; Engel, C.; Rizzo, J. State of the Evidence 2017: An Update on the Connection between Breast Cancer and the Environment. Environ. Health 2017, 16, 94. [Google Scholar] [CrossRef]
- Stewart, S.; Keates, A.K.; Redfern, A.; McMurray, J.J.V. Seasonal Variations in Cardiovascular Disease. Nat. Rev. Cardiol. 2017, 14, 654–664. [Google Scholar] [CrossRef]
- Yang, J.; Zhou, M.; Ou, C.-Q.; Yin, P.; Li, M.; Tong, S.; Gasparrini, A.; Liu, X.; Li, J.; Cao, L.; et al. Seasonal Variations of Temperature-Related Mortality Burden from Cardiovascular Disease and Myocardial Infarction in China. Environ. Pollut. 2017, 224, 400–406. [Google Scholar] [CrossRef]
- Davis, R.E.; Rossier, C.E.; Enfield, K.B. The Impact of Weather on Influenza and Pneumonia Mortality in New York City, 1975–2002: A Retrospective Study. PLoS ONE 2012, 7, e34091. [Google Scholar] [CrossRef]
- DuBose, D.A.; Agnew, J.W. Seasonal Effects on Human Physiological Adaptation Factors, Thermotolerance and Plasma Fibronectin. Aviat. Space Environ. Med. 1992, 63, 982–985. [Google Scholar]
- van der Toorn, J.E.; Cepeda, M.; Kiefte-de Jong, J.C.; Franco, O.H.; Voortman, T.; Schoufour, J.D. Seasonal Variation of Diet Quality in a Large Middle-Aged and Elderly Dutch Population-Based Cohort. Eur. J. Nutr. 2020, 59, 493–504. [Google Scholar] [CrossRef]
- Chiriboga, D.E.; Ma, Y.; Li, W.; Stanek, E.J., III; Hébert, J.R.; Merriam, P.A.; Rawson, E.S.; Ockene, I.S. Seasonal and Sex Variation of High-Sensitivity C-Reactive Protein in Healthy Adults: A Longitudinal Study. Clin. Chem. 2009, 55, 313–321. [Google Scholar] [CrossRef]
- Bjørnerem, Å.; Straume, B.; Øian, P.; Berntsen, G.K.R. Seasonal Variation of Estradiol, Follicle Stimulating Hormone, and Dehydroepiandrosterone Sulfate in Women and Men. J. Clin. Endocrinol. Metab. 2006, 91, 3798–3802. [Google Scholar] [CrossRef] [PubMed]
- Wehr, T.A. Effect of Seasonal Changes in Daylength on Human Neuroendocrine Function. Horm. Res. Paediatr. 1998, 49, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Shahar, D.R.; Yerushalmi, N.; Lubin, F.; Froom, P.; Shahar, A.; Kristal-Boneh, E. Seasonal Variations in Dietary Intake Affect the Consistency of Dietary Assessment. Eur. J. Epidemiol. 2001, 17, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Rossato, S.L.; Olinto, M.T.A.; Henn, R.L.; Moreira, L.B.; Camey, S.A.; Anjos, L.A.; Wahrlich, V.; Waissmann, W.; Fuchs, F.D.; Fuchs, S.C. Seasonal Variation in Food Intake and the Interaction Effects of Sex and Age among Adults in Southern Brazil. Eur. J. Clin. Nutr. 2015, 69, 1015–1022. [Google Scholar] [CrossRef]
- Locke, E.; Coronado, G.D.; Thompson, B.; Kuniyuki, A. Seasonal Variation in Fruit and Vegetable Consumption in a Rural Agricultural Community. J. Am. Diet. Assoc. 2009, 109, 45–51. [Google Scholar] [CrossRef]
- Yoon, J.Y.; Kwak, M.S.; Kim, H.I.; Cha, J.M. Seasonal Variations in the Diagnosis of the Top 10 Cancers in Korea: A Nationwide Population-based Study Using a Common Data Model. J. Gastroenterol. Hepatol. 2021, 36, 3371–3380. [Google Scholar] [CrossRef]
- Lambe, M.; Blomqvist, P.; Bellocco, R. Seasonal Variation in the Diagnosis of Cancer: A Study Based on National Cancer Registration in Sweden. Br. J. Cancer 2003, 88, 1358–1360. [Google Scholar] [CrossRef]
- Gao, F.; Machin, D.; Khoo, K.-S.; Ng, E.-H. Seasonal Variation in Breast Cancer Diagnosis in Singapore. Br. J. Cancer 2001, 84, 1185–1187. [Google Scholar] [CrossRef]
- Holdaway, I.M.; Mason, B.H.; Marshall, R.J.; Neave, L.M.; Kay, R.G. Seasonal Change in the Concentration of Progesterone Receptor in Breast Cancer. Cancer Res. 1990, 50, 5883–5886. [Google Scholar]
- Joensuu, H.; Toikkanen, S. Association between the Month of Diagnosis and Prognosis in Breast Carcinoma. Br. J. Cancer 1991, 64, 753–756. [Google Scholar] [CrossRef][Green Version]
- Paradiso, A.; Serio, G.; Fanelli, M.; Mangia, A.; Cellamare, G.; Schittulli, F. Predictability of Monthly and Yearly Rhythms of Breast Cancer Features. Breast Cancer Res. Treat. 2001, 67, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Loukas, M. Seasonality Pattern of Breast, Colorectal, and Prostate Cancer Is Dependent on Latitude. Med. Sci. Monit. 2014, 20, 818–824. [Google Scholar] [CrossRef] [PubMed]
- Kuzmickiene, I.; Atkocius, V.; Aleknavicius, E.; Ostapenko, V. Impact of Season of Diagnosis on Mortality among Breast Cancer Survivors. J. Can. Res. Ther. 2018, 14, 1091. [Google Scholar] [CrossRef] [PubMed]
- Mason, B.; Holdaway, I.; Stewart, A.; Neave, L.; Kay, R. Season of Initial Discovery of Tumour as an Independent Variable Predicting Survival in Breast Cancer. Br. J. Cancer 1990, 61, 137–141. [Google Scholar] [CrossRef]
- Balaton, A.J.; Doussal, V.L.; Arnould, L.; Barlier, C.; Bellocq, J.P.; Ettore, F.; Fiche, M.; Jacquemier, J.; Grogan, G.M.; Mathieu, M.C.; et al. Recommandations pour l’évaluation Immunohistochimique des Récepteurs Hormonaux sur Coupes en Paraffine dans les Carcinomes Mammaires Mise à jour 1999; Elsevier: Amsterdam, The Netherlands, 1999. [Google Scholar]
- Wolff, A.C.; Hammond, M.E.H.; Allison, K.H.; Harvey, B.E.; Mangu, P.B.; Bartlett, J.M.S.; Bilous, M.; Ellis, I.O.; Fitzgibbons, P.; Hanna, W.; et al. Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update. Arch. Pathol. Lab. Med. 2018, 142, 1364–1382. [Google Scholar] [CrossRef]
- Von Minckwitz, G.; Untch, M.; Blohmer, J.U.; Costa, S.D.; Eidtmann, H.; Fasching, P.A.; Gerber, B.; Eiermann, W.; Hilfrich, J.; Huober, J.; et al. Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J. Clin. Oncol. 2012, 30, 1796–1804. [Google Scholar] [CrossRef]
- Oh, E.-Y.; Ansell, C.; Nawaz, H.; Yang, C.-H.; Wood, P.A.; Hrushesky, W.J.M. Global Breast Cancer Seasonality. Breast Cancer Res. Treat. 2010, 123, 233–243. [Google Scholar] [CrossRef]
- Ross, J.A.; Severson, R.K.; Davis, S.; Stanford, J.L.; Potter, J.D. Seasonal Trends in the Self-Detection of Breast Cancer: Indications from the Cancer and Steroid Hormone (CASH) Study. Breast Cancer Res. Treat. 1997, 42, 187–192. [Google Scholar] [CrossRef]
- Welch, H.G.; Prorok, P.C.; O’Malley, A.J.; Kramer, B.S. Breast-Cancer Tumor Size, Overdiagnosis, and Mammography Screening Effectiveness. N. Engl. J. Med. 2016, 375, 1438–1447. [Google Scholar] [CrossRef]
- Wyse, C.; O’Malley, G.; Coogan, A.N.; McConkey, S.; Smith, D.J. Seasonal and Daytime Variation in Multiple Immune Parameters in Humans: Evidence from 329,261 Participants of the UK Biobank Cohort. iScience 2021, 24, 102255. [Google Scholar] [CrossRef]
- Roychoudhuri, R.; Robinson, D.; Coupland, V.; Holmberg, L.; Møller, H. Season of Cancer Diagnosis Exerts Distinct Effects upon Short- and Long-Term Survival. Int. J. Cancer 2009, 124, 2436–2441. [Google Scholar] [CrossRef] [PubMed]
- Porojnicu, A.C.; Lagunova, Z.; Robsahm, T.E.; Berg, J.P.; Dahlback, A.; Moan, J. Changes in Risk of Death from Breast Cancer with Season and Latitude. Breast Cancer Res. Treat. 2007, 102, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Teilum, D.; Bjerre, K.D.; Tjønneland, A.M.; Kroman, N. Breast Cancer Survival and Season of Surgery: An Ecological Open Cohort Study. BMJ Open 2012, 2, e000358. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kwon, H.W.; Lee, J.W.; Kim, H.J.; Koh, B.S.; Yu, J.H.; Lee, J.W.; Son, B.H.; Ahn, S.H. Impact of Seasonal and Geographical Differences on Breast Cancer Survival. Korean J. Clin. Oncol. 2013, 9, 168–174. [Google Scholar] [CrossRef]
- Holmberg, L.; Adolfsson, J.; Mucci, L.; Garmo, H.; Adami, H.O.; Möller, H.; Johansson, J.-E.; Stampfer, M. Season of Diagnosis and Prognosis in Breast and Prostate Cancer. Cancer Causes Control 2009, 20, 663–670. [Google Scholar] [CrossRef] [PubMed]
- Terranova-Barberio, M.; Pawlowska, N.; Dhawan, M.; Moasser, M.; Chien, A.J.; Melisko, M.E.; Rugo, H.; Rahimi, R.; Deal, T.; Daud, A.; et al. Exhausted T Cell Signature Predicts Immunotherapy Response in ER-Positive Breast Cancer. Nat. Commun. 2020, 11, 3584. [Google Scholar] [CrossRef]
- Daud, A.I.; Loo, K.; Pauli, M.L.; Sanchez-Rodriguez, R.; Sandoval, P.M.; Taravati, K.; Tsai, K.; Nosrati, A.; Nardo, L.; Alvarado, M.D.; et al. Tumor Immune Profiling Predicts Response to Anti–PD-1 Therapy in Human Melanoma. J. Clin. Investig. 2016, 126, 3447–3452. [Google Scholar] [CrossRef]
- Miyashita, M.; Sasano, H.; Tamaki, K.; Hirakawa, H.; Takahashi, Y.; Nakagawa, S.; Watanabe, G.; Tada, H.; Suzuki, A.; Ohuchi, N.; et al. Prognostic Significance of Tumor-Infiltrating CD8+ and FOXP3+ Lymphocytes in Residual Tumors and Alterations in These Parameters after Neoadjuvant Chemotherapy in Triple-Negative Breast Cancer: A Retrospective Multicenter Study. Breast Cancer Res. 2015, 17, 124. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Class | All | Winter | Spring | Summer | Fall | p | test | |
|---|---|---|---|---|---|---|---|---|
| n | 1199 | 304 | 288 | 281 | 326 | |||
| Age at BC diagnosis | 48.20 [40.90, 55.50] | 46.95 [39.90, 53.92] | 47.75 [41.80, 54.65] | 49.80 [41.50, 57.30] | 47.70 [41.90, 55.90] | 0.175 | nonnorm | |
| Menopausal status | Premenopausal | 747 (62.8) | 200 (66.2) | 182 (64.1) | 166 (59.1) | 199 (61.8) | 0.318 | |
| Postmenopausal | 442 (37.2) | 102 (33.8) | 102 (35.9) | 115 (40.9) | 123 (38.2) | |||
| BMI | 18.5–24.9 | 681 (57.1) | 173 (57.3) | 171 (59.6) | 156 (55.9) | 181 (55.7) | 0.699 | |
| <18.5 | 48 (4.0) | 9 (3.0) | 10 (3.5) | 12 (4.3) | 17 (5.2) | |||
| 25–29.9 | 304 (25.5) | 82 (27.2) | 72 (25.1) | 75 (26.9) | 75 (23.1) | |||
| >=30 | 160 (13.4) | 38 (12.6) | 34 (11.8) | 36 (12.9) | 52 (16.0) | |||
| BMI | 23.80 [21.50, 27.30] | 24.05 [21.50, 27.20] | 23.50 [21.50, 26.80] | 24.10 [21.70, 27.15] | 23.50 [21.20, 27.70] | 0.768 | nonnorm | |
| Smoking status | Never | 623 (65.2) | 175 (69.2) | 142 (62.8) | 141 (64.7) | 165 (63.7) | 0.476 | |
| Current | 179 (18.7) | 48 (19.0) | 43 (19.0) | 37 (17.0) | 51 (19.7) | |||
| Former | 154 (16.1) | 30 (11.9) | 41 (18.1) | 40 (18.3) | 43 (16.6) | |||
| Year BC diagnosis | 2002 | 89 (7.4) | 19 (6.2) | 24 (8.3) | 28 (10.0) | 18 (5.5) | <0.001 | |
| 2003 | 62 (5.2) | 17 (5.6) | 19 (6.6) | 8 (2.8) | 18 (5.5) | |||
| 2004 | 101 (8.4) | 17 (5.6) | 13 (4.5) | 30 (10.7) | 41 (12.6) | |||
| 2005 | 127 (10.6) | 22 (7.2) | 24 (8.3) | 33 (11.7) | 48 (14.7) | |||
| 2006 | 143 (11.9) | 32 (10.5) | 36 (12.5) | 42 (14.9) | 33 (10.1) | |||
| 2007 | 148 (12.3) | 34 (11.2) | 37 (12.8) | 40 (14.2) | 37 (11.3) | |||
| 2008 | 151 (12.6) | 48 (15.8) | 40 (13.9) | 31 (11.0) | 32 (9.8) | |||
| 2009 | 170 (14.2) | 34 (11.2) | 38 (13.2) | 46 (16.4) | 52 (16.0) | |||
| 2010 | 137 (11.4) | 55 (18.1) | 39 (13.5) | 13 (4.6) | 30 (9.2) | |||
| 2011 | 60 (5.0) | 18 (5.9) | 15 (5.2) | 10 (3.6) | 17 (5.2) | |||
| 2012 | 11 (0.9) | 8 (2.6) | 3 (1.0) | 0 (0.0) | 0 (0.0) | |||
| Genetic variants | No | 221 (82.8) | 58 (78.4) | 55 (85.9) | 48 (81.4) | 60 (85.7) | 0.581 | |
| Yes | 46 (17.2) | 16 (21.6) | 9 (14.1) | 11 (18.6) | 10 (14.3) | |||
| Clinical Tumor size (mm) | 40.00 [30.00, 55.00] | 40.00 [30.00, 55.00] | 40.00 [30.00, 50.00] | 40.00 [35.00, 55.00] | 45.00 [35.00, 60.00] | 0.332 | nonnorm | |
| Clinical T stage (TNM) | T0-T1 | 70 (5.8) | 19 (6.2) | 13 (4.5) | 20 (7.1) | 18 (5.5) | 0.372 | |
| T2 | 798 (66.6) | 201 (66.1) | 207 (72.1) | 181 (64.4) | 209 (64.1) | |||
| T3-T4 | 330 (27.5) | 84 (27.6) | 67 (23.3) | 80 (28.5) | 99 (30.4) | |||
| Clinical N stage (TNM) | N0 | 525 (43.8) | 120 (39.5) | 141 (49.0) | 130 (46.4) | 134 (41.1) | 0.067 | |
| N1-N2-N3 | 673 (56.2) | 184 (60.5) | 147 (51.0) | 150 (53.6) | 192 (58.9) | |||
| SBR grade | Grade I | 47 (4.1) | 11 (3.7) | 17 (6.0) | 13 (4.9) | 6 (1.9) | 0.249 | |
| Grade II | 432 (37.3) | 107 (36.1) | 104 (37.0) | 104 (39.0) | 117 (37.4) | |||
| Grade III | 678 (58.6) | 178 (60.1) | 160 (56.9) | 150 (56.2) | 190 (60.7) | |||
| KI67 | 30.00 [16.00, 55.00] | 27.50 [16.25, 50.00] | 30.00 [15.00, 50.00] | 30.00 [15.00, 55.00] | 33.00 [18.00, 60.00] | 0.438 | nonnorm | |
| KI67 | [0–10) | 65 (11.2) | 12 (8.5) | 20 (13.8) | 20 (14.6) | 13 (8.2) | 0.479 | |
| [10–20) | 110 (18.9) | 30 (21.1) | 27 (18.6) | 24 (17.5) | 29 (18.4) | |||
| >=20 | 407 (69.9) | 100 (70.4) | 98 (67.6) | 93 (67.9) | 116 (73.4) | |||
| Mitotic index | 15.00 [7.00, 28.00] | 14.00 [7.25, 28.00] | 14.00 [6.00, 28.00] | 14.00 [6.75, 26.00] | 15.00 [7.00, 30.00] | 0.967 | nonnorm | |
| Mitotic index | [0–7) mitose/2 mm2 | 341 (31.5) | 80 (29.6) | 89 (33.2) | 76 (31.1) | 96 (32.1) | 0.617 | |
| [7–13) mitose/2 mm2 | 295 (27.3) | 81 (30.0) | 64 (23.9) | 74 (30.3) | 76 (25.4) | |||
| >=13 mitose ou plus/2 mm2. | 445 (41.2) | 109 (40.4) | 115 (42.9) | 94 (38.5) | 127 (42.5) | |||
| BC subtype | Luminal | 528 (44.0) | 131 (43.1) | 143 (49.7) | 117 (41.6) | 137 (42.0) | 0.499 | |
| TNBC | 376 (31.4) | 100 (32.9) | 79 (27.4) | 91 (32.4) | 106 (32.5) | |||
| HER2+ | 295 (24.6) | 73 (24.0) | 66 (22.9) | 73 (26.0) | 83 (25.5) | |||
| DCIS component | No | 604 (60.8) | 159 (61.9) | 130 (53.9) | 142 (60.9) | 173 (66.0) | 0.048 | |
| Yes | 389 (39.2) | 98 (38.1) | 111 (46.1) | 91 (39.1) | 89 (34.0) | |||
| Stromal TIL levels (%) | 20.00 [10.00, 30.00] | 20.00 [10.00, 37.50] | 15.00 [10.00, 30.00] | 20.00 [10.00, 30.00] | 15.00 [10.00, 30.00] | 0.425 | nonnorm | |
| Stromal TIL levels (%) | [0–30] | 475 (66.2) | 116 (63.4) | 112 (68.7) | 110 (65.5) | 137 (67.5) | 0.730 | |
| >=30 | 242 (33.8) | 67 (36.6) | 51 (31.3) | 58 (34.5) | 66 (32.5) | |||
| IT TIL levels (%) | 5.00 [5.00, 15.00] | 5.00 [5.00, 20.00] | 5.00 [3.00, 15.00] | 5.00 [5.00, 11.25] | 5.00 [3.00, 15.00] | 0.559 | nonnorm | |
| IT TIL levels (%) | [0, 10] | 511 (71.3) | 122 (66.7) | 120 (73.6) | 126 (75.0) | 143 (70.4) | 0.315 | |
| (10, 100] | 206 (28.7) | 61 (33.3) | 43 (26.4) | 42 (25.0) | 60 (29.6) | |||
| LVI | No | 267 (61.0) | 61 (59.2) | 69 (63.3) | 69 (60.5) | 68 (60.7) | 0.942 | |
| Yes | 171 (39.0) | 42 (40.8) | 40 (36.7) | 45 (39.5) | 44 (39.3) | |||
| Histological type | NST | 1062 (93.5) | 276 (94.5) | 256 (93.1) | 247 (92.9) | 283 (93.4) | 0.859 | |
| Others | 74 (6.5) | 16 (5.5) | 19 (6.9) | 19 (7.1) | 20 (6.6) | |||
| Pathological complete response | No | 901 (75.5) | 232 (76.6) | 212 (73.9) | 213 (76.3) | 244 (75.3) | 0.870 | |
| Yes | 292 (24.5) | 71 (23.4) | 75 (26.1) | 66 (23.7) | 80 (24.7) | |||
| RCB index (continuous) | 1.82 [0.00, 3.06] | 1.76 [0.00, 2.77] | 1.67 [0.00, 3.01] | 1.79 [0.00, 3.04] | 2.06 [0.00, 3.30] | 0.203 | nonnorm | |
| Residual Cancer Burden class | RCB-0 | 202 (28.2) | 47 (25.7) | 54 (33.1) | 45 (26.8) | 56 (27.6) | 0.126 | |
| RCB-I | 65 (9.1) | 24 (13.1) | 11 (6.7) | 15 (8.9) | 15 (7.4) | |||
| RCB-II | 309 (43.1) | 84 (45.9) | 68 (41.7) | 77 (45.8) | 80 (39.4) | |||
| RCB-III | 141 (19.7) | 28 (15.3) | 30 (18.4) | 31 (18.5) | 52 (25.6) | |||
| ypN | 0 | 682 (57.0) | 172 (56.8) | 162 (56.4) | 173 (61.6) | 175 (53.7) | 0.746 | |
| [1–3] | 341 (28.5) | 84 (27.7) | 83 (28.9) | 68 (24.2) | 106 (32.5) | |||
| [4–9] | 145 (12.1) | 40 (13.2) | 35 (12.2) | 33 (11.7) | 37 (11.3) | |||
| 10 and more | 29 (2.4) | 7 (2.3) | 7 (2.4) | 7 (2.5) | 8 (2.5) | |||
| Stromal TIL levels (%) (post-NAC) | 10.00 [5.00, 15.00] | 10.00 [5.00, 20.00] | 10.00 [5.00, 15.00] | 7.00 [5.00, 15.00] | 10.00 [5.00, 20.00] | 0.013 | nonnorm | |
| Stromal TIL levels (%) (post-NAC) | [0, 10] | 473 (66.0) | 106 (57.6) | 115 (70.6) | 120 (71.4) | 132 (65.3) | 0.023 | |
| (10, 100] | 244 (34.0) | 78 (42.4) | 48 (29.4) | 48 (28.6) | 70 (34.7) | |||
| IT TIL levels (%) (post-NAC) | 5.00 [2.00, 10.00] | 5.00 [3.00, 10.00] | 5.00 [3.00, 10.00] | 5.00 [2.00, 6.25] | 5.00 [2.00, 10.00] | 0.163 | nonnorm | |
| IT TIL levels (%) (post-NAC) | [0, 10] | 420 (87.0) | 104 (83.9) | 92 (91.1) | 108 (90.0) | 116 (84.1) | 0.207 | |
| [10, 100] | 63 (13.0) | 20 (16.1) | 9 (8.9) | 12 (10.0) | 22 (15.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grandal, B.; Aljehani, A.; Dumas, E.; Daoud, E.; Jochum, F.; Gougis, P.; Hotton, J.; Lemoine, A.; Michel, S.; Laas, E.; et al. No Impact of Seasonality of Diagnoses on Baseline Tumor Immune Infiltration, Response to Treatment, and Prognosis in BC Patients Treated with NAC. Cancers 2022, 14, 3080. https://doi.org/10.3390/cancers14133080
Grandal B, Aljehani A, Dumas E, Daoud E, Jochum F, Gougis P, Hotton J, Lemoine A, Michel S, Laas E, et al. No Impact of Seasonality of Diagnoses on Baseline Tumor Immune Infiltration, Response to Treatment, and Prognosis in BC Patients Treated with NAC. Cancers. 2022; 14(13):3080. https://doi.org/10.3390/cancers14133080
Chicago/Turabian StyleGrandal, Beatriz, Ashwaq Aljehani, Elise Dumas, Eric Daoud, Floriane Jochum, Paul Gougis, Judicaël Hotton, Amélie Lemoine, Sophie Michel, Enora Laas, and et al. 2022. "No Impact of Seasonality of Diagnoses on Baseline Tumor Immune Infiltration, Response to Treatment, and Prognosis in BC Patients Treated with NAC" Cancers 14, no. 13: 3080. https://doi.org/10.3390/cancers14133080
APA StyleGrandal, B., Aljehani, A., Dumas, E., Daoud, E., Jochum, F., Gougis, P., Hotton, J., Lemoine, A., Michel, S., Laas, E., Laé, M., Pierga, J.-Y., Alaoui Ismaili, K., Lerebours, F., Reyal, F., & Hamy, A. S. (2022). No Impact of Seasonality of Diagnoses on Baseline Tumor Immune Infiltration, Response to Treatment, and Prognosis in BC Patients Treated with NAC. Cancers, 14(13), 3080. https://doi.org/10.3390/cancers14133080