
Finding Waldo: The Evolving Paradigm of Circulating Tumor DNA (ctDNA)—Guided Minimal Residual Disease (MRD) Assessment in Colorectal Cancer (CRC)


Abstract
:Simple Summary
Abstract
1. Introduction
2. Targeting MRD: Rationale and Evidence Supporting the Strategy
3. Biology of Cell-Free DNA
4. ctDNA Assays

{kind=link}
{kind=link}
| ctDNA Assay | Tumor-Informed | Assay Description | Target Alterations in Plasma DNA | Turnaround Time | Comments |
|---|---|---|---|---|---|
| Guardant REVEAL [28] | No | Plasma-only NGS-based test that integrates somatic alterations and epigenomic cancer signatures. | Somatic and epigenetic aberrations | 2 weeks | Integrating epigenomic signatures increased sensitivity by 25–36% versus genomic alterations alone. Fastest turnaround time as tumor sequencing is not required. |
| Safe-seqS [55] | Yes | Tumor sequencing followed by deep sequencing of plasma DNA with unique molecular barcoding to detect tumor-specific mutations. | One tumor-specific mutation in each patient | 2 weeks * | ctDNA result is classified as detectable (ctDNA-positive) or undetectable |
| Signatera [29] | Yes | A personalized, tumor-informed, multiplex PCR-based NGS assay. Sixteen patient-specific, somatic SNVs are selected for each patient based on the whole-exome sequencing of the tumor for interrogation in the cfDNA. Plasma samples with at least two tumor-specific SNVs are defined as ctDNA-positive. | 16 somatic variants | 7–10 days * | Limit of detection 0.01% variant allele frequency. Provides ctDNA level expressed as mean tumor molecules (MTM)/mL of plasma |
| ddPCR [58] | Yes | Targeted sequencing of the primary tumor for a predefined panel of 29 genes followed by an interrogation of plasma cfDNA by ddPCR to search for the tumor-specific mutations (1–2 mutations). | 1 to 2 alterations selected by tumor sequencing | 2–5 days * | Tracking at least two variants in plasma increased the ability to identify MRD to 87.5%. |
5. ctDNA-Guided MRD Assessment: Studies in Colorectal Cancer
6. ctDNA-Guided Surveillance
7. ctDNA-Guided Clinical Trials
8. Future Perspective
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; Sierra, M.S.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017, 66, 683–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, R.L.; Jakubowski, C.D.; Fedewa, S.A.; Davis, A.; Azad, N.S. Colorectal Cancer in the Young: Epidemiology, Prevention, Management. Am. Soc. Clin. Oncol. Educ. Book 2020, 40, e75–e88. [Google Scholar] [CrossRef] [PubMed]
- Rahib, L.; Wehner, M.R.; Matrisian, L.M.; Nead, K.T. Estimated Projection of US Cancer Incidence and Death to 2040. JAMA Netw. Open 2021, 4, e214708. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Guraya, S.Y. Pattern, Stage, and Time of Recurrent Colorectal Cancer After Curative Surgery. Clin. Colorectal. Cancer 2019, 18, e223–e228. [Google Scholar] [CrossRef]
- Luskin, M.R.; Murakami, M.A.; Manalis, S.R.; Weinstock, D.M. Targeting minimal residual disease: A path to cure? Nat. Rev. Cancer 2018, 18, 255–263. [Google Scholar] [CrossRef]
- Badia-Ramentol, J.; Linares, J.; Gómez-Llonin, A.; Calon, A. Minimal Residual Disease, Metastasis and Immunity. Biomolecules 2021, 11, 130. [Google Scholar] [CrossRef]
- Jessup, J.M.; Goldberg, R.M.; Aware, E.A. AJCC Cancer Staging Manual, 8th ed.; Amin, M.B., Ed.; AJCC: Chicago, IL, USA, 2017. [Google Scholar]
- Bockelman, C.; Engelmann, B.E.; Kaprio, T.; Hansen, T.F.; Glimelius, B. Risk of recurrence in patients with colon cancer stage II and III: A systematic review and meta-analysis of recent literature. Acta Oncol. 2015, 54, 5–16. [Google Scholar] [CrossRef]
- Osterman, E.; Glimelius, B. Recurrence Risk After Up-to-Date Colon Cancer Staging, Surgery, and Pathology: Analysis of the Entire Swedish Population. Dis. Colon Rectum 2018, 61, 1016–1025. [Google Scholar] [CrossRef]
- Påhlman, L.A.; Hohenberger, W.M.; Matzel, K.; Sugihara, K.; Quirke, P.; Glimelius, B. Should the Benefit of Adjuvant Chemotherapy in Colon Cancer Be Re-Evaluated? J. Clin. Oncol. 2016, 34, 1297–1299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osterman, E.; Hammarstrom, K.; Imam, I.; Osterlund, E.; Sjoblom, T.; Glimelius, B. Completeness and accuracy of the registration of recurrences in the Swedish Colorectal Cancer Registry (SCRCR) and an update of recurrence risk in colon cancer. Acta Oncol. 2021, 60, 842–849. [Google Scholar] [CrossRef] [PubMed]
- Argilés, G.; Tabernero, J.; Labianca, R.; Hochhauser, D.; Salazar, R.; Iveson, T.; Laurent-Puig, P.; Quirke, P.; Yoshino, T.; Taieb, J.; et al. Localised colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1291–1305. [Google Scholar] [CrossRef] [PubMed]
- Benson, A.I.; Venook, A.; Al-Hawary, M. NCCN Guidelines Version 1. 2022 Colon Cancer. Available online: https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf (accessed on 12 May 2022).
- Chakrabarti, S.; Peterson, C.Y.; Sriram, D.; Mahipal, A. Early stage colon cancer: Current treatment standards, evolving paradigms, and future directions. World J. Gastrointest. Oncol. 2020, 12, 808–832. [Google Scholar] [CrossRef]
- André, T.; Boni, C.; Navarro, M.; Tabernero, J.; Hickish, T.; Topham, C. Improved Overall Survival With Oxaliplatin, Fluorouracil, and Leucovorin As Adjuvant Treatment in Stage II or III Colon Cancer in the MOSAIC Trial. J. Clin. Oncol. 2009, 27, 3109–3116. [Google Scholar] [CrossRef] [Green Version]
- Andre, T.; de Gramont, A.; Vernerey, D.; Chibaudel, B.; Bonnetain, F.; Tijeras-Raballand, A.; Scriva, A.; Hickish, T.; Tabernero, J.; Van Laethem, J.L.; et al. Adjuvant Fluorouracil, Leucovorin, and Oxaliplatin in Stage II to III Colon Cancer: Updated 10-Year Survival and Outcomes According to BRAF Mutation and Mismatch Repair Status of the MOSAIC Study. J. Clin. Oncol. 2015, 33, 4176–4187. [Google Scholar] [CrossRef]
- Schmoll, H.J.; Tabernero, J.; Maroun, J.; de Braud, F.; Price, T.; Van Cutsem, E.; Hill, M.; Hoersch, S.; Rittweger, K.; Haller, D.G. Capecitabine Plus Oxaliplatin Compared With Fluorouracil/Folinic Acid As Adjuvant Therapy for Stage III Colon Cancer: Final Results of the NO16968 Randomized Controlled Phase III Trial. J. Clin. Oncol. 2015, 33, 3733–3740. [Google Scholar] [CrossRef]
- Bokey, L.; Chapuis, P.H.; Chan, C.; Stewart, P.; Rickard, M.J.F.X.; Keshava, A.; Dent, O.F. Long-term results following an anatomically based surgical technique for resection of colon cancer: A comparison with results from complete mesocolic excision. Colorectal Dis. 2016, 18, 676–683. [Google Scholar] [CrossRef] [Green Version]
- Chapuis, P.H.; Bokey, E.; Chan, C.; Keshava, A.; Rickard, M.; Stewart, P.; Young, C.J.; Dent, O.F. Recurrence and cancer-specific death after adjuvant chemotherapy for Stage III colon cancer. Colorectal Dis. 2019, 21, 164–173. [Google Scholar] [CrossRef]
- Iversen, L.H.; Green, A.; Ingeholm, P.; Østerlind, K.; Gögenur, I. Improved survival of colorectal cancer in Denmark during 2001–2012—The efforts of several national initiatives. Acta Oncol. 2016, 55, 10–23. [Google Scholar] [CrossRef] [Green Version]
- Lykke, J.; Roikjær, O.; Jess, P.; Group, T.D.C.C. The relation between lymph node status and survival in Stage I–III colon cancer: Results from a prospective nationwide cohort study. Colorectal Dis. 2013, 15, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Adams, R.A.; Meade, A.M.; Seymour, M.T.; Wilson, R.H.; Madi, A.; Fisher, D.; Kenny, S.L.; Kay, E.; Hodgkinson, E.; Pope, M.; et al. Intermittent versus continuous oxaliplatin and fluoropyrimidine combination chemotherapy for first-line treatment of advanced colorectal cancer: Results of the randomised phase 3 MRC COIN trial. Lancet Oncol. 2011, 12, 642–653. [Google Scholar] [CrossRef] [Green Version]
- Iveson, T.; Hanna, C.; Iveson, P.; Zhang, S.; Levasseur, A.; Meyerhardt, J. The Early Impact of the IDEA Collaboration Results: How the Results Changed Prescribing Practice. JNCI Cancer Spectr. 2021, 5, pkab043. [Google Scholar] [CrossRef] [PubMed]
- Chakrabarti, S.; Xie, H.; Urrutia, R.; Mahipal, A. The Promise of Circulating Tumor DNA (ctDNA) in the Management of Early-Stage Colon Cancer: A Critical Review. Cancers 2020, 12, 2808. [Google Scholar] [CrossRef]
- Henriksen, T.V.; Tarazona, N.; Frydendahl, A.; Reinert, T.; Gimeno-Valiente, F.; Carbonell-Asins, J.A.; Sharma, S.; Renner, D.; Hafez, D.; Roda, D.; et al. Circulating Tumor DNA in Stage III Colorectal Cancer, beyond Minimal Residual Disease Detection, toward Assessment of Adjuvant Therapy Efficacy and Clinical Behavior of Recurrences. Clin. Cancer Res. 2022, 28, 507–517. [Google Scholar] [CrossRef]
- Parikh, A.R.; Van Seventer, E.E.; Siravegna, G.; Hartwig, A.V.; Jaimovich, A.; He, Y.; Kanter, K.; Fish, M.G.; Fosbenner, K.D.; Miao, B.; et al. Minimal Residual Disease Detection using a Plasma-only Circulating Tumor DNA Assay in Patients with Colorectal Cancer. Clin. Cancer Res. 2021, 27, 5586–5594. [Google Scholar] [CrossRef]
- Reinert, T.; Henriksen, T.V.; Christensen, E.; Sharma, S.; Salari, R.; Sethi, H.; Knudsen, M.; Nordentoft, I.; Wu, H.-T.; Tin, A.S.; et al. Analysis of Plasma Cell-Free DNA by Ultradeep Sequencing in Patients With Stages I to III Colorectal Cancer. JAMA Oncol. 2019, 5, 1124–1131. [Google Scholar] [CrossRef] [Green Version]
- Tarazona, N.; Gimeno-Valiente, F.; Gambardella, V.; Zuñiga, S.; Rentero-Garrido, P.; Huerta, M.; Roselló, S.; Martinez-Ciarpaglini, C.; Carbonell-Asins, J.A.; Carrasco, F.; et al. Targeted next-generation sequencing of circulating-tumor DNA for tracking minimal residual disease in localized colon cancer. Ann. Oncol. 2019, 30, 1804–1812. [Google Scholar] [CrossRef] [Green Version]
- Tie, J.; Cohen, J.D.; Lo, S.N.; Wang, Y.; Li, L.; Christie, M.; Lee, M.; Wong, R.; Kosmider, S.; Skinner, I.; et al. Prognostic significance of postsurgery circulating tumor DNA in nonmetastatic colorectal cancer: Individual patient pooled analysis of three cohort studies. Int. J. Cancer 2021, 148, 1014–1026. [Google Scholar] [CrossRef]
- Tie, J.; Cohen, J.D.; Wang, Y.; Christie, M.; Simons, K.; Lee, M.; Wong, R.; Kosmider, S.; Ananda, S.; McKendrick, J.; et al. Circulating Tumor DNA Analyses as Markers of Recurrence Risk and Benefit of Adjuvant Therapy for Stage III Colon Cancer. JAMA Oncol. 2019, 5, 1710–1717. [Google Scholar] [CrossRef]
- Tie, J.; Cohen, J.D.; Wang, Y.; Li, L.; Christie, M.; Simons, K.; Elsaleh, H.; Kosmider, S.; Wong, R.; Yip, D.; et al. Serial circulating tumour DNA analysis during multimodality treatment of locally advanced rectal cancer: A prospective biomarker study. Gut 2019, 68, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Tie, J.; Kinde, I.; Wang, Y.; Wong, H.L.; Roebert, J.; Christie, M.; Tacey, M.; Wong, R.; Singh, M.; Karapetis, C.S.; et al. Circulating tumor DNA as an early marker of therapeutic response in patients with metastatic colorectal cancer. Ann. Oncol. 2015, 26, 1715–1722. [Google Scholar] [CrossRef] [PubMed]
- Blatter, S.; Rottenberg, S. Minimal residual disease in cancer therapy—Small things make all the difference. Drug Resist. Updates 2015, 21–22, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Batlle, E.; Clevers, H. Cancer stem cells revisited. Nat. Med. 2017, 23, 1124–1134. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Brenes, I.A.; Wodarz, D. Preventing clonal evolutionary processes in cancer: Insights from mathematical models. Proc. Natl. Acad. Sci. USA 2015, 112, 8843–8850. [Google Scholar] [CrossRef] [Green Version]
- McGranahan, N.; Swanton, C. Clonal Heterogeneity and Tumor Evolution: Past, Present, and the Future. Cell 2017, 168, 613–628. [Google Scholar] [CrossRef] [Green Version]
- Sargent, D.; Sobrero, A.; Grothey, A.; O’Connell, M.J.; Buyse, M.; Andre, T.; Zheng, Y.; Green, E.; Labianca, R.; O’Callaghan, C.; et al. Evidence for cure by adjuvant therapy in colon cancer: Observations based on individual patient data from 20,898 patients on 18 randomized trials. J. Clin. Oncol. 2009, 27, 872–877. [Google Scholar] [CrossRef]
- Kirkwood, J.M.; Tarhini, A.; Sparano, J.A.; Patel, P.; Schiller, J.H.; Vergo, M.T.; Benson Iii, A.B.; Tawbi, H. Comparative clinical benefits of systemic adjuvant therapy for paradigm solid tumors. Cancer Treat. Rev. 2013, 39, 27–43. [Google Scholar] [CrossRef] [Green Version]
- Pieters, R.; de Groot-Kruseman, H.; Van der Velden, V.; Fiocco, M.; van den Berg, H.; de Bont, E.; Egeler, R.M.; Hoogerbrugge, P.; Kaspers, G.; Van der Schoot, E.; et al. Successful Therapy Reduction and Intensification for Childhood Acute Lymphoblastic Leukemia Based on Minimal Residual Disease Monitoring: Study ALL10 From the Dutch Childhood Oncology Group. J. Clin. Oncol. 2016, 34, 2591–2601. [Google Scholar] [CrossRef] [Green Version]
- Braun, T.P.; Eide, C.A.; Druker, B.J. Response and Resistance to BCR-ABL1-Targeted Therapies. Cancer Cell. 2020, 37, 530–542. [Google Scholar] [CrossRef]
- Wu, Y.-L.; Tsuboi, M.; He, J.; John, T.; Grohe, C.; Majem, M.; Goldman, J.W.; Laktionov, K.; Kim, S.-W.; Kato, T.; et al. Osimertinib in Resected EGFR-Mutated Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2020, 383, 1711–1723. [Google Scholar] [CrossRef] [PubMed]
- Keller, L.; Belloum, Y.; Wikman, H.; Pantel, K. Clinical relevance of blood-based ctDNA analysis: Mutation detection and beyond. Brit. J. Cancer 2021, 124, 345–358. [Google Scholar] [CrossRef] [PubMed]
- Bronkhorst, A.J.; Ungerer, V.; Holdenrieder, S. The emerging role of cell-free DNA as a molecular marker for cancer management. Biomol. Detect. Quantif. 2019, 17, 100087. [Google Scholar] [CrossRef] [PubMed]
- Wan, J.C.M.; Massie, C.; Garcia-Corbacho, J.; Mouliere, F.; Brenton, J.D.; Caldas, C.; Pacey, S.; Baird, R.; Rosenfeld, N. Liquid biopsies come of age: Towards implementation of circulating tumour DNA. Nat. Rev. Cancer 2017, 17, 223–238. [Google Scholar] [CrossRef] [PubMed]
- Bando, H.; Nakamura, Y.; Taniguchi, H.; Shiozawa, M.; Yasui, H.; Esaki, T.; Kagawa, Y.; Denda, T.; Satoh, T.; Yamazaki, K.; et al. Effects of Metastatic Sites on Circulating Tumor DNA in Patients With Metastatic Colorectal Cancer. JCO Precis. Oncol. 2022, 6, e2100535. [Google Scholar] [CrossRef]
- Bettegowda, C.; Sausen, M.; Leary, R.J.; Kinde, I.; Wang, Y.; Agrawal, N.; Bartlett, B.R.; Wang, H.; Luber, B.; Alani, R.M.; et al. Detection of circulating tumor DNA in early- and late-stage human malignancies. Sci. Transl. Med. 2014, 6, 224ra224. [Google Scholar] [CrossRef] [Green Version]
- Diehl, F.; Schmidt, K.; Choti, M.A.; Romans, K.; Goodman, S.; Li, M.; Thornton, K.; Agrawal, N.; Sokoll, L.; Szabo, S.A.; et al. Circulating mutant DNA to assess tumor dynamics. Nat. Med. 2008, 14, 985–990. [Google Scholar] [CrossRef]
- Schwarzenbach, H.; Hoon, D.S.; Pantel, K. Cell-free nucleic acids as biomarkers in cancer patients. Nat. Rev. Cancer 2011, 11, 426–437. [Google Scholar] [CrossRef]
- Mouliere, F.; Chandrananda, D.; Piskorz, A.M.; Moore, E.K.; Morris, J.; Ahlborn, L.B.; Mair, R.; Goranova, T.; Marass, F.; Heider, K.; et al. Enhanced detection of circulating tumor DNA by fragment size analysis. Sci. Transl. Med. 2018, 10, eaat4921. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.S.; Kim, M.; Seong, M.W.; Kim, H.S.; Lee, Y.K.; Kang, H.J. Plasma vs. serum in circulating tumor DNA measurement: Characterization by DNA fragment sizing and digital droplet polymerase chain reaction. Clin. Chem. Lab. Med. 2020, 58, 527–532. [Google Scholar] [CrossRef] [Green Version]
- Henriksen, T.V.; Reinert, T.; Christensen, E.; Sethi, H.; Birkenkamp-Demtröder, K.; Gögenur, M.; Gögenur, I.; Zimmermann, B.G.; Group, I.S.; Dyrskjøt, L.; et al. The effect of surgical trauma on circulating free DNA levels in cancer patients-implications for studies of circulating tumor DNA. Mol. Oncol. 2020, 14, 1670–1679. [Google Scholar] [CrossRef] [PubMed]
- Shinde, S.; Saxena, S.; Dixit, V.; Tiwari, A.K.; Vishvakarma, N.K.; Shukla, D. Epigenetic Modifiers and Their Potential Application in Colorectal Cancer Diagnosis and Therapy. Crit. Rev. Oncog. 2020, 25, 95–109. [Google Scholar] [CrossRef] [PubMed]
- Tie, J.; Wang, Y.; Tomasetti, C.; Li, L.; Springer, S.; Kinde, I.; Silliman, N.; Tacey, M.; Wong, H.L.; Christie, M.; et al. Circulating tumor DNA analysis detects minimal residual disease and predicts recurrence in patients with stage II colon cancer. Sci. Transl. Med. 2016, 8, 346ra392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbosh, C.; Swanton, C.; Birkbak, N.J. Clonal haematopoiesis: A source of biological noise in cell-free DNA analyses. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2019, 30, 358–359. [Google Scholar] [CrossRef]
- Nikbakht, H.; Jessa, S.; Sukhai, M.A.; Arseneault, M.; Zhang, T.; Letourneau, L.; Thomas, M.; Bourgey, M.; Roehrl, M.H.A.; Eveleigh, R.; et al. Latency and interval therapy affect the evolution in metastatic colorectal cancer. Sci. Rep. 2020, 10, 581. [Google Scholar] [CrossRef]
- Tarazona, N.; Gimeno-Valiente, F.; Gambardella, V.; Huerta, M.; Roselló, S.; Zuniga, S.; Calon, A.; Carbonell-Asins, J.A.; Fontana, E.; Martinez-Ciarpaglini, C.; et al. Detection of postoperative plasma circulating tumour DNA and lack of CDX2 expression as markers of recurrence in patients with localised colon cancer. ESMO Open 2020, 5, e000847. [Google Scholar] [CrossRef]
- McDuff, S.G.R.; Hardiman, K.M.; Ulintz, P.J.; Parikh, A.R.; Zheng, H.; Kim, D.W.; Lennerz, J.K.; Hazar-Rethinam, M.; Seventer, E.E.V.; Fetter, I.J.; et al. Circulating Tumor DNA Predicts Pathologic and Clinical Outcomes Following Neoadjuvant Chemoradiation and Surgery for Patients With Locally Advanced Rectal Cancer. JCO Precis. Oncol. 2021, 5, 123–132. [Google Scholar] [CrossRef]
- Tie, J.; Wang, Y.; Cohen, J.; Li, L.; Hong, W.; Christie, M.; Wong, H.L.; Kosmider, S.; Wong, R.; Thomson, B.; et al. Circulating tumor DNA dynamics and recurrence risk in patients undergoing curative intent resection of colorectal cancer liver metastases: A prospective cohort study. PLoS Med. 2021, 18, e1003620. [Google Scholar] [CrossRef]
- Loupakis, F.; Sharma, S.; Derouazi, M.; Murgioni, S.; Biason, P.; Rizzato, M.D.; Rasola, C.; Renner, D.; Shchegrova, S.; Koyen Malashevich, A.; et al. Detection of Molecular Residual Disease Using Personalized Circulating Tumor DNA Assay in Patients With Colorectal Cancer Undergoing Resection of Metastases. JCO Precis. Oncol. 2021, 5, 1166–1177. [Google Scholar] [CrossRef]
- Kotaka, M.; Shirasu, H.; Watanabe, J.; Yamazaki, K.; Hirata, K.; Akazawa, N.; Matsuhashi, N.; Yokota, M.; Ikeda, M.; Kato, K.; et al. Association of circulating tumor DNA dynamics with clinical outcomes in the adjuvant setting for patients with colorectal cancer from an observational GALAXY study in CIRCULATE-Japan. J. Clin. Oncol. 2022, 40, 9. [Google Scholar] [CrossRef]
- Tie, J.; Cohen, J.D.; Lahouel, K.; Lo, S.N.; Wang, Y.; Kosmider, S.; Wong, R.; Shapiro, J.; Lee, M.; Harris, S.; et al. Circulating Tumor DNA Analysis Guiding Adjuvant Therapy in Stage II Colon Cancer. N. Engl. J. Med. 2022, 386, 2261–2272. [Google Scholar] [CrossRef]
- Litvak, A.; Cercek, A.; Segal, N.; Reidy-Lagunes, D.; Stadler, Z.K.; Yaeger, R.D.; Kemeny, N.E.; Weiser, M.R.; Pessin, M.S.; Saltz, L. False-positive elevations of carcinoembryonic antigen in patients with a history of resected colorectal cancer. J. Natl. Compr. Cancer Netw. JNCCN 2014, 12, 907–913. [Google Scholar] [CrossRef] [PubMed]
- Grothey, A.; Sobrero, A.F.; Shields, A.F.; Yoshino, T.; Paul, J.; Taieb, J.; Souglakos, J.; Shi, Q.; Kerr, R.; Labianca, R.; et al. Duration of Adjuvant Chemotherapy for Stage III Colon Cancer. N. Engl. J. Med. 2018, 378, 1177–1188. [Google Scholar] [CrossRef] [PubMed]
- Taieb, J.; Taly, V.; Henriques, J.; Bourreau, C.; Mineur, L.; Bennouna, J.; Desrame, J.; Louvet, C.; Lepere, C.; Mabro, M.; et al. Prognostic Value and Relation with Adjuvant Treatment Duration of ctDNA in Stage III Colon Cancer: A Post Hoc Analysis of the PRODIGE-GERCOR IDEA-France Trial. Clin. Cancer Res. 2021, 27, 5638–5646. [Google Scholar] [CrossRef] [PubMed]
- Desch, C.E.; Benson, A.B., III; Somerfield, M.R.; Flynn, P.J.; Krause, C.; Loprinzi, C.L.; Minsky, B.D.; Pfister, D.G.; Virgo, K.S.; Petrelli, N.J. Colorectal Cancer Surveillance: 2005 Update of an American Society of Clinical Oncology Practice Guideline. J. Clin. Oncol. 2005, 23, 8512–8519. [Google Scholar] [CrossRef] [PubMed]
- Jeffery, M.; Hickey, B.E.; Hider, P.N. Follow-up strategies for patients treated for non-metastatic colorectal cancer. Cochrane Database Syst. Rev. 2019, 9, CD002200. [Google Scholar] [CrossRef]
- Lepage, C.; Phelip, J.M.; Cany, L.; Faroux, R.; Manfredi, S.; Ain, J.F.; Pezet, D.; Baconnier, M.; Deguiral, P.; Terrebone, E.; et al. Effect of 5 years of imaging and CEA follow-up to detect recurrence of colorectal cancer: The FFCD PRODIGE 13 randomised phase III trial. Dig. Liver Dis. 2015, 47, 529–531. [Google Scholar] [CrossRef]
- Henriksen, T.V.; Tarazona, N.; Reinert, T.; Carbonell-Asins, J.A.; Renner, D.; Sharma, S.; Roda, D.; Huerta, M.; Roselló, S.; Iversen, L.H.; et al. Circulating tumor DNA analysis for assessment of recurrence risk, benefit of adjuvant therapy, and early relapse detection after treatment in colorectal cancer patients. J. Clin. Oncol. 2021, 39, 11. [Google Scholar] [CrossRef]
- Ungerer, V.; Bronkhorst, A.J.; Holdenrieder, S. Preanalytical variables that affect the outcome of cell-free DNA measurements. Crit. Rev. Clin. Lab. Sci. 2020, 57, 484–507. [Google Scholar] [CrossRef]
- Connors, D.; Allen, J.; Alvarez, J.D.; Boyle, J.; Cristofanilli, M.; Hiller, C.; Keating, S.; Kelloff, G.; Leiman, L.; McCormack, R.; et al. International liquid biopsy standardization alliance white paper. Crit. Rev. Oncol. Hematol. 2020, 156, 103112. [Google Scholar] [CrossRef]
- Dasari, A.; Morris, V.K.; Allegra, C.J.; Atreya, C.; Benson, A.B.; Boland, P.; Chung, K.; Copur, M.S.; Corcoran, R.B.; Deming, D.A.; et al. ctDNA applications and integration in colorectal cancer: An NCI Colon and Rectal–Anal Task Forces whitepaper. Nat. Rev. Clin. Oncol. 2020, 17, 757–770. [Google Scholar] [CrossRef] [PubMed]
- Reinert, T.; Scholer, L.V.; Thomsen, R.; Tobiasen, H.; Vang, S.; Nordentoft, I.; Lamy, P.; Kannerup, A.S.; Mortensen, F.V.; Stribolt, K.; et al. Analysis of circulating tumour DNA to monitor disease burden following colorectal cancer surgery. Gut 2016, 65, 625–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scholer, L.V.; Reinert, T.; Orntoft, M.W.; Kassentoft, C.G.; Arnadottir, S.S.; Vang, S.; Nordentoft, I.; Knudsen, M.; Lamy, P.; Andreasen, D.; et al. Clinical Implications of Monitoring Circulating Tumor DNA in Patients with Colorectal Cancer. Clin. Cancer Res. 2017, 23, 5437–5445. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Li, L.; Cohen, J.D.; Kinde, I.; Ptak, J.; Popoli, M.; Schaefer, J.; Silliman, N.; Dobbyn, L.; Tie, J.; et al. Prognostic Potential of Circulating Tumor DNA Measurement in Postoperative Surveillance of Nonmetastatic Colorectal Cancer. JAMA Oncol. 2019, 5, 1118–1123. [Google Scholar] [CrossRef] [PubMed]
- Kasi, P.M.; Fehringer, G.; Taniguchi, H.; Starling, N.; Nakamura, Y.; Kotani, D.; Powles, T.; Li, B.T.; Pusztai, L.; Aushev, V.N.; et al. Impact of Circulating Tumor DNA–Based Detection of Molecular Residual Disease on the Conduct and Design of Clinical Trials for Solid Tumors. JCO Precis. Oncol. 2022, 6, e2100181. [Google Scholar] [CrossRef]
- Rolfo, C.; Cardona, A.F.; Cristofanilli, M.; Paz-Ares, L.; Diaz Mochon, J.J.; Duran, I.; Raez, L.E.; Russo, A.; Lorente, J.A.; Malapelle, U.; et al. Challenges and opportunities of cfDNA analysis implementation in clinical practice: Perspective of the International Society of Liquid Biopsy (ISLB). Crit. Rev. Oncol. Hematol. 2020, 151, 102978. [Google Scholar] [CrossRef]
- Liu, M.C.; Oxnard, G.R.; Klein, E.A.; Swanton, C.; Seiden, M.V.; Liu, M.C.; Oxnard, G.R.; Klein, E.A.; Smith, D.; Richards, D.; et al. Sensitive and specific multi-cancer detection and localization using methylation signatures in cell-free DNA. Ann. Oncol. 2020, 31, 745–759. [Google Scholar] [CrossRef]
- Xie, H.; Mahoney, D.W.; Foote, P.H.; Burger, K.N.; Doering, K.A.; Taylor, W.R.; Then, S.S.; Cao, X.; McGlinch, M.; Berger, C.K.; et al. Novel Methylated DNA Markers in the Surveillance of Colorectal Cancer Recurrence. Clin. Cancer Res. 2021, 27, 141–149. [Google Scholar] [CrossRef]
- Naidoo, M.; Gibbs, P.; Tie, J. ctDNA and Adjuvant Therapy for Colorectal Cancer: Time to Re-Invent Our Treatment Paradigm. Cancers 2021, 13, 346. [Google Scholar] [CrossRef]

| Study | Patient Population | n | ctDNA Assay | ctDNA Testing Time Points | Major Findings | Comments |
|---|---|---|---|---|---|---|
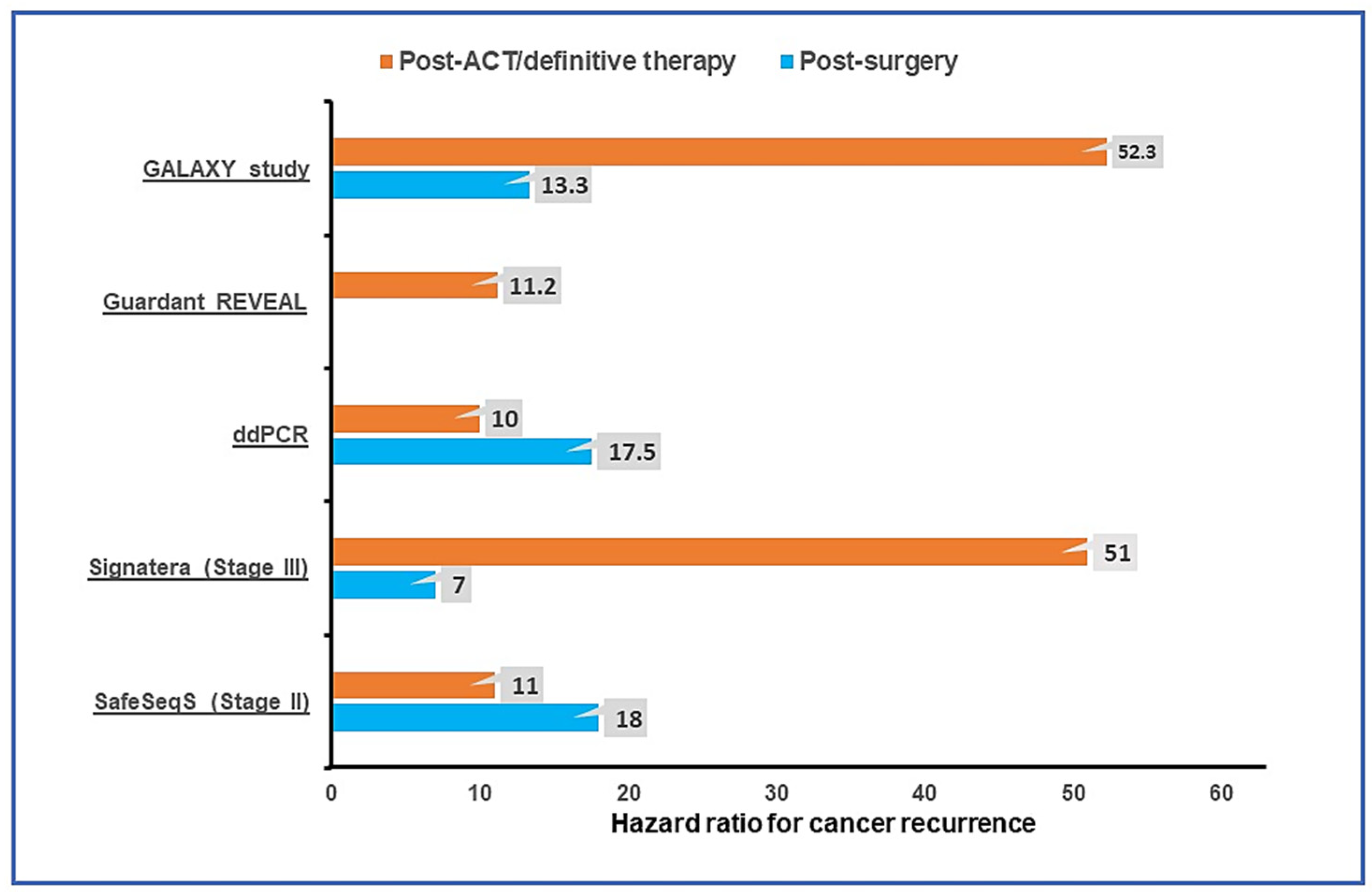
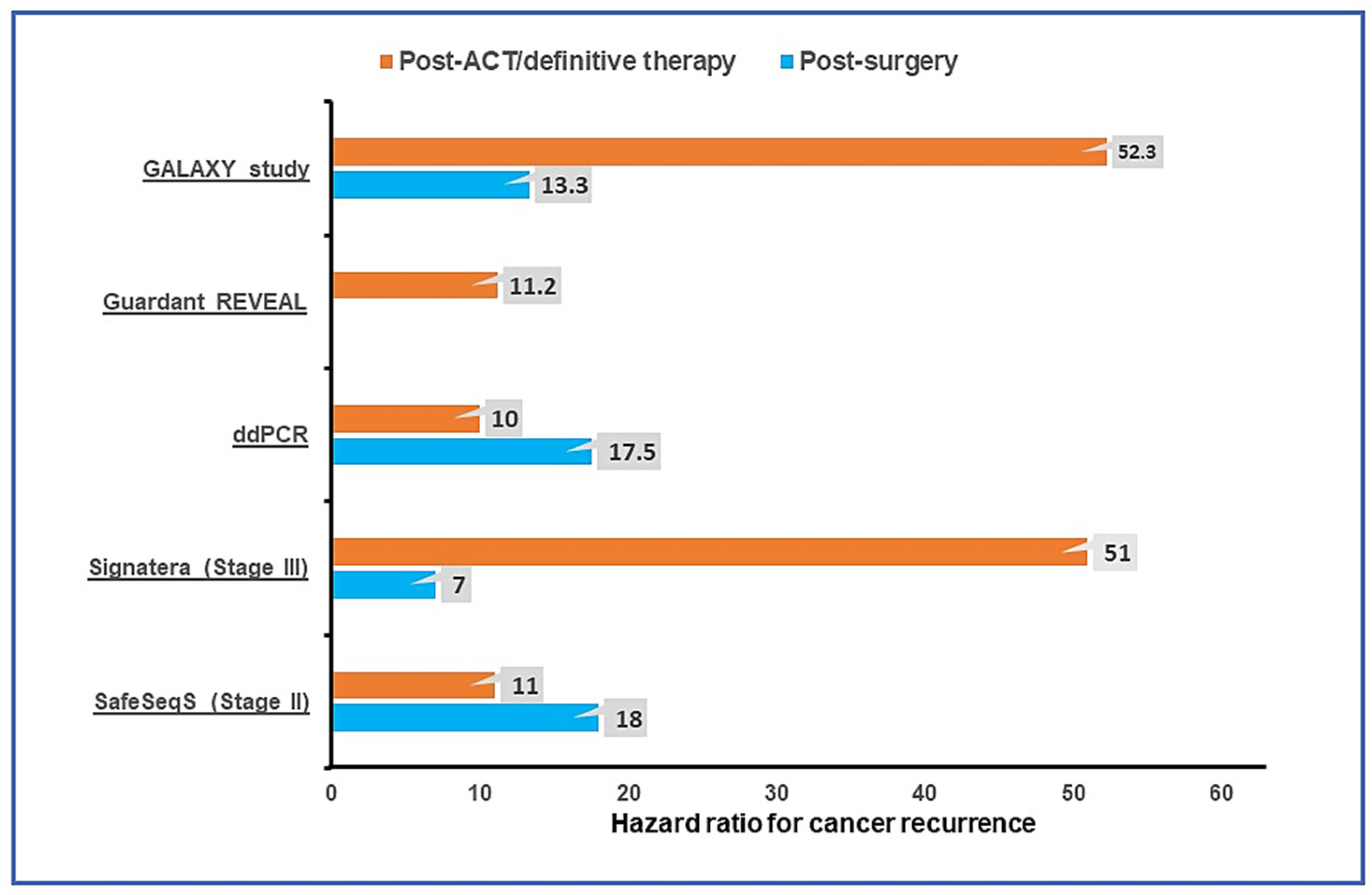
| Tie et al., 2016 [55] | Stage II CC | 230 | Safe-SeqS | 4–10 weeks post-op and every 3 months for 2 years | Cohort not receiving ACT If ctDNA-+ve post-op: HR for cancer recurrence—18 (95% CI, 7.9 to 40). Cohort receiving ACT If ctDNA-+ve post-ACT: HR for recurrence—11 (95% CI, 1.8 to 68). | ctDNA detection preceded radiologic recurrence by a median of 5.5 months. |
| Reinert et al., 2019 [29] | Stages I to III CRC | 130 | Signatera | Preop, post-op day 30, and every 3 months for up to 3 years. | HR for cancer recurrence with positive ctDNA:
| Serial ctDNA analyses revealed disease recurrence up to 16.5 months ahead of radiologic imaging (mean, 8.7 months; range, 0.8–16.5 months). |
| Tie et al., 2019 [32] | Stage III CC | 96 | Safe-SeqS | 4–10 weeks post-op and within 6 weeks of ACT completion | HR for cancer recurrence with positive ctDNA:
| RFS at 3 years in patients who are ctDNA-positive vs. -negative: post-op 47% vs. 76%, post-ACT 30% vs. 77%. |
| Tarazona et al., 2019 [30] | Stages I to III CC | 150 | Tumor-informed ddPCR | Preop, 6–8 weeks post-op and every 4 months up to 5 years. | HR for recurrence with positive ctDNA:
| ctDNA detection during surveillance preceded radiological recurrence by a median of 11.5 months. |
| Henriksen et al., 2022 [27] | Stage III CRC | 168 | Signatera | 2–4 weeks post-op and every 3 months thereafter | Detection of ctDNA was a strong recurrence predictor post-o (HR = 7.0; 95% CI, 3.7–13.5) and immediately after ACT (HR = 50.76; 95% CI, 15.4–167). | ctDNA detected recurrence with a median lead-time of 9.8 months compared with radiologic studies. |
| Parikh et al., 2021 [28] | Stages I–IV CRC | 103 | Tumor-uninformed assay (REVEAL) | Post-op, post-ACT, and longitudinally in some patients | HR for recurrence when +ve for ctDNA post definitive therapy and with >1 year of follow-up: 11.28. | Integrating epigenomic signatures increased sensitivity by 25–36% versus genomic alterations alone. |
| Tie et al., 2019 [33] | Locally advanced rectal carcinoma | 159 | Safe-SeqS | Pretreatment, post CRT, and 4–10 weeks after surgery. | Significantly worse RFS if ctDNA was detectable after CRT (HR, 6.6; p < 0.001) or after surgery (HR, 13.0; p < 0.001). | The estimated 3-year RFS was 33% for the post-op ctDNA-positive patients and 87% for the post-op ctDNA-negative patients. |
| McDuff et al., 2021 [59] | Locally advanced rectal carcinoma | 29 | ddPCR | Baseline, preop, and post-op | At a median follow-up of 20 months, patients with detectable post-op ctDNA experienced poorer RFS (HR, 11.56; p = 0.007). | All patients (4 of 4) with detectable post-op ctDNA recurred, whereas only 2 of 15 patients with undetectable ctDNA recurred (negative predictive value = 87%). |
| Tie et al., 2021 [60] | CRC with liver metastasis | 54 | Safe-SeqS | Preop and post-op samples, serial samples during pre- or post-op chemotherapy, and follow-up | Detectable post-op ctDNA predicted a significantly lower RFS (HR, 6.3; 95% CI, 2.58 to 15.2; p < 0.001) and OS (HR, 4.2; 95% CI, 1.5 to 11.8; p < 0.001) | End-of-treatment (surgery +/− ACT) ctDNA detection was associated with a 5-year RFS of 0% compared to 75.6% for patients with an undetectable end-of-treatment ctDNA (HR, 14.9; 95% CI, 4.94 to 44.7; p < 0.001). |
| Loupakis et al., 2021 [61] | CRC undergoing liver resection | 112 | Signatera | Post-op, at the time of radiologic relapse or last follow-up. | ctDNA-positive status was also associated with an inferior overall survival: HR: 16.0; 95% CI, 3.9 to 68.0; p < 0.001. | ctDNA was detectable in the post-op sample in 54.4% (61 of 112) of patients, of which 96.7% (59 of 61) progressed at the time of data cutoff (HR: 5.8; 95% CI, 3.5 to 9.7; p < 0.001). |
| Kotaka et al., 2022 (Galaxy study) [62] | Stages I–IV CRC patients | 1365 | Signatera | Before surgery, 1-month post-op and every 3 months thereafter for 2 years | Six-month DFS rate was significantly higher in patients whose ctDNA was converted with ACT compared to patients who remained positive after ACT with an HR of 52.3 (95% CI: 7.2–380.5; p < 0.001), after a median follow-up of 6.6 months. | Cumulative incidence of ctDNA clearance was significantly higher with ACT vs. non-ACT (67% vs. 7% by 24 weeks; cumulative HR = 17.1; 95% CI: 6.7–43.4, p < 0.001). |
| Tie et al., 2022 (DYNAMIC) [63] | Stage II CC | 455 | SafeSeqS | 4 and 7 weeks post-surgery | Adjuvant therapy guided by ctDNA resulted in chemotherapy administration in lower proportion of patients without any detriment to 2-year RFS. | DYNAMIC is the first reported prospective randomized study supporting the ctDNA-guided adjuvant therapy approach in stage II colon cancer. |
| Study Identifier | Study Phase | Study Population | n | ctDNA Assay | Study Description | Primary Endpoint |
|---|---|---|---|---|---|---|
| NCT04068103 (COBRA) | II/III | Stage II CC without high-risk features | 1408 | LUNAR-1 (Guardant Health) | Arm A: active surveillance. Arm B: ctDNA directed therapy (ctDNA-positive → FOLFOX/CAPOX for 6 months, ctDNA-negative → active surveillance) | Clearance of ctDNA with ACT (phase II) and RFS (phase III) |
| NCT05174169 (CIRCULATE-US) | II/III | Stage II and III CC | 1912 | Signatera | Cohort A: Arm 1—ctDNA-negative treated with FOLFOX 3–6 months/CAPOX 3 months. Arm 2—ctDNA-negative undergoing serial ctDNA monitoring and no treatment. Cohort B: Arm 3—ctDNA-+ve treated with FOLFOX/CAPOX for 6 months. Arm 4—ctDNA-+ve treated with mFOLFIRINOX | TTPos (time from randomization until ctDNA-positive event), DFS |
| NCT04120701 (CIRCULATE-PRODIGE 70) | III | Resected Stage II CC | 1980 | ddPCR | ctDNA-positive → randomized (2:1) to receive ACT or no ACT. ctDNA-negative → surveillance. | 3-year DFS in ctDNA-positive patients. |
| ACTRN12615000381583 (DYNAMIC-II) | III | Stage II CC | 450 | Safe-SeqS | Arm A: positive for ctDNA → ACT, negative for ctDNA → surveillance. Arm B: treated at the discretion of the clinicians. | RFS |
| ACTRN12617001566325 (DYNAMIC-III) | II/III | Stage III CC | 1000 | Safe-SeqS | Arm A: standard of care. Arm B: ctDNA-informed (ctDNA-negative → therapy de-escalation; ctDNA-positive → therapy escalation) | RFS |
| GALAXY (UMIN000039205) | Prospective observational | Stages II∓IV CRC | 2500 | Signatera | Serial ctDNA monitoring after surgery. If ctDNA-negative--> VEGA trial (therapy de-escalation). If ctDNA-+ve → ALTAIR trial. | DFS |
| VEGA (jRCT1031200006) | III | High-risk stage II or low-risk stage III CC | 1240 | Signatera | Designed to compare adjuvant CAPOX for 3 months vs. observation for GALAXY patients with negative ctDNA at week 4 after surgery. | DFS |
| NCT04089631 (CIRCULATE AIO-KRK-0217) | III | Stage II CC | 4812 | NGS | Patients positive for ctDNA post-resection are randomized to observation vs. capecitabine or CAPOX (investigator’s choice) × 6 months | DFS |
| MEDOCC-CrEATE (NL6281/NTR6455) | III | Stage II CC | 1320 | PGDx elio™ | Standard of care surveillance vs. ctDNA-guided ACT (ctDNA-positive: 6 months of CAPOX; ctDNA-negative: surveillance) | The proportion of patients receiving ACT after surgery if ctDNA-positive. |
| NCT03748680 (IMPROVE-IT) | II | Stage I and II CRC | 64 | ddPCR, NGS | ctDNA-positive patients randomized to observation vs.FOLFOX or CAPOX for 6 months. | DFS |
| NCT04264702 (BESPOKE) | Prospective Observational | Stage II and III CRC | 1000 | Signatera | Serial ctDNA testing following surgery and ACT vs. observation at the discretion of the treating clinician. Control arm-matched stage II and III patients with a minimum 2 years of follow-up data. | 1. Impact of ctDNA on adjuvant treatment decisions. 2. Rate of ctDNA detected recurrence while asymptomatic. |
| NCT04259944 (PEGASUS) | II | Resected MSS stage III and high-risk stage II (T4N0) CC | 140 | LUNAR-1 (Guardant Health) | ctDNA-guided ACT. (i) ctDNA-positive → CAPOX for 3 months; (ii) ctDNA-negative → capecitabine for 6 months but will be retested after 1 cycle, and if found ctDNA-positive, will be switched to CAPOX. | The number of patients negative for ctDNA post-op and post ACT later turning ctDNA-positive or developing radiographic relapse. |
| NCT04084249 (IMPROVE-IT2) | III | Stage III or high-risk stage II CRC | 254 | ddPCR, NGS | Patients were randomized to ctDNA-guided post-operative surveillance or standard-of-care CT-scan surveillance. | Fraction of patients with relapse receiving curative resection or local treatment |
| NCT03803553 (ACT-3) | III | Stage III CC | 500 | LUNAR-1 (Guardant Health) | ctDNA-enriched second-line adjuvant therapy: patients are distributed post-ACT as follows- 1. ctDNA-negative: active surveillance; 2. ctDNA-positive: (a) MSS patients- 6 months of FOLFIRI vs. active surveillance, (b) MSI high-6 months of nivolumab, (c) BRAF mutant and MSS-6 months of BRAF directed therapy. | DFS, ctDNA clearance rate |
| NCT04457297 (ALTAIR) | III | Stage II∓IV CRC | 240 | Signatera | TAS-102 for 6 months vs. placebo for patients positive for ctDNA following completion of standard ACT and no evidence of relapse radiologically in the GALAXY study | DFS |
| NCT03436563 | Ib/II | Stage IV CRC | 74 | Signatera | Patients with metastatic CRC positive for ctDNA following resection of all metastases will receive M7824 (anti-PDL1/TGFbetaRII fusion protein) for 6 doses | ctDNA clearance rate |
| NCT04589468 | Ia/b | CRC, breast, and prostate cancer stage I–III | 70 | Signatera | Patients with primary breast, prostate, or colorectal cancer and detectable ctDNA (n = 50) post definitive treatment will perform one of five escalating dose levels of exercise. | RP2D of exercise |
| NCT04853017 (Amplify-201) | I/II | Solid tumors, including CRC with RAS mutation | 18 | Signatera | Patients with tumors harboring RAS mutation and minimal residual disease with detection of ctDNA receive different dose levels of ELI-002, a RAS targeting vaccine. | 1. MTD of ELI-002 and the RP2D 2. Safety |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chakrabarti, S.; Kasi, A.K.; Parikh, A.R.; Mahipal, A. Finding Waldo: The Evolving Paradigm of Circulating Tumor DNA (ctDNA)—Guided Minimal Residual Disease (MRD) Assessment in Colorectal Cancer (CRC). Cancers 2022, 14, 3078. https://doi.org/10.3390/cancers14133078
Chakrabarti S, Kasi AK, Parikh AR, Mahipal A. Finding Waldo: The Evolving Paradigm of Circulating Tumor DNA (ctDNA)—Guided Minimal Residual Disease (MRD) Assessment in Colorectal Cancer (CRC). Cancers. 2022; 14(13):3078. https://doi.org/10.3390/cancers14133078
Chicago/Turabian StyleChakrabarti, Sakti, Anup Kumar Kasi, Aparna R. Parikh, and Amit Mahipal. 2022. "Finding Waldo: The Evolving Paradigm of Circulating Tumor DNA (ctDNA)—Guided Minimal Residual Disease (MRD) Assessment in Colorectal Cancer (CRC)" Cancers 14, no. 13: 3078. https://doi.org/10.3390/cancers14133078
APA StyleChakrabarti, S., Kasi, A. K., Parikh, A. R., & Mahipal, A. (2022). Finding Waldo: The Evolving Paradigm of Circulating Tumor DNA (ctDNA)—Guided Minimal Residual Disease (MRD) Assessment in Colorectal Cancer (CRC). Cancers, 14(13), 3078. https://doi.org/10.3390/cancers14133078