
Analysis of the Effect of Tumor-Grade Change on the Prognosis of Retroperitoneal Sarcoma

 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
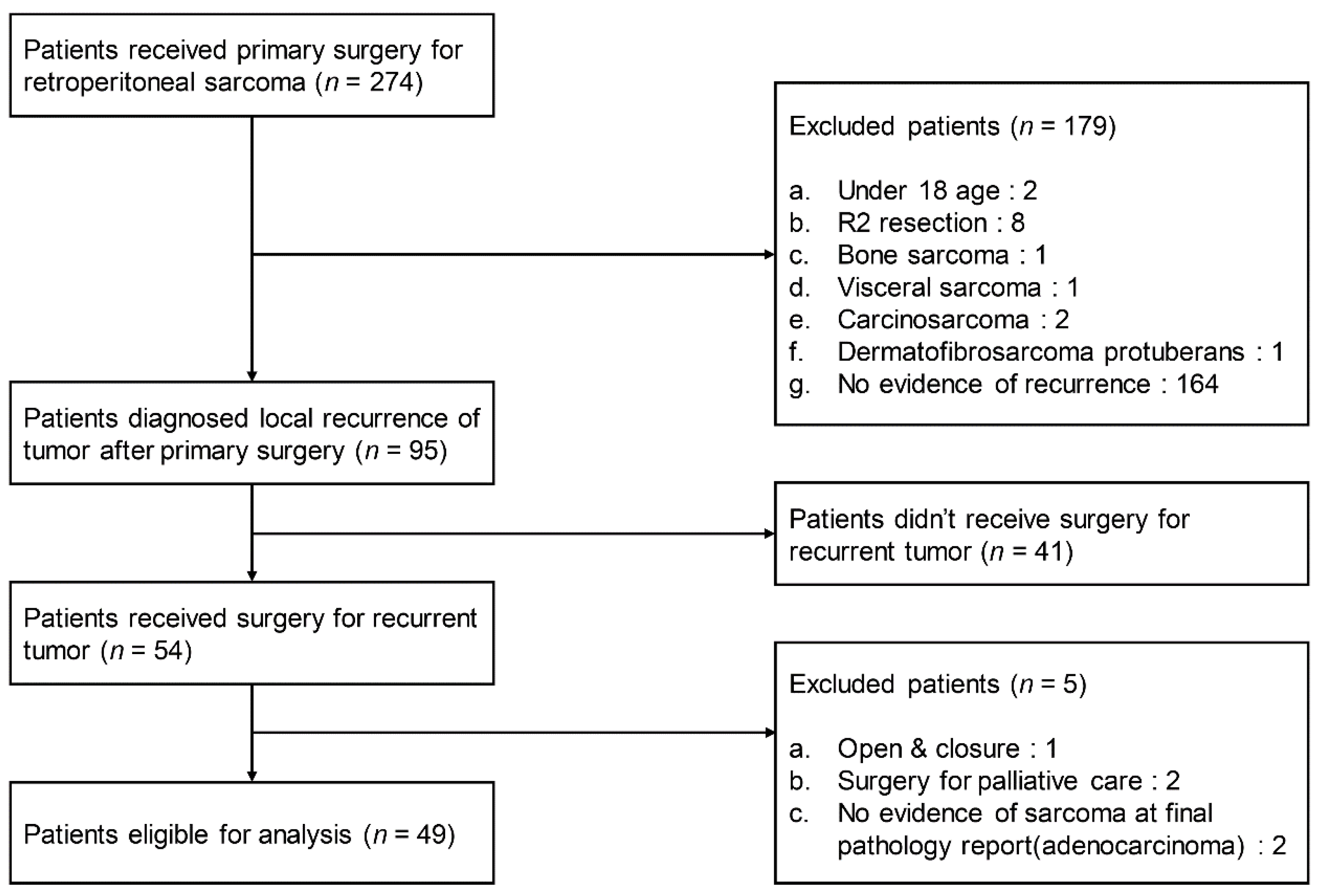
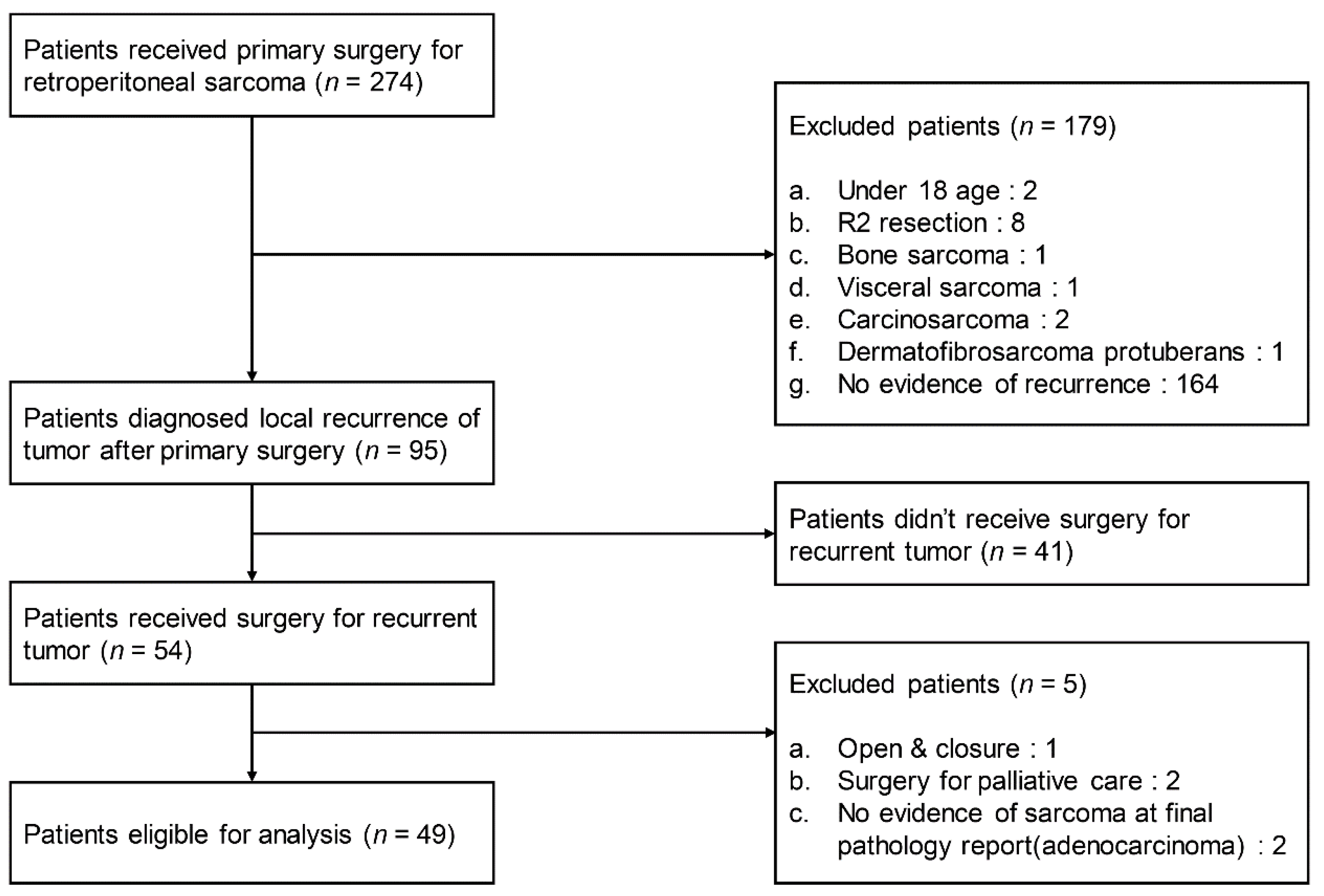
2.1. Patients
2.2. Definition of Changes in Tumor Grade
2.3. Statistical Analysis
2.4. Ethical Approval
2.5. Informed Consent
3. Results
3.1. Frequency of Changes in Tumor Grade
3.2. Patient Demographics
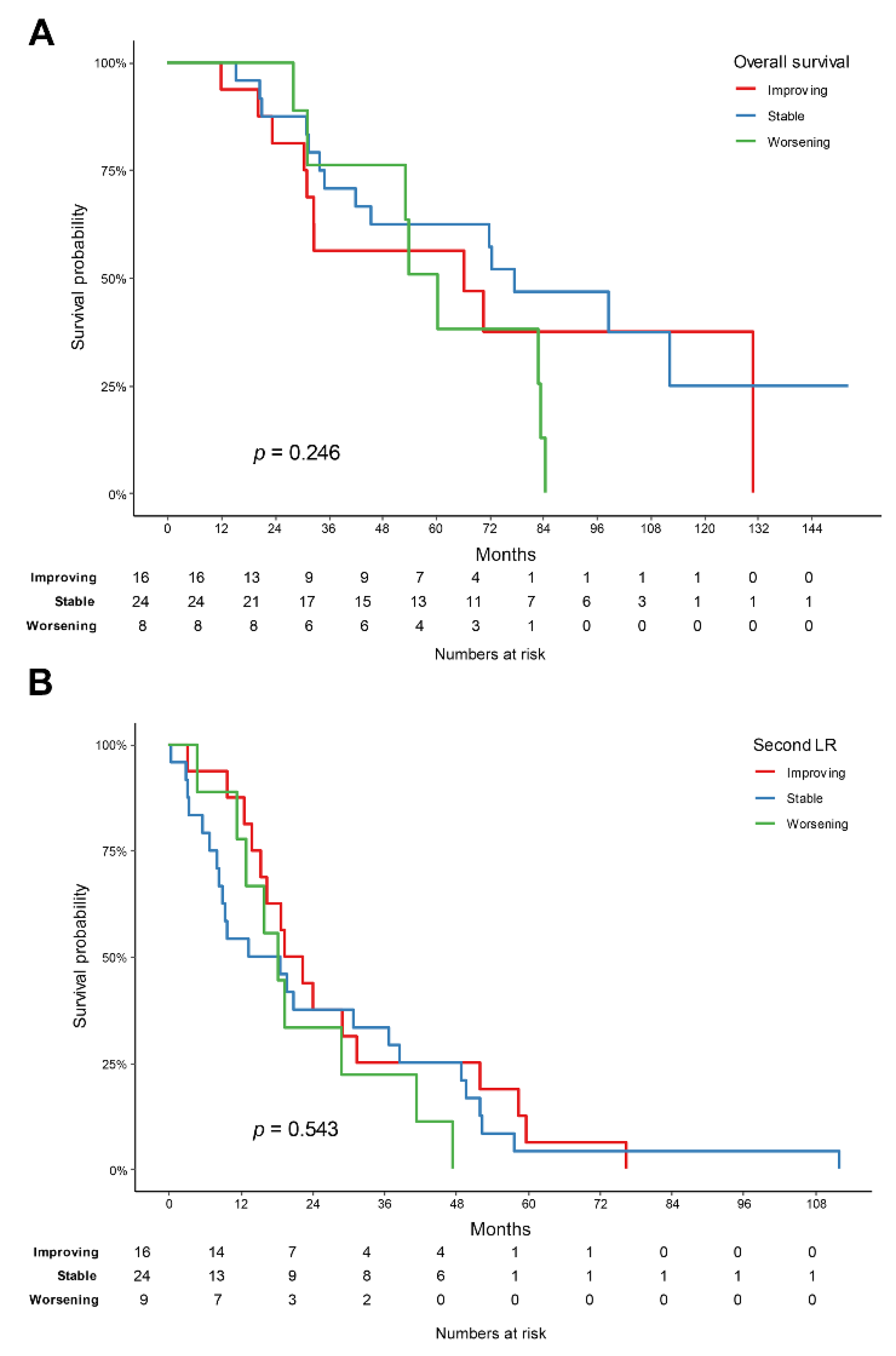
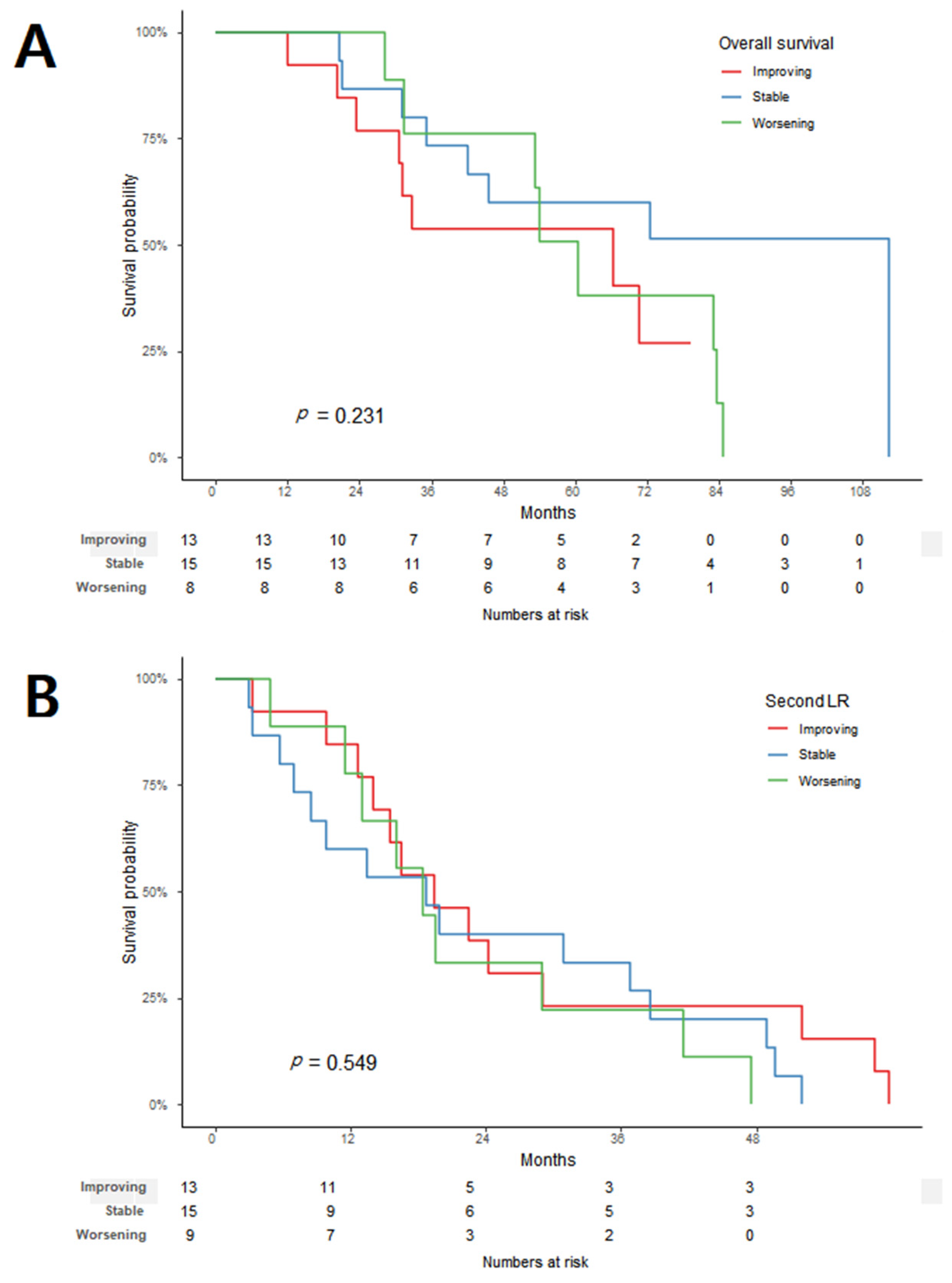
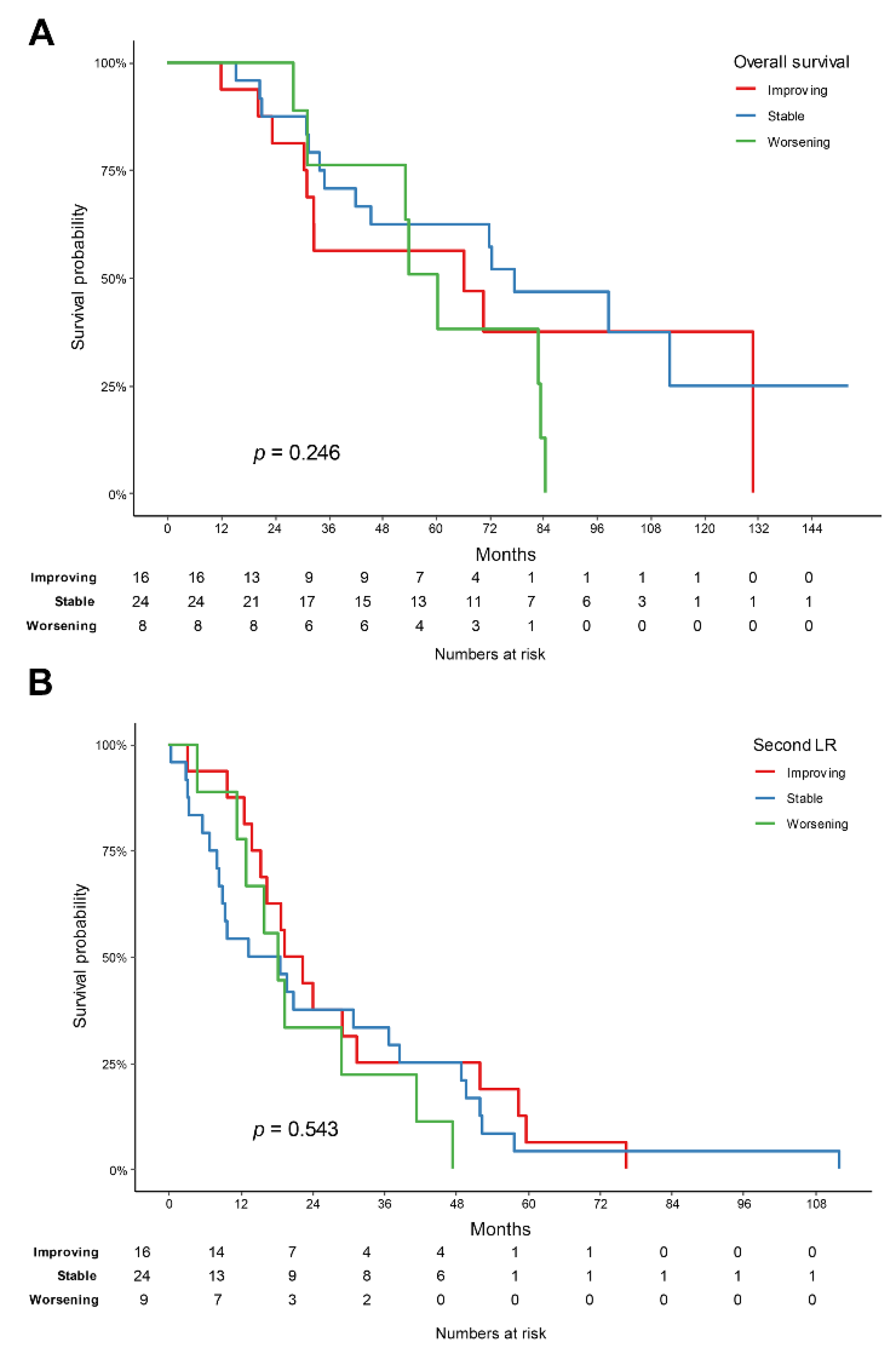
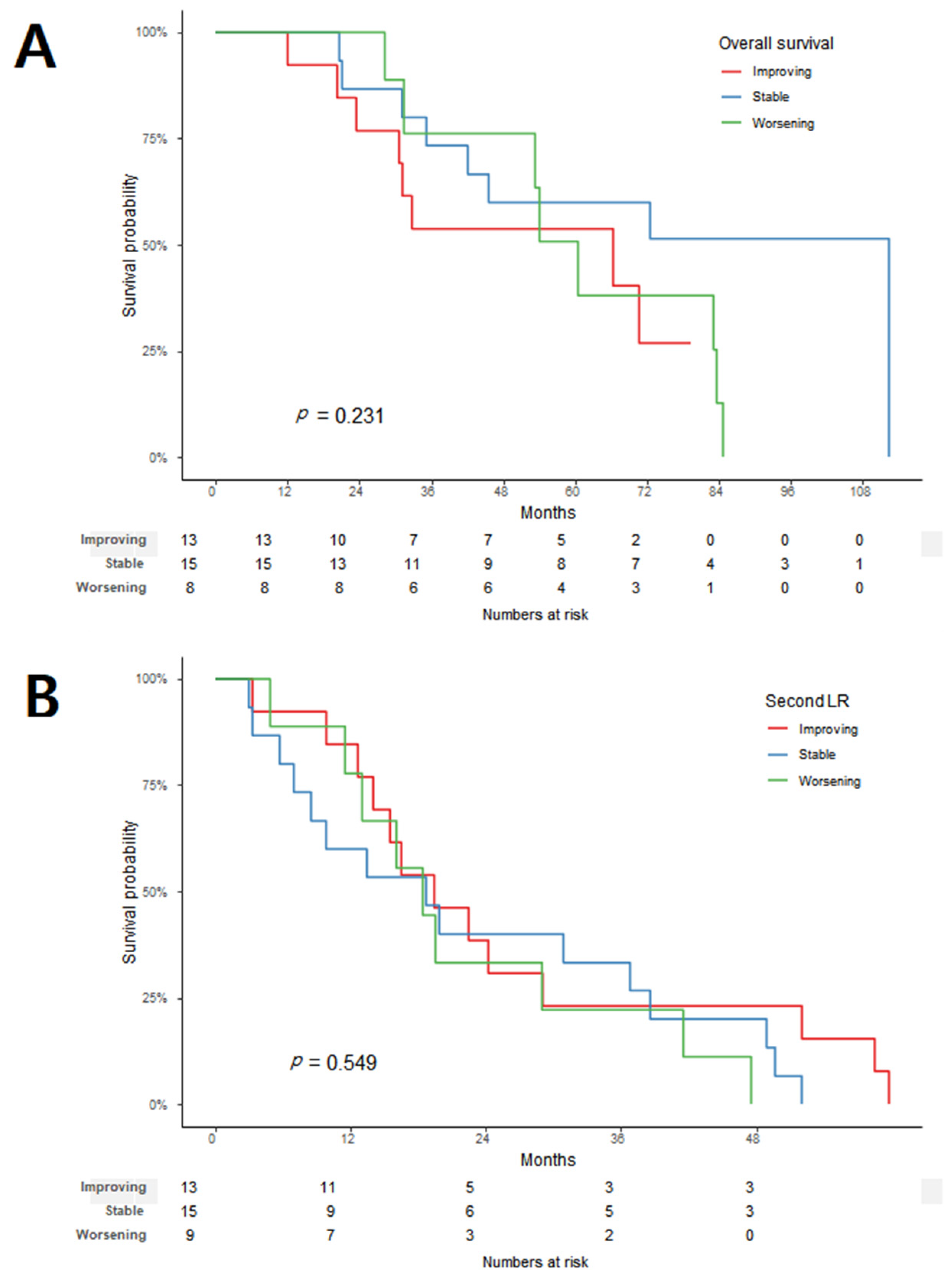
3.3. Tumor-Grade Change and Prognosis
3.4. Analyses of Factors Affecting Overall Survival and Second Local Recurrence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gronchi, A.; Vullo, S.L.; Fiore, M.; Mussi, C.; Stacchiotti, S.; Collini, P.; Lozza, L.; Pennacchioli, E.; Mariani, L.; Casali, P.G. Aggressive Surgical Policies in a Retrospectively Reviewed Single-Institution Case Series of Retroperitoneal Soft Tissue Sarcoma Patients. J. Clin. Oncol. 2009, 27, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Gronchi, A.; Bonvalot, S.; Le Cesne, A.; Casali, P.G. Resection of uninvolved adjacent organs can be part of surgery for ret-roperitoneal soft tissue sarcoma. J. Clin. Oncol. 2009, 27, 2106–2107. [Google Scholar] [CrossRef] [PubMed]
- Pasquali, S.; Vohra, R.; Tsimopoulou, I.; Vijayan, D.; Gourevitch, D.; Desai, A. Outcomes Following Extended Surgery for Retroperitoneal Sarcomas: Results From a UK Referral Centre. Ann. Surg. Oncol. 2015, 22, 3550–3556. [Google Scholar] [CrossRef] [PubMed]
- Gronchi, A.; Strauss, D.C.; Miceli, R.; Bonvalot, S.; Swallow, C.J.; Hohenberger, P.; Van Coevorden, F.; Rutkowski, P.; Call-egaro, D.; Hayes, A.J.; et al. Variability in Patterns of Recurrence After Resection of Primary Retroperitoneal Sarcoma (RPS): A Report on 1007 Patients From the Multi-institutional Collaborative RPS Working Group. Ann. Surg. 2016, 263, 1002–1009. [Google Scholar] [CrossRef]
- Tan, M.C.; Brennan, M.F.; Kuk, D.; Agaram, N.P.; Antonescu, C.R.; Qin, L.X.; Moraco, N.; Crago, A.M.; Singer, S. Histology-based Classification Predicts Pattern of Recurrence and Improves Risk Stratification in Primary Retroperitoneal Sarcoma. Ann. Surg. 2016, 263, 593–600. [Google Scholar] [CrossRef] [Green Version]
- Gronchi, A.; Miceli, R.; Allard, M.A.; Callegaro, D.; Le Péchoux, C.; Fiore, M.; Honoré, C.; Sanfilippo, R.; Coppola, S.; Stacchiotti, S.; et al. Personalizing the Approach to Retroperitoneal Soft Tissue Sarcoma: Histology-specific Patterns of Failure and Postrelapse Outcome after Primary Extended Resection. Ann. Surg. Oncol. 2014, 22, 1447–1454. [Google Scholar] [CrossRef]
- MacNeill, A.J.; Miceli, R.; Strauss, D.C.; Bonvalot, S.; Hohenberger, P.; Van Coevorden, F.; Rutkowski, P.; Callegaro, D.; Hayes, A.J.; Honoré, C.; et al. Post-relapse outcomes after primary extended resection of retroperitoneal sarcoma: A report from the Trans-Atlantic RPS Working Group. Cancer 2017, 123, 1971–1978. [Google Scholar] [CrossRef]
- Trans-Atlantic RPS Working Group. Management of Recurrent Retroperitoneal Sarcoma (RPS) in the Adult: A Consensus Approach from the Trans-Atlantic RPS Working Group. Ann. Surg. Oncol. 2016, 23, 3531–3540. [Google Scholar] [CrossRef]
- Bonvalot, S.; Gronchi, A.; Le Pechoux, C.; Swallow, C.J.; Strauss, D.; Meeus, P.; van Coevorden, F.; Stoldt, S.; Stoeckle, E.; Rutkowski, P.; et al. Preoperative radiotherapy plus surgery versus surgery alone for patients with primary retroperitoneal sar-coma (EORTC-62092: STRASS): A multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2020, 21, 1366–1377. [Google Scholar] [CrossRef]
- Van Houdt, W.J.; Raut, C.P.; Bonvalot, S.; Swallow, C.J.; Haas, R.; Gronchi, A. New research strategies in retroperitoneal sarcoma. The case of TARPSWG, STRASS and RESAR: Making progress through collaboration. Curr. Opin. Oncol. 2019, 31, 310–316. [Google Scholar] [CrossRef]
- Hager, S.; Makowiec, F.; Henne, K.; Hopt, U.T.; Wittel, U.A. Significant benefits in survival by the use of surgery combined with radiotherapy for retroperitoneal soft tissue sarcoma. Radiat. Oncol. 2017, 12, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almond, L.M.; Gronchi, A.; Strauss, D.; Jafri, M.; Ford, S.; Desai, A. Neoadjuvant and adjuvant strategies in retroperitoneal sarcoma. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2018, 44, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Lahat, G.; Anaya, D.A.; Wang, X.; Tuvin, D.; Lev, D.; Pollock, R.E. Resectable Well-Differentiated versus Dedifferentiated Liposarcomas: Two Different Diseases Possibly Requiring Different Treatment Approaches. Ann. Surg. Oncol. 2008, 15, 1585–1593. [Google Scholar] [CrossRef] [PubMed]
- Singer, S.; Antonescu, C.R.; Riedel, E.; Brennan, M.F. Histologic subtype and margin of resection predict pattern of recurrence and survival for retroperitoneal liposarcoma. Ann. Surg. 2003, 238, 358–370; discussion 351–370. [Google Scholar] [CrossRef] [PubMed]
- Nessim, C.; Raut, C.P.; Callegaro, D.; Barretta, F.; Miceli, R.; Fairweather, M.; Blay, J.-Y.; Strauss, D.; Rutkowski, P.; Ahuja, N.; et al. Analysis of Differentiation Changes and Outcomes at Time of First Recurrence of Retroperitoneal Liposarcoma by Transatlantic Australasian Retroperitoneal Sarcoma Working Group (TARPSWG). Ann. Surg. Oncol. 2021, 28, 7854–7863. [Google Scholar] [CrossRef]
- Guillou, L.; Coindre, J.M.; Bonichon, F.; Nguyen, B.B.; Terrier, P.; Collin, F.; O Vilain, M.; Mandard, A.M.; Le Doussal, V.; Leroux, A.; et al. Comparative study of the National Cancer Institute and French Federation of Cancer Centers Sarcoma Group grading systems in a population of 410 adult patients with soft tissue sarcoma. J. Clin. Oncol. 1997, 15, 350–362. [Google Scholar] [CrossRef]
- Tropea, S.; Mocellin, S.; Damiani, G.B.; Stramare, R.; Aliberti, C.; Del Fiore, P.; Rossi, C.R.; Rastrelli, M. Recurrent retroper-itoneal sarcomas: Clinical outcomes of surgical treatment and prognostic factors. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2021, 47, 1201–1206. [Google Scholar]
- Anaya, D.A.; Lahat, G.; Wang, X.; Xiao, L.; Pisters, P.W.; Cormier, J.N.; Hunt, K.K.; Feig, B.W.; Lev, D.C.; Pollock, R.E. Postoperative nomogram for survival of patients with retroperitoneal sarcoma treated with curative intent. Ann. Oncol. 2010, 21, 397–402. [Google Scholar] [CrossRef]
- Nathan, H.; Raut, C.P.; Thornton, K.; Herman, J.M.; Ahuja, N.; Schulick, R.D.; Choti, M.A.; Pawlik, T.M. Predictors of sur-vival after resection of retroperitoneal sarcoma: A population-based analysis and critical appraisal of the AJCC staging system. Ann. Surg. 2009, 250, 970–976. [Google Scholar] [CrossRef] [Green Version]
- Malinka, T.; Nebrig, M.; Klein, F.; Pratschke, J.; Bahra, M.; Andreou, A. Analysis of outcomes and predictors of long-term survival following resection for retroperitoneal sarcoma. BMC Surg. 2019, 19, 61. [Google Scholar] [CrossRef]
- Yang, J.-Y.; Kong, S.-H.; Ahn, H.S.; Lee, H.-J.; Jeong, S.-Y.; Ha, J.; Yang, H.-K.; Park, K.J.; Lee, K.U.; Choe, K.J. Prognostic factors for reoperation of recurrent retroperitoneal sarcoma: The role of clinicopathological factors other than histologic grade. J. Surg. Oncol. 2014, 111, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Squires, M.H.; Ethun, C.G.; Donahue, E.E.; Benbow, J.H.; Anderson, C.J.; Jagosky, M.H.; Salo, J.C.; Hill, J.S.; Ahrens, W.; Prabhu, R.S.; et al. A multi-institutional validation study of prognostic nomograms for retroperitoneal sarcoma. J. Surg. Oncol. 2021, 124, 829–837. [Google Scholar] [CrossRef] [PubMed]
- Chouliaras, K.; Senehi, R.; Ethun, C.G.; Poultsides, G.; Tran, T.; Grignol, V.; Gamblin, T.C.; Roggin, K.K.; Tseng, J.; Fields, R.C.; et al. Recurrence patterns after resection of retroperitoneal sarcomas: An eight-institution study from the US Sarcoma Col-laborative. J. Surg. Oncol. 2019, 120, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Tyler, R.; Lee, M.; Ierodiakonou, V.; Hodson, J.; Taniere, P.; Almond, M.; Ford, S.; Desai, A. Prognostic implications of his-tological organ involvement in retroperitoneal sarcoma. BJS open 2021, 5, zrab080. [Google Scholar] [CrossRef] [PubMed]
- Nizri, E.; Fiore, M.; Barretta, F.; Colombo, C.; Radaelli, S.; Callegaro, D.; Sanfilippo, R.; Sangalli, C.; Collini, P.; Stacchiotti, S.; et al. Intraperitoneal Invasion of Retroperitoneal Sarcomas: A Risk Factor for Dismal Prognosis. Ann. Surg. Oncol. 2019, 26, 3535–3541. [Google Scholar] [CrossRef]
- Park, J.O.; Qin, L.X.; Prete, F.P.; Antonescu, C.; Brennan, M.F.; Singer, S. Predicting outcome by growth rate of locally re-current retroperitoneal liposarcoma: The one centimeter per month rule. Ann. Surg. 2009, 250, 977–982. [Google Scholar] [CrossRef]
- Lewis, J.J.; Leung, D.; Woodruff, J.M.; Brennan, M.F. Retroperitoneal soft-tissue sarcoma: Analysis of 500 patients treated and followed at a single institution. Ann. Surg. 1998, 228, 355–365. [Google Scholar] [CrossRef]
- Neuhaus, S.J.; Barry, P.; A Clark, M.; Hayes, A.J.; Fisher, C.; Thomas, J.M. Surgical management of primary and recurrent retroperitoneal liposarcoma. Br. J. Surg. 2004, 92, 246–252. [Google Scholar] [CrossRef]
- Grobmyer, S.R.; Wilson, J.P.; Apel, B.; Knapik, J.; Bell, W.C.; Kim, T.; Bland, K.I.; Copeland, E.M.; Hochwald, S.N.; Heslin, M.J. Recurrent Retroperitoneal Sarcoma: Impact of Biology and Therapy on Outcomes. J. Am. Coll. Surg. 2010, 210, 602–608. [Google Scholar] [CrossRef]
- Van Dalen, T.; Hoekstra, H.J.; van Geel, A.N.; van Coevorden, F.; Albus-Lutter, C.; Slootweg, P.J.; Hennipman, A.; Dutch Soft Tissue Sarcoma, G. Locoregional recurrence of retroperitoneal soft tissue sarcoma: Second chance of cure for selected patients. Eur. J. Surg. Oncol. 2001, 27, 564–568. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Primary tumor | Grade 1 | Grade 2 | Grade 3 | n | |
|---|---|---|---|---|---|
| Recurrent tumor | |||||
| Grade 1 | 2 | 3 | 1 | n = 6 | |
| Grade 2 | 6 | 9 | 12 | n = 27 | |
| Grade 3 | 1 | 2 | 13 | n = 16 | |
| n | n = 9 | n = 14 | n = 26 | n = 49 | |
 : Improving group
: Improving group  : Stable group
: Stable group  : Worsening group.
: Worsening group.| Variable | Improving Group (n = 16) | Stable Group (n = 24) | Worsening Group (n = 9) | p Value |
|---|---|---|---|---|
| Age (years) | 56.77 ± 9.59 | 50.67 ± 11.11 | 60.86 ± 8.76 | 0.033 |
| Sex (n, %) | ||||
| Male | 7 (43.8) | 15 (62.5) | 6 (66.7) | |
| Female | 9 (56.2) | 9 (37.5) | 3 (33.3) | 0.474 |
| BMI | 23.18 ± 3.08 | 23.12 ± 2.51 | 23.71 ± 2.22 | 0.805 |
| Underlying disease (n) | ||||
| Diabetes mellitus | 1 | 1 | 1 | 0.760 |
| Hypertension | 6 | 2 | 2 | 0.054 |
| Coronary artery disease | 1 | 0 | 0 | 0.184 |
| Primary tumor | ||||
| Histologic subtype (n, %) | ||||
| Well-differentiated liposarcoma | 0 (0.0) | 2 (8.2) | 7 (77.8) | |
| Dedifferentiated liposarcoma | 13 (81.2) | 12 (50.0) | 2 (22.2) | <0.001 |
| Liposarcoma, NOS | 0 (0.0) | 1 (4.2) | 0 (0.0) | |
| Leiomyosarcoma | 1 (6.2) | 1 (4.2) | 0 (0.0) | |
| Malignant peripheral nerve sheath tumor | 2 (12.5) | 1 (4.2) | 0 (0.0) | |
| Others | 0 (0.0) | 7 (29.2) | 0 (0.0) | |
| FNCLCC grade (n, %) | ||||
| I | 0 (0.0) | 2 (8.3) | 7 (77.8) | <0.001 |
| II | 3 (18.8) | 9 (37.5) | 2 (22.2) | |
| III | 13 (81.2) | 13 (54.2) | 0 (0.0) | |
| Recurrent tumor | ||||
| Histologic subtype (n, %) | ||||
| Well-differentiated liposarcoma | 2 (12.5) | 2 (8.3) | 0 (0.0) | |
| Dedifferentiated liposarcoma | 11 (68.8) | 10 (41.7) | 9 (100.0) | 0.096 |
| Liposarcoma, NOS (not otherwise specified) | 0 (0.0) | 3 (12.5) | 0 (0.0) | |
| Leiomyosarcoma | 1 (6.2) | 1 (4.2) | 0 (0.0) | |
| Malignant peripheral nerve sheath tumor | 2 (12.5) | 2 (8.3) | 0 (0.0) | |
| Others | 0 (0.0) | 6 (25.0) | 0 (0.0) | |
| FNCLCC grade (n, %) | ||||
| I | 4 (25.0) | 2 (8.3) | 0 (0.0) | |
| II | 12 (75.0) | 9 (37.5) | 6 (66.7) | |
| III | 0 (0.0) | 13 (54.2) | 3 (33.3) | |
| Tumor size (mm, mean) | 63.12 ± 60.94 | 61.54 ± 34.73 | 75.55 ± 37.41 | 0.633 |
| R2 resection (n, %) | 3 (18.8) | 6 (25.0) | 1 (11.1) | 0.726 |
| Radiotherapy (n, %) | ||||
| Given | 8 (50.0) | 12 (50.0) | 5 (55.6) | |
| Not given | 8 (50.0) | 12 (50.0) | 4 (44.4) | 1.000 |
| Chemotherapy (n, %) | ||||
| Given | 1 (6.2) | 0 (0.0) | 0 (0.0) | 0.510 |
| Not given | 15 (93.8) | 24 (100.0) | 9 (100.0) |
| Variables | Univariate | Multivariate | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Improving + stable group vs. worsening group | 0.56 (0.25, 1.28) | 0.17 | ||
| FNCLCC grade of primary tumor | ||||
| High grade (III) vs. low to intermediate grades (I+II) | 2.21 (1.06, 4.6) | 0.034 | 2.37 (1.13, 4.99) | 0.023 |
| Histologic subtype of primary tumor: ref. = DDLPS | ||||
| WDLPS | 1.14 (0.47, 2.76) | 0.765 | ||
| LPS, NOS | 2.32 (0.3, 18) | 0.42 | ||
| LMS | 0.43 (0.05, 3.46) | 0.43 | ||
| MPNST | 1.43 (0.32, 6.32) | 0.637 | ||
| Other | 0.7 (0.23, 2.19) | 0.544 | ||
| FNCLCC grade of recurrent tumor | ||||
| High grade (III) vs. low to intermediate grades (I+II) | 1.74 (0.85, 3.57) | 0.131 | ||
| Tumor size of recurrent tumor | 1.01 (1, 1.02) | 0.007 | 1.01 (1, 1.02) | 0.004 |
| R2 resection of recurrent tumor: Yes vs. No | 1.79 (0.79, 4.06) | 0.163 | ||
| Variables | Univariate | |
|---|---|---|
| HR (95% CI) | p value | |
| Improving + stable group vs. worsening group | 0.71 (0.31, 1.58) | 0.398 |
| FNCLCC grade of primary tumor: ref. = 1 | ||
| 2 | 0.49 (0.19, 1.25) | 0.135 |
| 3 | 0.86 (0.38, 1.94) | 0.719 |
| Histologic subtype of primary tumor: ref. = DDLPS | ||
| WDLPS | 1.54 (0.68, 3.48) | 0.303 |
| LPS, NOS | 3.81 (0.47, 30.75) | 0.209 |
| LMS | 0.27 (0.03, 2.08) | 0.208 |
| MPNST | 1.66 (0.48, 5.76) | 0.422 |
| Other | 1.26 (0.42, 3.76) | 0.676 |
| FNCLCC grade of recurrent tumor: ref. = 1 | ||
| 2 | 2.2 (0.81, 5.93) | 0.12 |
| 3 | 3.32 (1.11, 9.94) | 0.032 |
| Tumor size of recurrent tumor | 1 (0.99, 1.01) | 0.615 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jo, S.J.; Kim, K.D.; Lim, S.H.; Kim, J.; Kim, M.J.; Park, J.B.; Lee, K.W. Analysis of the Effect of Tumor-Grade Change on the Prognosis of Retroperitoneal Sarcoma. Cancers 2022, 14, 3020. https://doi.org/10.3390/cancers14123020
Jo SJ, Kim KD, Lim SH, Kim J, Kim MJ, Park JB, Lee KW. Analysis of the Effect of Tumor-Grade Change on the Prognosis of Retroperitoneal Sarcoma. Cancers. 2022; 14(12):3020. https://doi.org/10.3390/cancers14123020
Chicago/Turabian StyleJo, Sung Jun, Kyeong Deok Kim, So Hee Lim, Jinseob Kim, Min Jung Kim, Jae Berm Park, and Kyo Won Lee. 2022. "Analysis of the Effect of Tumor-Grade Change on the Prognosis of Retroperitoneal Sarcoma" Cancers 14, no. 12: 3020. https://doi.org/10.3390/cancers14123020
APA StyleJo, S. J., Kim, K. D., Lim, S. H., Kim, J., Kim, M. J., Park, J. B., & Lee, K. W. (2022). Analysis of the Effect of Tumor-Grade Change on the Prognosis of Retroperitoneal Sarcoma. Cancers, 14(12), 3020. https://doi.org/10.3390/cancers14123020