
A Fibrosis Biomarker Early Predicts Cardiotoxicity Due to Anthracycline-Based Breast Cancer Chemotherapy

 , , ,
, , ,  , , , ,
, , , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients with BC (CUN Cohort)
2.1.1. Study Protocol
2.1.2. Study Endpoints
2.2. Patients with BC (HULAFE Cohort)
2.2.1. Study Protocol
2.2.2. Study Endpoints
2.3. Patients with ACC-Induced HF
2.4. Circulating Biomarkers
2.5. Statistical Analysis
3. Results
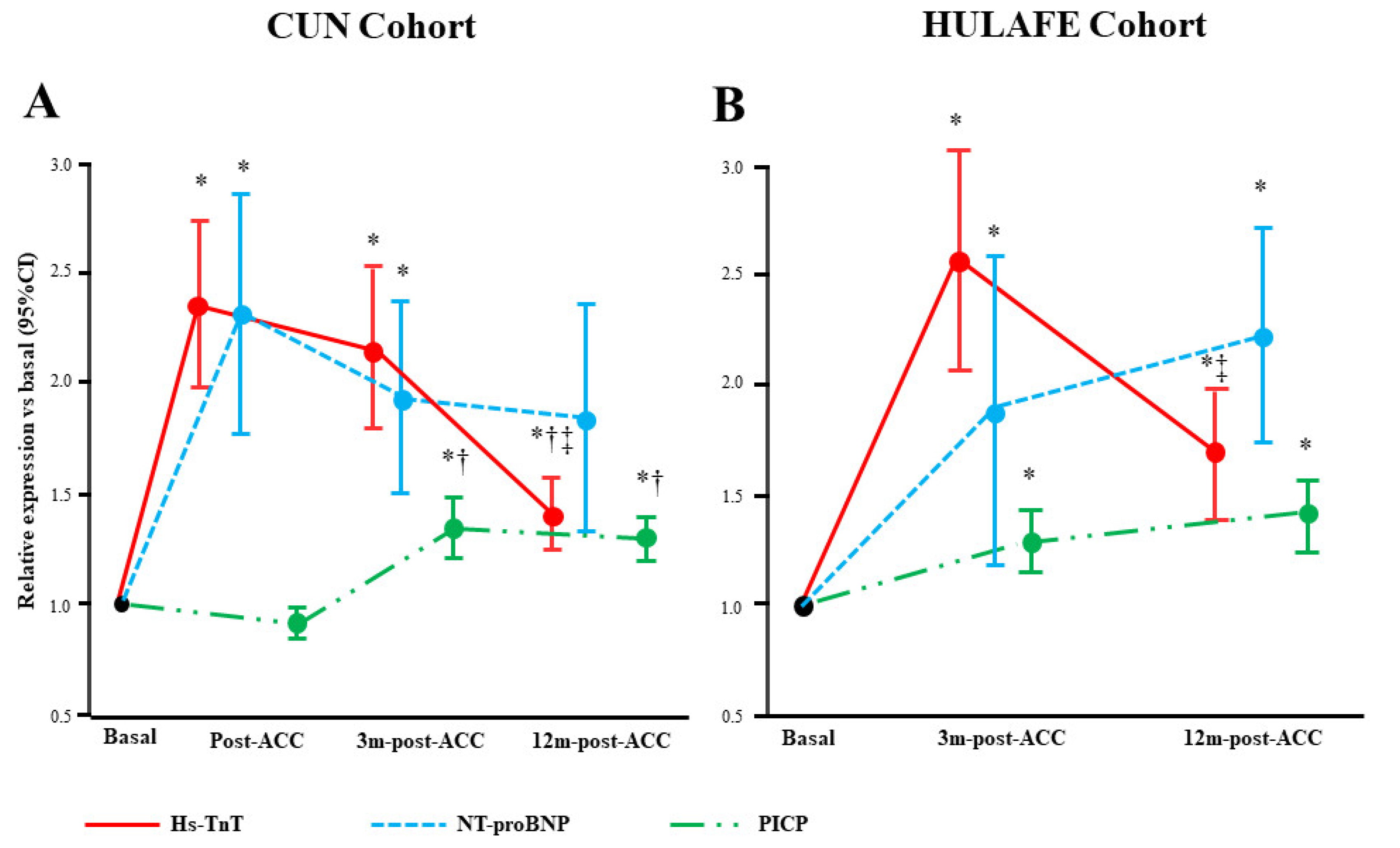
3.1. Serum Biomarkers and ACC-Induced Subclinical LVD at 3 Months-Post-ACC in BC Patients (CUN Cohort)
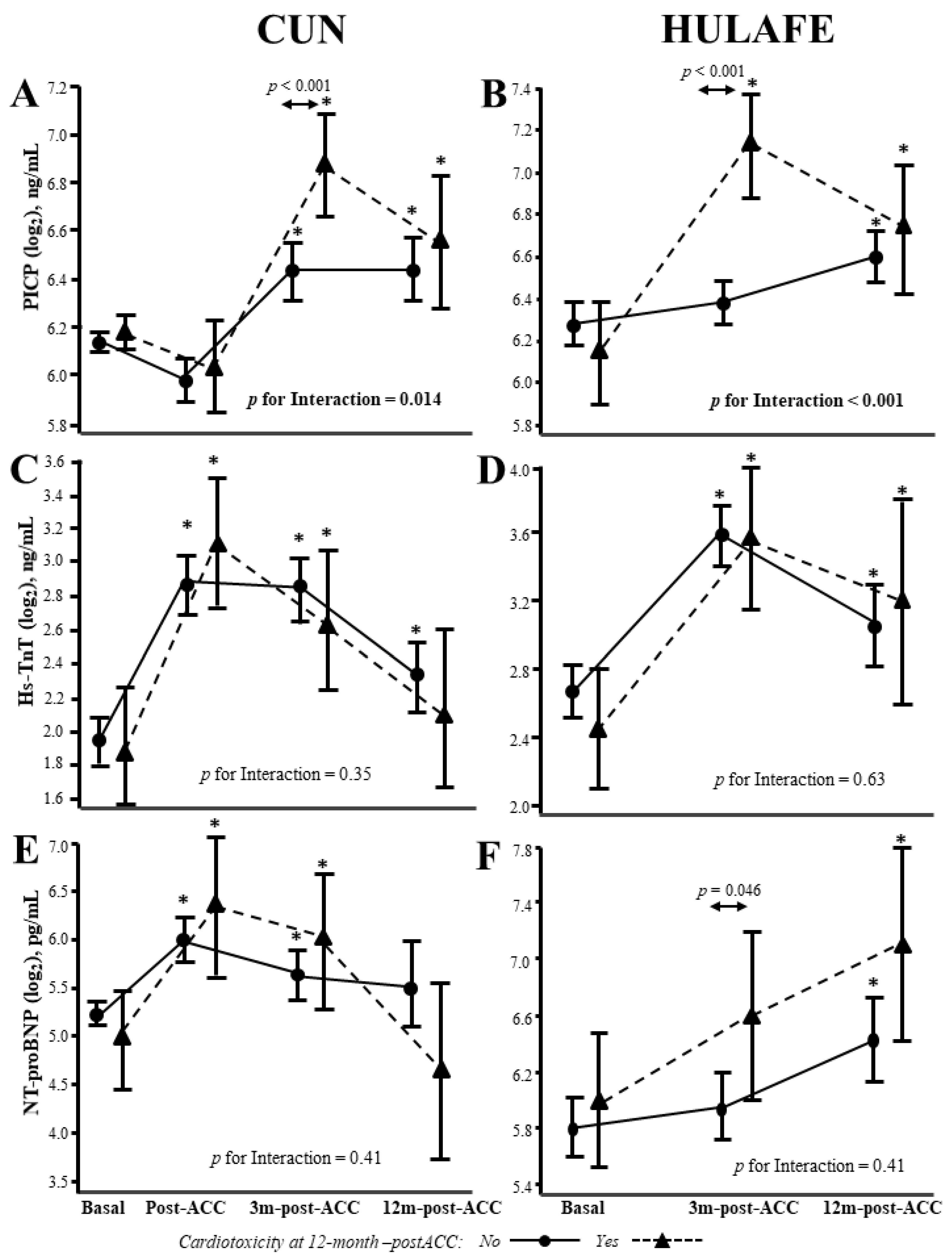
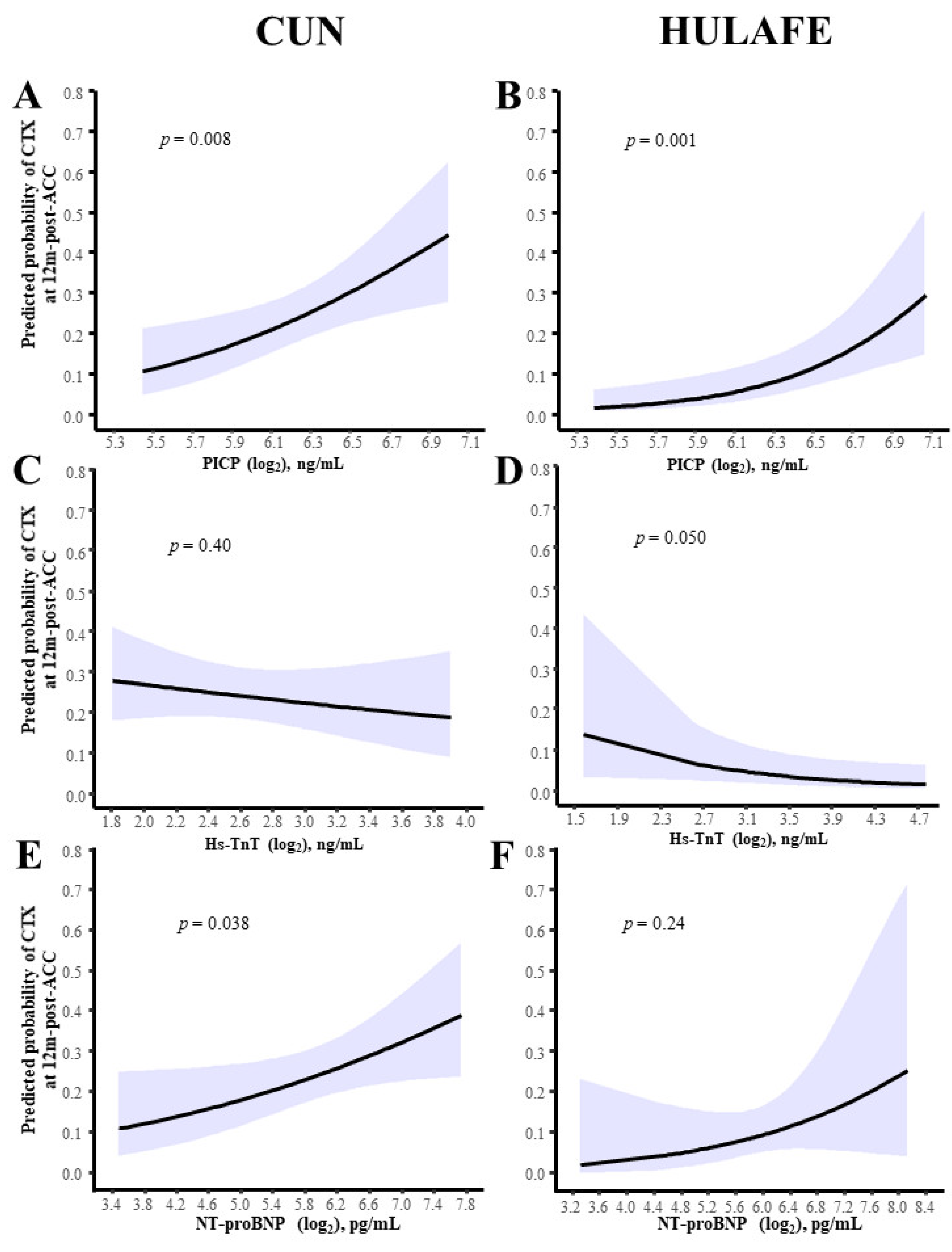
3.2. Serum Biomarkers and Prognosis of ACC-Induced Cardiotoxicity at 12 Months Post-ACC in BC Patients (CUN and HULAFE Cohorts)
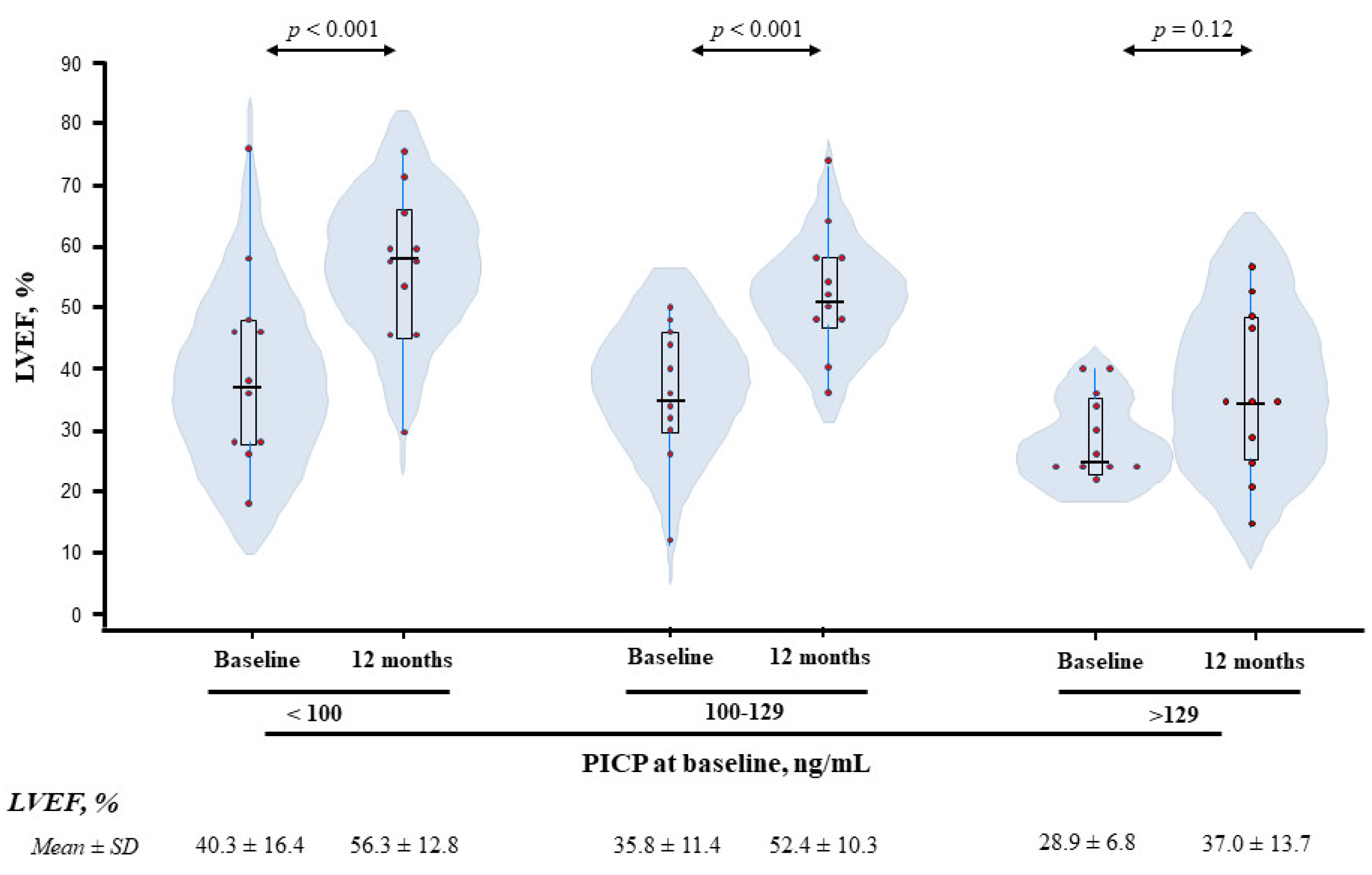
3.3. Serum Biomarkers and LVD in ACC-HF Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ramin, C.; Schaeffer, M.L.; Zheng, Z.; Connor, A.E.; Hoffman-Bolton, J.; Lau, B.; Visvanathan, K. All-Cause and Cardiovascular Disease Mortality Among Breast Cancer Survivors in CLUE II, a Long-Standing Community-Based Cohort. J. Natl. Cancer Inst. 2021, 113, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Anker, M.S.; Hadzibegovic, S.; Lena, A.; Belenkov, Y.; Bergler-Klein, J.; de Boer, R.A.; Farmakis, D.; von Haehling, S.; Iakobishvili, Z.; Maack, C.; et al. Recent advances in cardio-oncology: A report from the Heart Failure Association 2019 and World Congress on Acute Heart Failure 2019. ESC Heart Fail. 2019, 6, 1140–1148. [Google Scholar] [CrossRef] [PubMed]
- Pignatti, M.; Mantovani, F.; Bertelli, L.; Barbieri, A.; Pacchioni, L.; Loschi, P.; De Santis, G. Effects of silicone expanders and implants on echocardiographic image quality after breast reconstruction. Plast. Reconstr. Surg. 2013, 132, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Movahed, M.R. Impairment of echocardiographic acoustic window caused by breast implants. Eur. J. Echocardiogr. 2008, 9, 296–297. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Saleh, Y.; Abdelkarim, O.; Herzallah, K.; Abela, G.S. Anthracycline-induced cardiotoxicity: Mechanisms of action, incidence, risk factors, prevention, and treatment. Heart Fail. Rev. 2021, 26, 1159–1173. [Google Scholar] [CrossRef] [PubMed]
- Ananthan, K.; Lyon, A.R. The Role of Biomarkers in Cardio-Oncology. J. Cardiovasc. Transl. Res. 2020, 13, 431–450. [Google Scholar] [CrossRef]
- Meléndez, G.C.; Hundley, W.G. Is Myocardial Fibrosis a New Frontier for Discovery in Cardiotoxicity Related to the Administration of Anthracyclines? Circ. Cardiovasc. Imaging 2016, 9, e005797. [Google Scholar] [CrossRef]
- López, B.; Ravassa, S.; Moreno, M.U.; José, G.S.; Beaumont, J.; González, A.; Díez, J. Diffuse myocardial fibrosis: Mechanisms, diagnosis and therapeutic approaches. Nat. Rev. Cardiol. 2021, 18, 479–498. [Google Scholar] [CrossRef]
- López, B.; Querejeta, R.; González, A.; Larman, M.; Díez, J. Collagen cross-linking but not collagen amount associates with elevated filling pressures in hypertensive patients with stage C heart failure: Potential role of lysyl oxidase. Hypertension 2012, 60, 677–683. [Google Scholar] [CrossRef]
- Raafs, A.G.; Verdonschot, J.A.J.; Henkens, M.T.H.M.; Adriaans, B.P.; Wang, P.; Derks, K.; Abdul Hamid, M.A.; Knackstedt, C.; van Empel, V.P.M.; Díez, J.; et al. The combination of carboxy-terminal propeptide of procollagen type I blood levels and late gadolinium enhancement at cardiac magnetic resonance provides additional prognostic information in idiopathic dilated cardiomyopathy—A multilevel assessment of myocardial fibrosis in dilated cardiomyopathy. Eur J. Heart Fail. 2021, 23, 933–944. [Google Scholar] [CrossRef]
- López, B.; Ravassa, S.; González, A.; Zubillaga, E.; Bonavila, C.; Bergés, M.; Echegaray, K.; Beaumont, J.; Moreno, M.U.; San José, G.; et al. Myocardial collagen cross-linking is associated with heart failure hospitalization in patients with hypertensive heart failure. J. Am. Coll. Cardiol. 2016, 67, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Voigt, J.U.; Pedrizzetti, G.; Lysyansky, P.; Marwick, T.H.; Houle, H.; Baumann, R.; Pedri, S.; Ito, Y.; Abe, Y.; Metz, S.; et al. Definitions for a common standard for 2D speckle tracking echocardiography: Consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Čelutkienė, J.; Pudil, R.; López-Fernández, T.; Grapsa, J.; Nihoyannopoulos, P.; Bergler-Klein, J.; Cohen-Solal, A.; Farmakis, D.; Tocchetti, C.G.; von Haehling, S.; et al. Role of cardiovascular imaging in cancer patients receiving cardiotoxic therapies: A position statement on behalf of the Heart Failure Association (HFA), the European Association of Cardiovascular Imaging (EACVI) and the Cardio-Oncology Council of the European Society of Cardiology (ESC). Eur. J. Heart Fail. 2020, 22, 1504–1524. [Google Scholar] [CrossRef] [PubMed]
- Lupón, J.; Gaggin, H.K.; de Antonio, M.; Domingo, M.; Galán, A.; Zamora, E.; Vila, J.; Peñafiel, J.; Urrutia, A.; Ferrer, E.; et al. Biomarker-assist score for reverse remodeling prediction in heart failure: The ST2-R2 score. Int. J. Cardiol. 2015, 184, 337–343. [Google Scholar] [CrossRef]
- Zheng, Y.Z.; Heagerty, P.J. Partly conditional survival models for longitudinal data. Biometrics 2005, 61, 379–391. [Google Scholar] [CrossRef]
- Maziarz, M.; Heagerty, P.; Cai, T.; Zheng, Y. On longitudinal prediction with time-to-event outcome: Comparison of modeling options. Biometrics 2017, 73, 83–93. [Google Scholar] [CrossRef]
- Tan, L.L.; Lyon, A.R. Role of Biomarkers in Prediction of Cardiotoxicity During Cancer Treatment. Curr. Treat. Options Cardiovasc. Med. 2018, 20, 55. [Google Scholar] [CrossRef]
- Levis, B.E.; Binkley, P.F.; Shapiro, C.L. Cardiotoxic effects of anthracycline-based therapy: What is the evidence and what are the potential harms? Lancet Oncol. 2017, 18, e445–e456. [Google Scholar] [CrossRef]
- Gulati, G.; Heck, S.L.; Røsjø, H.; Ree, A.H.; Hoffmann, P.; Hagve, T.A.; Norseth, J.; Gravdehaug, B.; Steine, K.; Geisler, J.; et al. Neurohormonal Blockade and Circulating Cardiovascular Biomarkers During Anthracycline Therapy in Breast Cancer Patients: Results from the PRADA (Prevention of Cardiac Dysfunction During Adjuvant Breast Cancer Therapy) Study. J. Am. Heart Assoc. 2017, 6, e006513. [Google Scholar] [CrossRef]
- Giusca, S.; Korosoglou, G.; Montenbruck, M.; Geršak, B.; Schwarz, A.K.; Esch, S.; Kelle, S.; Wülfing, P.; Dent, S.; Lenihan, D.; et al. Multiparametric Early Detection and Prediction of Cardiotoxicity Using Myocardial Strain, T1 and T2 Mapping, and Biochemical Markers: A Longitudinal Cardiac Resonance Imaging Study During 2 Years of Follow-Up. Circ. Cardiovasc. Imaging 2021, 14, e012459. [Google Scholar] [CrossRef]
- Rüger, A.M.; Schneeweiss, A.; Seiler, S.; Tesch, H.; van Mackelenbergh, M.; Marmé, F.; Lübbe, K.; Sinn, B.; Karn, T.; Stickeler, E.; et al. Cardiotoxicity and Cardiovascular Biomarkers in Patients with Breast Cancer: Data From the GeparOcto-GBG 84 Trial. J. Am. Heart Assoc. 2020, 9, e018143. [Google Scholar] [CrossRef] [PubMed]
- Michel, L.; Mincu, R.I.; Mahabadi, A.A.; Settelmeier, S.; Al-Rashid, F.; Rassaf, T.; Totzeck, M. Troponins and brain natriuretic peptides for the prediction of cardiotoxicity in cancer patients: A meta-analysis. Eur. J. Heart Fail. 2020, 22, 350–361. [Google Scholar] [CrossRef] [PubMed]
- Potter, E.; Marwick, T.H. Assessment of Left Ventricular Function by Echocardiography: The Case for Routinely Adding Global Longitudinal Strain to Ejection Fraction. JACC Cardiovasc. Imaging 2018, 11, 260–274. [Google Scholar] [CrossRef] [PubMed]
- Leader, C.J.; Moharram, M.; Coffey, S.; Sammut, I.A.; Wilkins, G.W.; Walker, R.J. Myocardial global longitudinal strain: An early indicator of cardiac interstitial fibrosis modified by spironolactone, in a unique hypertensive rat model. PLoS ONE 2019, 14, e0220837. [Google Scholar] [CrossRef]
- Park, S.J.; Cho, S.W.; Kim, S.M.; Ahn, J.; Carriere, K.; Jeong, D.S.; Lee, S.C.; Park, S.W.; Choe, Y.H.; Park, P.W.; et al. Assessment of Myocardial Fibrosis Using Multimodality Imaging in Severe Aortic Stenosis: Comparison with Histologic Fibrosis. JACC Cardiovasc. Imaging 2019, 12, 109–119. [Google Scholar] [CrossRef]
- Slimani, A.; Melchior, J.; de Meester, C.; Pierard, S.; Roy, C.; Amzulescu, M.; Bouzin, C.; Maes, F.; Pasquet, A.; Pouleur, A.C.; et al. Relative Contribution of Afterload and Interstitial Fibrosis to Myocardial Function in Severe Aortic Stenosis. JACC Cardiovasc. Imaging 2020, 13, 589–600. [Google Scholar] [CrossRef]
- Fabiani, I.; Scatena, C.; Mazzanti, C.M.; Conte, L.; Pugliese, N.R.; Franceschi, S.; Lessi, F.; Menicagli, M.; De Martino, A.; Pratali, S.; et al. Micro-RNA-21 (biomarker) and global longitudinal strain (functional marker) in detection of myocardial fibrotic burden in severe aortic valve stenosis: A pilot study. J. Transl. Med. 2016, 14, 248. [Google Scholar] [CrossRef][Green Version]
- Cameli, M.; Mondillo, S.; Righini, F.M.; Lisi, M.; Dokollari, A.; Lindqvist, P.; Maccherini, M.; Henein, M. Left Ventricular Deformation and Myocardial Fibrosis in Patients with Advanced Heart Failure Requiring Transplantation. J. Card. Fail. 2016, 22, 901–907. [Google Scholar] [CrossRef]
- Ravassa, S.; López, B.; Querejeta, R.; Echegaray, K.; San José, G.; Moreno, M.U.; Beaumont, F.J.; González, A.; Díez, J. Phenotyping of myocardial fibrosis in hypertensive patients with heart failure. Influence on clinical outcome. J. Hypertens. 2017, 35, 853–861. [Google Scholar] [CrossRef]
- Cleland, J.G.F.; Ferreira, J.P.; Mariottoni, B.; Pellicori, P.; Cuthbert, J.; Verdonschot, J.A.J.; Petutschnigg, J.; Ahmed, F.Z.; Cosmi, F.; Brunner La Rocca, H.P.; et al. The effect of spironolactone on cardiovascular function and markers of fibrosis in people at increased risk of developing heart failure: The heart “OMics” in AGEing (HOMAGE) randomized clinical trial. Eur. Heart J. 2021, 42, 684–696. [Google Scholar] [CrossRef]
- Zannad, F.; Alla, F.; Dousset, B.; Perez, A.; Pitt, B. Limitation of excessive extracellular matrix turnover may contribute to survival benefit of spironolactone therapy in patients with congestive heart failure: Insights from the Randomized Aldactone Evaluation Study (RALES). Circulation 2000, 102, 2700–2706. [Google Scholar] [CrossRef] [PubMed]
- Iraqi, W.; Rossignol, P.; Angioi, M.; Fay, R.; Nuée, J.; Ketelslegers, J.M.; Vincent, J.; Pitt, B.; Zannad, F. Extracellular cardiac matrix biomarkers in patients with acute myocardial infarction complicated by left ventricular dysfunction and heart failure: Insights from the Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study (EP). Circulation 2009, 119, 2471–2479. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Clinical Characteristics | All Patients (n = 87) | Subclinical LVD | p-Value | |
|---|---|---|---|---|
| No (n = 69) | Yes (n = 18) | |||
| Age, years | 50.8 ± 11.6 | 50.7 ± 11.7 | 51.1 ± 11.7 | 0.90 |
| BMI, kg/m2 | 23.9 ± 4.5 | 23.8 ± 4.5 | 24.1 ± 4.2 | 0.81 |
| Oncologic parameters, n (%) | ||||
| Breast cancer side | ||||
| Left | 48 (55.2) | 37 (53.6) | 11 (61.1) | |
| Right | 38 (43.7) | 31 (44.9) | 7 (38.9) | 0.77 |
| Bilateral | 1 (1.1) | 1 (1.4) | 0 (0.0) | |
| Ki67, % | 40.6 ± 24.0 | 41.0 ± 25.3 | 39.1 ± 19.1 | 0.73 |
| HER2 positive, n (%) | 21 (24.1) | 17 (24.6) | 4 (22.2) | 0.83 |
| TNM Stage, n (%) | ||||
| I | 16 (18.4) | 14 (20.3) | 2 (11.1) | |
| II | 44 (50.6) | 31 (44.9) | 13 (72.2) | |
| III | 23 (26.4) | 21 (30.4) | 2 (11.1) | 0.19 |
| IV | 4 (4.6) | 3 (4.3) | 1 (5.6) | |
| Epirubicin, mg/m2 | 384 (353–396) | 390 (362–398) | 361 (274–392) | 0.06 |
| Taxanes, n (%) | ||||
| Paclitaxel | 27 (31.0) | 23 (33.3) | 4 (22.2) | 0.36 |
| Docetaxel | 60 (69.0) | 46 (66.7) | 14 (77.8) | |
| Other treatments, n (%) | ||||
| Carboplatin | 20 (23.0) | 16 (23.2) | 4 (22.2) | 0.93 |
| Anti-HER2 | ||||
| Trastuzumab | 10 (11.5) | 8 (11.6) | 2 (11.1) | 0.97 |
| Trastuzumab + Pertuzumab | 11 (12.6) | 9 (13.0) | 2 (11.1) | |
| Surgery before ACC, n (%) | 27 (31.0) | 25 (36.2) | 2 (11.1) | 0.040 |
| Radiotherapy, n (%) | 13 (14.9) | 12 (17.4) | 1 (5.6) | 0.21 |
| Cardiovascular comorbidities, n (%) | ||||
| Hypertension | 14 (16.1) | 11 (15.9) | 3 (16.7) | 0.94 |
| Obesity | 10 (11.5) | 8 (11.6) | 2 (11.1) | 0.95 |
| Dyslipidemia | 17 (19.5) | 14 (20.3) | 3 (16.7) | 0.73 |
| Diabetes Mellitus | 2 (2.3) | 1 (1.4) | 1 (5.6) | 0.37 |
| Current smoking | 7 (8.0) | 6 (8.7) | 1 (5.6) | 0.66 |
| eGFR < 60 mL/min/1.73 m2 | 2 (2.3) | 2 (2.9) | 0 (0.0) | |
| Atrial Fibrillation | 1 (1.1) | 1 (1.4) | 0 (0.0) | |
| Cardiovascular treatments, n (%) | ||||
| ACE inhibitor | 4 (4.6) | 3 (4.3) | 1 (5.6) | 0.83 |
| Angiotensin receptor blocker | 5 (5.7) | 3 (4.3) | 2 (11.1) | 0.28 |
| Beta-blockers | 2 (2.3) | 1 (1.4) | 1 (5.6) | 0.37 |
| Diuretics | 2 (2.3) | 1 (1.4) | 1 (5.6) | 0.37 |
| Lipid-lowering drug | 9 (10.3) | 8 (11.6) | 1 (5.6) | 0.68 |
| Glucose-lowering drug | 2 (2.3) | 1 (1.4) | 1 (5.6) | 0.37 |
| Liver function parameters | ||||
| AST, IU/L | 18.0 (15.0–20.0) | 18.0 (15.0–20.0) | 15.0 (13.0–18.5) | 0.05 |
| ALT, IU/L | 13.0 (11.0–18.0) | 14.0 (12.0–18.0) | 12.5 (9.3–16.8) | 0.18 |
| GGT, IU/L | 17.0 (13.0–26.0) | 18.0 (13.0–28.0) | 15.0 (12.0–18.3) | 0.13 |
| ALP, IU/L | 60.0 (50.0–72.0) | 61.0 (49.0–76.0) | 59.5 (48.8–69.3) | 0.35 |
| Echocardiographic parameters | ||||
| GLS, % | −20.6 ± 2.0 | −20.5 ± 2.0 | −21.2 ± 2.0 | 0.19 |
| LVEF (3D), % | 63.8 ± 5.3 | 63.9 ± 5.4 | 63.4 ± 5.0 | 0.70 |
| Biomarkers | ||||
| Cardiomyocyte stress/damage | ||||
| NTproBNP, pg/mL | 41.4 (24.2-64.2) | 41.1 (23.8–63.3) | 46.5 (28.2–71.8) | 0.34 |
| hs-TnT, ng/L | 3.0 (3.0-4.5) | 3.0 (3.0–4.2) | 3.0 (3.0–4.9) | 0.87 |
| Myocardial fibrosis | ||||
| PICP, ng/mL | 72.0 (59.5-86.5) | 74.4 (61.0–88.1) | 65.7 (57.6–77.9) | 0.26 |
| CITP:MMP1 ratio | 1.5 (1.2-3.0) | 1.6 (1.2–3.2) | 1.5 (1.0–2.5) | 0.17 |
| Clinical Characteristics | Univariable | Multivariable | ||
|---|---|---|---|---|
| Estimate (95%CI) | p-Value | Estimate (95%CI) | p-Value | |
| Age, years | 0.02 (−0.01 to 0.04) | 0.09 | −0.02 (−0.05 to 0.02) | 0.34 |
| BMI, kg/m2 | 0.04 (−0.02 to 0.10) | 0.15 | 0.03 (−0.03 to 0.09) | 0.34 |
| Left breast, yes/no | −0.20 (−0.69 to 0.28) | 0.41 | ||
| Ki67, % | 0.002 (−0.01 to 0.01) | 0.76 | ||
| Epirubicin cumulative dose, mg/m2 | 0.005 (0.001 to 0.01) | 0.018 | −0.004 (−0.008 to 0.001) | 0.15 |
| Paclitaxel, yes/no | −0.22 (−0.74 to 0.30) | 0.40 | ||
| Other treatments, yes/no | ||||
| Carboplatin | 0.19 (−0.38 to 0.76) | 0.50 | ||
| Anti-HER2 | −0.01 (−0.56 to 0.54) | 0.98 | ||
| Surgery before ACC | 0.03 (−0.51 to 0.56) | 0.92 | ||
| Radiotherapy | 0.09 (−0.60 to 0.78) | 0.79 | ||
| Comorbidities, yes/no | ||||
| Hypertension | 0.19 (−0.50 to 0.89) | 0.58 | ||
| Obesity | 0.05 (−0.73 to 0.84) | 0.89 | ||
| Dyslipidemia | 0.24 (−0.39 to 0.87) | 0.46 | ||
| Current smoking | −0.41 (−1.29 to 0.47) | 0.36 | ||
| Renal function parameter | ||||
| eGFR, mL/min/1.73 m2 | −0.02 (−0.03 to−0.01) | 0.006 | −0.01 (−0.03 to 0.01) | 0.32 |
| Liver function parameters (log2) | ||||
| AST, IU/L | 0.35 (−0.09 to 0.80) | 0.12 | 0.17 (−0.26 to 0.60) | 0.44 |
| ALT, IU/L | 0.16 (−0.10 to 0.42) | 0.23 | ||
| GGT, IU/L | −0.03 (−0.25 to 0.19) | 0.78 | ||
| ALP, IU/L | 0.27 (−0.20 to 0.74) | 0.27 | ||
| Biomarkers (log2) | ||||
| NT-proBNP, pg/mL | 0.29 (0.10 to 0.47) | 0.003 | 0.26 (0.06 to 0.46) | 0.010 |
| hs-TnT, ng/L | 0.25 (0.01 to 0.49) | 0.043 | 0.10 (−0.17 to 0.36) | 0.48 |
| PICP, ng/mL | 0.94 (0.51 to 1.37) | <0.001 | 0.88 (0.45 to 1.31) | <0.001 |
| CITP:MMP-1 ratio | 0.05 (−0.16 to 0.27) | 0.62 | ||
| GLS at baseline, % | 0.80 (0.68 to 0.93) | <0.001 | ||
| Baseline Clinical Characteristics | CUN Cohort | HULAFE Cohort | ||||
|---|---|---|---|---|---|---|
| Cardiotoxicity | p-Value | Cardiotoxicity | p-Value | |||
| No (n = 55) | Yes (n = 10) | No (n = 59) | Yes (n = 11) | |||
| Age, years (min-max) | 50.1 ± 11.6 | 51.3 ± 12.5 | 0.76 | 56.1 ± 12.8 | 46.8 ± 10.1 | 0.026 |
| BMI, kg/m2 | 23.2 ± 3.7 | 24.8 ± 5.0 | 0.24 | 26.5 ± 5.0 | 24.6 ± 4.6 | 0.26 |
| TNM Stage, n (%) | ||||||
| I | 12 (21.8) | 2 (20.0) | 10 (17.0) | 4 (36.4) | ||
| II | 26 (47.3) | 5 (50.0) | 0.89 | 36 (61.0) | 4 (36.4) | 0.24 |
| III | 14 (25.5) | 3 (30.0) | 13 (22.0) | 3 (27.3) | ||
| IV | 3 (5.5) | 0 (0.0) | ||||
| Oncologic treatment, n (%) | ||||||
| CUN cohort | ||||||
| Epirubicin, mg/m2 | 384 (354–397) | 375 (272–392) | 0.58 | |||
| Taxanes, n (%) | ||||||
| Docetaxel | 39 (70.9) | 10 (100) | 0.06 | |||
| Paclitaxel | 16 (29.1) | 0 (0.0) | ||||
| HULAFE cohort | ||||||
| ACC1 | 15 (25.4) | 7 (63.6) | 0.012 | |||
| ACC2 | 44 (74.6) | 4 (36.4) | ||||
| Current smoking, n (%) | 3 (5.5) | 1 (10.0) | 0.58 | 9 (15.3) | 1 (9.1) | 0.59 |
| eGFR < 60 mL/min/1.73 m2, n (%) | 1 (1.8) | 0 (0.0) | 1 (1.7) | 0 (0.0) | ||
| Cardiovascular comorbidities, n (%) | ||||||
| Hypertension | 7 (12.7) | 2 (20.0) | 0.54 | 17 (28.8) | 1 (9.1) | 0.17 |
| Obesity | 4 (7.3) | 2 (20.0) | 0.20 | 12 (20.3) | 1 (9.1) | 0.38 |
| Dyslipidemia | 7 (12.7) | 2 (20.0) | 0.54 | 13 (22.0) | 3 (27.3) | 0.70 |
| Diabetes Mellitus | 1 (1.8) | 0 (0.0) | 5 (8.5) | 2 (18.2) | 0.32 | |
| Cardiovascular treatment, n (%) | ||||||
| ACE inhibitor | 1 (1.8) | 1 (10.0) | 0.29 | 3 (5.1) | 2 (18.2) | 0.17 |
| Angiotensin receptor blocker | 3 (5.5) | 1 (10.0) | 0.50 | 9 (15.3) | 1 (9.1) | 0.59 |
| Beta-blockers | 1 (1.8) | 0 (0.0) | 5 (8.5) | 2 (18.2) | 0.32 | |
| Diuretics | 0 (0.0) | 0 (0.0) | 8 (13.6) | 1 (9.1) | 0.68 | |
| Lipid-lowering drug | 5 (9.1) | 2 (20.0) | 0.31 | 8 (13.6) | 3 (27.3) | 0.25 |
| Glucose-lowering drugs | 1 (1.8) | 0 (0.0) | 5 (8.5) | 2 (18.2) | 0.32 | |
| Echocardiographic parameters | ||||||
| GLS, % | −20.7 ± 1.9 | −20.1 ± 2.3 | 0.34 | −16.1 ± 1.9 | −17.5 ± 1.8 | 0.056 |
| LVEF (2D), % | 66.5 ± 5.9 | 68.8 ± 5.6 | 0.24 | |||
| LVEF (3D), % | 63.6 ± 4.8 | 61.7 ± 5.8 | 0.28 | |||
| Biomarkers | ||||||
| NT-proBNP, pg/mL | 38.7 (24.2–62.1) | 52.7 (9.8–90.4) | 0.98 | 60.8 (29.1–118) | 48.0 (33.6–98.7) | 0.81 |
| hs-TnT, ng/L | 3.0 (3.0–4.6) | 3.0 (3.0–4.1) | 0.49 | 7.2 (3.0–10.7) | 3.0 (3.0–7.6) | 0.14 |
| PICP, ng/mL | 66.6 (58.2–87.5) | 69.1(58.8–89.0) | 0.93 | 75.9 (59.1–107) | 60.7 (53.0–80.5) | 0.07 |
| Parameters | Difference vs Absence of Cardiotoxicity | p for Interaction | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Post-ACC | 3m-Post-ACC | 12m-Post-ACC | ||||||||
| Difference | 95% CI | p-Value | Difference | 95% CI | p-Value | Difference | 95% CI | p-Value | ||
| CUN cohort | ||||||||||
| Echocardiographic parameters | ||||||||||
| GLS, % | 0.14 | −0.87 to 1.15 | 0.79 | 0.69 | −0.62 to 2.01 | 0.30 | 1.53 | −0.22 to 3.28 | 0.09 | 0.40 |
| LVEF (3D), % | −0.25 | −3.31 to 2.82 | 0.87 | -1.83 | −5.03 to 1.37 | 0.26 | −11.2 | −15.0 to −7.38 | <0.001 | <0.001 |
| Biomarkers (log2) | ||||||||||
| Cardiomyocyte stress/damage | ||||||||||
| NTproBNP, pg/mL | 0.30 | −0.49 to 1.08 | 0.46 | 0.31 | −0.43 to 1.06 | 0.41 | −0.92 | −1.94 to 0.09 | 0.08 | 0.41 |
| hs-TnT, ng/L | 0.25 | −0.16 to 0.66 | 0.24 | -0.17 | −0.63 to 0.29 | 0.47 | −0.19 | −0.72 to 0.33 | 0.47 | 0.35 |
| Myocardial fibrosis | ||||||||||
| PICP, ng/mL | 0.06 | −0.15 to 0.27 | 0.57 | 0.44 | 0.20 to 0.68 | <0.001 * | 0.10 | −0.19 to 0.40 | 0.50 | 0.014 * |
| HULAFE cohort | ||||||||||
| Echocardiographic parameters | ||||||||||
| GLS, % | −1.17 | −2.56 to 0.21 | 0.10 | 1.28 | −0.21 to 2.77 | 0.09 | 4.08 | 1.45 to 6.70 | 0.002 | <0.001 |
| LVEF (2D), % | −1.06 | −5.00 to 2.88 | 0.60 | −2.34 | −5.83 to 1.15 | 0.19 | −11.8 | −14.6 to −9.06 | <0.001 | <0.001 |
| Biomarkers (log2) | ||||||||||
| Cardiomyocyte stress/damage | ||||||||||
| NTproBNP, pg/mL | 0.65 | 0.03-1.28 | 0.041 | 0.68 | −0.07-1.42 | 0.08 | 0.45 | |||
| hs-TnT, ng/L | −0.03 | −0.68 to 0.61 | 0.92 | 0.14 | −0.30 to 0.57 | 0.54 | 0.51 | |||
| Myocardial fibrosis | ||||||||||
| PICP, ng/mL | 0.74 | 0.47 to 1.01 | <0.001 * | 0.13 | −0.20 to 0.46 | 0.43 | <0.001 * | |||
| Biomarkers | CUN Cohort | HULAFE Cohort | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-value | OR | 95% CI | p-Value | |
| PICP | ||||||
| Model 1 | 3.42 | 1.40 to 8.60 | 0.007 * | 7.94 | 2.46 to 30.6 | 0.001 * |
| Model 2 | 3.44 | 1.38 to 8.76 | 0.008 * | 9.67 | 2.39 to 46.1 | 0.002 * |
| Model 3 | 3.49 | 1.40 to 8.90 | 0.008 * | 12.8 | 3.09 to 68.3 | 0.001 |
| Model 4 | 2.95 | 1.13 to 7.64 | 0.025 * | 8.13 | 2.03 to 41.4 | 0.006 * |
| Hs-TnT | ||||||
| Model 1 | 0.78 | 0.42 to 1.40 | 0.40 | 0.44 | 0.18 to 0.96 | 0.050 |
| NT-proBNP | ||||||
| Model 1 | 1.48 | 1.04 to 2.18 | 0.038 | 1.72 | 0.76 to 4.72 | 0.24 |
| Model 2 | 1.48 | 1.01 to 2.26 | 0.052 | |||
| Model 3 | 1.44 | 1.00 to 2.14 | 0.06 | |||
| Model 4 | 1.14 | 0.79 to 1.71 | 0.50 | |||
| Echocardiographic Parameters | CUN Cohort | HULAFE Cohort | ||||
|---|---|---|---|---|---|---|
| Estimate | 95% CI | p-Value | Estimate | 95% CI | p-Value | |
| GLS | ||||||
| Discrimination improvement | ||||||
| ROC analyses | ||||||
| AUCGLS | 0.600 | 0.4860.715 | 0.08 | 0.754 | 0.6450.862 | <0.001 |
| AUCGLS + PICP | 0.679 | 0.5680.789 | 0.002 | 0.804 | 0.7070.901 | <0.001 |
| ΔAUC | 0.079 | 0.0080.149 | 0.030 | 0.050 | 0.0190.080 | 0.002 |
| Reclassification improvement | ||||||
| IDI | 0.072 | 0.020–0.125 | 0.007 | 0.067 | 0.022–0.112 | 0.004 |
| Continuous NRI | ||||||
| Events | 0.121 | −0.220–0.453 | 0.49 | 0.364 | 0.018–0.646 | 0.023 |
| Non-events | 0.259 | 0.123–0.453 | <0.001 | 0.220 | 0.104–0.347 | <0.001 |
| All | 0.380 | 0.022–0.735 | 0.036 | 0.584 | 0.242–0.886 | <0.001 |
| LVEF * | ||||||
| Discrimination improvement | ||||||
| ROC analyses | ||||||
| AUCLVEF | 0.624 | 0.514–0.734 | 0.028 | 0.530 | 0.402–0.659 | 0.64 |
| AUCLVEF + PICP | 0.683 | 0.579–0.787 | <0.001 | 0.663 | 0.535–0.793 | 0.013 |
| ΔAUC | 0.059 | 0.006–0.112 | 0.029 | 0.133 | 0.008–0.259 | 0.037 |
| Reclassification improvement | ||||||
| IDI | 0.077 | 0.025–0.129 | 0.003 | 0.121 | 0.044–0.198 | 0.002 |
| Continuous NRI | ||||||
| Events | 0.152 | −0.159–0.472 | 0.35 | 0.182 | −0.250–0.579 | 0.40 |
| Non-events | 0.346 | 0.203–0.482 | <0.001 | 0.229 | 0.042–0.396 | 0.011 |
| All | 0.497 | 0.148–0.849 | 0.005 | 0.411 | −0.043–0.831 | 0.065 |
| Baseline Clinical Characteristics | PICP Tertiles, ng/mL | p for Trend | ||
|---|---|---|---|---|
| 1st (n = 11) | 2nd (n = 11) | 3rd (n = 11) | ||
| PICP, ng/mL | <100 | 100–129 | >129 | |
| Age, years | 61.5 ± 12.6 | 59.4 ± 11.5 | 60.6 ± 11.1 | 0.87 |
| Female gender, n (%) | 10 (90.9) | 10 (90.9) | 7 (63.6) | 0.10 |
| BMI, kg/m2 | 28.9 ± 6.1 | 26.7 ± 4.8 | 28.3 ± 5.0 | 0.80 |
| Sodium, mmol/L | 139 ± 2.4 | 139 ± 2.4 | 138 ± 3.3 | 0.13 |
| Potassium, mmol/L | 4.1 ± 0.4 | 4.1 ± 0.7 | 4.2 ± 0.5 | 0.61 |
| Hemoglobin, g/dL | 12.5 ± 0.9 | 12.6 ± 1.9 | 12.6 ± 1.8 | 0.89 |
| eGFR, mL/min/1.73 m2 | 69.2 ± 26.4 | 73.0 ± 36.8 | 59.9 ± 30.8 | 0.49 |
| NYHA Class, n (%) | ||||
| III-IV | 3 (27.3) | 1 (9.1) | 6 (54.5) | 0.17 |
| HF duration, months | 2.0 (1.0–24.0) | 1.0 (1.0–4.0) | 8.0 (1.0–84.0) | 0.20 |
| ≥2 previous hospitalizations, n (%) | 1 (9.1) | 1 (9.1) | 1 (9.1) | >0.99 |
| Comorbidities, n (%) | ||||
| Ischemic heart disease | 0 (0.0) | 0 (0.0) | 1 (9.1) | |
| Diabetes mellitus | 3 (27.3) | 3 (27.3) | 4 (36.4) | 0.65 |
| Hypertension | 8 (72.7) | 2 (18.2) | 2 (18.2) | 0.009 |
| Atrial fibrillation | 0 (0.0) | 0 (0.0) | 1 (9.1) | |
| Hypercholesterolemia | 3 (27.3) | 5 (45.5) | 5 (45.5) | 0.39 |
| Treatments, n (%) | ||||
| ACEIs/ARBs | 9 (81.8) | 11 (100) | 10 (90.9) | 0.47 |
| Beta-Blockers | 11 (100) | 9 (81.8) | 11 (100) | >0.99 |
| Diuretics | 7 (63.6) | 8 (72.7) | 10 (90.9) | 0.14 |
| MRA | 6 (54.5) | 6 (54.5) | 11 (100) | 0.022 |
| Digoxin | 1 (9.1) | 1 (9.1) | 6 (54.5) | 0.014 |
| Statins | 7 (63.6) | 5 (45.5) | 7 (63.6) | 0.80 |
| LVEF, % | 40.3 ± 16.4 | 35.8 ± 11.4 | 28.9 ± 6.8 | 0.034 |
| NT-proBNP, pg/mL | 1563 (396–2167) | 1510 (346–4990) | 1726 (960–7300) | 0.08 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de la Fuente, A.; Santisteban, M.; Lupón, J.; Aramendía, J.M.; Díaz, A.; Santaballa, A.; Hernándiz, A.; Sepúlveda, P.; Cediel, G.; López, B.; et al. A Fibrosis Biomarker Early Predicts Cardiotoxicity Due to Anthracycline-Based Breast Cancer Chemotherapy. Cancers 2022, 14, 2941. https://doi.org/10.3390/cancers14122941
de la Fuente A, Santisteban M, Lupón J, Aramendía JM, Díaz A, Santaballa A, Hernándiz A, Sepúlveda P, Cediel G, López B, et al. A Fibrosis Biomarker Early Predicts Cardiotoxicity Due to Anthracycline-Based Breast Cancer Chemotherapy. Cancers. 2022; 14(12):2941. https://doi.org/10.3390/cancers14122941
Chicago/Turabian Stylede la Fuente, Ana, Marta Santisteban, Josep Lupón, José Manuel Aramendía, Agnes Díaz, Ana Santaballa, Amparo Hernándiz, Pilar Sepúlveda, Germán Cediel, Begoña López, and et al. 2022. "A Fibrosis Biomarker Early Predicts Cardiotoxicity Due to Anthracycline-Based Breast Cancer Chemotherapy" Cancers 14, no. 12: 2941. https://doi.org/10.3390/cancers14122941
APA Stylede la Fuente, A., Santisteban, M., Lupón, J., Aramendía, J. M., Díaz, A., Santaballa, A., Hernándiz, A., Sepúlveda, P., Cediel, G., López, B., Picazo, J. M. L., Mazo, M. M., Rábago, G., Gavira, J. J., García-Bolao, I., Díez, J., González, A., Bayés-Genís, A., & Ravassa, S. (2022). A Fibrosis Biomarker Early Predicts Cardiotoxicity Due to Anthracycline-Based Breast Cancer Chemotherapy. Cancers, 14(12), 2941. https://doi.org/10.3390/cancers14122941