
Medium to Long-Term Clinical Outcomes of Spinal Metastasectomy

 ,
, 
 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
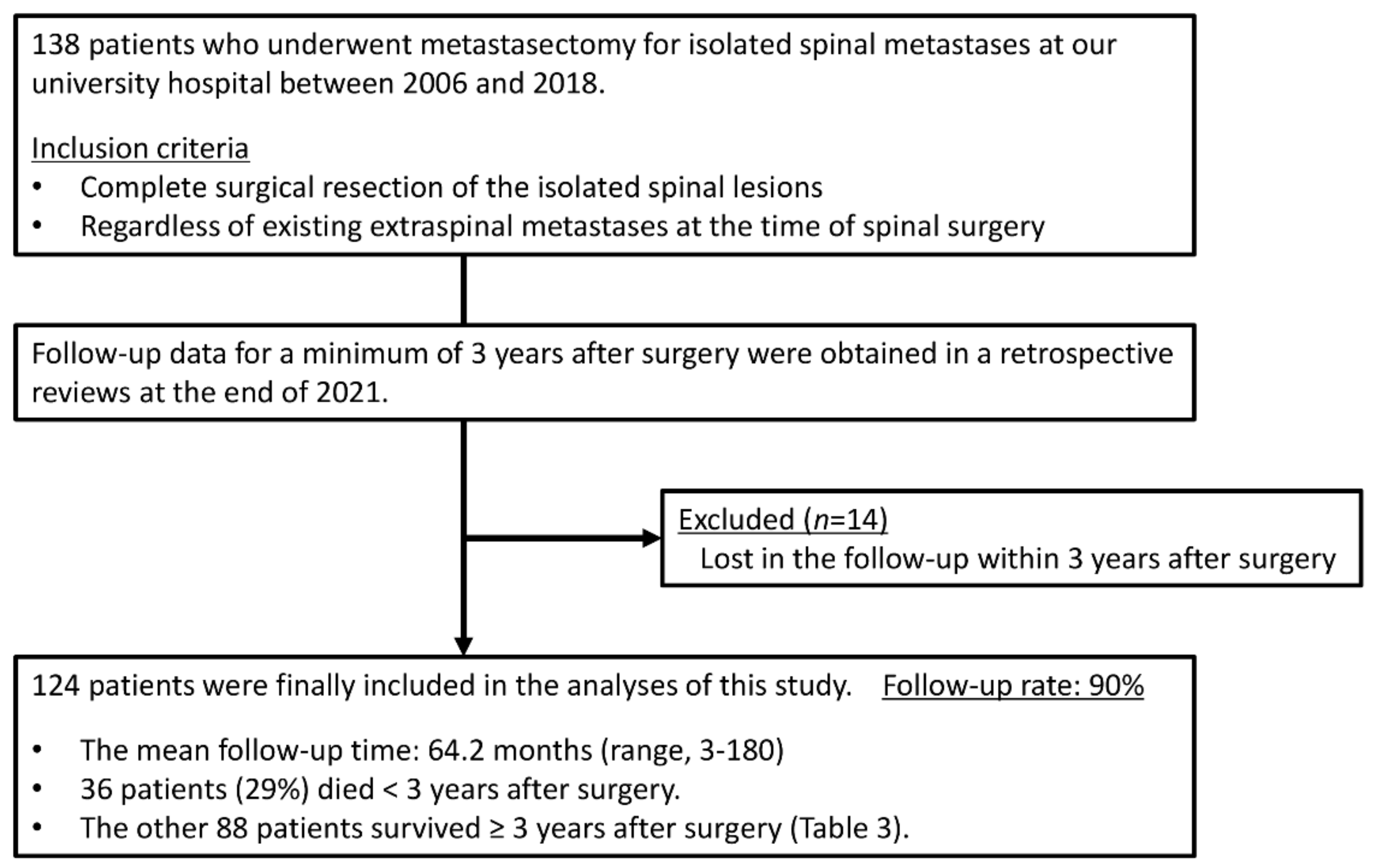
2.1. Patient Selection
2.2. Features Studied
2.3. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aaron, A.D. The management of cancer metastatic to bone. JAMA 1994, 272, 1206–1209. [Google Scholar] [CrossRef]
- Desforges, J.F.; Byrne, T.N. Spinal Cord Compression from Epidural Metastases. N. Engl. J. Med. 1992, 327, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Bilsky, M.H.; Lis, E.; Raizer, J.; Lee, H.; Boland, P. The Diagnosis and Treatment of Metastatic Spinal Tumor. Oncologist 1999, 4, 459–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klimo, P., Jr.; Schmidt, M.H. Surgical management of spinal metastases. Oncologist 2004, 9, 188–196. [Google Scholar] [CrossRef]
- Cetin, K.; Christiansen, C.F.; Jacobsen, J.B.; Nørgaard, M.; Sørensen, H.T. Bone metastasis, skeletal-related events, and mortality in lung cancer patients: A Danish population-based cohort study. Lung Cancer 2014, 86, 247–254. [Google Scholar] [CrossRef]
- Farooki, A.; Leung, V.; Tala, H.; Tuttle, R.M. Skeletal-Related Events due to Bone Metastases from Differentiated Thyroid Cancer. J. Clin. Endocrinol. Metab. 2012, 97, 2433–2439. [Google Scholar] [CrossRef] [PubMed]
- Laufer, I.; Bilsky, M.H. Advances in the treatment of metastatic spine tumors: The future is not what it used to be. J. Neurosurg. Spine 2019, 30, 299–307. [Google Scholar] [CrossRef]
- Kato, S.; Demura, S.; Shinmura, K.; Yokogawa, N.; Shimizu, T.; Murakami, H.; Kawahara, N.; Tomita, K.; Tsuchiya, H. Surgical Metastasectomy in the Spine: A Review Article. Oncologist 2021, 26, e1833–e1843. [Google Scholar] [CrossRef] [PubMed]
- Wood, T.J.; Racano, A.; Yeung, H.; Farrokhyar, F.; Ghert, M.; Deheshi, B.M. Surgical management of bone metastases: Quality of evidence and systematic review. Ann. Surg. Oncol. 2014, 21, 4081–4089. [Google Scholar] [CrossRef] [PubMed]
- Laufer, I.; Rubin, D.G.; Lis, E.; Cox, B.W.; Stubblefield, M.D.; Yamada, Y.; Bilsky, M.H. The NOMS Framework: Approach to the Treatment of Spinal Metastatic Tumors. Oncologist 2013, 18, 744–751. [Google Scholar] [CrossRef] [Green Version]
- Stener, B. Total spondylectomy in chondrosarcoma arising from the seventh thoracic vertebra. J. Bone Jt. Surg. Br. 1971, 53, 288–295. [Google Scholar] [CrossRef]
- Tomita, K.; Kawaahra, N.; Baba, H.; Tsuchiya, H.; Nagata, S.; Toribatake, Y. Total en bloc spondylectomy for spondylectomy for solitary spinal metastasis. Int. Orthop. 1994, 18, 291–298. [Google Scholar] [CrossRef]
- Demura, S.; Kato, S.; Shinmura, K.; Yokogawa, N.; Shimizu, T.; Handa, M.; Annen, R.; Kobayashi, M.; Yamada, Y.; Murakami, H.; et al. Perioperative complications of total en bloc spondylectomy for spinal tumours. Bone Jt. J. 2021, 103-B, 976–983. [Google Scholar] [CrossRef]
- Lee, B.H.; Park, J.-O.; Kim, H.S.; Park, Y.-C.; Lee, H.-M.; Moon, S.-H. Perioperative complication and surgical outcome in patients with spine metastases: Retrospective 200-case series in a single institute. Clin. Neurol. Neurosurg. 2014, 122, 80–86. [Google Scholar] [CrossRef]
- Roser, S.; Maharaj, M.M.; Taylor, M.A.; Kuru, R.; Hansen, M.A.; Ferch, R. Vertebrectomy in metastatic spinal tumours: A 10 year, single-centre review of outcomes and survival. J. Clin. Neurosci. 2019, 68, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Zhou, R.P.; Mummaneni, P.V.; Chen, K.-Y.; Lau, D.; Cao, K.; Amara, D.; Zhang, C.; Dhall, S.; Chou, D. Outcomes of Posterior Thoracic Corpectomies for Metastatic Spine Tumors: An Analysis of 90 Patients. World Neurosurg. 2019, 123, e371–e378. [Google Scholar] [CrossRef]
- Tomita, K.; Kawahara, N.; Murakami, H.; Demura, S. Total en bloc spondylectomy for spinal tumors: Improvement of the technique and its associated basic background. J. Orthop. Sci. 2006, 11, 3–12. [Google Scholar] [CrossRef] [Green Version]
- Kawahara, N.; Tomita, K.; Murakami, H.; Demura, S. Total en bloc spondylectomy for spinal tumors: Surgical techniques and related basic background. Orthop. Clin. N. Am. 2009, 40, 47–63. [Google Scholar] [CrossRef]
- Kato, S.; Murakami, H.; Demura, S.; Yoshioka, K.; Kawahara, N.; Tomita, K.; Tsuchiya, H. More Than 10-Year Follow-Up After Total En Bloc Spondylectomy for Spinal Tumors. Ann. Surg. Oncol. 2014, 21, 1330–1336. [Google Scholar] [CrossRef]
- Murakami, H.; Kawahara, N.; Demura, S.; Kato, S.; Yoshioka, K.; Tomita, K. Total en bloc spondylectomy for lung cancer metastasis to the spine. J. Neurosurg. Spine 2010, 13, 414–417. [Google Scholar] [CrossRef] [PubMed]
- Demura, S.; Kawahara, N.; Murakami, H.; Abdel-Wanis, M.E.; Kato, S.; Yoshioka, K.; Tomita, K.; Tsuchiya, H. Total en bloc spondylectomy for spinal metastases in thyroid carcinoma. J. Neurosurg. Spine 2011, 14, 172–176. [Google Scholar] [CrossRef]
- Kato, S.; Demura, S.; Murakami, H.; Yoshioka, K.; Shinmura, K.; Yokogawa, N.; Shimizu, T.; Kawahara, N.; Tsuchiya, H. Clinical outcomes and prognostic factors following the surgical resection of renal cell carcinoma spinal metastases. Cancer Sci. 2021, 112, 2416–2425. [Google Scholar] [CrossRef]
- Kato, S.; Demura, S.; Shinmura, K.; Yokogawa, N.; Yonezawa, N.; Shimizu, T.; Oku, N.; Kitagawa, R.; Murakami, H.; Kawahara, N.; et al. Clinical outcomes and survivals after total en bloc spondylectomy for metastatic leiomyosarcoma in the spine. Eur. Spine J. 2020, 29, 3237–3244. [Google Scholar] [CrossRef]
- Jia, Q.; Yin, H.; Yang, J.; Wu, Z.; Yan, W.; Zhou, W.; Yang, X.; Xiao, J. Treatment and outcome of metastatic paraganglioma of the spine. Eur. Spine J. 2018, 27, 859–867. [Google Scholar] [CrossRef]
- Jiang, L.; Ouyang, H.; Liu, X.; Wei, F.; Wu, F.; Dang, L.; Liu, Z. Surgical treatment of 21 patients with spinal metastases of differentiated thyroid cancer. Chin. Med. J. 2014, 127, 4092–4096. [Google Scholar]
- Ohashi, M.; Hirano, T.; Watanabe, K.; Hasegawa, K.; Ito, T.; Katsumi, K.; Shoji, H.; Mizouchi, T.; Takahashi, I.; Homma, T.; et al. En Bloc Spondylectomy for Spinal Metastases: Detailed Oncological Outcomes at a Minimum of 2 Years after Surgery. Asian Spine J. 2019, 13, 296–304. [Google Scholar] [CrossRef]
- Yang, S.-Z.; Zhang, Y.; Chen, W.-G.; Sun, J.; Qiu, H.; Niu, X.-J.; Chu, T.-W. Single-stage posterior total en bloc spondylectomy in the treatment of lumbar spinal metastases. Clin. Neurol. Neurosurg. 2020, 191, 105645. [Google Scholar] [CrossRef]
- Tokuhashi, Y.; Matsuzaki, H.; Oda, H.; Oshima, M.; Ryu, J. A Revised Scoring System for Preoperative Evaluation of Metastatic Spine Tumor Prognosis. Spine 2005, 30, 2186–2191. [Google Scholar] [CrossRef]
- Tomita, K.; Kawahara, N.; Kobayashi, T.; Yoshida, A.; Murakami, H.; Akamaru, T. Surgical Strategy for Spinal Metastases. Spine 2001, 26, 298–306. [Google Scholar] [CrossRef]
- Rothrock, R.; Pennington, Z.; Ehresman, J.; Bilsky, M.H.; Barzilai, O.; Szerlip, N.J.; Sciubba, D.M. Hybrid Therapy for Spinal Metastases. Neurosurg. Clin. N. Am. 2020, 31, 191–200. [Google Scholar] [CrossRef]
- Bartlett, E.K.; Simmons, K.D.; Wachtel, H.; Roses, R.E.; Fraker, D.L.; Kelz, R.R.; Karakousis, G.C. The rise in metastasectomy across cancer types over the past decade. Cancer 2015, 121, 747–757. [Google Scholar] [CrossRef]
- Bello, D.M.; Panageas, K.S.; Hollmann, T.; Shoushtari, A.N.; Momtaz, P.; Chapman, P.B.; Postow, M.A.; Callahan, M.K.; Wolchok, J.D.; Brady, M.S.; et al. Survival Outcomes After Metastasectomy in Melanoma Patients Categorized by Response to Checkpoint Blockade. Ann. Surg. Oncol. 2020, 27, 1180–1188. [Google Scholar] [CrossRef]
- Zong, Z.; Zhou, T.-C.; Tang, F.-X.; Tian, H.-K.; Wang, A.; Yi, C.-H. Impact of Site-Specific Metastases on Surgical Value and Survival among Metastatic Colorectal Cancer Patients. Am. Surg. 2020, 86, 220–227. [Google Scholar] [CrossRef]
- Lyon, T.D.; Thompson, R.H.; Shah, P.H.; Lohse, C.M.; Boorjian, S.A.; Costello, B.A.; Cheville, J.C.; Leibovich, B.C. Complete Surgical Metastasectomy of Renal Cell Carcinoma in the Post-Cytokine Era. J. Urol. 2020, 203, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Brouquet, A.; Abdalla, E.K.; Kopetz, S.; Garrett, C.R.; Overman, M.J.; Eng, C.; Andreou, A.; Loyer, E.M.; Madoff, D.C.; Curley, S.A.; et al. High survival rate after two-stage resection of advanced colorectal liver metastases: Response-based selection and complete resection define outcome. J. Clin. Oncol. 2011, 29, 1083–1090. [Google Scholar] [CrossRef] [Green Version]
- Farazdaghi, A.; Vaughn, D.J.; Singhal, S. Pulmonary Metastasectomy for Germ Cell Tumors. Ann. Thorac. Cardiovasc. Surg. 2019, 25, 289–295. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, M.; Iwata, T.; Ando, S.; Iida, T.; Nakajima, T.; Ishii, T.; Yonemoto, T.; Tatezaki, S.; Fujisawa, T.; Kimura, H. Predictors of long-term survival with pulmonary metastasectomy for osteosarcomas and soft tissue sarcomas. J. Cardiovasc. Surg. 2006, 47, 603–608. [Google Scholar]
- Lin, A.Y.; Kotova, S.; Yanagawa, J.; Elbuluk, O.; Wang, G.; Kar, N.; Elashoff, D.; Grogan, T.; Cameron, R.B.; Singh, A.; et al. Risk stratification of patients undergoing pulmonary metastasectomy for soft tissue and bone sarcomas. J. Thorac. Cardiovasc. Surg. 2015, 149, 85–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, F.P.-Y.; Alam, N.Z.; Wright, G.M. The Past, Present and Future of Pulmonary Metastasectomy: A Review Article. Ann. Thorac. Cardiovasc. Surg. 2019, 25, 129–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toyoda, Y.; Shinohara, N.; Harabayashi, T.; Abe, T.; Akino, T.; Sazawa, A.; Nonomura, K. Survival and prognostic classification of patients with metastatic renal cell carcinoma of bone. Eur. Urol. 2007, 52, 163–168. [Google Scholar] [CrossRef]
- Liu, A.; Sankey, E.W.; Goodwin, C.R.; Kosztowski, T.A.; Elder, B.D.; Bydon, A.; Witham, T.F.; Wolinsky, J.-P.; Gokaslan, Z.L.; Sciubba, D.M. Postoperative survival and functional outcomes for patients with metastatic gynecological cancer to the spine: Case series and review of the literature. J. Neurosurg. Spine 2016, 24, 131–144. [Google Scholar] [CrossRef] [Green Version]
- Motzer, R.J.; Jonasch, E.; Agarwal, N.; Bhayani, S.; Bro, W.P.; Chang, S.S.; Choueiri, T.K.; Costello, B.A.; Derweesh, I.H.; Fishman, M.; et al. Kidney Cancer, Version 2.2017, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2017, 15, 804–834. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. American Thyroid Association Management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The AMERICAN Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Cann, T.; Cornillie, J.; Wozniak, A.; Debiec-Rychter, M.; Sciot, R.; Hompes, D.; Vergote, I.; Schöffski, P. Retrospective Analysis of Outcome of Patients with Metastatic Leiomyosarcoma in a Tertiary Referral Center. Oncol. Res. Treat. 2018, 41, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Kato, S.; Murakami, H.; Demura, S.; Yoshioka, K.; Yokogawa, N.; Yonezawa, N.; Shimizu, T.; Oku, N.; Kitagawa, R.; Tsuchiya, H. Kidney and Thyroid Cancer-Specific Treatment Algorithm for Spinal Metastases: A Validation Study. World Neurosurg. 2019, 122, e1305–e1311. [Google Scholar] [CrossRef]
- Couñago, F.; Luna, J.; Guerrero, L.L.; Vaquero, B.; Guillén-Sacoto, M.C.; González-Merino, T.; Taboada, B.; Díaz, V.; Rubio-Viqueira, B.; Díaz-Gavela, A.A.; et al. Management of oligometastatic non-small cell lung cancer patients: Current controversies and future directions. World J. Clin. Oncol. 2019, 10, 318–339. [Google Scholar] [CrossRef]
- Majem, M.; Juan, O.; Insa, A.; Reguart, N.; Trigo, J.M.; Carcereny, E.; García-Campelo, R.; García, Y.; Guirado, M.; Provencio, M. SEOM clinical guidelines for the treatment of non-small cell lung cancer (2018). Clin. Transl. Oncol. 2019, 21, 3–17. [Google Scholar] [CrossRef] [Green Version]
- Planchard, D.; Popat, S.; Kerr, K.; Novello, S.; Smit, E.F.; Faivre-Finn, C.; Mok, T.S.; Reck, M.; van Schil, P.E.; Hellmann, M.D.; et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019, 30, 863–870. [Google Scholar] [CrossRef]
- He, M.; Lovell, J.; Ng, B.L.; Spillane, J.; Speakman, D.; Henderson, M.A.; Shackleton, M.; Gyorki, D.E. Post-operative survival following metastasectomy for patients receiving BRAF inhibitor therapy is associated with duration of pre-operative treatment and elective indication. J. Surg. Oncol. 2015, 111, 980–984. [Google Scholar] [CrossRef]
- Mehta, N.; Zavitsanos, P.J.; Moldovan, K.; Oyelese, A.; Fridley, J.S.; Gokaslan, Z.; Kinsella, T.J.; Hepel, J.T. Local failure and vertebral body fracture risk using multifraction stereotactic body radiation therapy for spine metastases. Adv. Radiat. Oncol. 2018, 3, 245–251. [Google Scholar] [CrossRef] [Green Version]
- Ito, K.; Ogawa, H.; Shimizuguchi, T.; Nihei, K.; Furuya, T.; Tanaka, H.; Karasawa, K. Stereotactic Body Radiotherapy for Spinal Metastases: Clinical Experience in 134 Cases From a Single Japanese Institution. Technol. Cancer Res. Treat. 2018, 17, 1533033818806472. [Google Scholar] [CrossRef]
- Tseng, C.-L.; Soliman, H.; Myrehaug, S.; Lee, Y.; Ruschin, M.; Atenafu, E.; Campbell, M.; Maralani, P.J.; Yang, V.; Yee, A.; et al. Imaging-Based Outcomes for 24 Gy in 2 Daily Fractions for Patients with de Novo Spinal Metastases Treated With Spine Stereotactic Body Radiation Therapy (SBRT). Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 499–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bishop, A.J.; Tao, R.; Rebueno, N.C.; Christensen, E.N.; Allen, P.K.; Wang, X.A.; Amini, B.; Tannir, N.M.; Tatsui, C.E.; Rhines, L.D. Outcomes for spine stereotactic body radiation therapy and an analysis of predictors of local recurrence. Int. J. Radiat. Oncol. Biol. Phys. 2015, 92, 1016–1026. [Google Scholar] [CrossRef]
- Guckenberger, M.; Mantel, F.; Gerszten, P.C.; Flickinger, J.C.; Sahgal, A.; Létourneau, D.; Grills, I.S.; Jawad, M.; Fahim, D.K.; Shin, J.H.; et al. Safety and efficacy of stereotactic body radiotherapy as primary treatment for vertebral metastases: A multi-institutional analysis. Radiat. Oncol. 2014, 9, 226. [Google Scholar] [CrossRef] [Green Version]
- Matsumoto, M.; Watanabe, K.; Tsuji, T.; Ishii, K.; Nakamura, M.; Chiba, K.; Toyama, Y. Late instrumentation failure after total en bloc spondylectomy. J. Neurosurg. Spine 2011, 15, 320–327. [Google Scholar] [CrossRef]
- Park, S.-J.; Lee, C.-S.; Chang, B.-S.; Kim, Y.-H.; Kim, H.; Kim, S.-I.; Chang, S.-Y. Rod fracture and related factors after total en bloc spondylectomy. Spine J. 2019, 19, 1613–1619. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Wei, F.; Liu, X.; Liu, X.; Jiang, L.; Yu, M.; Xu, N.; Wu, F.; Dang, L.; Zhou, H.; et al. Risk factors for instrumentation failure after total en bloc spondylectomy of thoracic and lumbar spine tumors using titanium mesh cage for anterior reconstruction. World Neurosurg. 2020, 135, e106–e115. [Google Scholar] [CrossRef] [PubMed]
- Shinmura, K.; Kato, S.; Demura, S.; Yokogawa, N.; Yonezawa, N.; Shimizu, T.; Oku, N.; Kitagawa, R.; Handa, M.; Annen, R.; et al. Revision surgery for instrumentation failure after total en bloc spondylectomy: A retrospective case series. BMC Musculoskelet. Disord. 2020, 21, 591. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | Total | Kidney | Thyroid | Low-Grade Sarcoma | Lung | Breast | p |
|---|---|---|---|---|---|---|---|
| Number of patients | 124 | 51 | 14 | 13 | 13 | 12 | - |
| Age (year), mean (SD) | 56.7 (10.7) | 59.2 (9.1) | 57.4 (9.5) | 51.5 (11.4) | 57.2 (8.2) | 56.8 (10.2) | - |
| Sex, female, n (%) | 51 (41.1) | 9 (17.6) | 12 (85.7) | 5 (38.5) | 7 (53.8) | 12 (100) | <0.05 |
| Level of metastatic lesion, n (%) | 0.48 | ||||||
| Thoracic | 82 (66.1) | 28 (54.9) | 11 (78.6) | 9 (69.2) | 9 (69.2) | 8 (66.7) | |
| Lumbar | 42 (33.9) | 23 (45.1) | 3 (21.4) | 4 (30.8) | 4 (30.8) | 4 (33.3) | |
| Preoperative ECOG PS, n (%) | 0.93 | ||||||
| 0–1 | 89 (71.8) | 35 (68.6) | 11 (78.6) | 9 (69.2) | 10 (76.9) | 9 (75.0) | |
| 2–3 | 35 (28.2) | 16 (31.4) | 3 (21.4) | 4 (30.8) | 3 (23.1) | 3 (25.0) | |
| Distinct metastatic sites, n (%) | 0.16 | ||||||
| One (only the spine) | 56 (45.2) | 16 (31.4) | 5 (35.7) | 6 (46.2) | 9 (69.2) | 5 (41.7) | |
| Two or more | 68 (54.8) | 35 (68.6) | 9 (64.3) | 7 (53.8) | 4 (30.8) | 7 (58.3) | |
| Location of other metastases, n (%) | |||||||
| Lung | 29 (23.4) | 15 (29.4) | 6 (42.9) | 4 (30.8) | 2 (15.4) | 0 (0) | 0.11 |
| Nonspinal bone | 32 (25.8) | 17 (33.3) | 4 (28.6) | 1 (7.7) | 1 (7.7) | 6 (50.0) | 0.06 |
| Lymph node | 13 (10.5) | 8 (15.7) | 0 (0) | 2 (15.4) | 1 (7.7) | 2 (16.7) | 0.56 |
| Other locations | 9 (7.3) | 8 (15.7) | 0 (0) | 1 (7.7) | 0 (0) | 0 (0) | 0.14 |
| Revised Tokuhashi score, mean (SD) | 11.5 (1.8) | 11.6 (1.3) #,¶,§ | 13.0 (1.6) †,\,¶ | 10.8 (1.2) #,¶,§ | 8.8 (1.7) †,#,\,§ | 13.7 (1.1) †,\,¶ | - |
| Tomita score, mean (SD) | 4.1 (1.3) | 3.7 (0.9) \,¶,§ | 3.1 (1.2) \,¶ | 5.6 (1.0) †,#,§ | 5.4 (0.8) †,#,§ | 2.5 (0.5) †,\,¶ | - |
| Preoperative systemic therapy, n (%) | 65 (52.4) | 28 (54.9) | 5 (35.7) | 3 (23.1) | 7 (53.8) | 9 (75.0) | 0.07 |
| Postoperative systemic therapy, n (%) | 85 (68.5) | 35 (68.6) | 10 (71.4) | 9 (69.2) | 9 (69.2) | 10 (83.3) | 0.88 |
| Groups | Total | Kidney | Thyroid | Low-Grade Sarcoma | Lung | Breast | p |
|---|---|---|---|---|---|---|---|
| Number of patients | 124 | 51 | 14 | 13 | 13 | 12 | - |
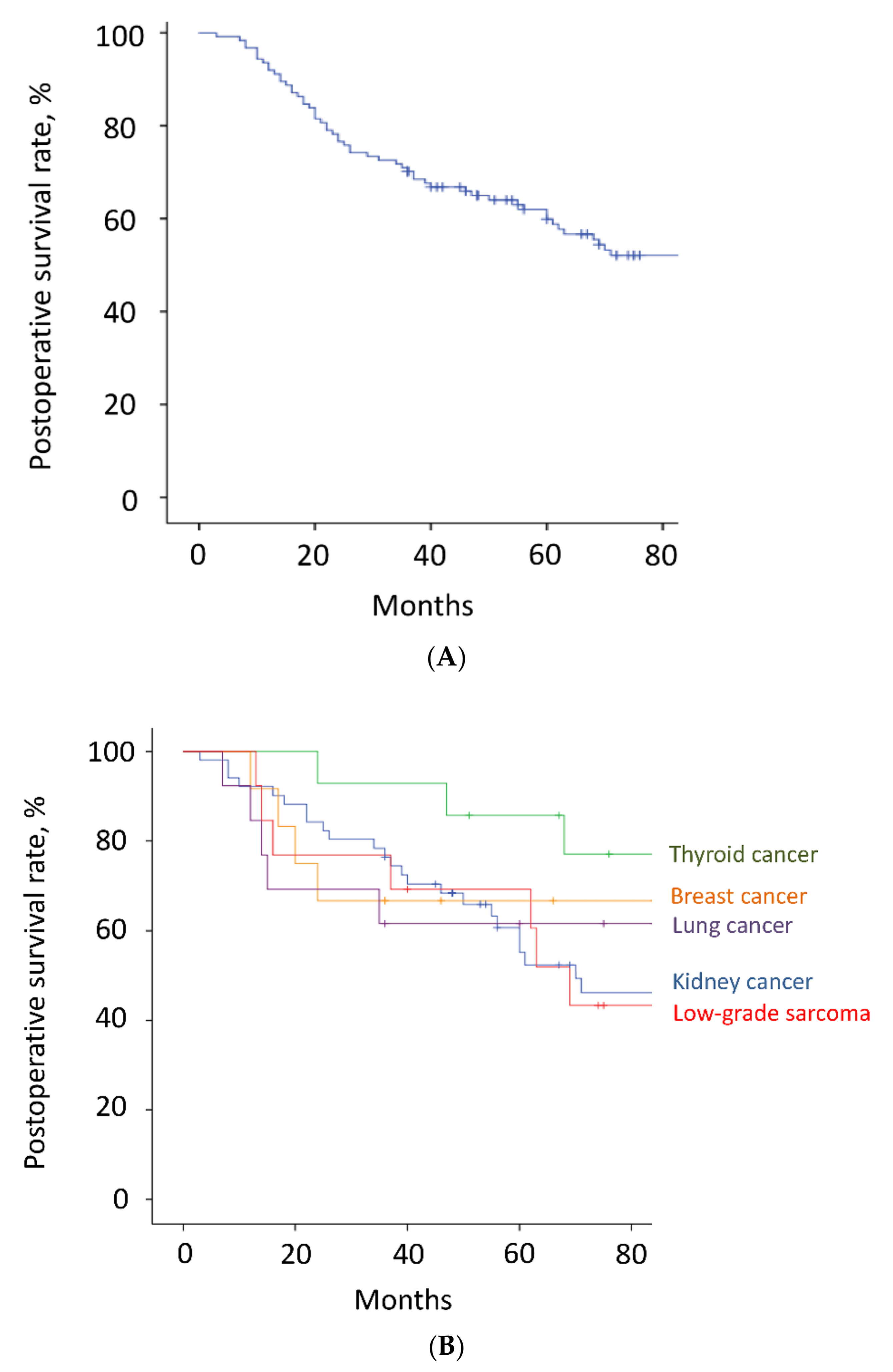
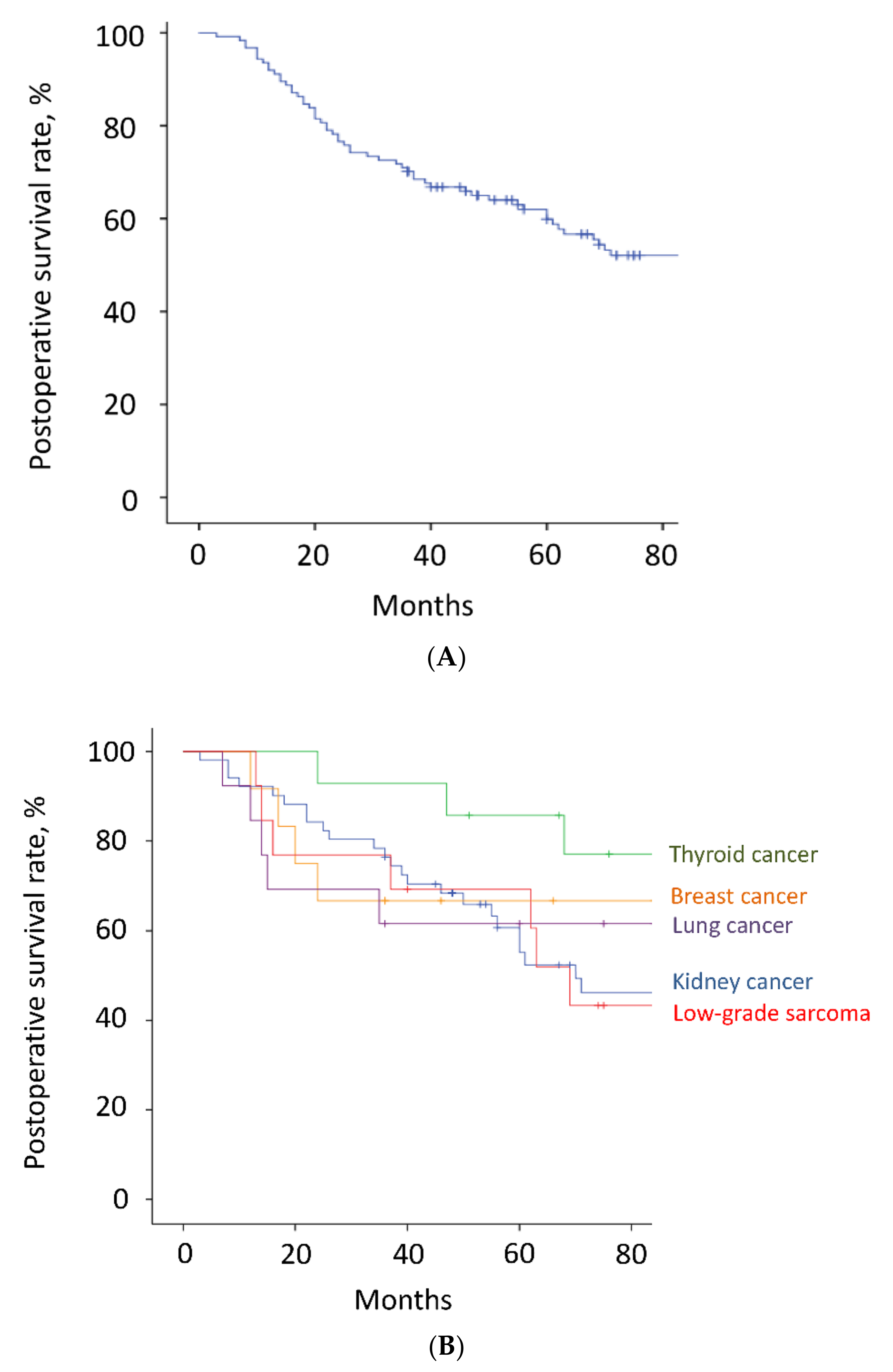
| 3-year survival, % | 70.2 | 76.5 | 92.9 | 76.9 | 61.5 | 66.7 | 0.45 |
| 5-year survival, % | 59.9 | 60.6 | 85.7 | 69.2 | 61.5 | 66.7 | |
| Median survival, months | 93 | 70 | ND | 69 | 101 | 116 | - |
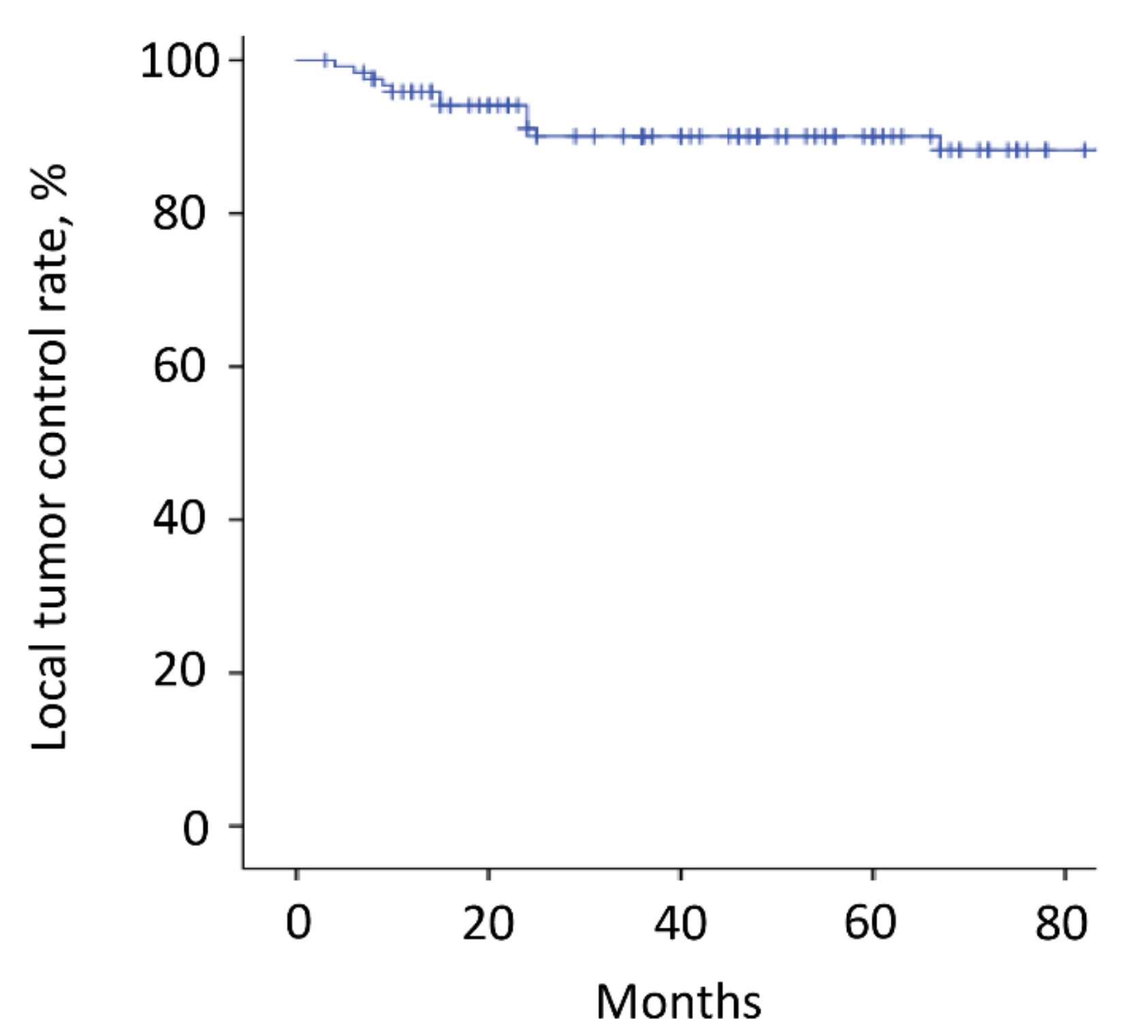
| Local recurrence of the operated spinal lesion, n (%) | 12 (9.7) | 3 (5.9) | 1 (7.1) | 2 (15.4) | 1 (7.7) | 1 (8.3) | 0.86 |
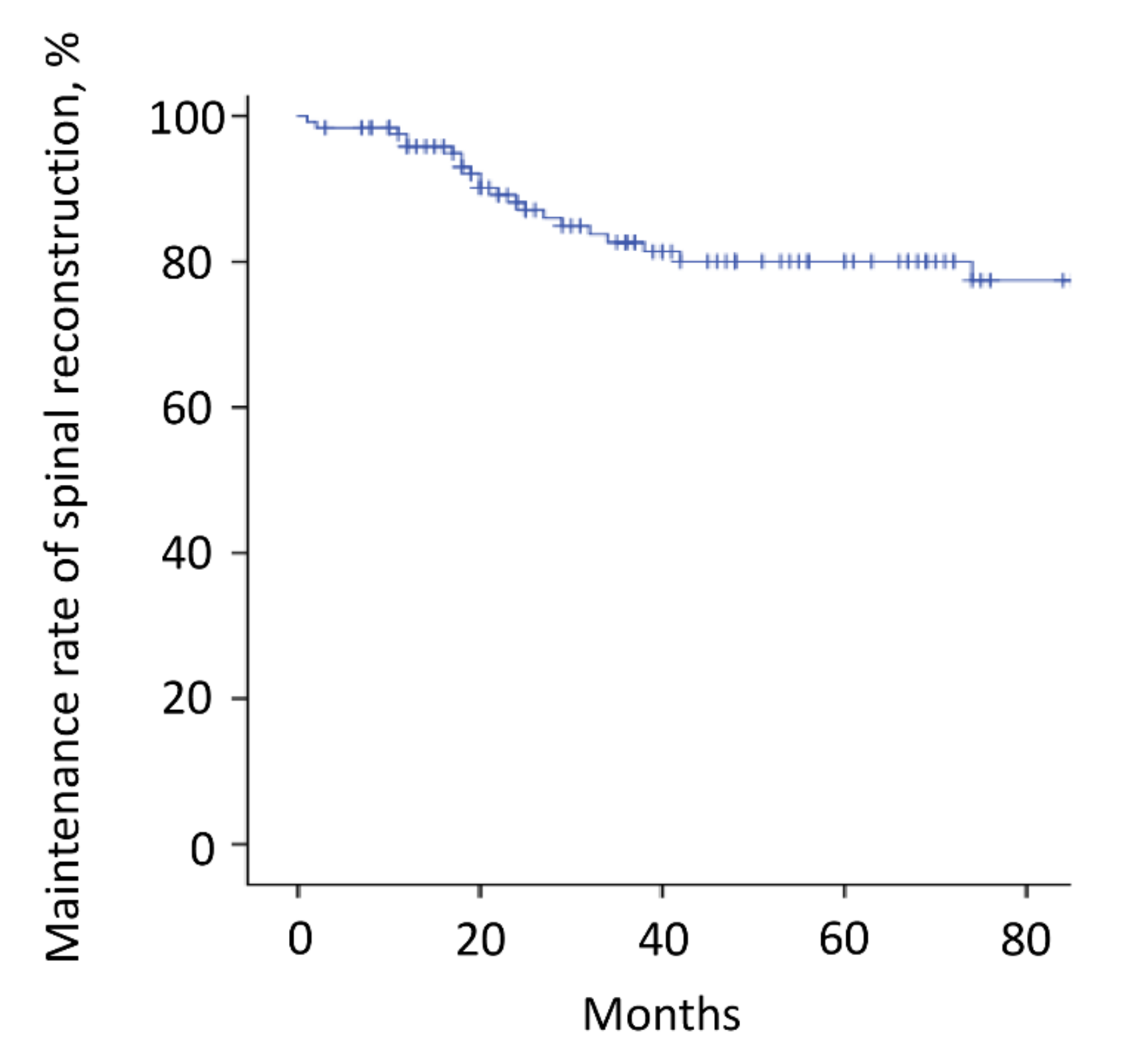
| Instrumentation failure requiring revision surgery, n (%) | 27 (21.8) | 10 (19.6) | 4 (28.6) | 3 (23.1) | 4 (30.8) | 1 (8.3) | 0.65 |
| Patients who had only one metastasis in the operated spine at the time of surgery | |||||||
| Number of patients | 56 | 16 | 5 | 6 | 9 | 5 | - |
| 3-year survival | 62.5 | 81.3 | 100 | 50.0 | 55.6 | 80.0 | 0.41 |
| 5-year survival | 56.6 | 65.6 | 80 | 50.0 | 55.6 | 80.0 | |
| 3-year survival with NED, n (%) | 24 (42.9) | 9 (56.3) | 4 (80.0) | 1 (16.7) | 4 (44.4) | 3 (60.0) | 0.29 |
| Groups | Total | Kidney | Thyroid | Low-Grade Sarcoma | Lung | Breast | p |
|---|---|---|---|---|---|---|---|
| Number of patients | 88 | 39 | 13 | 10 | 8 | 8 | - |
| Proportion of ≥3-year survivors | 71.0% | 76.5% | 92.9% | 76.9% | 61.5% | 66.7% | 0.38 |
| Good PS (ECOG PS: 0 or 1) 3 years after surgery, n (%) | 80 (90.9) | 35 (87.5) | 11 (84.6) | 10 (100) | 8 (100) | 7 (87.5) | 0.61 |
| Preoperative systemic therapy, n (%) | 46 (52.3) | 22 (56.4) | 4 (30.8) | 3 (30.0) | 5 (62.5) | 6 (75.0) | 0.15 |
| Postoperative systemic therapy, n (%) | 62 (70.5) | 28 (71.8) | 9 (69.2) | 6 (60.0) | 6 (75.0) | 7 (87.5) | 0.76 |
| Antiresorptive therapy, n (%) | 30 (34.1) | 16 (40.0) | 4 (30.8) | 1 (10.0) | 1 (12.5) | 7 (87.5) | <0.05 |
| Disease progression of BMs except for the operated spine lesions, n (%) | 27 (30.7) | 14 (35.0) | 4 (30.8) | 3 (30.0) | 1 (12.5) | 3 (37.5) | 0.79 |
| Additional excisional surgery for other BMs, n (% of patients with disease progression of BMs) | 12 (44.4) | 7 (50.0) | 3 (75.0) | 0 (0) | 0 (0) | 0 (0) | 0.12 |
| Disease progression of non-skeletal metastases, n (%) | 36 (40.9) | 19 (47.5) | 2 (15.4) | 8 (80.0) | 2 (25.0) | 2 (25.0) | <0.05 |
| Additional excisional surgery for non-skeletal lesions, n (% of patients with disease progression of non-skeletal metastases) | 8 (25.0) | 7 (36.8) | 0 (0) | 3 (37.5) | 0 (0) | 0 (0) | 0.53 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kato, S.; Demura, S.; Murakami, H.; Shinmura, K.; Yokogawa, N.; Annen, R.; Kobayashi, M.; Yamada, Y.; Nagatani, S.; Kawahara, N.; et al. Medium to Long-Term Clinical Outcomes of Spinal Metastasectomy. Cancers 2022, 14, 2852. https://doi.org/10.3390/cancers14122852
Kato S, Demura S, Murakami H, Shinmura K, Yokogawa N, Annen R, Kobayashi M, Yamada Y, Nagatani S, Kawahara N, et al. Medium to Long-Term Clinical Outcomes of Spinal Metastasectomy. Cancers. 2022; 14(12):2852. https://doi.org/10.3390/cancers14122852
Chicago/Turabian StyleKato, Satoshi, Satoru Demura, Hideki Murakami, Kazuya Shinmura, Noriaki Yokogawa, Ryohei Annen, Motoya Kobayashi, Yohei Yamada, Satoshi Nagatani, Norio Kawahara, and et al. 2022. "Medium to Long-Term Clinical Outcomes of Spinal Metastasectomy" Cancers 14, no. 12: 2852. https://doi.org/10.3390/cancers14122852
APA StyleKato, S., Demura, S., Murakami, H., Shinmura, K., Yokogawa, N., Annen, R., Kobayashi, M., Yamada, Y., Nagatani, S., Kawahara, N., & Tsuchiya, H. (2022). Medium to Long-Term Clinical Outcomes of Spinal Metastasectomy. Cancers, 14(12), 2852. https://doi.org/10.3390/cancers14122852