
Efficacy of Vinflunine for Patients with Metastatic Urothelial Cancer after Immune Checkpoint Inhibitor Pretreatment—A Retrospective Multicenter Analysis

 , ,
, ,  ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Characteristics of the Study Cohort
3.2. Treatment Exposure and Tolerability
3.3. Efficacy
3.3.1. Best Overall Response
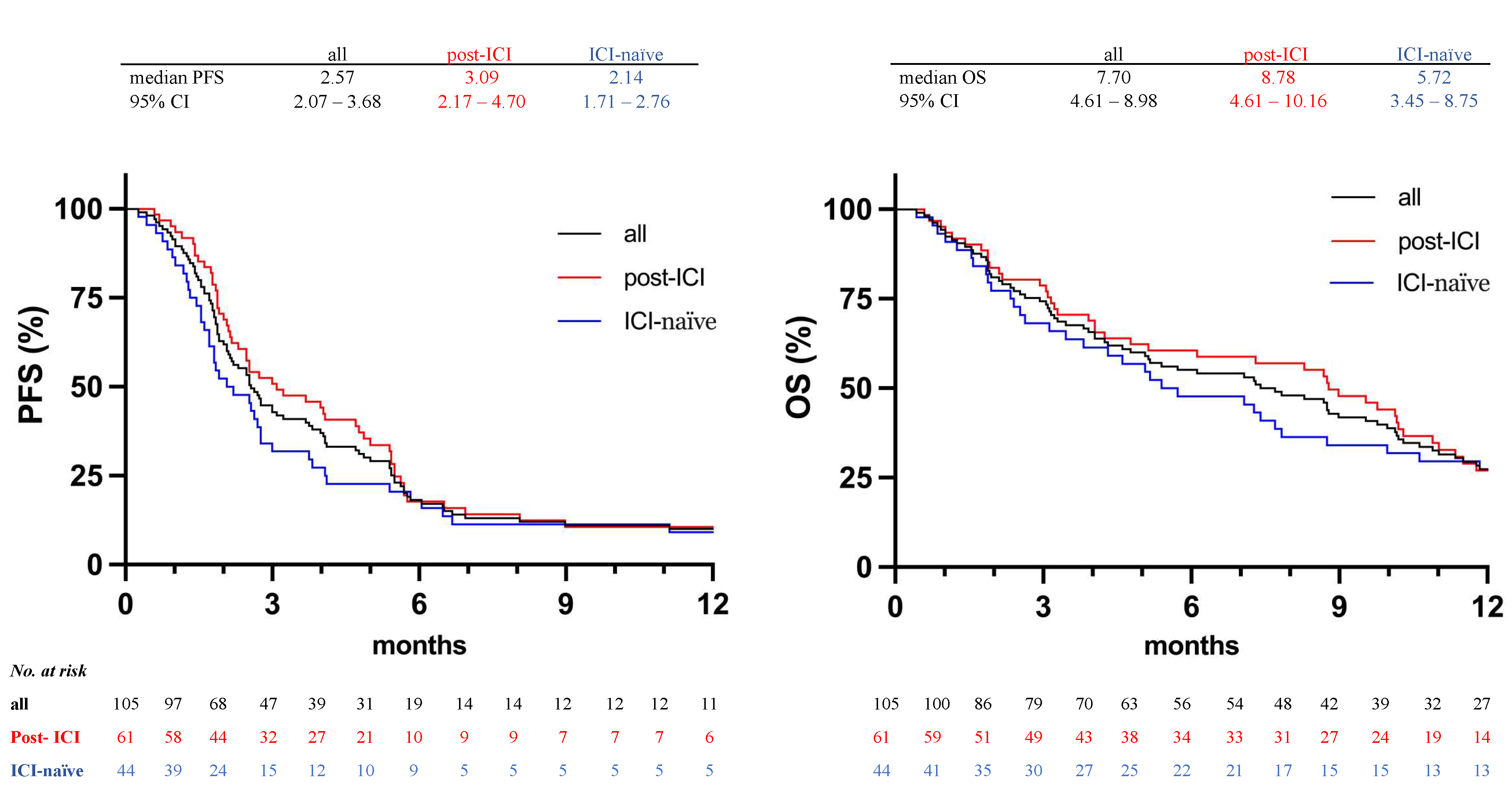
3.3.2. Survival
3.3.3. Clinical Predictors of Treatment Efficacy of Vinflunine
3.3.4. Clinical Predictors for the Risk of Death
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Powles, T.; Park, S.H.; Voog, E.; Caserta, C.; Valderrama, B.P.; Gurney, H.; Kalofonos, H.; Radulović, S.; Demey, W.; Ullén, A.; et al. Avelumab Maintenance Therapy for Advanced or Metastatic Urothelial Carcinoma. N. Engl. J. Med. 2020, 383, 1218–1230. [Google Scholar] [CrossRef] [PubMed]
- EAU Guidelines. Presented at the EAU Annual Congress Barcelona 2019. Available online: http://uroweb.org/guidelines/compilations-of-all-guidelines/ (accessed on 2 November 2021).
- Balar, A.V.; Galsky, M.D.; Rosenberg, J.E.; Powles, T.; Petrylak, D.P.; Bellmunt, J.; Loriot, Y.; Necchi, A.; Hoffman-Censits, J.; Perez-Gracia, J.L.; et al. Atezolizumab as first-line treatment in cisplatin-ineligible patients with locally advanced and metastatic urothelial carcinoma: A single-arm, multicentre, phase 2 trial. Lancet 2017, 389, 67–76. [Google Scholar] [CrossRef] [Green Version]
- O’Donnell, P.H.; Balar, A.V.; Vuky, J.; Castellano, D.; Bellmunt, J.; Powles, T.; Bajorin, D.F.; Grivas, P.; Hahn, N.M.; Plimack, E.R.; et al. First-line pembrolizumab (pembro) in cisplatin-ineligible patients with advanced urothelial cancer (UC): Response and survival results up to five years from the KEYNOTE-052 phase 2 study. J. Clin. Oncol. 2021, 39, 4508. [Google Scholar] [CrossRef]
- Soria, F.; Beleni, A.I.; D’Andrea, D.; Resch, I.; Gust, K.M.; Gontero, P.; Shariat, S.F. Pseudoprogression and hyperprogression during immune checkpoint inhibitor therapy for urothelial and kidney cancer. World J. Urol. 2018, 36, 1703–1709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richters, A.; Aben, K.K.H.; Kiemeney, L.A.L.M. The global burden of urinary bladder cancer: An update. World J. Urol. 2020, 38, 1895–1904. [Google Scholar] [CrossRef] [Green Version]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Brousell, S.C.; Fantony, J.J.; Van Noord, M.; Harrison, M.R.; Inman, B.A. Vinflunine for the treatment of advanced or metastatic transitional cell carcinoma of the urothelial tract: An evidence-based review of safety, efficacy, and place in therapy. Core Évid. 2018, 13, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Bellmunt, J.; Théodore, C.; Demkov, T.; Komyakov, B.; Sengelov, L.; Daugaard, G.; Caty, A.; Carles, J.; Jagiello-Gruszfeld, A.; Karyakin, O.; et al. Phase III Trial of Vinflunine Plus Best Supportive Care Compared With Best Supportive Care Alone After a Platinum-Containing Regimen in Patients With Advanced Transitional Cell Carcinoma of the Urothelial Tract. J. Clin. Oncol. 2009, 27, 4454–4461. [Google Scholar] [CrossRef]
- Bamias, A.; Hegele, A.; Medioni, J.; Castellano, D.; Doni, L.; Passalacqua, R.; Zagouri, F.; Tzannis, K.; Hussain, S.; Ullen, A. Vinflunine in the treatment of relapsed metastatic urothelial cancer: A systematic review and meta-analysis of real-world series. Crit. Rev. Oncol. 2019, 140, 80–87. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Vinflunine for the Treatment of Advanced or Metastatic Transitional Cell Carcinoma of the Urothelial Tract: Technology Appraisal Guidance (TA272). 23 January 2013. Available online: https://www.nice.org.uk/guidance/ta272/chapter/1-Guidance (accessed on 10 March 2022).
- Deininger, S.; Törzsök, P.; Oswald, D.; Lusuardi, L. Current Systemic Treatment Options in Metastatic Urothelial Carcinoma after Progression on Checkpoint Inhibition Therapy—A Systemic Review Combined with Single-Group Meta-Analysis of Three Studies Testing Enfortumab Vedotin. Cancers 2021, 13, 3206. [Google Scholar] [CrossRef]
- Bellmunt, J.; Choueiri, T.K.; Fougeray, R.; Schutz, F.A.; Salhi, Y.; Winquist, E.; Culine, S.; Von Der Maase, H.; Vaughn, D.J.; Rosenberg, J.E. Prognostic Factors in Patients With Advanced Transitional Cell Carcinoma of the Urothelial Tract Experiencing Treatment Failure With Platinum-Containing Regimens. J. Clin. Oncol. 2010, 28, 1850–1855. [Google Scholar] [CrossRef] [PubMed]
- Common Terminology Criteria for Adverse Events (CTCAE) Version 5. Published: November 27, 2017. US Department of Health and Human Services, National Institutes of Health, National Cancer Institute. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_5x7.pdf (accessed on 19 March 2020).
- Powles, T.; Rosenberg, J.E.; Sonpavde, G.P.; Loriot, Y.; Durán, I.; Lee, J.-L.; Matsubara, N.; Vulsteke, C.; Castellano, D.; Wu, C.; et al. Enfortumab Vedotin in Previously Treated Advanced Urothelial Carcinoma. N. Engl. J. Med. 2021, 384, 1125–1135. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Bellmunt, J.; Comperat, E.; De Santis, M.; Huddart, R.; Loriot, Y.; Necchi, A.; Valderrama, B.; Ravaud, A.; Shariat, S.; et al. Bladder cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2021, 33, 244–258. [Google Scholar] [CrossRef] [PubMed]
- Bersanelli, M.; Buti, S.; Cortellini, A.; Bandini, M.; Banna, G.L.; Pederzoli, F.; Farè, E.; Raggi, D.; Giannatempo, P.; De Giorgi, U.; et al. Clinical Outcomes of Patients With Metastatic Urothelial Carcinoma After Progression to Immune Checkpoint Inhibitors: A Retrospective Analysis by the Meet-Uro Group (Meet-URO 1 Study). Clin. Med. Insights Oncol. 2021, 15, 117955492110216. [Google Scholar] [CrossRef] [PubMed]
- Dwary, A.D.; Master, S.; Patel, A.; Cole, C.; Mansour, R.; Mills, G.; Koshy, N.; Peddi, P.; Burton, G.; Hammoud, D.; et al. Excellent response to chemotherapy post immunotherapy. Oncotarget 2017, 8, 91795–91802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hadash-Bengad, R.; Hajaj, E.; Klein, S.; Merims, S.; Frank, S.; Eisenberg, G.; Yakobson, A.; Orevi, M.; Caplan, N.; Peretz, T.; et al. Immunotherapy Potentiates the Effect of Chemotherapy in Metastatic Melanoma—A Retrospective Study. Front. Oncol. 2020, 10, 70. [Google Scholar] [CrossRef]
- Saleh, K.; Daste, A.; Martin, N.; Pons-Tostivint, E.; Auperin, A.; Herrera-Gomez, R.G.; Baste-Rotllan, N.; Bidault, F.; Guigay, J.; Le Tourneau, C.; et al. Response to salvage chemotherapy after progression on immune check-point inhibitors in patients with recurrent and/or metastatic squamous cell carcinoma of the head and neck. Eur. J. Cancer 2019, 121, 123–129. [Google Scholar] [CrossRef]
- Schvartsman, G.; Peng, S.A.; Bis, G.; Lee, J.J.; Benveniste, M.F.K.; Zhang, J.; Roarty, E.B.; Lacerda, L.; Swisher, S.; Heymach, J.V.; et al. Response rates to single-agent chemotherapy after exposure to immune checkpoint inhibitors in advanced non-small cell lung cancer. Lung Cancer 2017, 112, 90–95. [Google Scholar] [CrossRef]
- Bracci, L.; Schiavoni, G.; Sistigu, A.; Belardelli, F. Immune-based mechanisms of cytotoxic chemotherapy: Implications for the design of novel and rationale-based combined treatments against cancer. Cell Death Differ. 2014, 21, 15–25. [Google Scholar] [CrossRef] [Green Version]
- Montazeri, K.; Sonpavde, G. Salvage systemic therapy for metastatic urothelial carcinoma: An unmet clinical need. Expert Rev. Anticancer Ther. 2021, 21, 299–313. [Google Scholar] [CrossRef]
- Stecca, C.; Abdeljalil, O.; Sridhar, S.S. Metastatic Urothelial Cancer: A rapidly changing treatment landscape. Ther. Adv. Med Oncol. 2021, 13, 175883592110473. [Google Scholar] [CrossRef] [PubMed]
- Bernardini, A.; Dueñas, M.; Martín-Soberon, M.C.; Rubio, C.; Suarez-Cabrera, C.; Ruiz-Palomares, R.; Munera-Maravilla, E.; Lázaro, S.; Lodewijk, I.; Rueda, D.; et al. Genomic Landscape of Vinflunine Response in Metastatic Urothelial Cancer. Cancers 2022, 14, 378. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Patient Characteristics at Baseline | Post-ICI n = 61 (58.1%) April 2016–December 2021 | ICI-Naïve n = 44 (41.9%) February 2010–May 2019 | p |
|---|---|---|---|
| Age (years) | |||
| median | 66.5 | 66.3 | 0.9549 |
| IQR range | 14.65 49–87 | 11.97 51–84 | |
| Site of primary tumor | |||
| lower tract | 82.0% (50) | 72.7% (32) | 0.2587 |
| upper tract | 18.0% (11) | 27.3% (12) | |
| Therapy line | |||
| median mean SD | 3 3.2 0.68 | 2 2.36 0.61 | <0.0001 |
| range | 3–6 | 2–5 | |
| Period from initial diagnosis of MIBC 1 or primary mUC to first Vinflunine administration (months) | |||
| median IQR | 24.4 33.0 | 15.5 30.4 | 0.0333 |
| range | 6.6–156.6 | 3.3–128.7 | |
| Metastatic site | |||
| lymph node | 86.9% (53) | 84.1% (37) | 0.6864 |
| bone | 57.4% (35) | 22.7% (10) | 0.0341 |
| pulmonary | 44.3% (27) | 36.4% (16) | 0.4167 |
| visceral liver | 63.9% (39) 34.4% (21) | 63.6% (28) 40.9% (18) | 0.9750 0.4976 |
| Negative prognostic factors by Bellmunt et al. [13] | |||
| median | 1 | 1 | 0.9855 |
| mean SD | 1.28 0.90 | 1.27 0.95 | |
| Hb < 10 g/dL 2 | 24.6% (15) | 22.7% (10) | 0.8250 |
| ECOG 3 | |||
| 0 1 2 3 median mean SD | 31.1% (19) 49.2% (30) 16.4% (10) 3.3% (2) 1 0.92 0.78 | 36.4% (16) 52.3% (23) 9.1% (4) 2.3% (1) 1 0.77 0.71 | 0.5759 0.7545 0.3859 >0.9999 0.3638 |
| Renal function (GFR; ml/min) 4 | |||
| median IQR range | 53 28.0 22–99 | 58 25.5 27–133 | 0.3551 |
| Prior cystectomy or nephroureterectomy | 63.3% (38) | 56.8% (25) | 0.5018 |
| Neoadjuvant therapy | 11.7% (7) | 2.3% (1) | 0.1340 |
| Prior irradiation of the pelvis | 23.3% (14) | 6.8% (3) | 0.0314 |
| End Point | All | Post-ICI | ICI-Naïve | p |
|---|---|---|---|---|
| No. of included patients | 105 | 61 | 44 | |
| Overall response in evaluable patients | ||||
| No. of patients | 81 | 49 | 32 | |
| Complete response | ||||
| No. of patients | 1 | 1 | 0 | |
| % | 1.2 | 2.0 | 0 | |
| Partial response | ||||
| No. of patients | 15 | 10 | 5 | |
| % | 18.5 | 20.4 | 15.6 | |
| Stable disease | ||||
| No. of patients | 17 | 14 | 3 | |
| % | 21.0 | 28.6 | 9.4 | |
| Overall response rate | 0.4508 | |||
| No. of patients | 16 | 11 | 5 | |
| % | 19.8 | 22.4 | 15.6 | |
| 95% CI,% | 12.5–29.7 | 13.0–35.9 | 6.9–31.8 | |
| Clinical benefit rate | 0.0198 | |||
| No. of patients | 33 40.7 30.1–51.6 | 25 51.0 37.5–64.4 | 8 25.0 13.3–42.1 | |
| % 95% CI,% |
| Survival | All | Post-ICI (n = 61) | ICI-Naïve (n = 44) |
|---|---|---|---|
| PFS after 3 months (%) | 44.8 (47/105) | 52.5 (32/61) | 34.1 (15/44) |
| PFS after 6 months (%) | 18.4 (19/103) | 16.9 (10/59) | 20.4 (9/44) |
| PFS after 9 months (%) | 11.7 (12/103) | 11.9 (7/59) | 11.4 (5/44) |
| PFS after 12 months (%) | 10.7 (11/103) | 10.2 (6/59) | 11.4 (5/44) |
| OS after 3 months (%) | 75.2 (79/105) | 80.3 (49/61) | 68.2 (30/44) |
| OS after 6 months (%) | 54.9 (56/102) | 58.6 (34/58) | 50.0 (22/44) |
| OS after 9 months (%) | 41.6 (42/101) | 47.4 (27/57) | 34.1 (15/44) |
| OS after 12 months (%) | 27.0 (27/100) | 25.0 (14/56) | 29.5 (13/44) |
| Variable | OR | 95% CI | p |
|---|---|---|---|
| ICI pretreatment | 3.900 | 1.494–10.99 | 0.0071 |
| age > 70 years | 0.6293 | 0.2423–1.586 | 0.3310 |
| GFR 1 < 60 mL/min | 0.6923 | 0.2785–1.704 | 0.4241 |
| lymph node disease only | 0.6705 | 0.1882–2.166 | 0.5134 |
| liver metastases | 0.7292 | 0.2730–1.888 | 0.5190 |
| prior pelvic irradiation | 0.6944 | 0.1946–2.249 | 0.5517 |
| pulmonary metastases | 1.254 | 0.5035–3.130 | 0.6257 |
| Hb 2 < 10 g/dL | 1.224 | 0.4272–3.479 | 0.7027 |
| initial dose of 320 mg/m2 body surface | 1.588 | 0.8738–2.969 | 0.7621 |
| bone metastases | 0.8942 | 0.3538–2.232 | 0.8109 |
| Upper tract urothelial carcinoma | 0.8815 | 0.2861–2.603 | 0.8206 |
| Bellmunt risk factors ≥ 1 | 0.9832 | 0.3880–2.468 | 0.9712 |
| ECOG 3 ≥ 1 | 0.9890 | 0.3976–2.475 | 0.9810 |
| Variable | OR | 95% CI | p |
|---|---|---|---|
| ICI pretreatment | 6.895 | 2.139–25.66 | 0.0021 |
| bone metastases | 0.4234 | 0.1076–1.276 | 0.1557 |
| prior pelvic irradiation | 0.4824 | 0.1213–1.780 | 0.2820 |
| Variable | HR | 95% CI | p |
|---|---|---|---|
| ECOG 1 ≥ 1 | 2.248 | 1.365–3.825 | 0.0020 |
| Hb 2 < 10 g/dL | 1.737 | 1.013–2.897 | 0.0386 |
| liver metastases | 1.565 | 0.9802–2.483 | 0.0581 |
| ICI pretreatment | 0.6451 | 0.3983–1.045 | 0.0742 |
| bone metastases | 1.255 | 0.7529–2.103 | 0.3857 |
| initial dose of 320 mg/m2 body surface | 1.129 | 0.7103–1.777 | 0.6021 |
| GFR 3 < 60 mL/min | 0.9126 | 0.5737–1.454 | 0.6987 |
| age > 70 years | 0.9323 | 0.5784–1.483 | 0.7700 |
| prior pelvic irradiation | 1.009 | 0.5512–1.764 | 0.9746 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riedel, F.; Münker, M.; Roghmann, F.; Breyer, J.; Schnabel, M.J.; Burger, M.; Sikic, D.; Büttner, T.; Ritter, M.; Hiller, K.; et al. Efficacy of Vinflunine for Patients with Metastatic Urothelial Cancer after Immune Checkpoint Inhibitor Pretreatment—A Retrospective Multicenter Analysis. Cancers 2022, 14, 2850. https://doi.org/10.3390/cancers14122850
Riedel F, Münker M, Roghmann F, Breyer J, Schnabel MJ, Burger M, Sikic D, Büttner T, Ritter M, Hiller K, et al. Efficacy of Vinflunine for Patients with Metastatic Urothelial Cancer after Immune Checkpoint Inhibitor Pretreatment—A Retrospective Multicenter Analysis. Cancers. 2022; 14(12):2850. https://doi.org/10.3390/cancers14122850
Chicago/Turabian StyleRiedel, Felix, Mara Münker, Florian Roghmann, Johannes Breyer, Marco J. Schnabel, Maximilian Burger, Danijel Sikic, Thomas Büttner, Manuel Ritter, Kiriaki Hiller, and et al. 2022. "Efficacy of Vinflunine for Patients with Metastatic Urothelial Cancer after Immune Checkpoint Inhibitor Pretreatment—A Retrospective Multicenter Analysis" Cancers 14, no. 12: 2850. https://doi.org/10.3390/cancers14122850
APA StyleRiedel, F., Münker, M., Roghmann, F., Breyer, J., Schnabel, M. J., Burger, M., Sikic, D., Büttner, T., Ritter, M., Hiller, K., Wezel, F., Bolenz, C., & Zengerling, F. (2022). Efficacy of Vinflunine for Patients with Metastatic Urothelial Cancer after Immune Checkpoint Inhibitor Pretreatment—A Retrospective Multicenter Analysis. Cancers, 14(12), 2850. https://doi.org/10.3390/cancers14122850