
The Association between the Pan-Immune-Inflammation Value and Cancer Prognosis: A Systematic Review and Meta-Analysis

 ,
,  ,
,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection and Data Extraction
2.4. Meta-Analyses
3. Results
3.1. The Study Characteristics
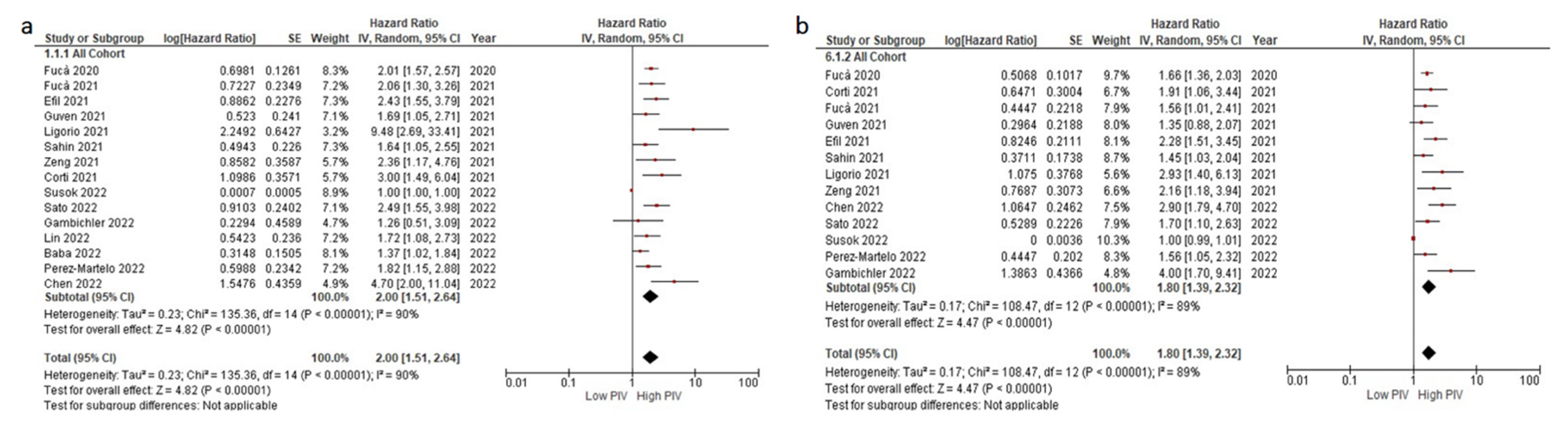
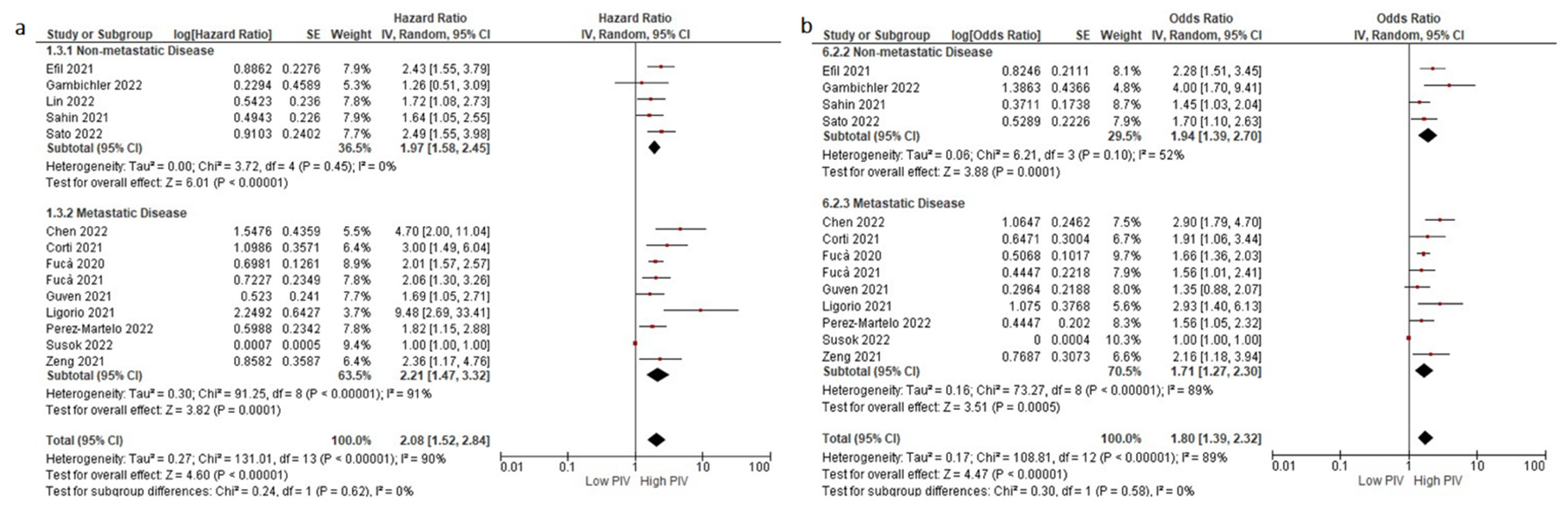
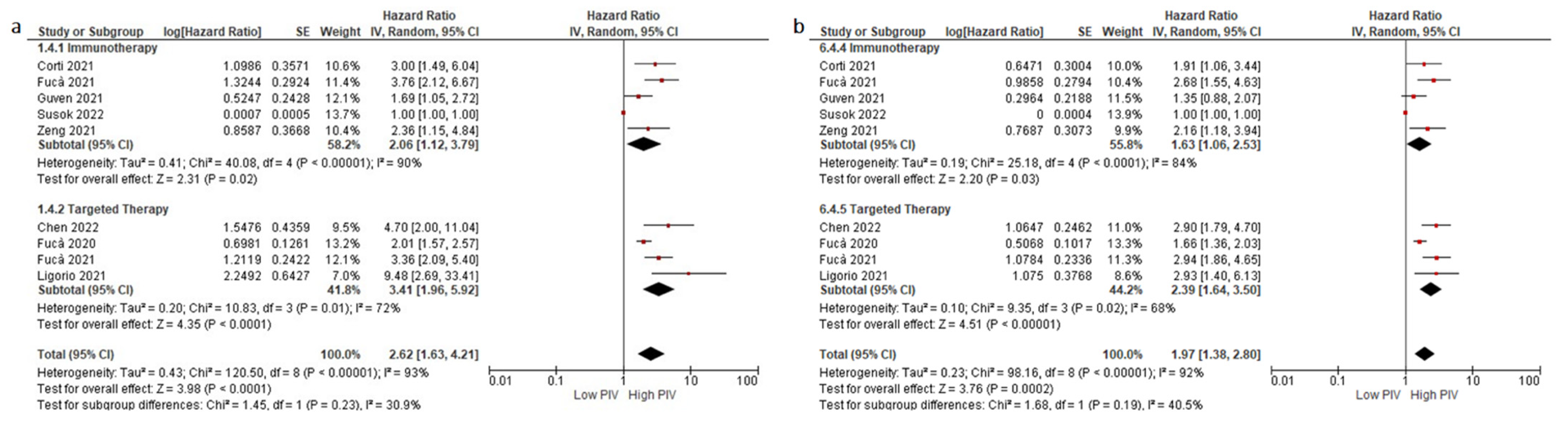
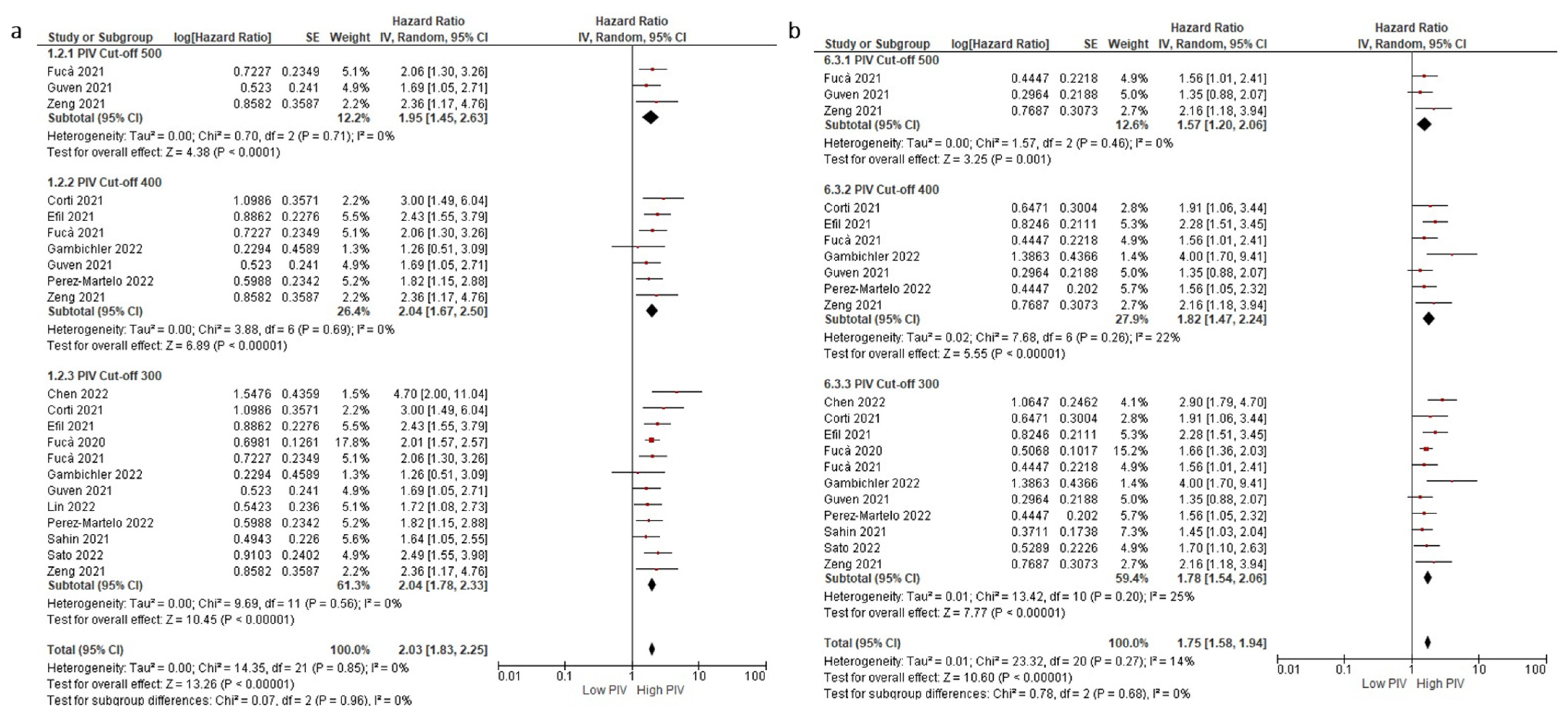
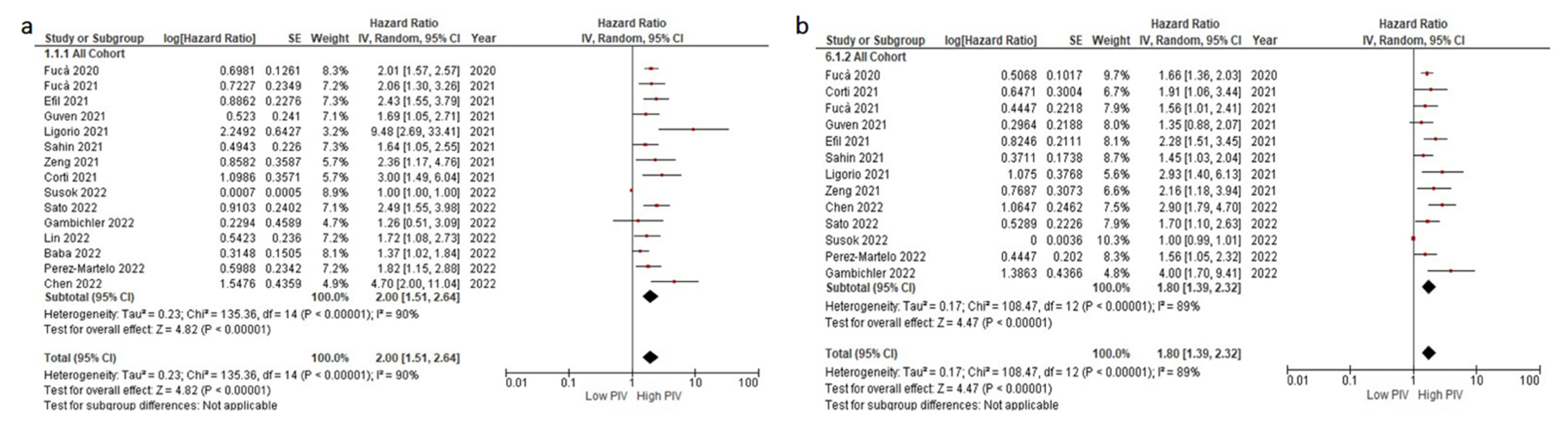
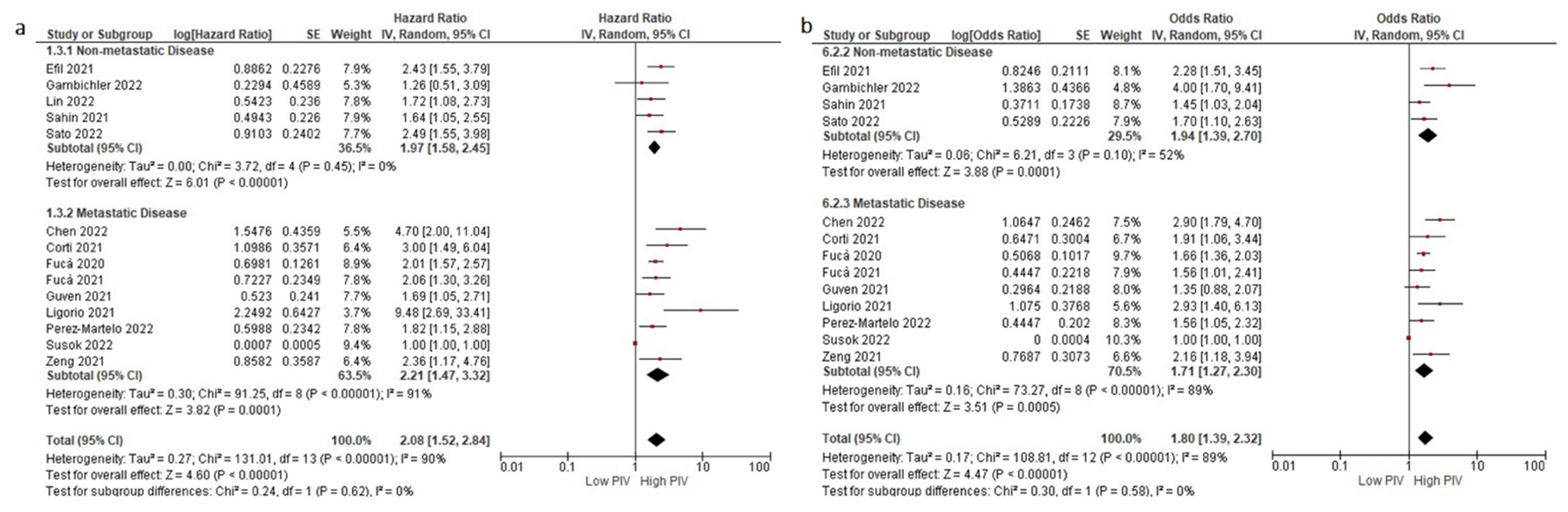
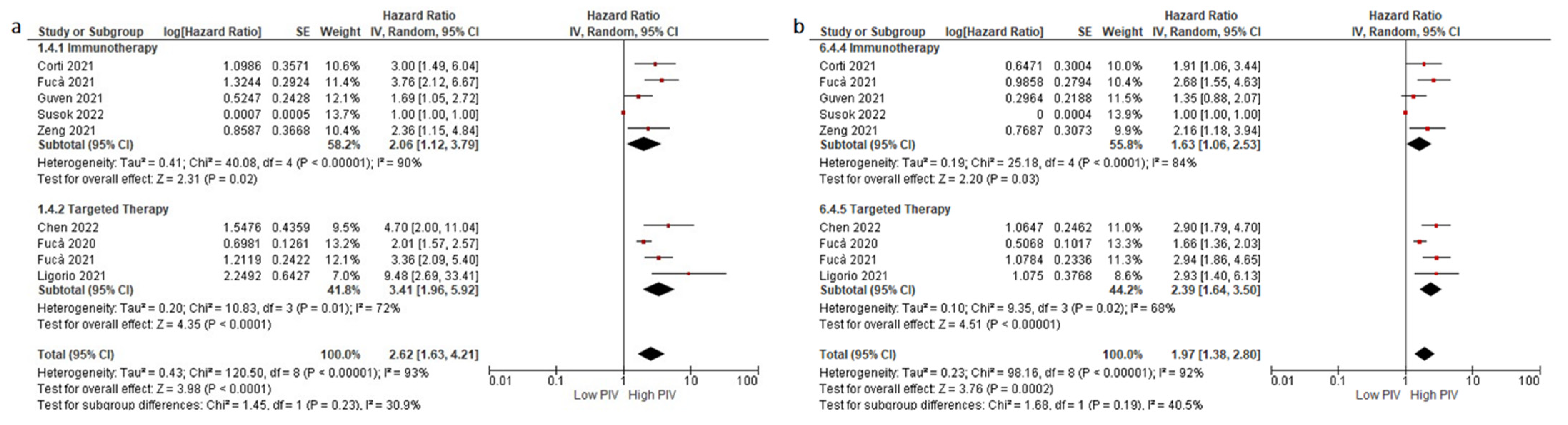
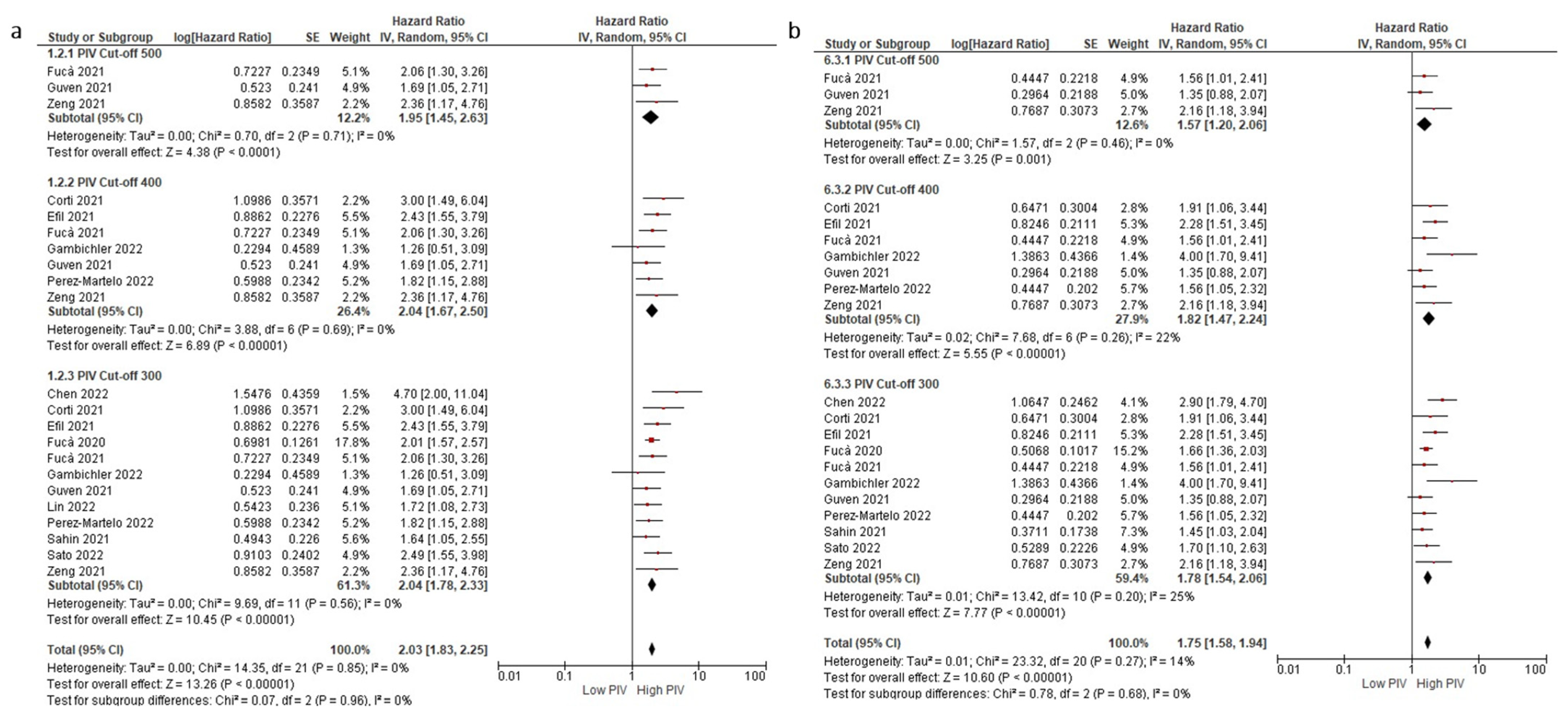
3.2. Association between OS and PIV Levels
3.3. Association between DFS/PFS and PIV Levels
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Mattiuzzi, C.; Lippi, G. Current Cancer Epidemiology. J. Epidemiol. Glob. Health 2019, 9, 217–222. [Google Scholar] [CrossRef] [Green Version]
- Bray, F.; Laversanne, M.; Weiderpass, E.; Soerjomataram, I. The ever-increasing importance of cancer as a leading cause of premature death worldwide. Cancer 2021, 127, 3029–3030. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Carrera, P.M.; Kantarjian, H.M.; Blinder, V.S. The financial burden and distress of patients with cancer: Understanding and stepping-up action on the financial toxicity of cancer treatment. CA Cancer J. Clin. 2018, 68, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.D.; Nogueira, L.; Mariotto, A.B.; Rowland, J.H.; Yabroff, K.R.; Alfano, C.M.; Jemal, A.; Kramer, J.L.; Siegel, R.L. Cancer treatment and survivorship statistics, 2019. CA Cancer J. Clin. 2019, 69, 363–385. [Google Scholar] [CrossRef] [Green Version]
- Goossens, N.; Nakagawa, S.; Sun, X.; Hoshida, Y. Cancer biomarker discovery and validation. Transl. Cancer Res. 2015, 4, 256–269. [Google Scholar] [CrossRef] [PubMed]
- Sauter, E.R. Reliable Biomarkers to Identify New and Recurrent Cancer. Eur. J. Breast Health 2017, 13, 162–167. [Google Scholar] [CrossRef]
- Guven, D.C.; Sahin, T.K.; Dizdar, O.; Kilickap, S. Predictive biomarkers for immunotherapy efficacy in non-small-cell lung cancer: Current status and future perspectives. Biomark. Med. 2020, 14, 1383–1392. [Google Scholar] [CrossRef]
- Lei, Y.; Li, X.; Huang, Q.; Zheng, X.; Liu, M. Progress and Challenges of Predictive Biomarkers for Immune Checkpoint Blockade. Front. Oncol. 2021, 11, 609. [Google Scholar] [CrossRef]
- Chow, M.T.; Möller, A.; Smyth, M.J. Inflammation and immune surveillance in cancer. Semin. Cancer Biol. 2012, 22, 23–32. [Google Scholar] [CrossRef]
- Xiao, T.S. Innate immunity and inflammation. Cell. Mol. Immunol. 2017, 14, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Pandya, P.H.; Murray, M.E.; Pollok, K.E.; Renbarger, J.L. The Immune System in Cancer Pathogenesis: Potential Therapeutic Approaches. J. Immunol. Res. 2016, 2016, 4273943. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, H.; Hagerling, C.; Werb, Z. Roles of the immune system in cancer: From tumor initiation to metastatic progression. Genes Dev. 2018, 32, 1267–1284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coley, W.B. The treatment of inoperable sarcoma with the mixed toxins of erysipelas and bacillus prodigiosus: Immediate and final results in one hundred and forty cases. J. Am. Med. Assoc. 1898, XXXI, 456–465. [Google Scholar] [CrossRef]
- Lamm, D.L.; Blumenstein, B.A.; Crawford, E.D.; Montie, J.E.; Scardino, P.; Grossman, H.B.; Stanisic, T.H.; Smith, J.A., Jr.; Sullivan, J.; Sarosdy, M.F.; et al. A randomized trial of intravesical doxorubicin and immunotherapy with bacille Calmette-Guérin for transitional-cell carcinoma of the bladder. N. Engl. J. Med. 1991, 325, 1205–1209. [Google Scholar] [CrossRef]
- Mayor, P.C.; Eng, K.H.; Singel, K.L.; Abrams, S.I.; Odunsi, K.; Moysich, K.B.; Fuleihan, R.; Garabedian, E.; Lugar, P.; Ochs, H.D. Cancer in primary immunodeficiency diseases: Cancer incidence in the United States Immune Deficiency Network Registry. J. Allergy Clin. Immunol. 2018, 141, 1028–1035. [Google Scholar] [CrossRef] [Green Version]
- Simard, E.P.; Pfeiffer, R.M.; Engels, E.A. Spectrum of cancer risk late after AIDS onset in the United States. Arch. Intern. Med. 2010, 170, 1337–1345. [Google Scholar] [CrossRef] [Green Version]
- Engels, E.A.; Pfeiffer, R.M.; Fraumeni, J.F.; Kasiske, B.L.; Israni, A.K.; Snyder, J.J.; Wolfe, R.A.; Goodrich, N.P.; Bayakly, A.R.; Clarke, C.A.; et al. Spectrum of Cancer Risk among US Solid Organ Transplant Recipients. JAMA 2011, 306, 1891–1901. [Google Scholar] [CrossRef]
- Majhail, N.S.; Brazauskas, R.; Rizzo, J.D.; Sobecks, R.M.; Wang, Z.; Horowitz, M.M.; Bolwell, B.; Wingard, J.R.; Socie, G. Secondary solid cancers after allogeneic hematopoietic cell transplantation using busulfan-cyclophosphamide conditioning. Blood J. Am. Soc. Hematol. 2011, 117, 316–322. [Google Scholar] [CrossRef]
- Singh, N.; Baby, D.; Rajguru, J.P.; Patil, P.B.; Thakkannavar, S.S.; Pujari, V.B. Inflammation and cancer. Ann. Afr. Med. 2019, 18, 121–126. [Google Scholar] [CrossRef]
- Keir, M.E.; Butte, M.J.; Freeman, G.J.; Sharpe, A.H. PD-1 and its ligands in tolerance and immunity. Annu. Rev. Immunol. 2008, 26, 677–704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mantovani, A. Inflammation by remote control. Nature 2005, 435, 752–753. [Google Scholar] [CrossRef] [PubMed]
- Mittal, D.; Gubin, M.M.; Schreiber, R.D.; Smyth, M.J. New insights into cancer immunoediting and its three component phases—elimination, equilibrium and escape. Curr. Opin. Immunol. 2014, 27, 16–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leach, D.R.; Krummel, M.F.; Allison, J.P. Enhancement of antitumor immunity by CTLA-4 blockade. Science 1996, 271, 1734–1736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandfeld-Paulsen, B.; Meldgaard, P.; Sorensen, B.S.; Safwat, A.; Aggerholm-Pedersen, N. The prognostic role of inflammation-scores on overall survival in lung cancer patients. Acta Oncol. 2019, 58, 371–376. [Google Scholar] [CrossRef] [Green Version]
- Winther-Larsen, A.; Aggerholm-Pedersen, N.; Sandfeld-Paulsen, B. Inflammation-scores as prognostic markers of overall survival in lung cancer: A register-based study of 6,210 Danish lung cancer patients. BMC Cancer 2022, 22, 63. [Google Scholar] [CrossRef]
- Kumarasamy, C.; Tiwary, V.; Sunil, K.; Suresh, D.; Shetty, S.; Muthukaliannan, G.K.; Baxi, S.; Jayaraj, R. Prognostic Utility of Platelet-Lymphocyte Ratio, Neutrophil-Lymphocyte Ratio and Monocyte-Lymphocyte Ratio in Head and Neck Cancers: A Detailed PRISMA Compliant Systematic Review and Meta-Analysis. Cancers 2021, 13, 4166. [Google Scholar] [CrossRef]
- Ventriglia, J.; Petrillo, A.; Huerta Alváro, M.; Laterza, M.M.; Savastano, B.; Gambardella, V.; Tirino, G.; Pompella, L.; Diana, A.; Iovino, F.; et al. Neutrophil to Lymphocyte Ratio as a Predictor of Poor Prognosis in Metastatic Pancreatic Cancer Patients Treated with Nab-Paclitaxel plus Gemcitabine: A Propensity Score Analysis. Gastroenterol. Res. Pract. 2018, 2018, 2373868. [Google Scholar] [CrossRef]
- Cao, W.; Yao, X.; Cen, D.; Zhi, Y.; Zhu, N.; Xu, L. The prognostic role of platelet-to-lymphocyte ratio on overall survival in gastric cancer: A systematic review and meta-analysis. BMC Gastroenterol. 2020, 20, 16. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Q.; Dong, J.; Sun, Q.; Lu, N.; Pan, Y.; Han, X. Role of neutrophil-to-lymphocyte ratio as a prognostic biomarker in patients with breast cancer receiving neoadjuvant chemotherapy: A meta-analysis. BMJ Open 2021, 11, e047957. [Google Scholar] [CrossRef]
- Aktepe, O.H.; Güner, G.; Güven, D.C.; Şahin, T.K.; Ardıç, F.S.; Yüce, D.; Yalçın, Ş.; Erman, M. The platelet to lymphocyte ratio predicts overall survival better than the neutrophil to lymphocyte ratio in metastatic renal cell carcinoma. Turk. J. Med. Sci. 2021, 51, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Fucà, G.; Guarini, V.; Antoniotti, C.; Morano, F.; Moretto, R.; Corallo, S.; Marmorino, F.; Lonardi, S.; Rimassa, L.; Sartore-Bianchi, A.; et al. The Pan-Immune-Inflammation Value is a new prognostic biomarker in metastatic colorectal cancer: Results from a pooled-analysis of the Valentino and TRIBE first-line trials. Br. J. Cancer 2020, 123, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B.; et al. Meta-analysis of Observational Studies in EpidemiologyA Proposal for Reporting. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Xi, H.; Wei, B.; Cui, J.; Zhang, K.; Li, H.; Cai, A.; Shen, W.; Li, J.; Rosell, R.; et al. Association between Liquid Biopsy and Prognosis of Gastric Cancer Patients: A Systematic Review and Meta-Analysis. Front. Oncol. 2019, 9, 1222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Şahin, A.B.; Cubukcu, E.; Ocak, B.; Deligonul, A.; Oyucu Orhan, S.; Tolunay, S.; Gokgoz, M.S.; Cetintas, S.; Yarbas, G.; Senol, K.; et al. Low pan-immune-inflammation-value predicts better chemotherapy response and survival in breast cancer patients treated with neoadjuvant chemotherapy. Sci. Rep. 2021, 11, 14662. [Google Scholar] [CrossRef]
- Fucà, G.; Beninato, T.; Bini, M.; Mazzeo, L.; Di Guardo, L.; Cimminiello, C.; Randon, G.; Apollonio, G.; Bisogno, I.; Del Vecchio, M.; et al. The Pan-Immune-Inflammation Value in Patients with Metastatic Melanoma Receiving First-Line Therapy. Target. Oncol. 2021, 16, 529–536. [Google Scholar] [CrossRef]
- Corti, F.; Lonardi, S.; Intini, R.; Salati, M.; Fenocchio, E.; Belli, C.; Borelli, B.; Brambilla, M.; Prete, A.A.; Quarà, V.; et al. The Pan-Immune-Inflammation Value in microsatellite instability-high metastatic colorectal cancer patients treated with immune checkpoint inhibitors. Eur. J. Cancer 2021, 150, 155–167. [Google Scholar] [CrossRef]
- Guven, D.C.; Yildirim, H.C.; Bilgin, E.; Aktepe, O.H.; Taban, H.; Sahin, T.K.; Cakir, I.Y.; Akin, S.; Dizdar, O.; Aksoy, S.; et al. PILE: A candidate prognostic score in cancer patients treated with immunotherapy. Clin. Transl. Oncol. 2021, 23, 1630–1636. [Google Scholar] [CrossRef]
- Efil, S.C.; Güner, G.; Guven, D.C.; Çelikten, B.; Çelebiyev, E.; Taban, H.; Akyol, A.; Kilickap, S.; Yalcin, Ş.; Dizdar, Ö. Prognostic and predictive value of tumor-infiltrating lymphocytes in combination with systemic inflammatory markers in colon cancer. Ann. Oncol. 2021, 32, S561. [Google Scholar] [CrossRef]
- Ligorio, F.; Fucà, G.; Zattarin, E.; Lobefaro, R.; Zambelli, L.; Leporati, R.; Rea, C.; Mariani, G.; Bianchi, G.V.; Capri, G.; et al. The pan-immune-inflammation-value predicts the survival of patients with human epidermal growth factor receptor 2 (Her2)—positive advanced breast cancer treated with first-line taxane-trastuzumab-pertuzumab. Cancers 2021, 13, 1964. [Google Scholar] [CrossRef] [PubMed]
- Susok, L.; Said, S.; Reinert, D.; Mansour, R.; Scheel, C.H.; Becker, J.C.; Gambichler, T. The pan-immune-inflammation value and systemic immune-inflammation index in advanced melanoma patients under immunotherapy. J. Cancer Res. Clin. Oncol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Gambichler, T.; Said, S.; Abu Rached, N.; Scheel, C.H.; Susok, L.; Stranzenbach, R.; Becker, J.C. Pan-immune-inflammation value independently predicts disease recurrence in patients with Merkel cell carcinoma. J. Cancer Res. Clin. Oncol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Sato, S.; Shimizu, T.; Ishizuka, M.; Suda, K.; Shibuya, N.; Hachiya, H.; Iso, Y.; Takagi, K.; Aoki, T.; Kubota, K. The preoperative pan-immune-inflammation value is a novel prognostic predictor for with stage I-III colorectal cancer patients undergoing surgery. Surg. Today 2022. [Google Scholar] [CrossRef]
- Chen, X.; Hong, X.; Chen, G.; Xue, J.; Huang, J.; Wang, F.; Ali, W.; Li, J.; Zhang, L. The Pan-Immune-Inflammation Value predicts the survival of patients with anaplastic lymphoma kinase-positive non-small cell lung cancer treated with first-line ALK inhibitor. Transl. Oncol. 2022, 17, 101338. [Google Scholar] [CrossRef]
- Baba, Y.; Nakagawa, S.; Toihata, T.; Harada, K.; Iwatsuki, M.; Hayashi, H.; Miyamoto, Y.; Yoshida, N.; Baba, H. Pan-immune-inflammation Value and Prognosis in Patients With Esophageal Cancer. Ann. Surg. Open 2022, 3, 113. [Google Scholar] [CrossRef]
- Lin, F.; Zhang, L.P.; Xie, S.Y.; Huang, H.Y.; Chen, X.Y.; Jiang, T.C.; Guo, L.; Lin, H.X. Pan-Immune-Inflammation Value: A New Prognostic Index in Operative Breast Cancer. Front. Oncol. 2022, 12, 830138. [Google Scholar] [CrossRef]
- Pérez-Martelo, M.; González-García, A.; Vidal-Ínsua, Y.; Blanco-Freire, C.; Brozos-Vázquez, E.M.; Abdulkader-Nallib, I.; Álvarez-Fernández, J.; Lázare-Iglesias, H.; García-Martínez, C.; Betancor, Y.Z.; et al. Clinical significance of baseline Pan-Immune-Inflammation Value and its dynamics in metastatic colorectal cancer patients under first-line chemotherapy. Sci. Rep. 2022, 12, 6893. [Google Scholar] [CrossRef]
- Zeng, R.; Liu, F.; Fang, C.; Yang, J.; Luo, L.; Yue, P.; Gao, B.; Dong, Y.; Xiang, Y. PIV and PILE Score at Baseline Predict Clinical Outcome of Anti-PD-1/PD-L1 Inhibitor Combined With Chemotherapy in Extensive-Stage Small Cell Lung Cancer Patients. Front. Immunol. 2021, 12, 724443. [Google Scholar] [CrossRef]
- Fisher, D.T.; Appenheimer, M.M.; Evans, S.S. The two faces of IL-6 in the tumor microenvironment. Semin. Immunol. 2014, 26, 38–47. [Google Scholar] [CrossRef] [Green Version]
- Aguilar-Cazares, D.; Chavez-Dominguez, R.; Carlos-Reyes, A.; Lopez-Camarillo, C.; Hernadez de la Cruz, O.N.; Lopez-Gonzalez, J.S. Contribution of Angiogenesis to Inflammation and Cancer. Front. Oncol. 2019, 9, 1399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basheer, A.S.; Abas, F.; Othman, I.; Naidu, R. Role of Inflammatory Mediators, Macrophages, and Neutrophils in Glioma Maintenance and Progression: Mechanistic Understanding and Potential Therapeutic Applications. Cancers 2021, 13, 4226. [Google Scholar] [CrossRef] [PubMed]
- Greten, F.R.; Grivennikov, S.I. Inflammation and Cancer: Triggers, Mechanisms, and Consequences. Immunity 2019, 51, 27–41. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Romero, K.; Rodríguez, R.M.; Amedei, A.; Barceló-Coblijn, G.; Lopez, D.H. Immune Landscape in Tumor Microenvironment: Implications for Biomarker Development and Immunotherapy. Int. J. Mol. Sci. 2020, 21, 5521. [Google Scholar] [CrossRef]
- Mwafy, S.E.; El-Guindy, D.M. Pathologic assessment of tumor-associated macrophages and their histologic localization in invasive breast carcinoma. J. Egypt. Natl. Cancer Inst. 2020, 32, 6. [Google Scholar] [CrossRef] [Green Version]
- Hu, C.; Liu, C.; Tian, S.; Wang, Y.; Shen, R.; Rao, H.; Li, J.; Yang, X.; Chen, B.; Ye, L. Comprehensive analysis of prognostic tumor microenvironment-related genes in osteosarcoma patients. BMC Cancer 2020, 20, 814. [Google Scholar] [CrossRef]
- Ye, J.H.; Wang, X.H.; Shi, J.J.; Yin, X.; Chen, C.; Chen, Y.; Wu, H.Y.; Jiong, S.; Sun, Q.; Zhang, M.; et al. Tumor-associated macrophages are associated with response to neoadjuvant chemotherapy and poor outcomes in patients with triple-negative breast cancer. J. Cancer 2021, 12, 2886–2892. [Google Scholar] [CrossRef]
- Ali, S.; Borin, T.F.; Piranlioglu, R.; Ara, R.; Lebedyeva, I.; Angara, K.; Achyut, B.R.; Arbab, A.S.; Rashid, M.H. Changes in the tumor microenvironment and outcome for TME-targeting therapy in glioblastoma: A pilot study. PLoS ONE 2021, 16, 0246646. [Google Scholar] [CrossRef] [PubMed]
- Marrugo-Ramírez, J.; Mir, M.; Samitier, J. Blood-Based Cancer Biomarkers in Liquid Biopsy: A Promising Non-Invasive Alternative to Tissue Biopsy. Int. J. Mol. Sci. 2018, 19, 2877. [Google Scholar] [CrossRef] [Green Version]
- Shoji, F.; Kozuma, Y.; Toyokawa, G.; Yamazaki, K.; Takeo, S. Complete Blood Cell Count-Derived Inflammatory Biomarkers in Early-Stage Non-Small-Cell Lung Cancer. Ann. Thorac. Cardiovasc. Surg. 2020, 26, 248–255. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.X.; Lin, J.P.; Xie, J.W.; Wang, J.B.; Lu, J.; Chen, Q.Y.; Cao, L.L.; Lin, M.; Tu, R.; Zheng, C.H.; et al. Complete blood count-based inflammatory score (CBCS) is a novel prognostic marker for gastric cancer patients after curative resection. BMC Cancer 2020, 20, 11. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Ni, X.; Tang, G. Prognostic Role of Platelet-to-Lymphocyte Ratio in Patients With Bladder Cancer: A Meta-Analysis. Front. Oncol. 2019, 9, 757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, J.; Yang, L.; Liu, D.; Li, W. Association of the neutrophil to lymphocyte ratio and clinical outcomes in patients with lung cancer receiving immunotherapy: A meta-analysis. BMJ Open 2020, 10, 035031. [Google Scholar] [CrossRef] [PubMed]
- Stone, R.L.; Nick, A.M.; McNeish, I.A.; Balkwill, F.; Han, H.D.; Bottsford-Miller, J.; Rupairmoole, R.; Armaiz-Pena, G.N.; Pecot, C.V.; Coward, J.; et al. Paraneoplastic thrombocytosis in ovarian cancer. N. Engl. J. Med. 2012, 366, 610–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haemmerle, M.; Taylor, M.L.; Gutschner, T.; Pradeep, S.; Cho, M.S.; Sheng, J.; Lyons, Y.M.; Nagaraja, A.S.; Dood, R.L.; Wen, Y.; et al. Platelets reduce anoikis and promote metastasis by activating YAP1 signaling. Nat. Commun. 2017, 8, 310. [Google Scholar] [CrossRef]
- Petty, A.J.; Yang, Y. Tumor-associated macrophages: Implications in cancer immunotherapy. Immunotherapy 2017, 9, 289–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shibutani, M.; Maeda, K.; Nagahara, H.; Fukuoka, T.; Nakao, S.; Matsutani, S.; Hirakawa, K.; Ohira, M. The peripheral monocyte count is associated with the density of tumor-associated macrophages in the tumor microenvironment of colorectal cancer: A retrospective study. BMC Cancer 2017, 17, 404. [Google Scholar] [CrossRef] [PubMed]
- Dumitru, C.A.; Lang, S.; Brandau, S. Modulation of neutrophil granulocytes in the tumor microenvironment: Mechanisms and consequences for tumor progression. Semin. Cancer Biol. 2013, 23, 141–148. [Google Scholar] [CrossRef]
- Deryugina, E.I.; Zajac, E.; Juncker-Jensen, A.; Kupriyanova, T.A.; Welter, L.; Quigley, J.P. Tissue-Infiltrating Neutrophils Constitute the Major In Vivo Source of Angiogenesis-Inducing MMP-9 in the Tumor Microenvironment. Neoplasia 2014, 16, 771–788. [Google Scholar] [CrossRef] [Green Version]
- Galli, F.; Aguilera, J.V.; Palermo, B.; Markovic, S.N.; Nisticò, P.; Signore, A. Relevance of immune cell and tumor microenvironment imaging in the new era of immunotherapy. J. Exp. Clin. Cancer Res. 2020, 39, 89. [Google Scholar] [CrossRef]
- Bigot, F.; Castanon, E.; Baldini, C.; Hollebecque, A.; Carmona, A.; Postel-Vinay, S.; Angevin, E.; Armand, J.P.; Ribrag, V.; Aspeslagh, S.; et al. Prospective validation of a prognostic score for patients in immunotherapy phase I trials: The Gustave Roussy Immune Score (GRIm-Score). Eur. J. Cancer 2017, 84, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Garrido-Laguna, I.; Janku, F.; Vaklavas, C.; Falchook, G.S.; Fu, S.; Hong, D.S.; Naing, A.; Tsimberidou, A.M.; Wen, S.; Kurzrock, R. Validation of the Royal Marsden Hospital prognostic score in patients treated in the Phase I Clinical Trials Program at the MD Anderson Cancer Center. Cancer 2012, 118, 1422–1428. [Google Scholar] [CrossRef] [PubMed]
- Huber, V.; Vallacchi, V.; Fleming, V.; Hu, X.; Cova, A.; Dugo, M.; Shahaj, E.; Sulsenti, R.; Vergani, E.; Filipazzi, P. Tumor-derived microRNAs induce myeloid suppressor cells and predict immunotherapy resistance in melanoma. J. Clin. Investig. 2018, 128, 5505–5516. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lead Author, Year | Country | Sample Size | Treatment | PIV Cut-Off Value | Cut-Off Selection | Tumor Type | Tumor Stage | Adjustment Factors | Outcome | Additional Comments |
|---|---|---|---|---|---|---|---|---|---|---|
| Fucà, 2020, [32] | Italy | 438 | Tribe study: FOLFIRI + Bevacizumab vs. FOLFOXIRI + Bevacizumab Valentino study: mFOLFOX6 + Panitumumab | 390 | MSR | CRC | IV | - ECOG - Prior adjuvant treatment - Primary tumor resected - Synchronous metastases - Number of metastatic sites - Primary tumor sidedness - RAS/BRAF status - NLR - PLT - Monocyte - SII | - PFS - OS | PIV outperformed the other immune-inflammatory biomarkers in regression model |
| Corti, 2021, [38] | Italy | 163 | - Nivolumab plus ipilimumab (32.5%) - Nivolumab (47.3%) - Pembrolizumab (9.8%) - Dostarlimab (10.4%) | 492 | MSR | CRC | IV | - ECOG - ICI regimen | - PFS - OS - CBR | Early PIV increase was independently correlated with clinical benefit (aOR: 0.23, 95% CI 0.08–0.66, p = 0.007) |
| Fucà, 2021, [37] | Italy | 228 | ICI: - Nivolumab (61.3%) - Pembrolizumab (38.7%) TT: - Vemurafenib (22.0%) - Dabrafenib (2.8%) - Vemurafenib plus cobimetinib (10.1%) - Dabrafenib plus trametinib (65.1%) | 600 | MSR | Melanoma | IV | - ECOG - M substage - Metastatic sites - LDH - Steroids use | - PFS - OS - Best response | High PIV was associated with primary resistance to both targeted therapy (OR: 8.42; 95% CI 2.50–34.5, p < 0.001) and ICI (OR: 3.98, 95% CI 1.45–12.32, p = 0.005) |
| Guven, 2021, [39] | Turkey | 120 | - Nivolumab (78.3%) - Atezolizumab (17.5%) - Pembrolizumab (4.2%) | 513.4 | Median value | RCC, NSCLC, Melanoma, Other | IV | - ECOG - LDH levels - Liver metastasis - BMI category | - PFS - OS | A model combining PIV, ECOG status, and LDH levels (PILE Score) was able to predict 12-week PFS and 24-week OS |
| Ligorio, 2021, [41] | Italy | 57 | - Taxane-Transtuzumab - Pertuzumab | 285 | Median value | Breast Cancer | IV | - Number of metastatic sites - Visceral metastasis - Brain metastasis | - PFS - OS - Response | PIV outperformed MLR, PLR, and NLR in predicting OS |
| Sahin, 2021, [36] | Turkey | 743 | - Anthracycline plus taxane (68.6%) - Anthracycline-based regimens (27.5%) - Taxane-based regimens (3.9%) | 306.4 | ROC curve | Breast Cancer | I-IV | - Clinical T stage - NLR - MLR - PLR - ER status - Her-2 status - Ki-67 index | - pCR - DFS - OS | Pre-treatment PIV appears to be a predictor for pCR and survival, outperforming NLR, MLR, PLR in predicting pCR |
| Zeng, 2021, [49] | China | 53 | Control group of NCT03041311 (53 patients): carboplatin, etoposide, and atezolizumab Validation group (84 patients): - PD-1 antibody (29.8%) - PD-L1 antibody (70.2%) | 581.95 | Median value | SCLC | Extensive Stage | - LDH | - PFS - OS - DCR - DCB | Higher PILE score was associated with worse treatment efficacy (DCR: 84.21% vs. 100%, p = 0.047, DCB rate: 10% vs. 48.5%, p = 0.060) |
| Efil, 2021, [40] | Turkey | 304 | Adjuvant chemotherapy (52%) | 491 | Median | CRC | II-III | - Age - Stage | - DFS | A model combining PIV and CD8 + TIL density was able to predict DFS |
| Sato, 2022, [44] | Japan | 758 | Adjuvant chemotherapy (30%) | 376 | ROC curve | CRC | I-III | - Age - CA19-9 - CEA - AGR - Post-operative complication | - RFS - OS | A high preoperative PIV was significantly associated with depth of tumor invasion and advanced TNM stage (II, III) |
| Gambichler, 2022, [43] | Germany | 49 | N/A | 372 | ROC curve | MCC | I-III | - Age > 75 - Disease stage - Elevated CRP | - Recurrence - OS | An association between PIV levels and stage was present |
| Susok, 2022, [42] | Germany | 62 | - Nivolumab (38.7%) - Pembrolizumab (24.5%) - Ipilimumab (14.5%) - Nivolumab plus Ipilimumab (22.6%) | 455 | ROC curve | Melanoma | III-IV | N/A | - PFS - DSS - Best response | SII and PIV were not significantly associated with best response to ICI treatment (p = 0.87/0.64), PFS (p = 0.73/0.91), and melanoma-specific survival (p = 0.13/0.17). |
| Chen, 2022, [45] | China | 94 | - Crizotinib (89.4%) - Alectinib (10.6%) - Ceritinib (1.0%) | 364 | Median | Lung Cancer | III-IV | - Liver metastasis | - PFS - OS | Although PIV, NLR, PLR, and SII were associated with poor median OS, only higher PIV was independently associated with poor survival outcomes (HR = 4.70, 95% Cl: 2.00–11.02, p < 0.001). |
| Baba, 2022, [46] | Japan | 433 (Validation Cohort) | N/A | 164.6 | ROC | Esophageal Cancer | I-IV | - Preoperative therapy - Pathological stage | - OS | The PIV-high cases were significantly associated with a low TIL status (p < 0.001) and low CD8-positive cell counts (p = 0.011) |
| Lin, 2022, [47] | China | 1312 | Adjuvant chemotherapy (81.3%) | 310.2 | MSR | Breast Cancer | I-III | - Stage (T and N) - PR status - Ki-67 - Histopathological type | - OS | The prognostic model showed a good discriminating ability for OS prediction, with a C-index of 0.759 (95% CI 0.715–0.802) |
| Perez-Martelo, 2022, [48] | Spain | 130 | - Oxaliplatin-based regimen (74%) - Non-oxaliplatin-based regimen (26%) | 424.05 | MSR | CRC | IV | - CEA - ECOG-PS - Primary tumor location - Lymph node metastases - Primary tumor resection | - PFS - OS - DCR - ORR | - Baseline PIV was not correlated either with DCR or ORR |
| Lead Author, Year | Selection | Comparability | Exposure/Outcome | Reference |
|---|---|---|---|---|
| Fucà, 2020 | **** | ** | ** | [32] |
| Corti, 2021 | *** | ** | *** | [38] |
| Fucà, 2021 | **** | ** | *** | [37] |
| Guven, 2021 | **** | ** | *** | [39] |
| Ligorio, 2021 | *** | ** | *** | [41] |
| Sahin, 2021 | *** | ** | *** | [36] |
| Zeng, 2021 | **** | ** | *** | [49] |
| Efil, 2021 | No full-text data available | [40] | ||
| Sato, 2022 | *** | ** | *** | [44] |
| Gambichler, 2022 | *** | ** | *** | [43] |
| Susok, 2022 | *** | * | ** | [42] |
| Chen, 2022 | **** | ** | ** | [45] |
| Baba, 2022 | **** | ** | ** | [46] |
| Lin, 2022 | **** | ** | *** | [47] |
| Perez-Martelo, 2022 | **** | ** | *** | [48] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guven, D.C.; Sahin, T.K.; Erul, E.; Kilickap, S.; Gambichler, T.; Aksoy, S. The Association between the Pan-Immune-Inflammation Value and Cancer Prognosis: A Systematic Review and Meta-Analysis. Cancers 2022, 14, 2675. https://doi.org/10.3390/cancers14112675
Guven DC, Sahin TK, Erul E, Kilickap S, Gambichler T, Aksoy S. The Association between the Pan-Immune-Inflammation Value and Cancer Prognosis: A Systematic Review and Meta-Analysis. Cancers. 2022; 14(11):2675. https://doi.org/10.3390/cancers14112675
Chicago/Turabian StyleGuven, Deniz Can, Taha Koray Sahin, Enes Erul, Saadettin Kilickap, Thilo Gambichler, and Sercan Aksoy. 2022. "The Association between the Pan-Immune-Inflammation Value and Cancer Prognosis: A Systematic Review and Meta-Analysis" Cancers 14, no. 11: 2675. https://doi.org/10.3390/cancers14112675
APA StyleGuven, D. C., Sahin, T. K., Erul, E., Kilickap, S., Gambichler, T., & Aksoy, S. (2022). The Association between the Pan-Immune-Inflammation Value and Cancer Prognosis: A Systematic Review and Meta-Analysis. Cancers, 14(11), 2675. https://doi.org/10.3390/cancers14112675