
Tooth Loss and Risk of Lung Cancer among Urban Chinese Adults: A Cohort Study with Meta-Analysis

 ,
,  , ,
, ,  , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Study Population
2.2. Ascertainment of Incident Lung Cancer Cases
2.3. Statistical Methods for Cohort Analyses
2.4. Meta-Analysis
3. Results
3.1. Cohort Analyses for the SMHS and SWHS
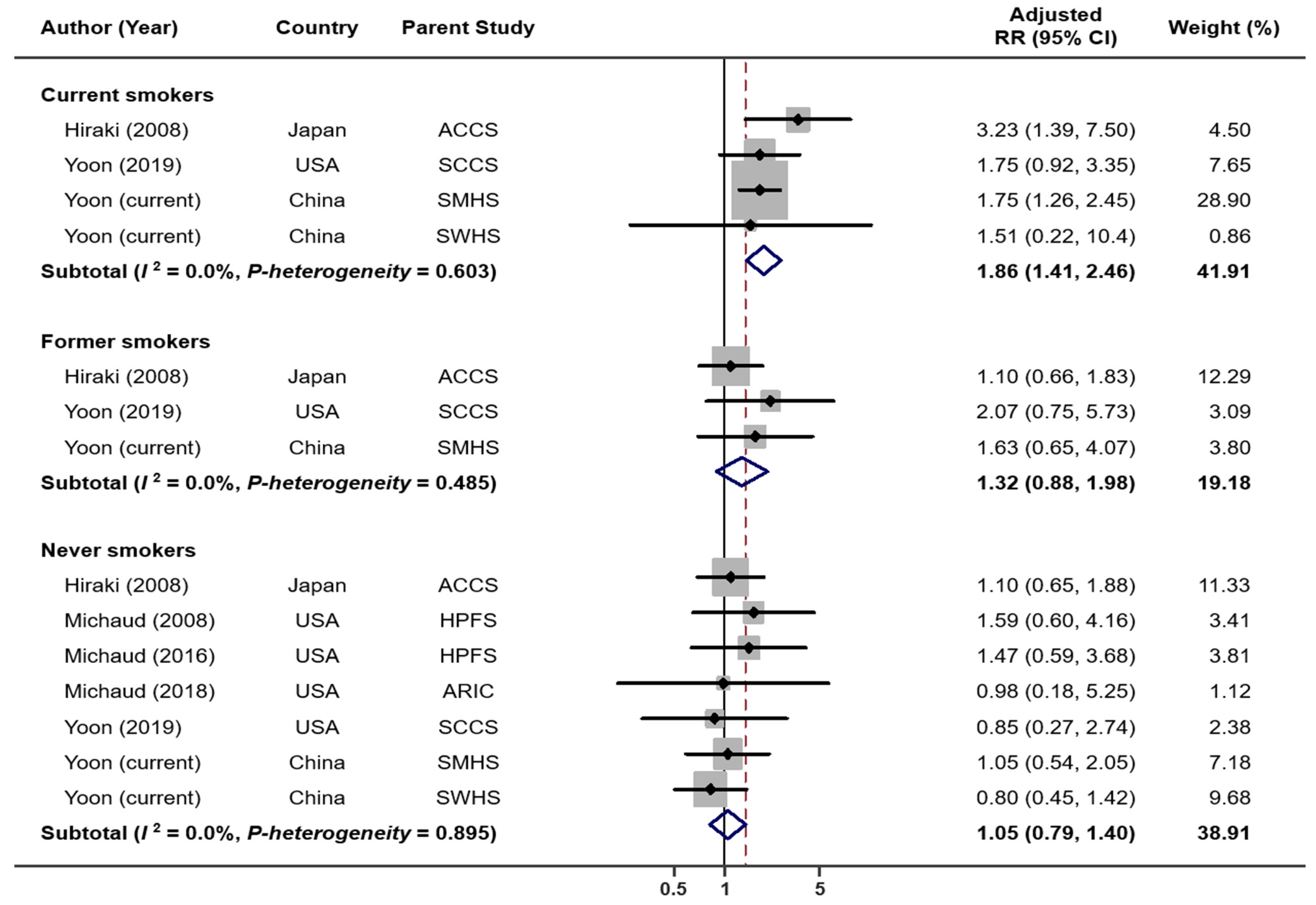
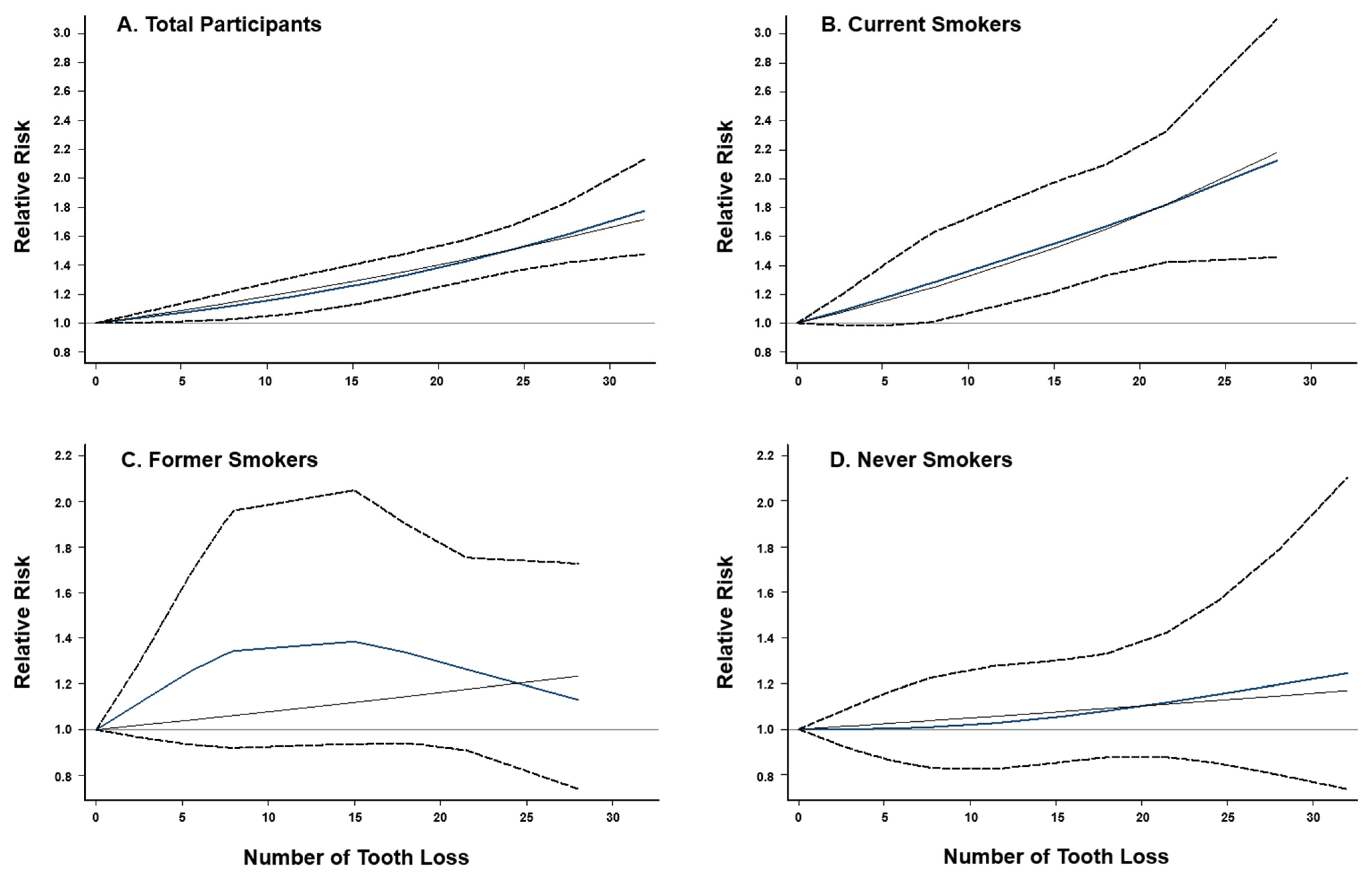
3.2. Results of Meta-Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Platz, E.A. Reducing Cancer Burden in the Population: An Overview of Epidemiologic Evidence to Support Policies, Systems, and Environmental Changes. Epidemiol. Rev. 2017, 39, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, M.; York, B.R.; Michaud, D.S. Oral Health and Cancer. Curr. Oral. Health Rep. 2019, 6, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Ren, H.G.; Luu, H.N.; Cai, H.; Xiang, Y.B.; Steinwandel, M.; Gao, Y.T.; Hargreaves, M.; Zheng, W.; Blot, W.J.; Long, J.R.; et al. Oral Health and Risk of Colorectal Cancer: Results from Three Cohort Studies and a Meta-Analysis. Ann. Oncol. 2016, 27, 1329–1336. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Leng, W.; Zhao, L.; Deng, C.; Xu, C.; Wang, J.; Wang, Y.; Peng, X. Tooth Loss and Cancer Risk: A Dose-Response Meta Analysis of Prospective Cohort Studies. Oncotarget 2017, 9, 15090–15100. [Google Scholar] [CrossRef] [Green Version]
- Hiraki, A.; Matsuo, K.; Suzuki, T.; Kawase, T.; Tajima, K. Teeth Loss and Risk of Cancer at 14 Common Sites in Japanese. Cancer Epidemiol. Biomark. Prev. 2008, 17, 1222–1227. [Google Scholar] [CrossRef] [Green Version]
- Michaud, D.S.; Liu, Y.; Meyer, M.; Giovannucci, E.; Joshipura, K. Periodontal Disease, Tooth Loss, and Cancer Risk in Male Health Professionals: A Prospective Cohort Study. Lancet Oncol. 2008, 9, 550–558. [Google Scholar] [CrossRef] [Green Version]
- Mai, X.; LaMonte, M.J.; Hovey, K.M.; Nwizu, N.; Freudenheim, J.L.; Tezal, M.; Scannapieco, F.; Hyland, A.; Andrews, C.A.; Genco, R.J.; et al. History of Periodontal Disease Diagnosis and Lung Cancer Incidence in the Women’s Health Initiative Observational Study. Cancer Causes Control 2014, 25, 1045–1053. [Google Scholar] [CrossRef] [Green Version]
- Michaud, D.S.; Kelsey, K.T.; Papathanasiou, E.; Genco, C.A.; Giovannucci, E. Periodontal Disease and Risk of All Cancers among Male Never Smokers: An Updated Analysis of the Health Professionals Follow-up Study. Ann. Oncol. 2016, 27, 941–947. [Google Scholar] [CrossRef]
- Michaud, D.S.; Lu, J.; Peacock-Villada, A.Y.; Barber, J.R.; Joshu, C.E.; Prizment, A.E.; Beck, J.D.; Offenbacher, S.; Platz, E.A. Periodontal Disease Assessed Using Clinical Dental Measurements and Cancer Risk in the ARIC Study. J. Natl. Cancer Inst. 2018, 110, 843–854. [Google Scholar] [CrossRef]
- Yoon, H.S.; Wen, W.; Long, J.; Zheng, W.; Blot, W.J.; Cai, Q. Association of Oral Health with Lung Cancer Risk in a Low-Income Population of African Americans and European Americans in the Southeastern United States. Lung Cancer 2019, 127, 90–95. [Google Scholar] [CrossRef]
- Grivennikov, S.I.; Greten, F.R.; Karin, M. Immunity, Inflammation, and Cancer. Cell 2010, 140, 883–899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scannapieco, F.A. Role of Oral Bacteria in Respiratory Infection. J. Periodontol. 1999, 70, 793–802. [Google Scholar] [CrossRef] [PubMed]
- Bergström, J.; Eliasson, S.; Dock, J. A 10-Year Prospective Study of Tobacco Smoking and Periodontal Health. J. Periodontol. 2000, 71, 1338–1347. [Google Scholar] [CrossRef] [PubMed]
- Souto, M.L.S.; Rovai, E.S.; Villar, C.C.; Braga, M.M.; Pannuti, C.M. Effect of Smoking Cessation on Tooth Loss: A Systematic Review with Meta-Analysis. BMC Oral. Health. 2019, 19, 245. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Peters, B.A.; Dominianni, C.; Zhang, Y.; Pei, Z.; Yang, L.; Ma, Y.; Purdue, M.P.; Jacobs, E.J.; Gapstur, S.M.; et al. Cigarette Smoking and the Oral Microbiome in a Large Study of American Adults. ISME J. 2016, 10, 2435–2446. [Google Scholar] [CrossRef]
- Yang, Y.; Zheng, W.; Cai, Q.Y.; Shrubsole, M.J.; Pei, Z.; Brucker, R.; Steinwandel, M.D.; Bordenstein, S.R.; Li, Z.; Blot, W.J.; et al. Cigarette Smoking and Oral Microbiota in Low-Income and African-American Populations. J. Epidemiol. Community Health 2019, 73, 1108–1115. [Google Scholar] [CrossRef]
- Macgregor, I.D. Effects of Smoking on Oral Ecology. A Review of the Literature. Clin. Prev. Dent. 1989, 11, 3–7. [Google Scholar]
- Yang, J.J.; Yu, D.; Wen, W.; Shu, X.O.; Saito, E.; Rahman, S.; Gupta, P.C.; He, J.; Tsugane, S.; Xiang, Y.-B.; et al. Tobacco Smoking and Mortality in Asia: A Pooled Meta-Analysis. JAMA Netw. Open 2019, 2, e191474. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.; Luo, X.; Xu, S.; Liu, W.; Ding, F.; Zhang, X.; Wang, L.; Liu, J.; Hu, J.; Wang, W. Trends in Smoking Prevalence and Implication for Chronic Diseases in China: Serial National Cross-Sectional Surveys from 2003 to 2013. Lancet Respir. Med. 2019, 7, 35–45. [Google Scholar] [CrossRef]
- Qi, X.; Qu, X.; Wu, B. Urban-Rural Disparities in Dental Services Utilization among Adults in China’s Megacities. Front. Oral. Health 2021, 2, 673296. [Google Scholar] [CrossRef]
- Shu, X.O.; Li, H.; Yang, G.; Gao, J.; Cai, H.; Takata, Y.; Zheng, W.; Xiang, Y.B. Cohort Profile: The Shanghai Men’s Health Study. Int. J. Epidemiol. 2015, 44, 810–818. [Google Scholar] [CrossRef] [PubMed]
- Zheng, W.; Chow, W.H.; Yang, G.; Jin, F.; Rothman, N.; Blair, A.; Li, H.L.; Wen, W.; Ji, B.T.; Li, Q.; et al. The Shanghai Women’s Health Study: Rationale, Study Design, and Baseline Characteristics. Am. J. Epidemiol. 2005, 162, 1123–1131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ansai, T.; Takata, Y.; Yoshida, A.; Soh, I.; Awano, S.; Hamasaki, T.; Sogame, A.; Shimada, N. Association between Tooth Loss and Orodigestive Cancer Mortality in an 80-Year-Old Community-Dwelling Japanese Population: A 12-Year Prospective Study. BMC Public Health 2013, 13, 814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goto, Y.; Wada, K.; Uji, T.; Koda, S.; Mizuta, F.; Yamakawa, M.; Nagata, C. Number of Teeth and All-Cause and Cancer Mortality in a Japanese Community: The Takayama Study. J. Epidemiol. 2020, 30, 213–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hujoel, P.P.; Drangsholt, M.; Spiekerman, C.; Weiss, N.S. An Exploration of the Periodontitis-Cancer Association. Ann. Epidemiol. 2003, 13, 312–316. [Google Scholar] [CrossRef]
- Tu, Y.K.; Galobardes, B.; Smith, G.D.; McCarron, P.; Jeffreys, M.; Gilthorpe, M.S. Associations between Tooth Loss and Mortality Patterns in the Glasgow Alumni Cohort. Heart 2007, 93, 1098–1103. [Google Scholar] [CrossRef] [Green Version]
- Lam, M.; Zhu, J.W.; Tadrous, M.; Drucker, A.M. Association Between Topical Calcineurin Inhibitor Use and Risk of Cancer, Including Lymphoma, Keratinocyte Carcinoma, and Melanoma: A Systematic Review and Meta-Analysis. JAMA Dermatol. 2021, 157, 549–558. [Google Scholar] [CrossRef]
- Eyawo, O.; Brockman, G.; Goldsmith, C.H.; Hull, M.W.; Lear, S.A.; Bennett, M.; Guillemi, S.; Franco-Villalobos, C.; Adam, A.; Mills, E.J.; et al. Risk of Myocardial Infarction among People Living with HIV: An Updated Systematic Review and Meta-Analysis. BMJ Open 2019, 9, e025874. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trials. Control. Clin. Trials. 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Macaskill, P.; Walter, S.D.; Irwig, L. A Comparison of Methods to Detect Publication Bias in Meta-Analysis. Stat. Med. 2001, 20, 641–654. [Google Scholar] [CrossRef] [PubMed]
- Orsini, N.; Li, R.; Wolk, A.; Khudyakov, P.; Spiegelman, D. Meta-Analysis for Linear and Nonlinear Dose-Response Relations: Examples, an Evaluation of Approximations, and Software. Am. J. Epidemiol. 2012, 175, 66–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Zhu, B.; Wu, C.; Lin, R.; Zhang, X. Periodontal Disease and Tooth Loss Are Associated with Lung Cancer Risk. Biomed Res. Int. 2020, 2020, 5107696. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, T.; Walter, C.; Oluwagbemigun, K.; Bergmann, M.; Pischon, T.; Pischon, N.; Boeing, H. Smoking, Smoking Cessation, and Risk of Tooth Loss: The EPIC-Potsdam Study. J. Dent. Res. 2015, 94, 1369–1375. [Google Scholar] [CrossRef] [PubMed]
- Mai, X.; Wactawski-Wende, J.; Hovey, K.M.; LaMonte, M.J.; Chen, C.; Tezal, M.; Genco, R.J. Associations between Smoking and Tooth Loss According to the Reason for Tooth Loss: The Buffalo OsteoPerio Study. J. Am. Dent. Assoc. 2013, 144, 252–265. [Google Scholar] [CrossRef]
- Cunningham, T.J.; Eke, P.I.; Ford, E.S.; Agaku, I.T.; Wheaton, A.G.; Croft, J.B. Cigarette Smoking, Tooth Loss, and Chronic Obstructive Pulmonary Disease: Findings from the Behavioral Risk Factor Surveillance System. J. Periodontol. 2016, 87, 385–394. [Google Scholar] [CrossRef] [Green Version]
- Rad, M.; Kakoie, S.; Niliye Brojeni, F.; Pourdamghan, N. Effect of Long-Term Smoking on Whole-Mouth Salivary Flow Rate and Oral Health. J. Dent. Res. Dent. Clin. Dent. Prospect. 2010, 4, 110–114. [Google Scholar]
- You, Z.; Cushman, M.; Jenny, N.S.; Howard, G.; REGARDS. Tooth Loss, Systemic Inflammation, and Prevalent Stroke among Participants in the Reasons for Geographic and Racial Difference in Stroke (REGARDS) Study. Atherosclerosis 2009, 203, 615–619. [Google Scholar] [CrossRef] [Green Version]
- Meisel, P.; Wilke, P.; Biffar, R.; Holtfreter, B.; Wallaschofski, H.; Kocher, T. Total Tooth Loss and Systemic Correlates of Inflammation: Role of Obesity. Obesity 2012, 20, 644–650. [Google Scholar] [CrossRef]
- Meyer, M.S.; Joshipura, K.; Giovannucci, E.; Michaud, D.S. A Review of the Relationship between Tooth Loss, Periodontal Disease, and Cancer. Cancer Causes Control 2008, 19, 895–907. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, K.B.; Hotchkiss, J.H.; Roe, D.A. Quantitative Relationship between Oral Nitrate-Reducing Activity and the Endogenous Formation of N-Nitrosoamino Acids in Humans. Food Chem. Toxicol. 1991, 29, 751–755. [Google Scholar] [CrossRef]
- Nair, J.; Ohshima, H.; Nair, U.J.; Bartsch, H. Endogenous Formation of Nitrosamines and Oxidative DNA-Damaging Agents in Tobacco Users. Crit. Rev. Toxicol. 1996, 26, 149–161. [Google Scholar] [CrossRef] [PubMed]
- Risch, H.A. Etiology of Pancreatic Cancer, with a Hypothesis Concerning the Role of N-Nitroso Compounds and Excess Gastric Acidity. J. Natl. Cancer Inst. 2003, 95, 948–960. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Yang, Y.; Xie, H.; Wang, X.; Wu, J.; Long, J.; Courtney, R.; Shu, X.-O.; Zheng, W.; Blot, W.J.; et al. Association of Oral Microbiota with Lung Cancer Risk in a Low-Income Population in the Southeastern USA. Cancer Causes Control 2021, 32, 1423–1432. [Google Scholar] [CrossRef] [PubMed]
- Hosgood, H.D.; Cai, Q.; Hua, X.; Long, J.; Shi, J.; Wan, Y.; Yang, Y.; Abnet, C.; Bassig, B.A.; Hu, W.; et al. Variation in Oral Microbiome Is Associated with Future Risk of Lung Cancer among Never-Smokers. Thorax 2021, 76, 256–263. [Google Scholar] [CrossRef]
- Yan, X.; Yang, M.; Liu, J.; Gao, R.; Hu, J.; Li, J.; Zhang, L.; Shi, Y.; Guo, H.; Cheng, J.; et al. Discovery and Validation of Potential Bacterial Biomarkers for Lung Cancer. Am. J. Cancer Res. 2015, 5, 3111–3122. [Google Scholar]
- Gao, S.; Li, N.; Wang, S.; Zhang, F.; Wei, W.; Li, N.; Bi, N.; Wang, Z.; He, J. Lung Cancer in People’s Republic of China. J. Thorac. Oncol. 2020, 15, 1567–1576. [Google Scholar] [CrossRef]
- De Groot, P.M.; Wu, C.C.; Carter, B.W.; Munden, R.F. The Epidemiology of Lung Cancer. Transl. Lung Cancer Res. 2018, 7, 220–233. [Google Scholar] [CrossRef]
- Rivera, G.A.; Wakelee, H. Lung Cancer in Never Smokers. Adv. Exp. Med. Biol. 2016, 893, 43–57. [Google Scholar]
- Kailembo, A.; Preet, R.; Stewart Williams, J. Common Risk Factors and Edentulism in Adults, Aged 50 Years and over, in China, Ghana, India and South Africa: Results from the WHO Study on Global AGEing and Adult Health (SAGE). BMC Oral. Health 2016, 17, 29. [Google Scholar] [CrossRef] [Green Version]
- Warren, J.J.; Levy, S.M.; Hand, J.S. The Accuracy of Tooth Loss Data Collected by Nurses. Spec. Care Dent. 1999, 19, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Nwizu, N.N.; Marshall, J.R.; Moysich, K.; Genco, R.J.; Hovey, K.M.; Mai, X.; LaMonte, M.J.; Freudenheim, J.L.; Wactawski-Wende, J. Periodontal Disease and Incident Cancer Risk among Postmenopausal Women: Results from the Women’s Health Initiative Observational Cohort. Cancer Epidemiol. Biomark. Prev. 2017, 26, 1255–1265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, Q.Y.; Wu, G.M.; Qian, G.S.; Hu, C.P.; Zhou, J.Y.; Chen, L.A.; Li, W.M.; Li, S.Y.; Wang, K.; Wang, Q.; et al. Prevention and Management of Lung Cancer in China. Cancer 2015, 121 (Suppl. 17), 3080–3088. [Google Scholar] [CrossRef] [PubMed]
- Cao, M.; Chen, W. Epidemiology of Lung Cancer in China: Epidemiology of Lung Cancer in China. Thorac. Cancer 2019, 10, 3–7. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Men (SMHS) | Women (SWHS) | |||||
|---|---|---|---|---|---|---|
| Characteristics | LC Cases (n = 613) | Non-cases (n = 49,255) | p-Value † | LC Cases (n = 360) | Non-Cases (n = 43,949) | p-Value † |
| Age, a mean (SD) | 65.8 (9.6) | 60.8 (9.6) | <0.001 | 64.1 (8.3) | 60.8 (8.2) | <0.001 |
| Education | ||||||
| Less than high school | 314 (51.2) | 19,740 (40.1) | <0.001 | 203 (56.4) | 25,084 (57.1) | <0.001 |
| Completed high school | 176 (28.7) | 17,925 (36.4) | 84 (23.3) | 13,127 (29.9) | ||
| More than high school | 123 (20.1) | 11,590 (23.5) | 73 (20.3) | 5738 (13.1) | ||
| Income b | ||||||
| Low | 65 (10.6) | 6209 (12.6) | 0.03 | 57 (15.8) | 6318 (14.4) | 0.72 |
| Medium | 504 (82.2) | 38,358 (77.9) | 270 (75.0) | 33,372 (75.9) | ||
| High | 44 (7.2) | 4688 (9.5) | 33 (9.2) | 4259 (9.7) | ||
| Smoking Status | ||||||
| Never | 97 (15.8) | 15,079 (30.6) | <0.001 | 339 (94.2) | 43,067 (98.0) | <0.001 |
| Former | 85 (13.9) | 5210 (10.6) | 3 (0.8) | 118 (0.3) | ||
| Current | 431 (70.3) | 28,966 (58.8) | 18 (5.0) | 764 (1.7) | ||
| Pack-years, c mean (SD) | 33.6 (18.9) | 24.1 (15.8) | <0.001 | 17.2 (11.7) | 8.0 (10.2) | <0.001 |
| Alcohol consumption d | ||||||
| None | 371 (60.5) | 32,904 (66.8) | <0.001 | 354 (98.3) | 43,097 (98.1) | 0.91 |
| Low-to-moderate | 132 (21.5) | 9866 (20.0) | 5 (1.4) | 677 (1.5) | ||
| Heavy | 110 (18.0) | 6485 (13.2) | 1 (0.3) | 175 (0.4) | ||
| BMI (kg/m2) | ||||||
| Under weight, <18.5 | 36 (5.9) | 1996 (4.1) | 0.02 | 3 (0.8) | 1373 (3.1) | 0.04 |
| Normal, 18.5–24.9 | 404 (65.9) | 30,889 (62.7) | 237 (65.8) | 27,577 (62.8) | ||
| Overweight, 25.0–29.9 | 159 (25.9) | 15,112 (30.7) | 99 (27.5) | 12,960 (29.5) | ||
| Obese, ≥30 | 14 (2.3) | 1258 (2.6) | 21 (5.8) | 2039 (4.6) | ||
| COPD e | ||||||
| No | 496 (80.9) | 44,095 (89.5) | <0.001 | 310 (86.1) | 38,441 (87.5) | 0.44 |
| Yes | 117 (19.1) | 5160 (10.5) | 50 (13.9) | 5508 (12.5) | ||
| Menopausal status | ||||||
| Pre | - | - | N.A. | 144 (40.0) | 25,650 (58.4) | <0.001 |
| Post | - | - | 216 (60.0) | 18,299 (41.6) | ||
| Number of tooth loss | ||||||
| None | 87 (14.2) | 13,446 (27.3) | <0.001 | 94 (26.1) | 12,859 (29.3) | 0.03 |
| 1–5 | 211 (34.4) | 20,430 (41.5) | 174 (48.3) | 22,565 (51.3) | ||
| 6–10 | 86 (14.0) | 5663 (11.5) | 75 (20.8) | 6844 (15.6) | ||
| >10 | 229 (37.4) | 9716 (19.7) | 17 (4.7) | 1681 (3.8) | ||
| Model 1 b | Model 2 c | Model 3 d | ||||
|---|---|---|---|---|---|---|
| Number of Tooth Loss | Incident Cases, n | Person- Years | Incidence Rate a | HR (95% CI) | HR (95% CI) | HR (95% CI) |
| Men | ||||||
| None | 87 | 91,068 | 95.5 | 1 (ref.) | 1 (ref.) | 1 (ref.) |
| 1–5 | 211 | 137,070 | 153.9 | 1.29 (1.00–1.66) | 1.19 (0.92–1.54) | 1.19 (0.92–1.54) |
| 6–10 | 86 | 37,239 | 230.9 | 1.60 (1.17–2.19) | 1.32 (0.96–1.80) | 1.30 (0.95–1.78) |
| > 10 | 229 | 62,592 | 365.9 | 2.23 (1.70–2.93) | 1.65 (1.25–2.18) | 1.59 (1.21–2.11) |
| p for trend | <0.001 | <0.001 | <0.001 | |||
| Women | ||||||
| None | 94 | 102,588 | 91.6 | 1 (ref.) | 1 (ref.) | 1 (ref.) |
| 1–5 | 174 | 178,702 | 97.4 | 0.86 (0.67–1.11) | 0.86 (0.66–1.11) | 0.87 (0.67–1.12) |
| 6–10 | 75 | 53,650 | 139.8 | 1.00 (0.73–1.38) | 1.00 (0.72–1.38) | 1.01 (0.73–1.40) |
| >10 | 17 | 13,139 | 129.4 | 0.86 (0.50–1.46) | 0.83 (0.49–1.42) | 0.86 (0.50–1.46) |
| p for trend | 0.81 | 0.75 | 0.84 |
| Current | Former | Never | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Number of tooth loss | Incident Cases, n | Person- Years | Incidence Rate a | HR (95% CI) b | Incident Cases, n | Person- Years | Incidence Rate a | HR (95% CI) b | Incident Cases, n | Person- Years | Incidence Rate a | HR (95% CI) b |
| Men | ||||||||||||
| None | 62 | 57,533 | 107.8 | 1 (ref.) | 6 | 6497 | 92.4 | 1 (ref.) | 19 | 27,038 | 70.3 | 1 (ref.) |
| 1–5 | 147 | 81,974 | 179.3 | 1.23 (0.91–1.67) | 21 | 13,014 | 161.4 | 1.20 (0.48–3.00) | 43 | 42,082 | 102.2 | 1.11 (0.64–1.94) |
| 6–10 | 62 | 21,027 | 294.9 | 1.44 (1.00–2.08) | 13 | 4449 | 292.2 | 1.44 (0.53–3.94) | 11 | 11,763 | 93.5 | 0.85 (0.39–1.84) |
| > 10 | 160 | 32,799 | 487.8 | 1.75 (1.26–2.45) | 45 | 10,102 | 445.5 | 1.63 (0.65–4.07) | 24 | 19,691 | 121.9 | 1.05 (0.54–2.05) |
| p for trend | <0.001 | 0.18 | 0.92 | |||||||||
| p-interaction | 0.04 | |||||||||||
| Women | ||||||||||||
| None | 2 | 1320 | 151.5 | 1 (ref.) | 0 | 159 | - | 1 (ref.) | 92 | 101,110 | 91.0 | 1 (ref.) |
| 1–5 | 6 | 2974 | 201.7 | 0.88 (0.16–4.70) | 1 | 462 | 216.5 | - | 167 | 175,267 | 95.3 | 0.87 (0.67–1.13) |
| 6–10 | 7 | 1184 | 591.2 | 1.78 (0.33–9.69) | 2 | 181 | 1105.5 | - | 66 | 52,286 | 126.2 | 0.95 (0.68–1.33) |
| >10 | 3 | 465 | 645.2 | 1.51 (0.22–10.4) | 0 | 92 | - | - | 14 | 12,582 | 111.3 | 0.80 (0.45–1.42) |
| p for trend | 0.37 | N.A. | 0.55 | |||||||||
| p-interaction | 0.09 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, H.-S.; Shu, X.-O.; Gao, Y.-T.; Yang, G.; Cai, H.; Shi, J.; Yang, J.J.; Rothman, N.; Lan, Q.; Zheng, W.; et al. Tooth Loss and Risk of Lung Cancer among Urban Chinese Adults: A Cohort Study with Meta-Analysis. Cancers 2022, 14, 2428. https://doi.org/10.3390/cancers14102428
Yoon H-S, Shu X-O, Gao Y-T, Yang G, Cai H, Shi J, Yang JJ, Rothman N, Lan Q, Zheng W, et al. Tooth Loss and Risk of Lung Cancer among Urban Chinese Adults: A Cohort Study with Meta-Analysis. Cancers. 2022; 14(10):2428. https://doi.org/10.3390/cancers14102428
Chicago/Turabian StyleYoon, Hyung-Suk, Xiao-Ou Shu, Yu-Tang Gao, Gong Yang, Hui Cai, Jiajun Shi, Jae Jeong Yang, Nathaniel Rothman, Qing Lan, Wei Zheng, and et al. 2022. "Tooth Loss and Risk of Lung Cancer among Urban Chinese Adults: A Cohort Study with Meta-Analysis" Cancers 14, no. 10: 2428. https://doi.org/10.3390/cancers14102428
APA StyleYoon, H.-S., Shu, X.-O., Gao, Y.-T., Yang, G., Cai, H., Shi, J., Yang, J. J., Rothman, N., Lan, Q., Zheng, W., & Cai, Q. (2022). Tooth Loss and Risk of Lung Cancer among Urban Chinese Adults: A Cohort Study with Meta-Analysis. Cancers, 14(10), 2428. https://doi.org/10.3390/cancers14102428