
Effects of COVID-19 Lockdown on Melanoma Diagnosis in Switzerland: Increased Tumor Thickness in Elderly Females and Shift towards Stage IV Melanoma during Lockdown

 ,
,  , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Data Analysis
2.2.1. Time Series of Diagnosed Melanomas
2.2.2. Dependence of Breslow Thickness and Ulceration on the Time of Diagnosis
2.2.3. Influence of Lockdown Period on the Proportional Distribution of Stage of Diagnosed Melanoma and Corresponding Age
3. Results
3.1. Patient Characteristics
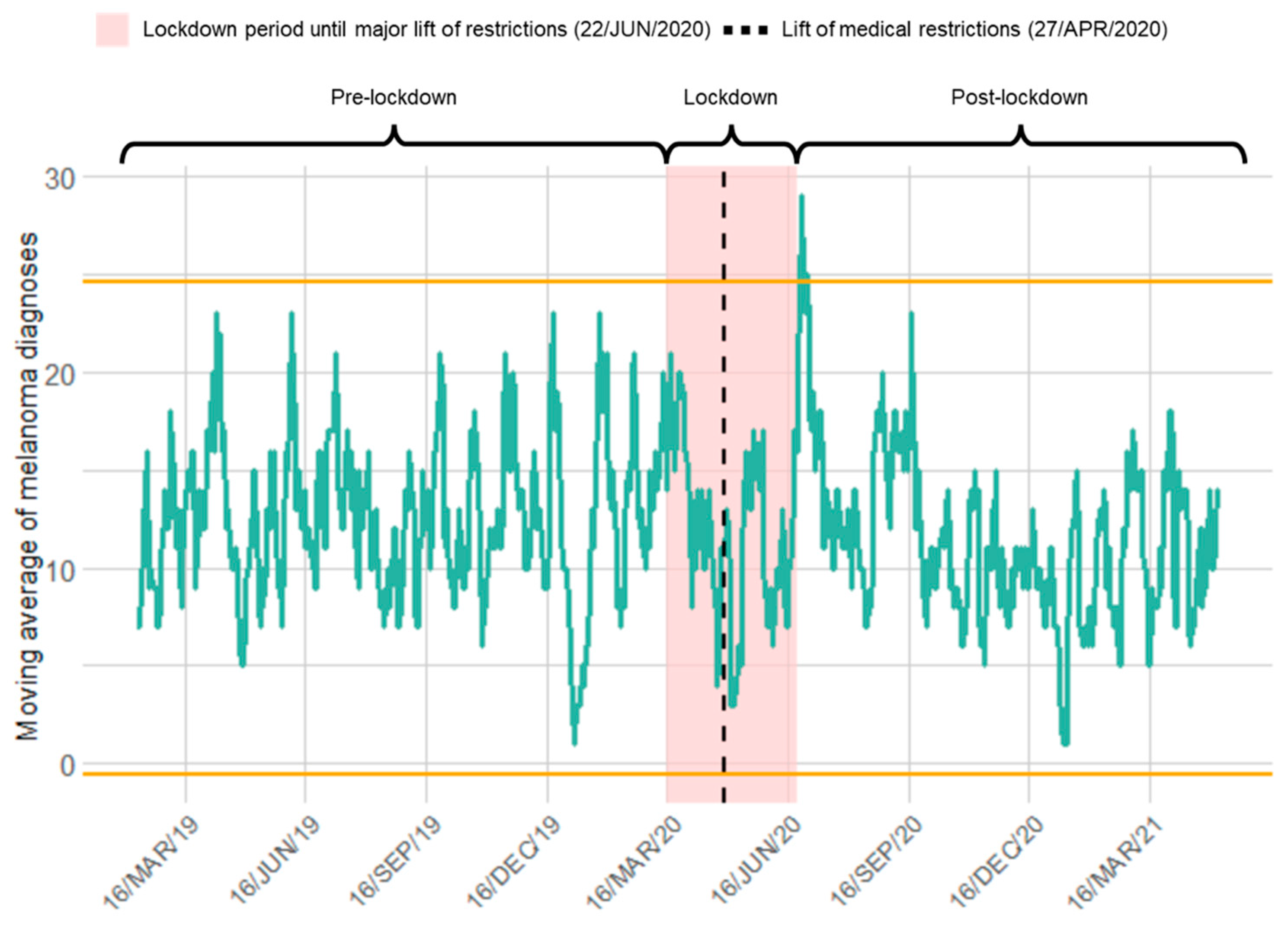
3.2. Time Series of Melanoma Diagnosis in Switzerland Relative to COVID-19 Lockdown
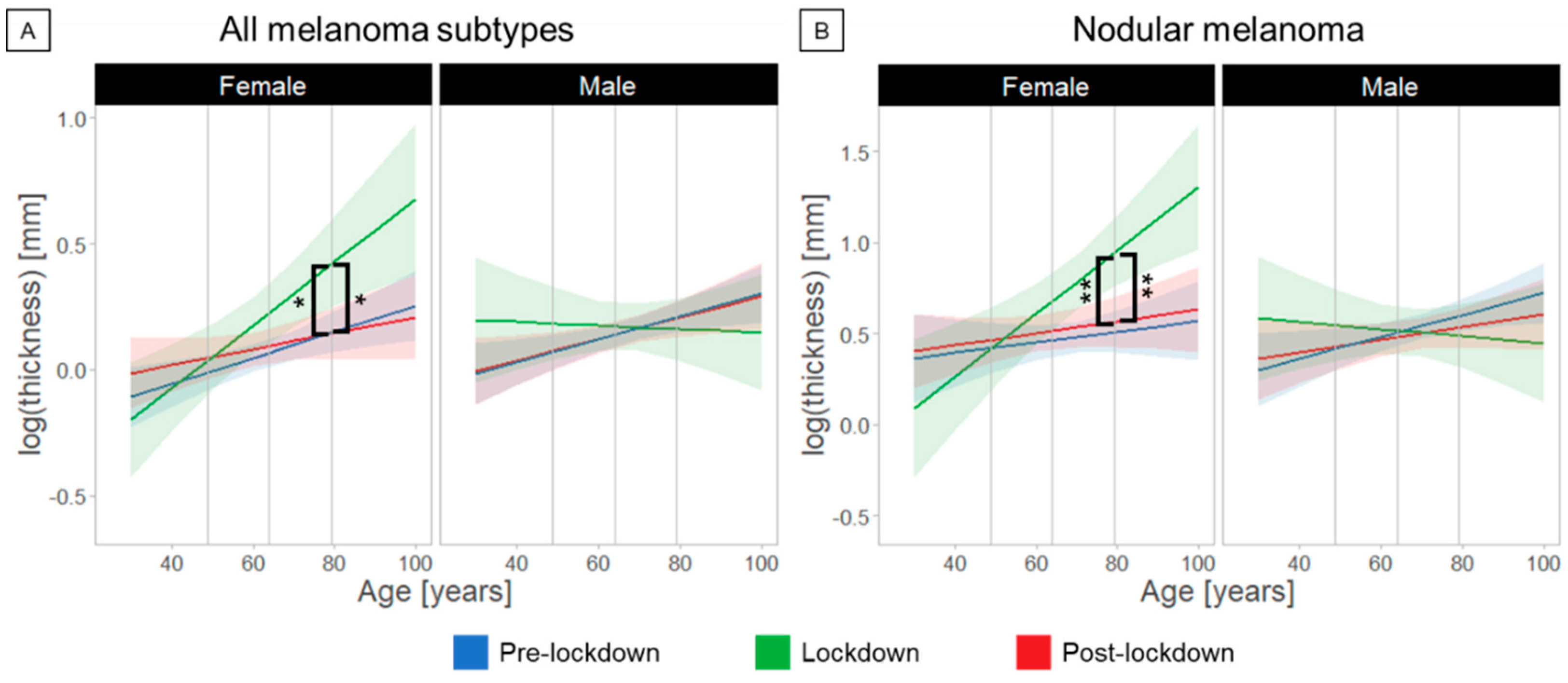
3.3. Effects of COVID-19 Lockdown on Thickness and Subtype of Diagnosed Melanomas in Switzerland
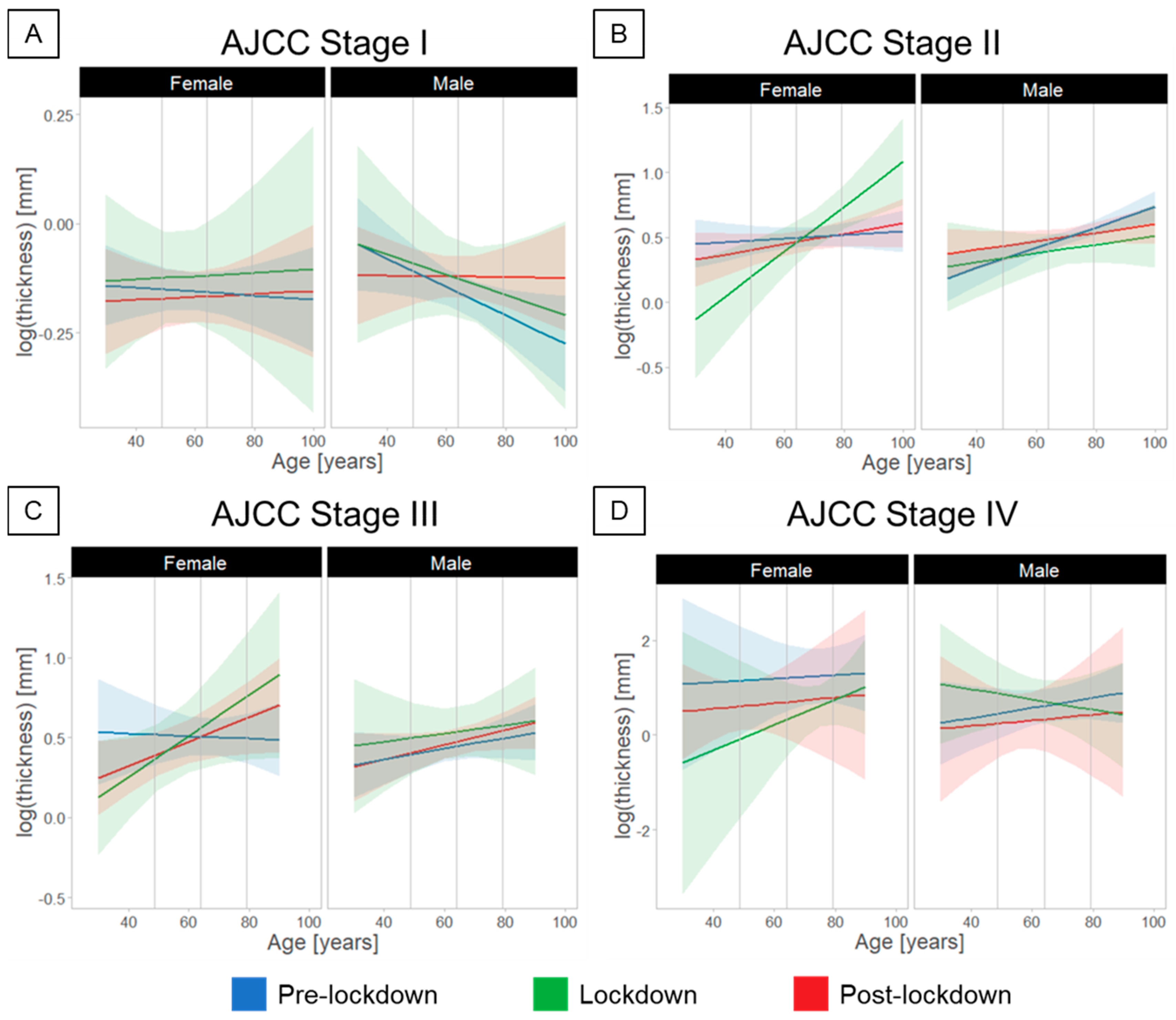
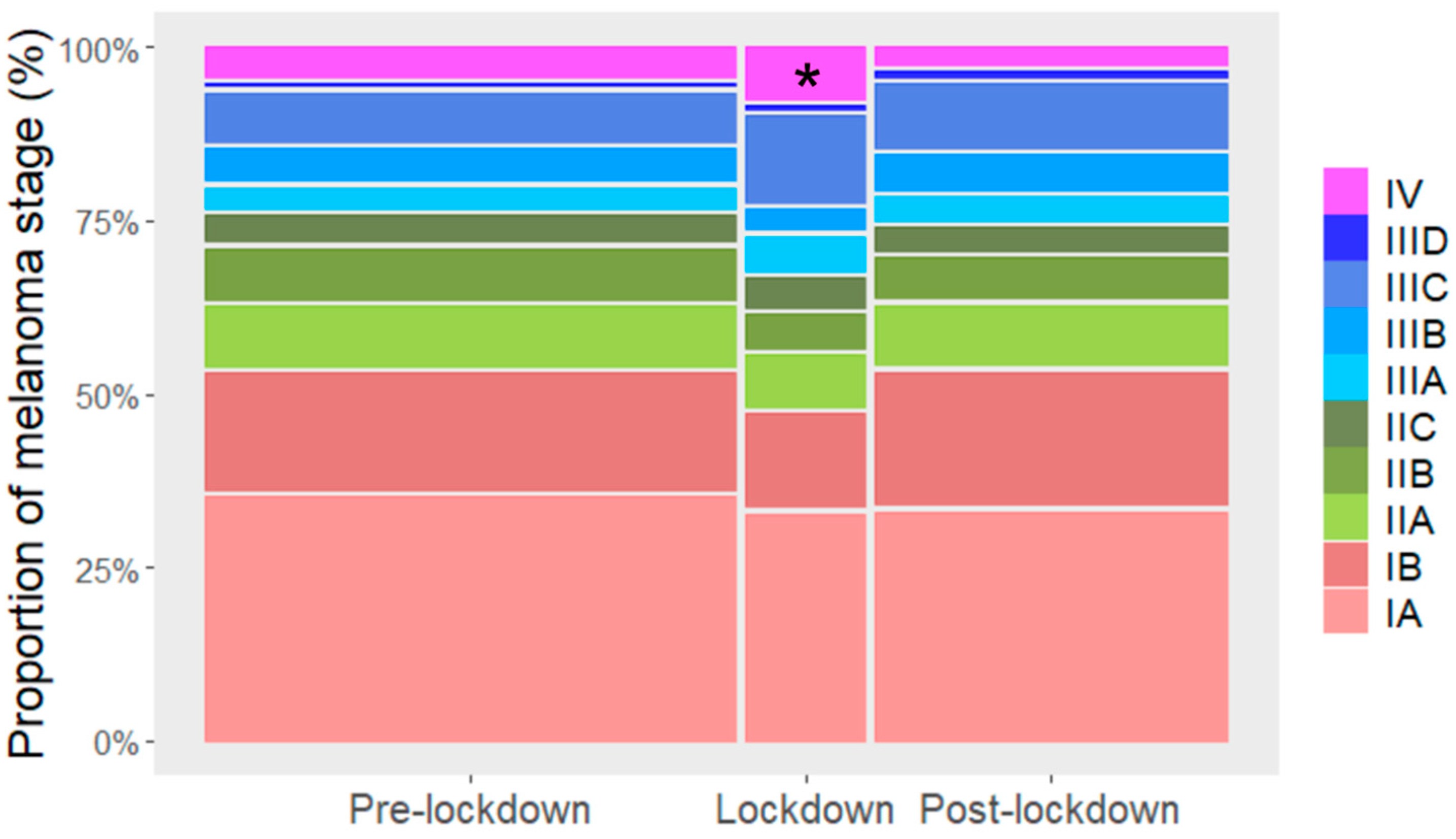
3.4. Stage-Dependent Effects on the Melanoma Diagnosis Relative to COVID-19 Lockdown
4. Discussion
4.1. Main Findings
4.2. Perspective
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Onyeaka, H.; Anumudu, C.K.; Al-Sharify, Z.T.; Egele-Godswill, E.; Mbaegbu, P. COVID-19 pandemic: A review of the global lockdown and its far-reaching effects. Sci. Prog. 2021, 104, 00368504211019854. [Google Scholar] [CrossRef] [PubMed]
- Peacock, H.M.; Tambuyzer, T.; Verdoodt, F.; Calay, F.; Poirel, H.A.; De Schutter, H.; Francart, J.; Van Damme, N.; Van Eycken, L. Decline and incomplete recovery in cancer diagnoses during the COVID-19 pandemic in Belgium: A year-long, population-level analysis. ESMO Open 2021, 6, 100197. [Google Scholar] [CrossRef] [PubMed]
- Andrew, T.W.; Alrawi, M.; Lovat, P. Reduction in skin cancer diagnoses in the UK during the COVID-19 pandemic. Clin Exp. Dermatol. 2021, 46, 145–146. [Google Scholar] [CrossRef] [PubMed]
- Marson, J.W.; Maner, B.S.; Harding, T.P.; Meisenheimer, J.V.; Solomon, J.A.; Leavitt, M.; Levin, N.J.; Dellavalle, R.; Brooks, I.; Rigel, D.S. The magnitude of COVID-19’s effect on the timely management of melanoma and nonmelanoma skin cancers. J. Am. Acad. Dermatol. 2021, 84, 1100–1103. [Google Scholar] [CrossRef] [PubMed]
- Spot the Dot. Survey Reveals One Fifth of Melanomas Globally Went Undiagnosed during COVID-19 Pandemic. Available online: https://spotthedot.org/en/news/survey-reveals-one-fifth-of-melanomas-globally-went-undiagnosed-during-covid-19-pandemic/ (accessed on 25 January 2022).
- Lallas, A.; Kyrgidis, A.; Manoli, S.M.; Papageorgiou, C.; Lallas, K.; Sotiriou, E.; Vakirlis, E.; Sidiropoulos, T.; Ioannides, D.; Apalla, Z. Delayed skin cancer diagnosis in 2020 because of the COVID-19-related restrictions: Data from an institutional registry. J. Am. Acad. Dermatol. 2021, 85, 721–723. [Google Scholar] [CrossRef] [PubMed]
- Ricci, F.; Fania, L.; Paradisi, A.; Di Lella, G.; Pallotta, S.; Sobrino, L.; Panebianco, A.; Annessi, G.; Abeni, D. Delayed melanoma diagnosis in the COVID-19 era: Increased breslow thickness in primary melanomas seen after the COVID-19 lockdown. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e778–e779. [Google Scholar] [CrossRef]
- Gualdi, G.; Porreca, A.; Amoruso, G.F.; Atzori, L.; Calzavara-Pinton, P.; De Tursi, M.; Buduo, A.D.; Marino, P.D.; Fabroncini, G.; Fantini, F.; et al. The Effect of the COVID-19 Lockdown on Melanoma Diagnosis in Italy. Clin. Dermatol. 2021, 39, 911–919. [Google Scholar] [CrossRef]
- Molinier, R.; Roger, A.; Genet, B.; Blom, A.; Longvert, C.; Chaplain, L.; Fort, M.; Saiag, P.; Funck-Brentano, E. Impact of the French COVID-19 pandemic lockdown on newly diagnosed melanoma delay and severity. J. Eur. Acad. Dermatol. Venereol. 2021, 36, e164–e166. [Google Scholar] [CrossRef]
- van Not, O.J.; van Breeschoten, J.; van den Eertwegh, A.J.M.; Hilarius, D.L.; De Meza, M.M.; Haanen, J.B.; Blank, C.U.; Aarts, M.J.B.; van den Berkmortel, F.; de Groot, J.W.B.; et al. The unfavorable effects of COVID-19 on Dutch advanced melanoma care. Int. J. Cancer 2022, 150, 816–824. [Google Scholar] [CrossRef]
- Maringe, C.; Spicer, J.; Morris, M.; Purushotham, A.; Nolte, E.; Sullivan, R.; Rachet, B.; Aggarwal, A. The impact of the COVID-19 pandemic on cancer deaths due to delays in diagnosis in England, UK: A national, population-based, modelling study. Lancet Oncol. 2020, 21, 1023–1034. [Google Scholar] [CrossRef]
- Promoting Cancer Early Diagnosis. Available online: http://who.int/cancer/prevention/diagnosis-screening/en/ (accessed on 25 January 2022).
- Gershenwald, J.E.; Scolyer, R.A.; Hess, K.R.; Sondak, V.K.; Long, G.V.; Ross, M.I.; Lazar, A.J.; Faries, M.B.; Kirkwood, J.M.; McArthur, G.A.; et al. Melanoma staging: Evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2017, 67, 472–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hubner, J.; Eisemann, N.; Brunssen, A.; Katalinic, A. Skin cancer screening in Germany: Review after ten years. Bundesgesundheitsblatt Gesundh. Gesundh. 2018, 61, 1536–1543. [Google Scholar] [CrossRef]
- Johansson, M.; Brodersen, J.; Gotzsche, P.C.; Jorgensen, K.J. Screening for reducing morbidity and mortality in malignant melanoma. Cochrane Database Syst. Rev. 2019, 6, CD012352. [Google Scholar] [CrossRef] [PubMed]
- Welch, H.G.; Mazer, B.L.; Adamson, A.S. The Rapid Rise in Cutaneous Melanoma Diagnoses. N. Engl. J. Med. 2021, 384, 72–79. [Google Scholar] [CrossRef]
- MoleMap, T. A Growing Concern: The Impact of Lockdowns on Skin Cancer Rates. Available online: https://www.molemap.co.nz/skin-cancer/covid-and-skin-cancer-rates (accessed on 29 October 2021).
- Seretis, K.; Boptsi, E.; Boptsi, A.; Lykoudis, E.G. The impact of treatment delay on skin cancer in COVID-19 era: A case-control study. World J. Surg. Oncol. 2021, 19, 350. [Google Scholar] [CrossRef] [PubMed]
- Arenbergerova, M.; Lallas, A.; Nagore, E.; Rudnicka, L.; Forsea, A.M.; Pasek, M.; Meier, F.; Peris, K.; Olah, J.; Posch, C. Position statement of the EADV Melanoma Task Force on recommendations for the management of cutaneous melanoma patients during COVID-19. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e427–e428. [Google Scholar] [CrossRef]
- Wikipedia. COVID-19 Lockdowns. Available online: https://en.wikipedia.org/wiki/COVID-19_lockdowns#Table_of_pandemic_lockdown (accessed on 26 February 2022).
- BAG. Coronavirus: Federal Council Declares ‘Extraordinary Situation’ and Introduces More Stringent Measures. Available online: https://www.bag.admin.ch/bag/de/home/das-bag/aktuell/medienmitteilungen.msg-id-78454.html (accessed on 17 March 2020).
- SRF. So Sieht der Fahrplan des Bundesrates aus. Available online: https://www.srf.ch/news/schweiz/alle-schritte-aus-dem-lockdown-so-sieht-der-fahrplan-des-bundesrates-aus (accessed on 1 February 2022).
- Ilyas, I.F.; Chu, X. Data Cleaning; Association for Computing Machinery: New York, NY, USA, 2019. [Google Scholar] [CrossRef]
- Cohen, J.; Cohen, P. Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences; Taylor & Francis Group: Abingdon, UK, 1983. [Google Scholar] [CrossRef]
- West, S.G.; Aiken, L.S.; Krull, J.L. Experimental Personality Designs: Analyzing Categorical by Continuous Variable Interactions. J. Pers. 1996, 64, 1–48. [Google Scholar] [CrossRef]
- Vose, J.M. Delay in Cancer Screening and Diagnosis During the COVID-19 Pandemic: What Is the Cost? Oncology 2020, 34, 343. [Google Scholar] [CrossRef]
- Ferrara, G.; De Vincentiis, L.; Ambrosini-Spaltro, A.; Barbareschi, M.; Bertolini, V.; Contato, E.; Crivelli, F.; Feyles, E.; Mariani, M.P.; Morelli, L.; et al. Cancer Diagnostic Delay in Northern and Central Italy During the 2020 Lockdown Due to the Coronavirus Disease 2019 Pandemic. Am. J. Clin. Pathol. 2021, 155, 64–68. [Google Scholar] [CrossRef]
- Longo, C.; Pampena, R.; Fossati, B.; Pellacani, G.; Peris, K. Melanoma diagnosis at the time of COVID-19. Int. J. Dermatol. 2021, 60, e29–e30. [Google Scholar] [CrossRef]
- Schauer, A.A.; Kulakov, E.L.; Martyn-Simmons, C.L.; Bunker, C.B.; Edmonds, E.V.J. Melanoma defies ‘lockdown’: Ongoing detection during COVID-19 in central London. Clin. Exp. Dermatol. 2020, 45, 900. [Google Scholar] [CrossRef] [PubMed]
- Mehrotra, A.; Chernew, M.E.; Linetsky, D.; Hatch, H.; Cutler, D.A. The Impact of the COVID-19 Pandemic on Outpatient Visits: A Rebound Emerges. Available online: https://www.commonwealthfund.org/publications/2020/apr/impact-covid-19-outpatient-visits (accessed on 19 May 2020).
- Barruscotti, S.; Giorgini, C.; Brazzelli, V.; Vassallo, C.; Michelerio, A.; Klersy, C.; Chiellino, S.; Tomasini, C.F. A significant reduction in the diagnosis of melanoma during the COVID-19 lockdown in a third-level center in the Northern Italy. Dermatol. Ther. 2020, 33, e14074. [Google Scholar] [CrossRef] [PubMed]
- Gerli, A.G.; Centanni, S.; Miozzo, M.R.; Virchow, J.C.; Sotgiu, G.; Canonica, G.W.; Soriano, J.B. COVID-19 mortality rates in the European Union, Switzerland, and the UK: Effect of timeliness, lockdown rigidity, and population density. Minerva Med. 2020, 111, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Conforti, C.; Lallas, A.; Argenziano, G.; Dianzani, C.; Di Meo, N.; Giuffrida, R.; Kittler, H.; Malvehy, J.; Marghoob, A.A.; Soyer, H.P.; et al. Impact of the COVID-19 Pandemic on Dermatology Practice Worldwide: Results of a Survey Promoted by the International Dermoscopy Society (IDS). Dermatol. Pract. Concept 2021, 11, e2021153. [Google Scholar] [CrossRef]
- Chuchu, N.; Dinnes, J.; Takwoingi, Y.; Matin, R.N.; Bayliss, S.E.; Davenport, C.; Moreau, J.F.; Bassett, O.; Godfrey, K.; O’Sullivan, C.; et al. Teledermatology for diagnosing skin cancer in adults. Cochrane Database Syst. Rev. 2018, 12, CD013193. [Google Scholar] [CrossRef] [PubMed]
- Scoggins, C.R.; Ross, M.I.; Reintgen, D.S.; Noyes, R.D.; Goydos, J.S.; Beitsch, P.D.; Urist, M.M.; Ariyan, S.; Sussman, J.J.; Edwards, M.J.; et al. Gender-related differences in outcome for melanoma patients. Ann. Surg. 2006, 243, 693–698, discussion 698-700. [Google Scholar] [CrossRef] [PubMed]
- Behbahani, S.; Maddukuri, S.; Cadwell, J.B.; Lambert, W.C.; Schwartz, R.A. Gender differences in cutaneous melanoma: Demographics, prognostic factors, and survival outcomes. Dermatol. Ther. 2020, 33, e14131. [Google Scholar] [CrossRef]
- Bellenghi, M.; Puglisi, R.; Pontecorvi, G.; De Feo, A.; Care, A.; Mattia, G. Sex and Gender Disparities in Melanoma. Cancers 2020, 12, 1819. [Google Scholar] [CrossRef]
- Galasso, V.; Pons, V.; Profeta, P.; Becher, M.; Brouard, S.; Foucault, M. Gender differences in COVID-19 attitudes and behavior: Panel evidence from eight countries. Proc. Natl. Acad. Sci. USA 2020, 117, 27285–27291. [Google Scholar] [CrossRef]
- Sigorski, D.; Sobczuk, P.; Osmola, M.; Kuc, K.; Walerzak, A.; Wilk, M.; Ciszewski, T.; Kopec, S.; Hryn, K.; Rutkowski, P.; et al. Impact of COVID-19 on anxiety levels among patients with cancer actively treated with systemic therapy. ESMO Open 2020, 5, e000970. [Google Scholar] [CrossRef] [PubMed]
- Courtenay, W.H. Behavioral Factors Associated with Disease, Injury, and Death among Men: Evidence and Implications for Prevention. J. Men’s Stud. 2000, 9, 81–142. [Google Scholar] [CrossRef]
- Paddock, L.E.; Lu, S.E.; Bandera, E.V.; Rhoads, G.G.; Fine, J.; Paine, S.; Barnhill, R.; Berwick, M. Skin self-examination and long-term melanoma survival. Melanoma Res. 2016, 26, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Tejera-Vaquerizo, A.; Paradela, S.; Toll, A.; Santos-Juanes, J.; Jaka, A.; Lopez, A.; Canueto, J.; Bernal, A.; Villegas-Romero, I.; Ferrandiz-Pulido, C.; et al. Effects of COVID-19 Lockdown on Tumour Burden of Melanoma and Cutaneous Squamous Cell Carcinoma. Acta. Derm. Venereol. 2021, 101, adv00525. [Google Scholar] [CrossRef] [PubMed]
- Minini, R.; Rohrmann, S.; Braun, R.; Korol, D.; Dehler, S. Incidence trends and clinical-pathological characteristics of invasive cutaneous melanoma from 1980 to 2010 in the Canton of Zurich, Switzerland. Melanoma Res. 2017, 27, 145–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teuscher, M.; Diehl, K.; Schaarschmidt, M.L.; Weilandt, J.; Sasama, B.; Ohletz, J.; Konnecke, A.; Harth, W.; Hillen, U.; Peitsch, W.K. Effects of the COVID-19 pandemic on care of melanoma patients in Berlin, Germany: The Mela-COVID survey. Eur. J. Dermatol. 2021, 31, 521–529. [Google Scholar] [CrossRef]
- Gebbia, V.; Piazza, D.; Valerio, M.R.; Borsellino, N.; Firenze, A. Patients with Cancer and COVID-19: A WhatsApp Messenger-Based Survey of Patients’ Queries, Needs, Fears, and Actions Taken. JCO Glob. Oncol. 2020, 6, 722–729. [Google Scholar] [CrossRef]
- Lattanzi, M.; Lee, Y.; Simpson, D.; Moran, U.; Darvishian, F.; Kim, R.H.; Hernando, E.; Polsky, D.; Hanniford, D.; Shapiro, R.; et al. Primary Melanoma Histologic Subtype: Impact on Survival and Response to Therapy. J. Natl. Cancer Inst. 2019, 111, 180–188. [Google Scholar] [CrossRef]
- Shannon, A.B.; Sharon, C.E.; Straker, R.J., 3rd; Miura, J.T.; Ming, M.E.; Chu, E.Y.; Karakousis, G.C. The impact of the COVID-19 pandemic on the presentation status of newly diagnosed melanoma: A single institution experience. J. Am. Acad. Dermatol. 2021, 84, 1096–1098. [Google Scholar] [CrossRef] [PubMed]
- Tejera-Vaquerizo, A.; Nagore, E. Estimated effect of COVID-19 lockdown on melanoma thickness and prognosis: A rate of growth model. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e351–e353. [Google Scholar] [CrossRef]
- Degeling, K.; Baxter, N.N.; Emery, J.; Jenkins, M.A.; Franchini, F.; Gibbs, P.; Mann, G.B.; McArthur, G.; Solomon, B.J.; Izerman, M.J. An inverse stage-shift model to estimate the excess mortality and health economic impact of delayed access to cancer services due to the COVID-19 pandemic. Asia Pac. J. Clin. Oncol. 2021, 17, 359–367. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n = 1240 | |
|---|---|---|
| Mean age in years (SD) | 64 (±15.4) | |
| Gender (n, %) | Female | 497 (40.0) |
| Male | 741 (59.8) | |
| Not specified | 2 (0.2) | |
| Number of patients grouped by hospital in which diagnosis was received (n, %) | Aarau | 152 (12.3) |
| Basel | 195 (15.7) | |
| Lucerne | 130 (10.5) | |
| St. Gallen | 184 (14.8) | |
| Zurich | 579 (46.7) | |
| Breslow thickness (median, (Q1–Q3)) [mm] | Total | 1.2 (0.7–2.6) |
| Women | 1.1 (0.6–2.2) | |
| Men | 1.4 (0.8–2.8) | |
| Pre-lockdown 1 | 1.2 (0.6–2.6) | |
| Women | 1.1 (0.5–2.1) | |
| Men | 1.4 (0.7–2.8) | |
| Lockdown 1 | 1.4 (0.7–3.0) | |
| Women | 1.2 (0.7–3.0) | |
| Men | 1.4 (0.7–3.0) | |
| Post-lockdown 1 | 1.2 (0.8–2.5) | |
| Women | 1.2 (0.7–2.4) | |
| Men | 1.3 (0.8–2.7) | |
| Stage (8th edition AJCC; n, %) | Stage I | 695 (57.0) |
| IA | 461 (37.2) | |
| IB | 234 (18.9) | |
| Stage II | 254 (20.5) | |
| IIA | 115 (9.3) | |
| IIB | 88 (7.1) | |
| IIC | 51 (4.1) | |
| Stage III | 233 (18.8) | |
| IIIA | 46 (3.7) | |
| IIIB | 63 (5.1) | |
| IIIC | 114 (9.2) | |
| IIID | 8 (0.7) | |
| III (not specified) * | 2 (0.2) | |
| Stage IV | 54 (4.4) | |
| Stage not specified | 4 (0.3) | |
| Ulceration (n, %) | Yes | 240 (19.4) |
| No | 914 (73.7) | |
| Not specified | 86 (6.9) | |
| Melanoma subtype (n, %) | Superficial spreading | 543 (43.8) |
| Nodular | 230 (18.5) | |
| Lentigo maligna | 144 (11.6) | |
| Acral | 43 (3.5) | |
| Others ** | 38 (3.1) | |
| Amelanotic | 13 (1.0) | |
| Not specified | 229 (18.5) | |
| All Melanoma Subtypes(n = 1240) | ||||||
| Interaction Period × Gender × Age—F(2,1182) = 3.15, p = 0.04 | ||||||
| Period | Gender | Age | Difference ± SE [mm] | DoF | n | p-Value |
| Lockdown minus pre-lockdown | Female | Old | 1.9 ± 1.3 | 207 | 333 | 0.03 |
| Lockdown minus post-lockdown | 1.9 ± 1.3 | 133 | 226 | 0.048 | ||
| Pre-lockdown | Female minus male | Average | −1.2 ± 1.1 | 1183 | 654 | 0.045 |
| Lockdown | Old | 1.8 ± 1.3 | 1174 | 148 | 0.019 | |
| Nodular Melanoma(n = 230) | ||||||
| Interaction Period × Gender × Age—F(2,209) = 4.49, p = 0.012 | ||||||
| Period | Gender | Age | Difference ± SE [mm] | DoF | n | p-Value |
| Lockdown minus pre-lockdown | Female | Old | 2.9 ± 1.3 | 39 | 57 | 0.0021 |
| Lockdown minus post-lockdown | 2.6 ± 1.4 | 41 | 46 | 0.008 | ||
| Lockdown | Female minus male | Average | 1.7 ± 1.3 | 196 | 34 | 0.03 |
| Old | 3.3 ± 1.4 | 133 | 34 | 0.0013 | ||
| AJCC Stage II(n = 254) | ||||||
| Interaction Period × Gender × Age—F(2,173) = 3.39, p = 0.04 | ||||||
| Period | Gender | Age | Difference ± SE [mm] | DoF | n | p-Value |
| Lockdown | Female minus male | Old | 2.2 ± 1.4 | 160 | 27 | 0.016 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kostner, L.; Cerminara, S.E.; Pamplona, G.S.P.; Maul, J.-T.; Dummer, R.; Ramelyte, E.; Mangana, J.; Wagner, N.B.; Cozzio, A.; Kreiter, S.; et al. Effects of COVID-19 Lockdown on Melanoma Diagnosis in Switzerland: Increased Tumor Thickness in Elderly Females and Shift towards Stage IV Melanoma during Lockdown. Cancers 2022, 14, 2360. https://doi.org/10.3390/cancers14102360
Kostner L, Cerminara SE, Pamplona GSP, Maul J-T, Dummer R, Ramelyte E, Mangana J, Wagner NB, Cozzio A, Kreiter S, et al. Effects of COVID-19 Lockdown on Melanoma Diagnosis in Switzerland: Increased Tumor Thickness in Elderly Females and Shift towards Stage IV Melanoma during Lockdown. Cancers. 2022; 14(10):2360. https://doi.org/10.3390/cancers14102360
Chicago/Turabian StyleKostner, Lisa, Sara Elisa Cerminara, Gustavo Santo Pedro Pamplona, Julia-Tatjana Maul, Reinhard Dummer, Egle Ramelyte, Johanna Mangana, Nikolaus Benjamin Wagner, Antonio Cozzio, Saskia Kreiter, and et al. 2022. "Effects of COVID-19 Lockdown on Melanoma Diagnosis in Switzerland: Increased Tumor Thickness in Elderly Females and Shift towards Stage IV Melanoma during Lockdown" Cancers 14, no. 10: 2360. https://doi.org/10.3390/cancers14102360
APA StyleKostner, L., Cerminara, S. E., Pamplona, G. S. P., Maul, J.-T., Dummer, R., Ramelyte, E., Mangana, J., Wagner, N. B., Cozzio, A., Kreiter, S., Kogler, A., Streit, M., Wysocki, A., Zippelius, A., Läubli, H., Navarini, A. A., & Maul, L. V. (2022). Effects of COVID-19 Lockdown on Melanoma Diagnosis in Switzerland: Increased Tumor Thickness in Elderly Females and Shift towards Stage IV Melanoma during Lockdown. Cancers, 14(10), 2360. https://doi.org/10.3390/cancers14102360