Acupuncture and Moxibustion for Cancer-Related Fatigue: An Overview of Systematic Reviews and Meta-Analysis



Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Study Registration
2.2. Database and Search
2.3. Eligibility Criteria
2.3.1. Types of Studies
2.3.2. Types of Participants
2.3.3. Types of Interventions and Comparators
2.3.4. Types of Outcome Measures
2.3.5. Exclusion Criteria
2.4. Studies Selection
2.5. Data Extraction
2.6. Quality Assessment
2.7. Certainty of Evidence (CoE)
2.8. Data Analysis
3. Results
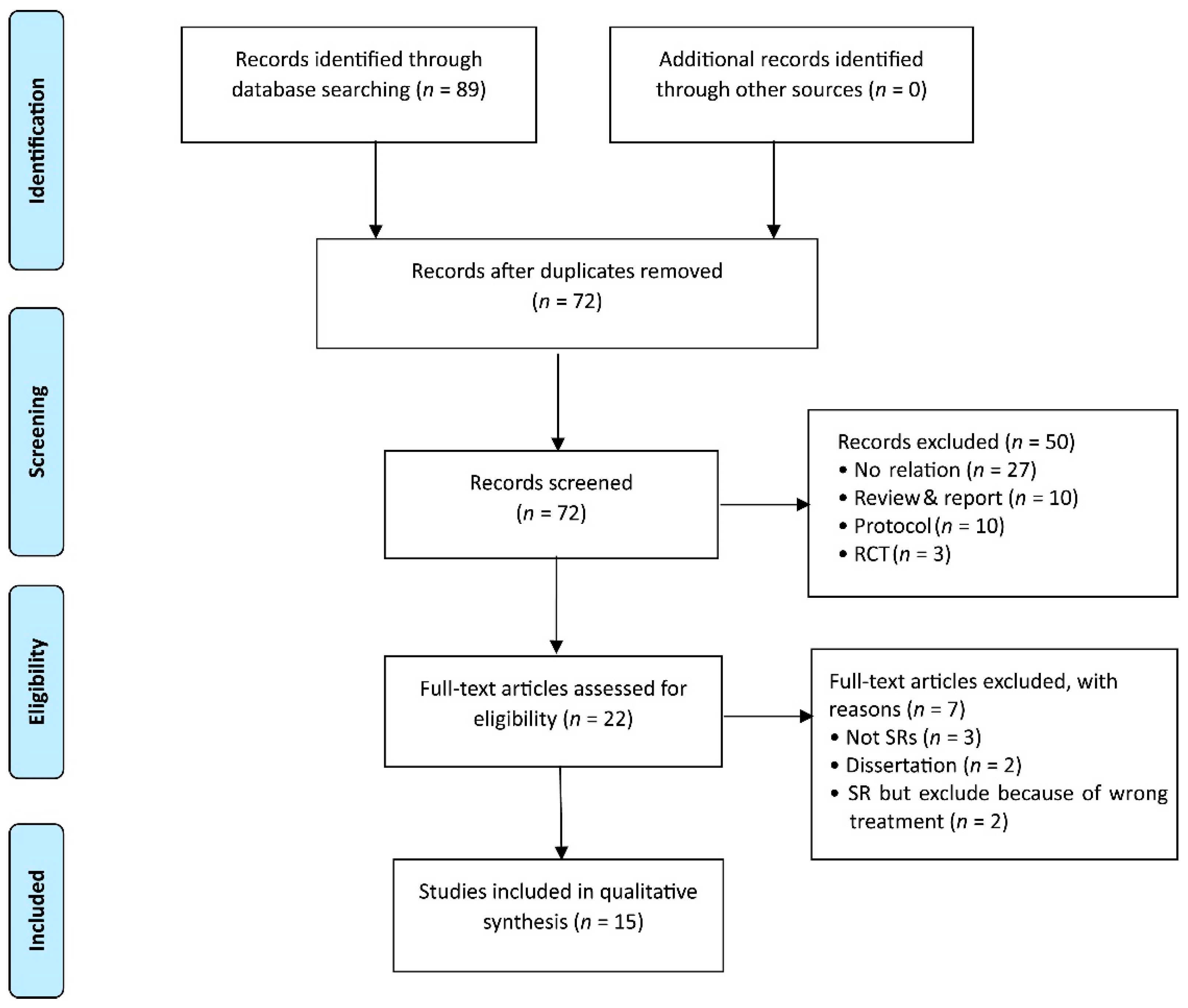
3.1. Study Identification
3.2. Characteristics of Included Studies
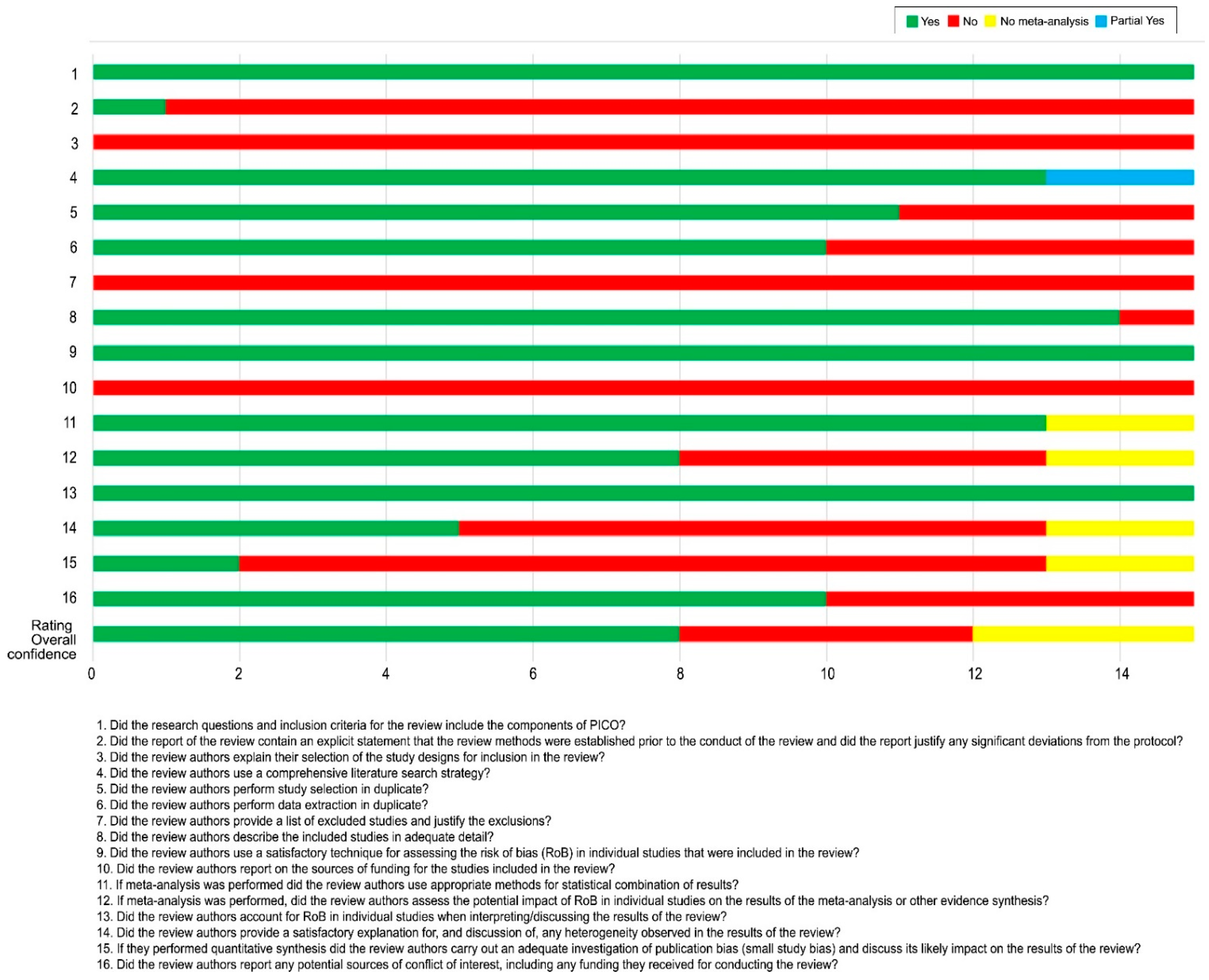
3.3. Assessment of Quality
3.4. Certainty of Evidence (CoE)
3.5. Effectiveness of Acupuncture for CRF
3.6. Adverse Events (AEs)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Iop, A.; Manfredi, A.M.; Bonura, S. Fatigue in cancer patients receiving chemotherapy: An analysis of published studies. Ann. Oncol. 2004, 15, 712–720. [Google Scholar] [CrossRef] [PubMed]
- Escalante, C.P.; Manzullo, E.F. Cancer-related fatigue: The approach and treatment. J. Gen. Intern. Med. 2009, 24 (Suppl. S2), S412–S416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cella, D.; Davis, K.; Breitbart, W.; Curt, G. Cancer-related fatigue: Prevalence of proposed diagnostic criteria in a United States sample of cancer survivors. J. Clin. Oncol. 2001, 19, 3385–3391. [Google Scholar] [CrossRef]
- Ebede, C.C.; Jang, Y.; Escalante, C.P. Cancer-Related Fatigue in Cancer Survivorship. Med. Clin. N. Am. 2017, 101, 1085–1097. [Google Scholar] [CrossRef] [PubMed]
- Berger, A.M.; Mooney, K.; Alvarez-Perez, A.; Breitbart, W.S.; Carpenter, K.M.; Cella, D.; Cleeland, C.; Dotan, E.; Eisenberger, M.A.; Escalante, C.P.; et al. Cancer-Related Fatigue, Version 2.2015. J. Natl. Compr. Canc. Netw. 2015, 13, 1012–1039. [Google Scholar] [CrossRef] [PubMed]
- Minton, O.; Stone, P. How common is fatigue in disease-free breast cancer survivors? A systematic review of the literature. Breast Cancer Res. Treat. 2008, 112, 5–13. [Google Scholar] [CrossRef]
- Stasi, R.; Abriani, L.; Beccaglia, P.; Terzoli, E.; Amadori, S. Cancer-related fatigue: Evolving concepts in evaluation and treatment. Cancer 2003, 98, 1786–1801. [Google Scholar] [CrossRef]
- Prue, G.; Rankin, J.; Allen, J.; Gracey, J.; Cramp, F. Cancer-related fatigue: A critical appraisal. Eur. J. Cancer 2006, 42, 846–863. [Google Scholar] [CrossRef]
- Kristoffersen, A.E.; Stub, T.; Broderstad, A.R.; Hansen, A.H. Use of traditional and complementary medicine among Norwegian cancer patients in the seventh survey of the Tromso study. BMC Complement. Altern. Med. 2019, 19, 341. [Google Scholar] [CrossRef]
- Hilfiker, R.; Meichtry, A.; Eicher, M.; Nilsson Balfe, L.; Knols, R.H.; Verra, M.L.; Taeymans, J. Exercise and other non-pharmaceutical interventions for cancer-related fatigue in patients during or after cancer treatment: A systematic review incorporating an indirect-comparisons meta-analysis. Br. J. Sports Med. 2018, 52, 651–658. [Google Scholar] [CrossRef]
- Lau, C.H.Y.; Wu, X.; Chung, V.C.H.; Liu, X.; Hui, E.P.; Cramer, H.; Lauche, R.; Wong, S.Y.S.; Lau, A.Y.L.; Sit, R.W.S.; et al. Acupuncture and related therapies for symptom management in palliative cancer care: Systematic review and meta-analysis. Medicine 2016, 95, e2901. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.S.; Woodruff, J.F. Cancer-related and treatment-related fatigue. Gynecol. Oncol. 2015, 136, 446–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacPherson, H.; Thomas, K.; Walters, S.; Fitter, M. The York acupuncture safety study: Prospective survey of 34 000 treatments by traditional acupuncturists. BMJ Clin. Res. Ed. 2001, 323, 486–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melchart, D.; Weidenhammer, W.; Streng, A.; Reitmayr, S.; Hoppe, A.; Ernst, E.; Linde, K. Prospective investigation of adverse effects of acupuncture in 97,733 patients. Arch. Intern. Med. 2004, 164, 104–105. [Google Scholar] [CrossRef]
- White, A.; Hayhoe, S.; Hart, A.; Ernst, E. Adverse events following acupuncture: Prospective survey of 32 000 consultations with doctors and physiotherapists. BMJ Clin. Res. Ed. 2001, 323, 485–486. [Google Scholar] [CrossRef] [Green Version]
- Filshie, J.; Hester, J. Guidelines for providing acupuncture treatment for cancer patients--a peer-reviewed sample policy document. Acupunct. Med. 2006, 24, 172–182. [Google Scholar] [CrossRef]
- He, X.R.; Wang, Q.; Li, P.P. Acupuncture and moxibustion for cancer-related fatigue: A systematic review and meta-analysis. Asian Pac. J. Cancer Prev. 2013, 14, 3067–3074. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Lin, L.; Li, H.; Hu, Y.; Tian, L. Effects of acupuncture on cancer-related fatigue: A meta-analysis. Supp. Care Cancer 2018, 26, 415–425. [Google Scholar] [CrossRef]
- Zhao, Y.; Wang, S.; Li, J.; Zhou, Y.; Wu, W.; Swei Sunny, H. Effectiveness and safety of traditional Chinese medical therapy for cancer-related fatigue: A systematic review and Meta-analysis of randomized controlled trials. J. Tradit. Chin. Med. 2020, 40, 738–748. [Google Scholar] [CrossRef]
- Wu, X.; Chung, V.C.; Hui, E.P.; Ziea, E.T.; Ng, B.F.; Ho, R.S.; Tsoi, K.K.; Wong, S.Y.; Wu, J.C. Effectiveness of acupuncture and related therapies for palliative care of cancer: Overview of systematic reviews. Sci. Rep. 2015, 5, 16776. [Google Scholar] [CrossRef] [Green Version]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ Clin. Res. Ed. 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, J.B.; Wang, T.; Kirshbaum, M.N.; Zhao, I.; Eliseeva, S.; Polotan, M.J.; Yao, L.Q.; Huang, H.Q.; Zheng, S.L. Acupoint stimulation for cancer-related fatigue: A quantitative synthesis of randomised controlled trials. Complement. Ther. Clin. Pract. 2021, 45, 101490. [Google Scholar] [CrossRef] [PubMed]
- Jang, A.; Brown, C.; Lamoury, G.; Morgia, M.; Boyle, F.; Marr, I.; Clarke, S.; Back, M.; Oh, B. The effects of acupuncture on cancer-related fatigue: Updated systematic review and meta-analysis. Integr. Cancer Ther. 2020, 19, 1534735420949679. [Google Scholar] [CrossRef] [PubMed]
- Yuan, C.; Xiao, J.; Qin, W.X.; Zhang, Y.; Yuan, Q. Efficacy of acupuncture and moxibustion for cancer related fatigue: A meta-analysis. J. Yunnan Univ. Tradit. Chin. Med. 2020, 43, 61–70. [Google Scholar]
- Ling, W.M.; Lui, L.Y.; So, W.K.; Chan, K. Effects of acupuncture and acupressure on cancer-related fatigue: A systematic review. Oncol. Nurs. Forum. 2014, 41, 581–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Posadzki, P.; Moon, T.W.; Choi, T.Y.; Park, T.Y.; Lee, M.S.; Ernst, E. Acupuncture for cancer-related fatigue: A systematic review of randomized clinical trials. Supp. Care Cancer 2013, 21, 2067–2073. [Google Scholar] [CrossRef]
- Zeng, Y.; Luo, T.; Finnegan-John, J.; Cheng, A.S. Meta-Analysis of Randomized Controlled Trials of Acupuncture for Cancer-Related Fatigue. Integr. Cancer Ther. 2014, 13, 193–200. [Google Scholar] [CrossRef] [Green Version]
- Han, Q.; Yang, L.; Huang, S.Y.; Yeung, J.W.F.; Chen, X.H.; Xue, H.; Xu, L.P.; Suen, L.K.P. Effectiveness of auricular point therapy for cancer-related fatigue: A systematic review and meta-analysis. J. Adv. Nurs. 2020, 79, 1924–1935. [Google Scholar] [CrossRef]
- Huang, S.Y.; Yang, L.; Han, Q.; Xue, H.; Xu, L.P. Meta-analysis of the efficacy and safety of moxibustion in the treatment of cancer-related fatigue. China Mod. Med. 2021, 28, 15. [Google Scholar]
- Han, J.Q.; Zhang, Y.J.; Jiang, E.S. Intervention effect of moxibustion on cancer-related fatigue in cancer patients:a Meta-analysis. Chin. Evid.-Based Nurs. 2021, 7, 719–726. [Google Scholar]
- Hu, Y.; Jiang, Y.L.; Li, Z.; Jiang, C.; Zhou, X.D.; Zeng, Y.Y. A systematic review for clinical efficacy and safety of moxibustion therapy in treatment of cancer-related fatigue. J. Chengdu Univ. Tradit. Chin. Med. 2020, 43, 65–72. [Google Scholar]
- Yu, T.; Liu, J.; Yang, B.; Tang, D.X. Clinical effects of moxibustion on cancer-related fatigue in cancer patients: A systematic review and meta-analysis. Mod. Tradit. Chin. Med. Mater. Med.-World Sci. Technol. 2020, 22, 4175–4184. [Google Scholar]
- Lee, S.; Jerng, U.M.; Liu, Y.; Kang, J.W.; Nam, D.; Lee, J.D. The effectiveness and safety of moxibustion for treating cancer-related fatigue: A systematic review and meta-analyses. Supp. Care Cancer 2014, 22, 1429–1440. [Google Scholar] [CrossRef] [Green Version]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Glasziou, P.; Jaeschke, R.; Akl, E.A.; et al. GRADE guidelines: 7. Rating the quality of evidence—Inconsistency. J. Clin. Epidemiol. 2011, 64, 1294–1302. [Google Scholar] [CrossRef]
- Grant, S.J.; Smith, C.A.; de Silva, N.; Su, C. Defining the quality of acupuncture: The case of acupuncture for cancer-related fatigue. Integr. Cancer Ther. 2015, 14, 258–270. [Google Scholar] [CrossRef] [PubMed]
- Yim, Y.K.; Lee, H.; Hong, K.E.; Kim, Y.I.; Lee, B.R.; Son, C.G.; Kim, J.E. Electro-acupuncture at acupoint ST36 reduces inflammation and regulates immune activity in Collagen-Induced Arthritic Mice. Evid. Based Complement. Altern. Med. 2007, 4, 51–57. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.K.; Bae, H. Acupuncture and immune modulation. Auton. Neurosci. 2010, 157, 38–41. [Google Scholar] [CrossRef]
- Yin, Y.; Chen, T.W.; Zhang, R.; Ma, W.Z. [Effect of Moxibustion on Serum IL-17 and TNF-α Levels in Collagen-induced Arthritis Rats]. Zhen Ci Yan Jiu 2017, 42, 149–152. [Google Scholar]
- Lin, Z.P.; Lan, L.W.; He, T.Y.; Lin, S.P.; Lin, J.G.; Jang, T.R.; Ho, T.J. Effects of acupuncture stimulation on recovery ability of male elite basketball athletes. Am. J. Chin. Med. 2009, 37, 471–481. [Google Scholar] [CrossRef]
- Dong, J.Z.; Wei, Y.T.; Xu, H.Y.; Zhang, Y.; Yong, R.L.; Xue, Y.N.; Zhang, L.D. [Electroacupuncture of “Zusanli” (ST 36) Raises Muscular Force by Adjusting AMPK/PGC-1 α Signaling in Rats with Chronic Fatigue Syndrome]. Zhen Ci Yan Jiu 2018, 43, 335–340. [Google Scholar] [CrossRef]
- Smith, C.; Carmady, B.; Thornton, C.; Perz, J.; Ussher, J.M. The effect of acupuncture on post-cancer fatigue and well-being for women recovering from breast cancer: A pilot randomised controlled trial. Acupunct. Med. 2013, 31, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Li, T.T.; Chu, Y.T.; Chen, K.; Tian, S.D.; Chen, X.Y.; Yang, G.W. Traditional Chinese medical comprehensive therapy for cancer-related fatigue. Chin. J. Integr. Med. 2016, 22, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Cybularz, P.A.; Brothers, K.; Singh, G.M.; Feingold, J.L.; Lewis, M.E.; Niesley, M.L. The Safety of Acupuncture in Patients with Cancer Therapy–Related Thrombocytopenia. Med. Acupunct. 2015, 27, 224–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Höxtermann, M.D.; Haller, H.; Aboudamaah, S.; Bachemir, A.; Dobos, G.; Cramer, H.; Voiss, P. Safety of acupuncture in oncology: A systematic review and meta-analysis of randomized controlled trials. Cancer, 2022; online ahead of print. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| First Author (Year) [Ref] Country | Search Date/ No. of Searched Databases | No. of Included RCTs (Sample Size) | Intervention | Comparator | Overall Risk of Bias | Overall Confidence Rating | Conclusion (Quote from the Original Paper) | Adverse Events |
|---|---|---|---|---|---|---|---|---|
| Tan (2021) [22] Australia | February 2021/13 DBs | 15 (1468) | AT/APT | SAT/UC | Moderate to high | Moderate | “…identified a promising role of AT in improving CRF…” | Yes |
| Jang (2020) [23] Australia | May 2019/4DBs | 9 (809) | AT | SAT/UC | Moderate to high | Low | “…suggests that AT has therapeutic potential in management of CRF…” | No |
| Yuan (2020) [24] China | March 2020/8DBs | 11 (832) | AT | APT/SAT/UC | High | Low | “…can effectively…, especially for those who have finished anti-tumor therapy and rarely have adverse effects.” | No |
| Zhao (2020) [19] China | June 2017/18DBs | 5 (547) | AT/Moxa | SAT/UC | Moderate to high | Critically Low | “…to be effective and safe in the treatment of CRF.” | Yes |
| Zhang (2018) [18] China | November 2016/7DBs | 10 (1327) | AT | SAT/UC | Moderate to high | Moderate | “…management and should be recommended as a beneficial alternative therapy…” | Yes |
| Ling (2014) [25] China | April 2014/16DBs | 11 (731) | AT/APT | SAT/UC | n.r. | Critically Low | “…be effective in relieving CRF, with the former producing a greater improvement.” | No |
| He (2013) [17] China | December 2012/8DBs | 7 (804) | AT/APT/Moxa | SAT | Moderate to high | Critically Low | “…appeared to be efficacious auxiliary therapeutic methods…” | Yes |
| Posadzki (2013) [26] Korea | November 2012/14DBs | 7 (548) | AT | SAT/UC | Moderate to high | Critically Low | “…it remained unclear whether the observed outcome was due to specific effects of AT…” | No |
| Zeng (2014) [27] China | May 2013/5DBs | 7 (689) | AT | SAT/UC/Self-AT/ No treatment/Waiting list | Moderate to high | Moderate | “…no statistically significant.” | Yes |
| Han (2020) [28] China | December 2018/8DBs | 6 (394) | APT | SAPT/UC | High | Critically Low | “…may be a safe therapy to relieve CRF and enhance the QoL …” | Yes |
| Huang (2021) [29] China | July 2020/9BDs | 18 (1312) | Moxa | UC | Moderate to high | Critically Low | “…can effectively improve the CRF of patients, improve the QoL …” | Yes |
| Han (2021) [30] China | May 2020/8BDs | 13 (899) | Moxa | UC | Moderate to high | Low | “… can effectively reduce cancer-related fatigue, improve QoL …” | Yes |
| Hu (2021) [31] China | April 2018/8BDs | 28 (2249) | Moxa | UC | Moderate to high | Critically Low | “… safe and effective in treating…” | Yes |
| Yu (2020) [32] China | April 2018/6BDs | 18 (1409) | Moxa | UC | Moderate to high | Low | “…can alleviate the symptoms of CRF and improve the QoL of cancer patients to a certain extent.” | No |
| Lee (2014) [33] Korea | April 2013/18BDs | 4 (374) | Moxa | UC | Moderate to high | Critically Low | “…difficult to draw the conclusion that moxibustion is an effective and safe treatment…” | Yes |
| Acupuncture-and-Moxibustion-Related Therapies | No. of Primary Studies (Total/Reported Studies) | Acupuncture Points (No. of Primary Study) |
|---|---|---|
| Acupuncture | 28/24 | ST36 (19), SP6 (15), CV6 (11), CV4 (8) |
| Acupressure | 5/4 | LI4(4), SP6 (4), ST36 (4), DU20 (3), CV6 (3), HT7 (3), LR3 (3), KI3 (3) |
| Auricular acupuncture | 7 | TF4 (6), AH6a (6), CO12 (4), CO13 (4), CO4 (3) |
| Moxibustion | 46/40 | ST36 (26), CV4 (23), CV6 (21), CV12 (13), CV8 (12) |
| Total | 79/68 | ST36 (49), CV6 (35), CV4 (32), SP6 (21), CV12 (15), CV8 (12), LI4 (11) |
| First Author (Year) | Outcomes | Number of RCTs (Number of Participants) | Relative Absolute (95% CI) | p-Value | Quality of Evidence |
|---|---|---|---|---|---|
| Tan (2021) [22] | Fatigue (short-term) (AS vs. UC) | 8 (426) | SMD −0.95 [−1.72, −0.18] | 0.02 | Low |
| Fatigue (medium-term) (AS vs. UC) | 2 (44) | SMD −0.96 [−1.60, −0.33] | 0.003 | Very low | |
| Fatigue (medium-term) (AS vs. SAS) | 2 (133) | SMD −0.29 [−0.65, −0.07] | 0.11 | Very low | |
| Fatigue (AT vs. UC) | 7 (361) | SMD −1.25 [−2.05, −0.45] | 0.0002 | Low | |
| Fatigue (AT vs. SAT) | 2 (123) | SMD −0.29 [−0.65, −0.07] | 0.11 | Very low | |
| Fatigue (acupressure vs. sham acupressure) | 2 (100) | SMD −0.26 [−0.66, −0.14] | 0.20 | Very low | |
| Jang (2020) [23] | Fatigue (BFI) (AT vs. SAT) | 6 (189) | SMD −0.93 [−1.65, −0.20] | <0.00001 | Low |
| Fatigue (BFI) (AT vs. UC) | 3(78) | SMD −2.12 [−3.21, −1.04] | <0.00001 | Low | |
| Yuan (2020) [24] | Fatigue | 11 (832) | SMD −1.06 [−1.73, −0.40] | 0.002 | Moderate |
| Fatigue (F/U) | 3 (129) | SMD −0.85 [−2.86, 1.16] | 0.41 | Very low | |
| QoL | 4 (187) | SMD 0.26 [−0.03, 0.55] | 0.08 | Very low | |
| Zhao (2020) [19] | Fatigue | 5 (547) | SMD 0.48 [0.30, 0.66] | <0.00001 | Moderate |
| Zhang (2018) [18] | Fatigue | 10 (1327) | SMD −1.26 [−1.80, −0.71] | <0.00001 | Low |
| He (2013) [17] | Fatigue | 2 (198) | OR 0.16 [0.07, 0.37] | <0.00001 | Very low |
| Zeng (2013) [27] | Fatigue (AT vs. SAT) | 3 (121) | SMD −0.82 [−1.90, 0.26] | 0.14 | Very low |
| Fatigue (AT vs. UC) | 2 (314) | SMD −2.12 [−3.21, −1.03] | 0.001 | Very low | |
| Fatigue (AT vs. no treatment) | 2 (150) | SMD −1.46 [−3.56, 0.63] | 0.17 | Very low | |
| Fatigue (AT vs. other treatment) | 2 (163) | SMD −1.12 [−3.03, 0.78] | 0.17 | Very low | |
| QoL | 3 (121) | SMD 0.99 [−0.70, 2.68] | <0.00001 | Very low | |
| Functional well-being | 3 (121) | SMD 1.38 [−1.02, 3.79] | <0.00001 | Very low | |
| Han (2020) [28] | Fatigue | 5 (170) | RR 1.76 [1.42, 2.17] | <0.00001 | Low |
| QoL | 3 (215) | MD 7.34 [5.11, 9.57] | <0.00001 | Low | |
| Huang (2021) [29] | Fatigue | 15 (1040) | SMD −1.30 [−1.44, −1.16] | <0.00001 | Low |
| QoL | 9 (572) | SMD 1.39 [0.87, 1.90] | <0.00001 | Low | |
| Han (2021) [30] | Fatigue | 13 (892) | SMD −1.58 [−2.05, −1.11] | <0.00001 | Low |
| QoL | 5 (283) | MD 11.50 [7.94, 15.06] | <0.00001 | Very low | |
| TCM syndrome | 4 (298) | MD −1.21 [−1.58, −0.84] | <0.00001 | Very low | |
| Hu (2021) [31] | Fatigue (response rate) | 6 (538) | OR 5.21 [2.66, 10.19] | <0.00001 | Low |
| Fatigue | 15 (1147) | MD 1.91 [1.29, 2.52] | <0.00001 | Low | |
| Yu (2020) [32] | Fatigue (PFS) | 8 (668) | MD −1.29 [−1.88, −0.70] | <0.001 | Moderate |
| Fatigue (BFI) | 5 (438) | MD −0.93 [−2.72, −0.86] | <0.00001 | Very low | |
| Fatigue (KPS) | 10 (714) | MD 7.08 [3.31, 10.85] | <0.00001 | Low | |
| QoL | 5 (365) | MD 9.88 [5.03, 14.73] | <0.00001 | Very low | |
| Lee (2014) [33] | Fatigue (response rate) | 4 (340) | RR 1.73 [1.29, 2.32] | 0.0003 | Very low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, T.-Y.; Ang, L.; Jun, J.H.; Alraek, T.; Lee, M.S. Acupuncture and Moxibustion for Cancer-Related Fatigue: An Overview of Systematic Reviews and Meta-Analysis. Cancers 2022, 14, 2347. https://doi.org/10.3390/cancers14102347
Choi T-Y, Ang L, Jun JH, Alraek T, Lee MS. Acupuncture and Moxibustion for Cancer-Related Fatigue: An Overview of Systematic Reviews and Meta-Analysis. Cancers. 2022; 14(10):2347. https://doi.org/10.3390/cancers14102347
Chicago/Turabian StyleChoi, Tae-Young, Lin Ang, Ji Hee Jun, Terje Alraek, and Myeong Soo Lee. 2022. "Acupuncture and Moxibustion for Cancer-Related Fatigue: An Overview of Systematic Reviews and Meta-Analysis" Cancers 14, no. 10: 2347. https://doi.org/10.3390/cancers14102347
APA StyleChoi, T.-Y., Ang, L., Jun, J. H., Alraek, T., & Lee, M. S. (2022). Acupuncture and Moxibustion for Cancer-Related Fatigue: An Overview of Systematic Reviews and Meta-Analysis. Cancers, 14(10), 2347. https://doi.org/10.3390/cancers14102347