
Pencil Beam Scanning (PBS) Intensity-Modulated Proton Therapy (IMPT) Chemoradiotherapy for Anal Canal Cancer—Single Institution Experience

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Radiotherapy
- −
- CTV-1: Tumour with a margin plus involved lymph nodes, total dose: 57.5 GyE.
- −
- CTV-2: Regional lymph node groups—perirectal (mesorectal), obturatory, inguinal, internal, external and common iliac—total dose: 45 GyE.
- −
- PTVs were generated by an expansion of 5 mm.
- −
- Both doses in 25 fractions, 5 fractions/week, simultaneous integrated boost.
2.2. Chemotherapy
2.3. Follow-Up
2.4. Statistics
3. Results
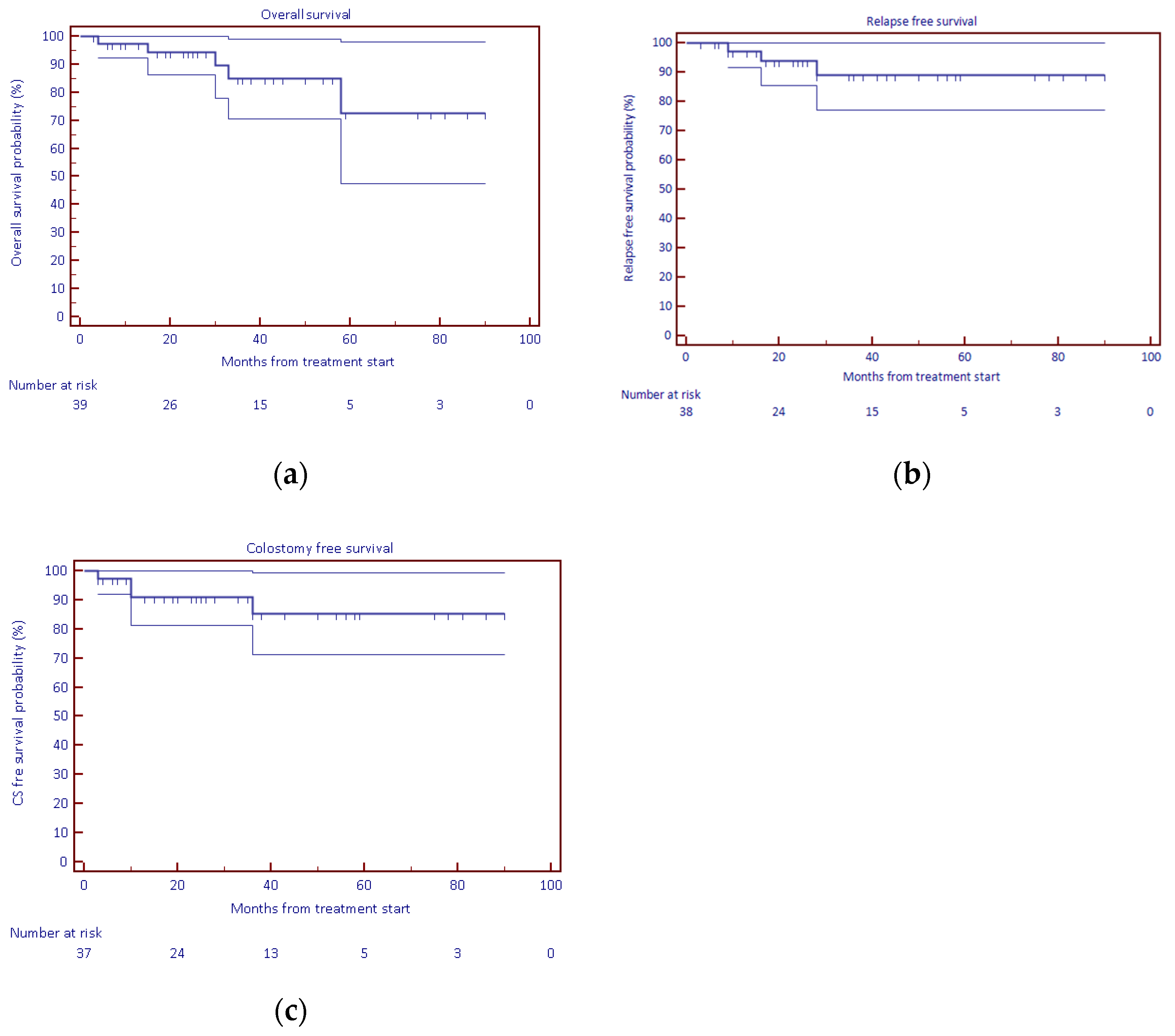
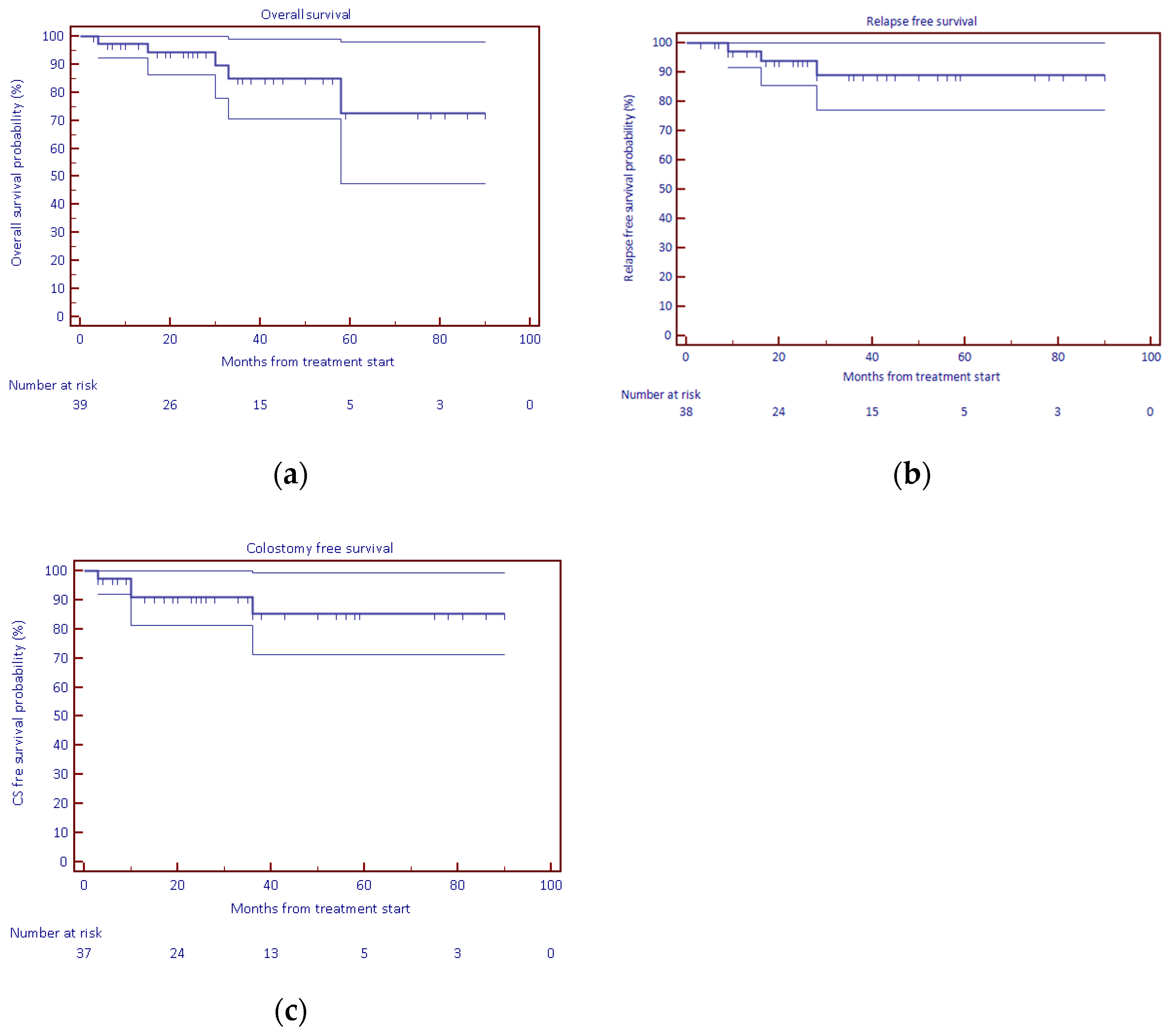
3.1. Treatment Efficacy
3.2. Colostomy
3.3. Toxicity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nigro, N.D.; Vaitkevicius, V.K.; Considine, B., Jr. Combined therapy for cancer of the anal canal: A preliminary report. Dis. Colon Rectum 1974, 17, 354–356. [Google Scholar] [CrossRef] [PubMed]
- James, R.D.; Glynne-Jones, R.; Meadows, H.M.; Cunningham, D.; Myint, A.S.; Saunders, M.P.; Maughan, T.; McDonald, A.; Essapen, S.; Leslie, M.; et al. Mitomycin or cisplatin chemoradiation with or without maintenance chemotherapy for treatment of squamous-cell carcinoma of the anus (ACT II): A randomised, phase 3, open-label, 2 × 2 factorial trial. Lancet Oncol. 2013, 14, 516–524. [Google Scholar] [CrossRef]
- Gunderson, L.L.; Winter, K.A.; Ajani, J.A.; Pedersen, J.E.; Moughan, J.; Benson, A.B.; Thomas, C.R., Jr.; Mayer, R.J.; Haddock, M.G.; Rich, T.A.; et al. Long-term update of US GI intergroup RTOG 98-11 phase III trial for anal carcinoma: Survival, relapse, and colostomy failure with concurrent chemoradiation involving fluorouracil/mitomycin versus fluorouracil/cisplatin. J. Clin. Oncol. 2012, 30, 4344–4351. [Google Scholar] [CrossRef] [PubMed]
- Ajani, J.A.; Winter, K.A.; Gunderson, L.L.; Pedersen, J.; Benson, A.B.; Thomas, C.R.; Mayer, R.J.; Haddock, M.G.; Rich, T.A.; Willett, C. Fluorouracil, mitomycin, and radiotherapy vs. fluorouracil, cisplatin, and radiotherapy for carcinoma of the anal canal: A randomized controlled trial. JAMA 2008, 299, 1914–1921. [Google Scholar] [CrossRef] [PubMed]
- Kachnic, L.A.; Winter, K.; Myerson, R.J.; Goodyear, M.D.; Willins, J.; Esthappan, J.; Haddock, M.G.; Rotman, M.; Parikh, P.J.; Safran, H.; et al. RTOG 0529: A phase 2 evaluation of dose-painted intensity modulated radiation therapy in combination with 5-fluorouracil and mitomycin-C for the reduction of acute morbidity in carcinoma of the anal canal. Int. J. Radiat. Oncol. 2013, 86, 27–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ojerholm, E.; Kirk, M.L.; Thompson, R.; Zhai, H.; Metz, J.M.; Both, S.; Ben-Josef, E.; Plastaras, J. Pencil-beam scanning proton therapy for anal cancer: A dosimetric comparison with intensity-modulated radiotherapy. Acta Oncol. 2015, 54, 1209–1217. [Google Scholar] [CrossRef] [PubMed]
- Anand, A.; Bues, M.; Rule, W.G.; Keole, S.R.; Beltran, C.J.; Yin, J.; Haddock, M.G.; Hallemeier, C.L.; Miller, R.; Ashman, J.B. Scanning proton beam therapy reduces normal tissue exposure in pelvic radiotherapy for anal cancer. Radiother. Oncol. 2015, 117, 505–508. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.; Williamson, T.; Yepes, P.; Poenisch, F.; Melkun, M.; Titt, U.; Mirkovic, D.; Beddar, S.; Mohan, R.; Holliday, E. Intensity Modulated Proton Therapy (IMPT) for Anal Canal Cancer Scientific Abstracts and Sessions. Med. Phys. 2018, 45, 484. [Google Scholar] [CrossRef]
- Meier, T.; Mascia, A.; Wolf, E.; Kharofa, J. Modelling of High-Grade Hematologic Toxicity in Anal Cancer Patients Treated with Intensity Modulated Proton Therapy (IMPT) and Volumetric Modulated Arc Therapy (VMAT). Int. J. Radiat. Oncol. 2016, 96, E145. [Google Scholar] [CrossRef]
- Kronborg, C.; Serup-Hansen, E.; Lefevre, A.; Wilken, E.E.; Petersen, J.B.; Hansen, J.; Schouboe, A.; Nyvang, L.; Spindler, K.-L.G. Prospective evaluation of acute toxicity and patient reported outcomes in anal cancer and plan optimization. Radiother. Oncol. 2018, 128, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Glynne-Jones, R.; Lim, F. Anal cancer: An examination of radiotherapy strategies. Int. J. Radiat. Oncol. 2011, 79, 1290–1301. [Google Scholar] [CrossRef] [PubMed]
- Wo, J.Y.; Plastaras, J.P.; Metz, J.M.; Jiang, W.; Yeap, B.Y.; Drapek, L.C.; Adams, J.; Baglini, C.; Ryan, D.P.; Murphy, J.E.; et al. Pencil Beam Scanning Proton Beam Chemoradiation Therapy with 5-Fluorouracil and Mitomycin-C for Definitive Treatment of Carcinoma of the Anal Canal: A Multi-institutional Pilot Feasibility Study. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Proton Therapy in Reducing Toxicity in Anal Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT03018418 (accessed on 23 September 2021).
- LET IMPT and Standard Chemotherapy in Treating Patients With Newly Diagnosed Stage I-III Anal Canla Squamous Cell Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT03690921 (accessed on 23 September 2021).
- Vitek, P.; Kubes, J.; Vondracek, V.; Vinakurau, S. Pencil beam scanning (PBS) proton radiotherapy for anal canal squamous cell cancer, dosimetry correlates with clinical outcome. In Proceedings of the 56th Annual Meeting of the Particle Therapy Cooperative Group (PTCOG), Yokohama, Japan, 11–13 May 2017. [Google Scholar]
- Mell, L.K.; Schomas, D.A.; Salama, J.K.; Devisetty, K.; Aydogan, B.; Miller, R.; Jani, A.B.; Kindler, H.L.; Mundt, A.J.; Roeske, J.; et al. Association between bone marrow dosimetric parameters and acute hematologic toxicity in anal cancer patients treated with concurrent chemotherapy and intensity-modulated radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 1431–1437. [Google Scholar] [CrossRef] [PubMed]
- Bazan, J.G.; Luxton, G.; Mok, E.C.; Koong, A.; Chang, D.T. Normal tissue complication probability modeling of acute hematologic toxicity in patients treated with intensity-modulated radiation therapy for squamous cell carcinoma of the anal canal. Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, 700–706. [Google Scholar] [CrossRef] [PubMed]
- Lesca, A.; Arcadipane, F.; Ragona, R.; Lesca, A.; Gallio, E.; Mistrangelo, M.; Trino, E.; Cassoni, P.; Arena, V.; Baccega, M.; et al. Dose to Pelvic Bone Marrow Defined with FDG-PET Predicts for Hematologic Nadirs in Anal Cancer Patients Treated with Concurrent Chemo-radiation. Cancer Investig. 2018, 36, 279–288. [Google Scholar] [CrossRef]
- Knowles, G.; Haigh, R.; McLean, C.; Phillips, H. Late effects and quality of life after chemo-radiation for the treatment of anal cancer. Eur. J. Oncol. Nurs. 2015, 19, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Sodergren, S.C.; Vassiliou, V.; Dennis, K.; Tomaszewski, K.A.; Gilbert, A.; Glynne-Jones, R.; Nugent, K.; Sebag-Montefiore, D.; Johnson, C.D.; EORTC Quality of Life Group. Systematic review of the quality of life issues associated with anal cancer and its treatment with radiochemotherapy. Support. Care Cancer 2015, 23, 3613–3623. [Google Scholar] [CrossRef] [PubMed]
- Welzel, G.; Hägele, V.; Wenz, F.; Mai, S.K. Quality of life outcomes in patients with anal cancer after combined radiochemotherapy. Strahlenther. Onkol. 2011, 187, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Haas, S.; Faaborg, P.; Liao, D.; Laurberg, S.; Gregersen, H.; Lundby, L.; Christensen, P.; Krogh, K. Anal sphincter dysfunction in patients treated with primary radiotherapy for anal cancer: A study with the functional lumen imaging probe. Acta Oncol. 2018, 57, 465–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Epidermoid Anal Cancer: Results from the UKCCCR randomised trial of radiotherapy alone versus radiotherapy, 5-fluorouracil, and mitomycin. UKCCCR Anal Cancer Trial Working Party. UK Co-ordinating Committee on Cancer Research. Lancet 1996, 348, 1049–1054.


{kind=link}
{kind=link}
| Parameter | Nr. | Rem. | |
|---|---|---|---|
| N | 39 | ||
| Male | 8 | 20.5% | |
| Female | 31 | 79.5% | |
| Race | All Caucasian | ||
| ECOG status 0 | 35 | 89.7% | |
| ECOG status 1 | 4 | 10.3% | |
| Age at diagnosis | Median 58 (41–82) | ||
| Staging (all M0) | |||
| T1N0 | 3 | 7.7% | |
| T2N0 | 14 | 35.9% | |
| T3N0 | 7 | 17.9% | |
| T4N0 | 1 | 2.6% | |
| T2N1 | 4 | 10.3% | |
| T3N1 | 3 | 7.7% | |
| T2N2 | 1 | 2.6% | |
| T4N2 | 2 | 5.1% | |
| T1N3 | 1 | 2.6% | |
| T2N3 | 1 | 2.6% | |
| T3N3 | 1 | 2.6% | |
| T4N3 | 1 | 2.6% | |
| Histology | |||
| Spinocellular carcinoma | 39 | ||
| Grade 1 | 5 | 12.8% | |
| Grade 2 | 15 | 38.5% | |
| Grade 3 | 8 | 20.5% | |
| Unknown | 11 | 28.2% | |
| p16 positive/negative/not assessed | 9/5/25 | 23.1%/12.8%/64.1% | |
| Synchronous malignancy | 1 | Synchronous uterine cervical cancer | |
| Colostomy before radiotherapy | 2 | Derivative colostomy in locally advanced disease |
| Survival Proportion | Standard Error Confidence Interval 95% | ||
|---|---|---|---|
| 2-year overall survival | 94.2% | 4.0 | 90.2–98.2% |
| 2-year relapse free survival | 93.8% | 4.3 | 89.5–98.1% |
| 2-year colostomy free survival | 91.0% | 5.0 | 96.0–96.0% |
| Grade 1 | Grade 2 | Grade 3 | Grade 4 | |
|---|---|---|---|---|
| Leukopenia | 9 (23.08%) | 7 (17.9%) | 3 (7.7%) | 2 (5.1%) |
| Neutropenia | 1 (2.56%) | 1 (2.6%) | 3 (7.7%) | 2 (5.1%) |
| Thrombocytopenia | 1 (2.56%) | 2 (5.1%) | 0 | 0 |
| Anaemia | 8 (20.5%) | 1 (2.6%) | 0 | 0 |
| Worst overall | 10 (25.6%) | 8 (20.5%) | 3 (7.7%) | 2 (5.1%) |
| Grade 1 | Grade 2 | Grade 3 | Grade 4 | |
|---|---|---|---|---|
| Dermatitis | 4 (10.3%) | 24 (61.5%) | 9 (23.1%) | 0 |
| Gastrointestinal | ||||
| Diarrhoea | 1 (2.6%) | 13 (38.2%) | 2 (5.1%) | 1 (2.6%) |
| Anal pain | 1 (2.6%) | 2 (5.1%) | 2 (5.1%) | 0 |
| Proctitis | 0 | 4 (10.3%) | 0 | 0 |
| Enterocolitis | 0 | 0 | 1 (2.6%) | 1 (2.6%) |
| Ileal obstruction | 0 | 0 | 0 | 1 (2.6%) |
| Nausea | 0 | 3 (7.7%) | 0 | 0 |
| Genitourinary | ||||
| Urinary tract pain | 3 (7.7%) | 4 (10.3%) | 0 | 0 |
| Urinary urgency | 1 (2.6%) | 2 (5.1%) | 0 | 0 |
| Other (general) | ||||
| Dehydration | 0 | 2 (5.1%) | 3 (7.7%) | 0 |
| Sepsis | 0 | 0 | 0 | 1 (2.6%) |
| Other (laboratory) | ||||
| Transaminase (AST, ALT) increased | 4 (10.3%) | |||
| GGT, ALP increased | 3 (7.7%) | |||
| Creatinine increased | 3 (7.7%) | 3 (7.7%) | 0 | |
| Hypomagnesemia | 3 (7.7%) | |||
| Hypoalbuminemia | 1 (2.6%) | |||
| Hypokalaemia | 0 | 2 (5.1%) | 2 (5.1%) | 1 (2.6%) |
| Grade 1 | Grade 2 | Grade 3 | Grade 4 | |
|---|---|---|---|---|
| Skin (perianal region) | ||||
| Skin atrophy | 12 (35.3%) | 9 (26.5%) | 0 | 0 |
| Telangiectasia | 14 (41.2%) | 0 | 0 | 0 |
| Skin ulceration | 0 | 0 | 1 (2.9%) | 1 (2.9%) |
| Subcutaneous tissue fibrosis (perianal region) | 4 (11.8%) | 0 | 1 (2.9%) | 0 |
| Proctitis (post-radiation) | 5 (14.7%) | 13 (38.2%) | 1 (2.9%) | 0 |
| Vaginal stricture (synechia) | 0 | 3 (11.5%) | 2 (7.7%) | 0 |
| Anal stenosis | 4 (11.8%) | 8 (23.5%) | 1 (2.9%) | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vítek, P.; Kubeš, J.; Vondráček, V.; Andrlik, M.; Navrátíl, M.; Zapletal, R.; Haas, A.; Dědečková, K.; Ondrová, B.; Grebenyuk, A.; et al. Pencil Beam Scanning (PBS) Intensity-Modulated Proton Therapy (IMPT) Chemoradiotherapy for Anal Canal Cancer—Single Institution Experience. Cancers 2022, 14, 185. https://doi.org/10.3390/cancers14010185
Vítek P, Kubeš J, Vondráček V, Andrlik M, Navrátíl M, Zapletal R, Haas A, Dědečková K, Ondrová B, Grebenyuk A, et al. Pencil Beam Scanning (PBS) Intensity-Modulated Proton Therapy (IMPT) Chemoradiotherapy for Anal Canal Cancer—Single Institution Experience. Cancers. 2022; 14(1):185. https://doi.org/10.3390/cancers14010185
Chicago/Turabian StyleVítek, Pavel, Jiří Kubeš, Vladimír Vondráček, Michal Andrlik, Matěj Navrátíl, Radek Zapletal, Alexandra Haas, Kateřina Dědečková, Barbora Ondrová, Alexander Grebenyuk, and et al. 2022. "Pencil Beam Scanning (PBS) Intensity-Modulated Proton Therapy (IMPT) Chemoradiotherapy for Anal Canal Cancer—Single Institution Experience" Cancers 14, no. 1: 185. https://doi.org/10.3390/cancers14010185
APA StyleVítek, P., Kubeš, J., Vondráček, V., Andrlik, M., Navrátíl, M., Zapletal, R., Haas, A., Dědečková, K., Ondrová, B., Grebenyuk, A., & Rosina, J. (2022). Pencil Beam Scanning (PBS) Intensity-Modulated Proton Therapy (IMPT) Chemoradiotherapy for Anal Canal Cancer—Single Institution Experience. Cancers, 14(1), 185. https://doi.org/10.3390/cancers14010185