
Meta-Analysis of Survival and Development of a Prognostic Nomogram for Malignant Pleural Mesothelioma Treated with Systemic Chemotherapy

Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Selection of Articles
2.2. Outcome Measures and Statistical Analysis
3. Results
3.1. Demographic Data of Platinum-Pemetrexed Regimen
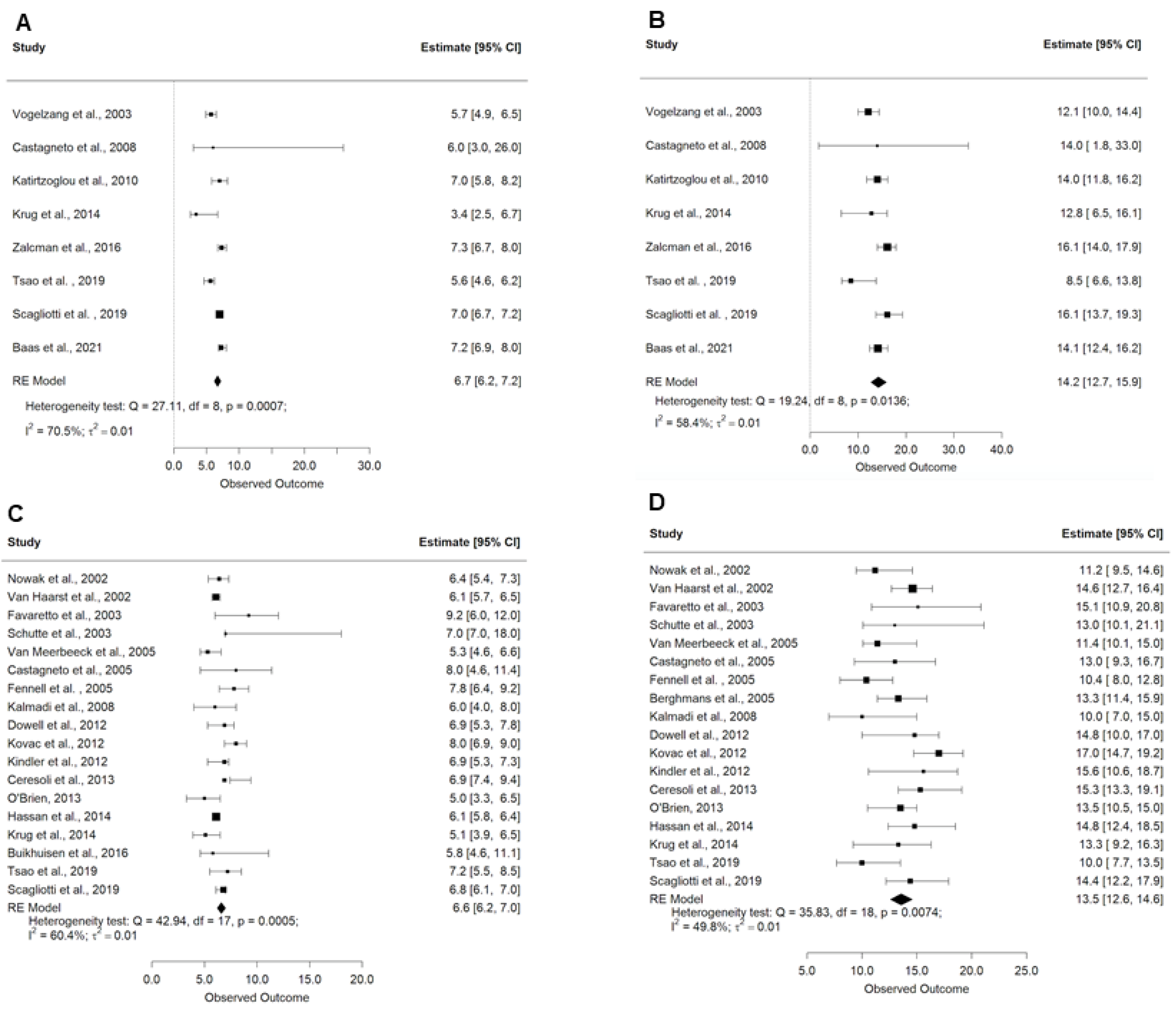
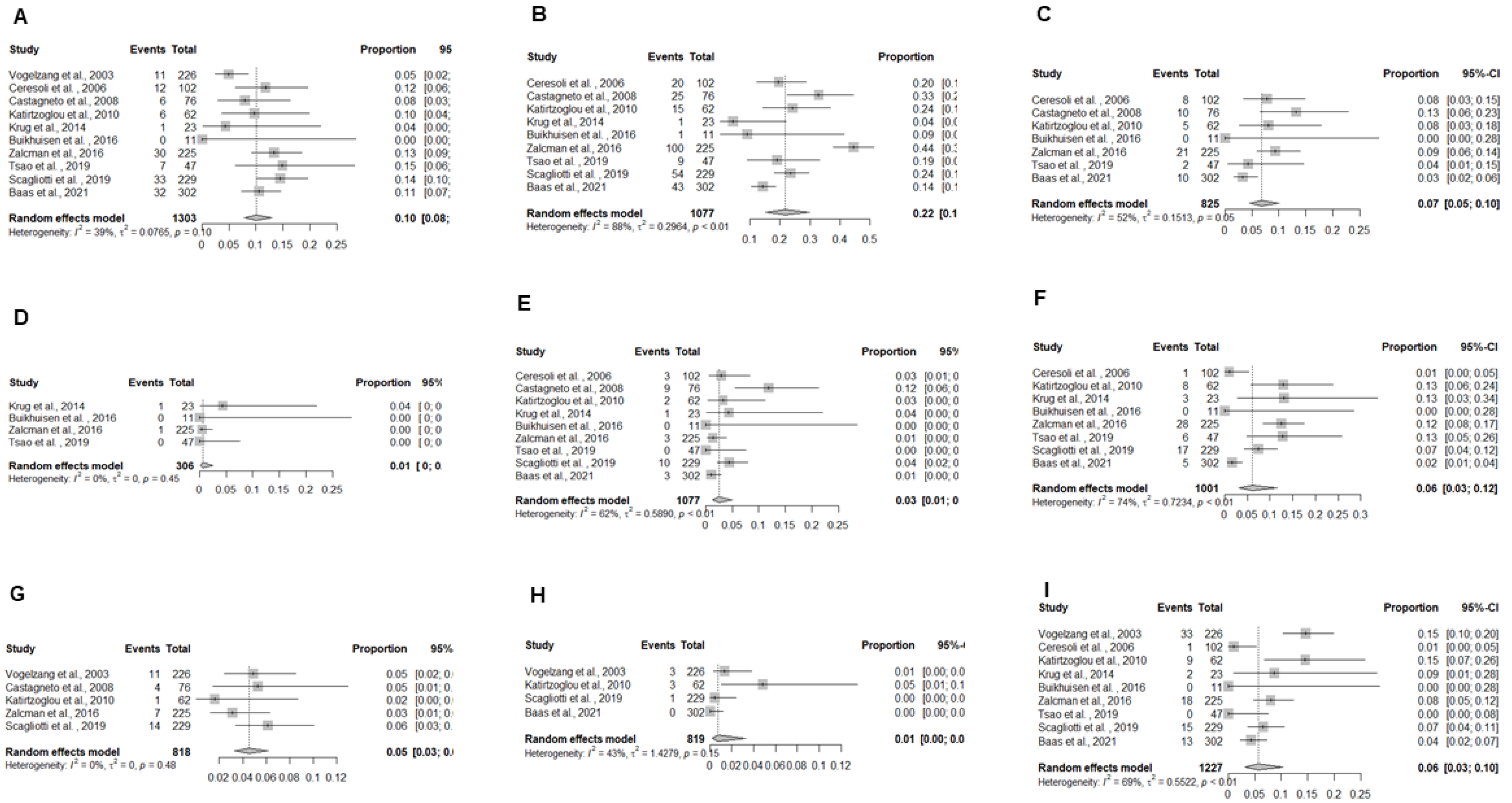
3.2. Treatment Outcomes, Radiological Response, and Toxicity Summary Data of Platinum-Pemetrexed Regimen
3.3. Demographic Data of Experimental Regimens
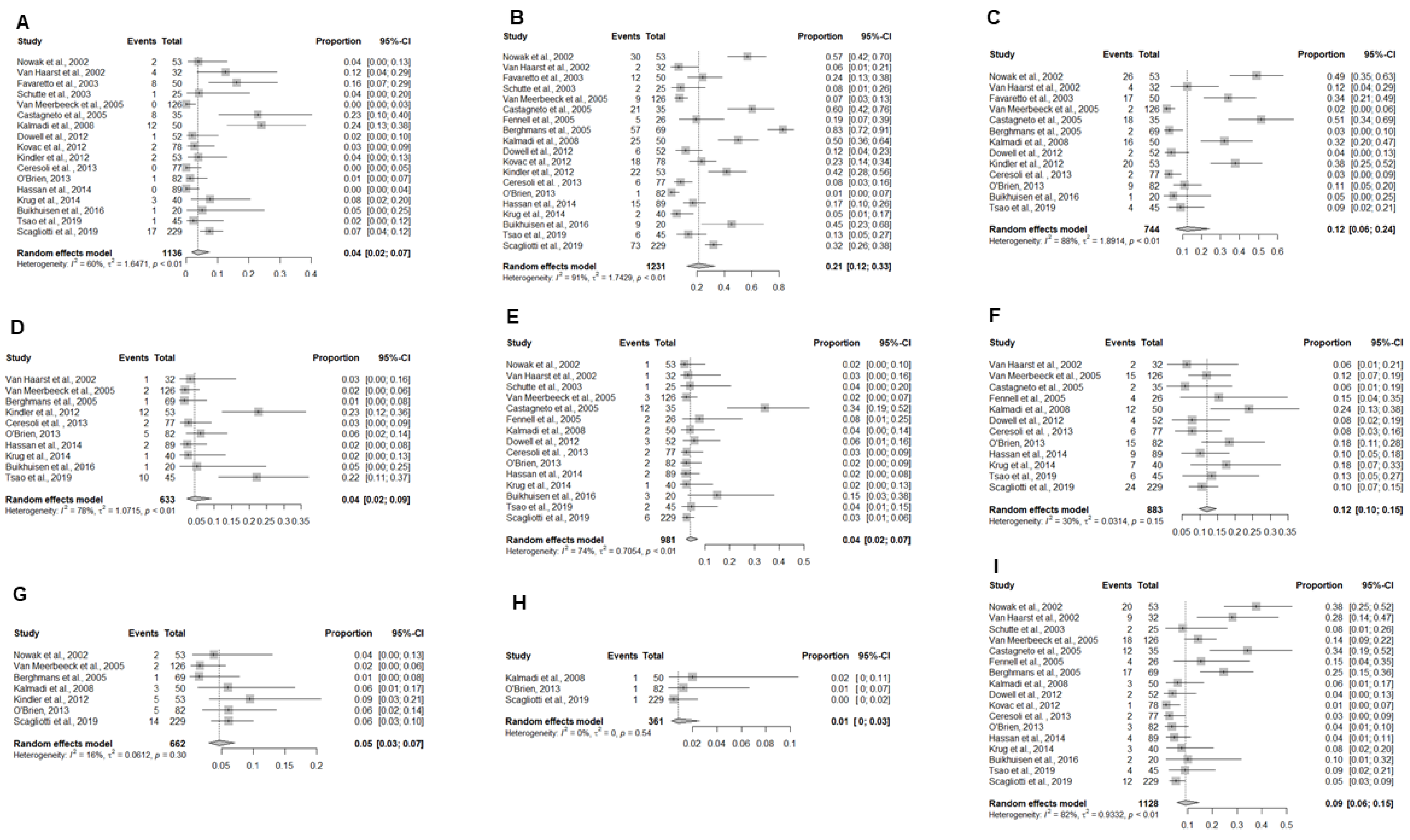
3.4. Outcomes, Radiological Response, and Toxicity Summary Data of Experimental Regimens
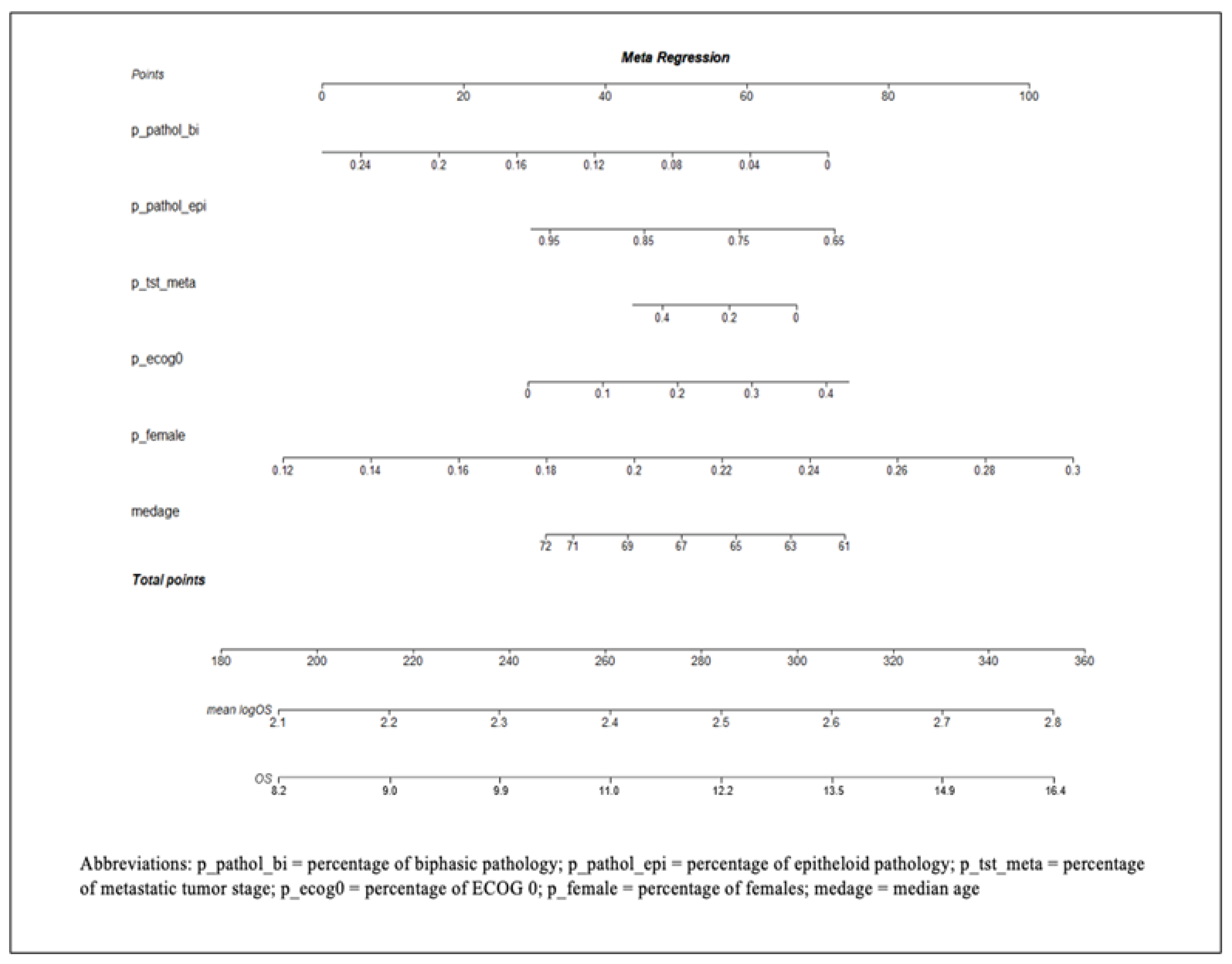
3.5. Development of a Prognostic Nomogram to Estimate Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Acronyms | Duration | Type of Study | Treatment | Primary End Point | Secondary Endpoint | N | Median Age | Sex [No.(%)] | ECOG Performance Status [No.(%)] | Tumour stage | Tumour Pathology | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | 0 | 1 | 2 | Locally Advanced | Metastatic | Epithelioid | Biphasic | Sarcomatoid | ||||||||||
| Nowak et al. [34] | 2002 | NA | NA | II | Cisplatin + Gemcitabine | ORR | PFS, OS, QoL | 53 | 63 | 45 (85%) | 8 (15%) | 17 (32%) | 31 (59%) | 5 (9%) | 33 (62%) | 13 (25%) | 42 (79%) | 2 (4%) | 7 (13%) |
| Van Haarst et al. [35] | 2002 | NA | April 1999–Dec 1999 | II | Cisplatin + Gemcitabine | ORR | PFS, OS, QoL | 32 | 56 | 27 (86%) | 5 (14%) | 5 (14%) | 26 (85%) | 1 (1%) | 15 (48%) | 13 (41%) | 26 (82%) | 3 (9%) | 3 (9%) |
| Favaretto et al. [36] | 2003 | NA | 1996–2000 | II | Carboplatin + Gemcitabine | RR | OS, PFS, Toxicity | 50 | 60 | 34 (68%) | 16 (32%) | 11 (22%) | 33 (66%) | 6 (12%) | 11 (22%) | 12 (24%) | 34 (68%) | 13 (26%) | 3 (6%) |
| Schutte et al. [37] | 2003 | NA | 1999–2001 | II | Oxaliplatin + Gemcitabine | ORR | OS, PFS, Toxicity | 25 | 65 | 18 (72%) | 7 (28%) | 7 (28%) | 13 (52%) | 5 (20%) | 13 (52%) | 10 (25%) | 16 (64%) | 8 (32%) | 1 (3%) |
| Van Meerbeeck et al. [38] | 2005 | NA | NA | III | Cisplatin + Raltitrexed | OS | PFS, RR, safety, QoL | 126 | 59 | 104 (83%) | 22 (17%) | 32 (25%) | 77 (61%) | 17 (14%) | NA | NA | 95 (75%) | 18 (14%) | 5 (4%) |
| Castagneto et al. [39] | 2005 | NA | 1999–2001 | II | Cisplatin + Gemcitabine | ORR | OS, PFS | 35 | 61 | 21 (60%) | 14 (40%) | 33 (94%) | 2 (6%) | 8 (23%) | 16 (46%) | 22 (63%) | 10 (29%) | 3 (8%) | |
| Fennell et al. [40] | 2005 | NA | NA | II | Oxaliplatin + Vinorelbine | ORR | OS, PFS | 26 | 60 | 21 (87%) | 5 (13%) | 6 (16%) | 15 (69%) | 5 (13%) | 6 (16%) | 15 (79%) | 13 (75%) | 7 (18%) | 5 (13%) |
| Berghmans et al. [41] | 2005 | NA | 1998–2003 | II | Cisplatin + Epirubicin | ORR | Toxicity and OS | 69 | 62 | 59 (93%) | 10 (7%) | NA | NA | NA | 18 (12%) | 23 (19%) | 43 (74%) | 6 (10%) | 9 (16) |
| Kalmadi et al. [42] | 2008 | SWOG 9810 | 1999–2000 | II | Cisplatin + Gemcitabine | OS | ORR, Toxicity | 50 | 69 | 44 (88%) | 6 (12%) | 13 (26%) | 27 (54%) | 10 (20%) | NA | NA | 25 (50%) | 3 (6%) | 4 (8%) |
| Dowell et al. [43] | 2012 | NA | NA | II | Cisplatin + Pemetrexed + Bevacizumab | PFS | RR, OS and toxicity | 52 | 66 | 44 (85%) | 8 (15%) | 17 (33%) | 35 (67%) | NA | NA | NA | 32 (62%) | 11 (21%) | 7 (13%) |
| Kovac et al. [44] | 2012 | NA | 2002–2008 | II | Cisplatin + Gemcitabine | RR | OS, PFS, Toxicity | 78 | 58 | 58 (74%) | 20 (26%) | 14 (18%) | 51 (65%) | 13 (17%) | 38 (49%) | 22 (29%) | 56 (72%) | 15 (19%) | 4 (5%) |
| Kindler et al. [45] | 2012 | NA | 2001–2005 | II | Cisplatin + Gemcitabine + Bevacizumab | PFS | OS | 53 | 62 | 39 (73%) | 14 (27%) | 24 (45%) | 29 (55%) | NA | NA | NA | 39 (74%) | 14 (26%) | NA |
| Ceresoli et al. [46] | 2013 | NA | 2007–2009 | II | Carboplatin + Pemetrexed + Bevacizumab | PFS | Toxicity, RR and OS | 77 | 67 | 49 (64%) | 27 (36%) | 58 (76%) | 18 (24%) | NA | NA | NA | 61 (80%) | 6 (8%) | 5 (7%) |
| O’Brien et al. [47] | 2013 | EORTC 08052 | 2007–2010 | II | Cisplatin + Bortezomib | PFSR-18 | ORR, OS, PFS and safety | 82 | 55 | 55 (67%) | 27 (33%) | NA | 73 (89%) | NA | 35 (43%) | 28 (34%) | 48 (59%) | 11 (13%) | 6 (7%) |
| Hassan et al. [48] | 2014 | NA | 2009–2010 | II | Cisplatin + Pemetrexed+ Amatuximab | 6 months PFS | ORR, OS, PFS and safety | 89 | 67 | 69 (78%) | 20 (22%) | NA | NA | NA | 35 (39%) | 43 (48%) | 79 (89%) | 10 (11%) | NA |
| Krug et al. [16] | 2014 | NA | NA | II | Cisplatin + Pemetrexed + CBP50 | PFS | OS, DCR, and safety/toxicity | 40 | 64 | 32 (80%) | 8 (20%) | 14 (35%) | 25 (63%) | 1 (3%) | NA | NA | 30 (75%) | 6 (15%) | 4 (10%) |
| Buikhuisen et al. [17] | 2016 | NA | 2009–2012 | II | Cisplatin + Pemetrexed + Axitinib | RR | OS, PFS | 20 | 63 | 15 (75%) | 5 (25%) | NA | NA | NA | NA | NA | 16 (80%) | 2 (10%) | 2 (10%) |
| Tsao et al. [18] | 2019 | SWOG S0905 | 2011–2016 | II | Cisplatin + Pemetrexed + Ceradinib | PFS | OS, DCR, and safety/toxicity | 45 | 72 | 38 (84%) | 7 (16%) | NA | NA | NA | NA | NA | 34 (76%) | 11 (24%) | NA |
| Scagliotti et al. [19] | 2019 | LUME-Meso | 2016–2018 | III | Cispatin + Pemetrexed + Nintedinab | PFS | OS, ORR, DCR, QoL | 229 | 66 | 165 (72%) | 64 (28%) | 99 (43%) | 130 (57%) | NA | 89 (39%) | 113 (49%) | 220 (96%) | 9 (4%) | NA |
| Author | Year | OS (Months) | 1 yr. Survival Rates | 2 yr. Survival Rates | PFS (Months) | Objective Response Rate (ORR %) | Radiological Response Rate [No. (%)] | Toxicity summary (Grade 3 and 4) n (%) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Complete Response | Partial Response | Stable Disease | Progressive Disease | Disease Control Rate (%) | Blood and Lymphatic System Disorders | Cardiac Disorders | Gastrointestinal Disorders | Fatigue | Infections | Respiratory Disorders | Skin Disorders | Nausea and Vomiting | |||||||||
| Anemia | Neutropenia | Thrombocytopenia | |||||||||||||||||||
| Nowak et al. [34] | 2002 | 17.3 | NA | NA | 6.4 | 33 | 0 | 17 (33%) | 31 (60%) | 4 (7%) | 93 | 2 (7%) | 30 (56%) | 26 (49%) | NA | 1 (2%) | NA | 2 (4%) | NA | NA | 20 (37%) |
| Van Haarst et al. [35] | 2002 | 14.6 | NA | NA | 6.1 | 16 | 0 | 4 (16%) | 18 (72%) | 3 (12%) | 88 | 4 (13%) | 2 (6%) | 4 (13%) | 1 (3%) | 1 (3%) | 2 (6%) | 0 | 0 | 0 | 9 (29%) |
| Favaretto et al. [36] | 2003 | 15.1 | 8 | 4.5 | 9.2 | 26 | 0 | 13 (26%) | 25 (50%) | 12 (24%) | 76 | 8 (16%) | 12 (24%) | 17 (34%) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Schutte et al. [37] | 2003 | 13 | 6.7 | NA | 7 | 40 | 0 | 10 (40%) | 6 (24%) | 9 (36%) | 64 | 1 (4%) | 2 (8%) | 0 | NA | 1 (4%) | NA | NA | NA | NA | 2 (8%) |
| Van Meerbeeck et al. [38] | 2005 | 11.4 | 5.2 | 2.1 | 5.3 | 24 | 2 (2%) | 24 (26%) | 58 (63%) | NA | 89 | 4 (3%) | 9 (7%) | 2 (2%) | 2 (2%) | 3 (2%) | 15 (12%) | 2 (2%) | NA | NA | 18 (14%) |
| Castagneto et al. [39] | 2005 | 13 | NA | NA | 8 | 26 | 0 | 9 (26%) | 14 (40%) | 11 (31%) | 66 | 8 (24%) | 21 (61%) | 18 (52%) | NA | 12 (35%) | 2 (6%) | NA | NA | NA | 12 (35%) |
| Fennell et al. [40] | 2005 | 10.4 | 2.8 | NA | 7.8 | 23 | 0 | 6 (23%) | 17 (65%) | 3 (12%) | 88 | NA | 5 (18%) | NA | NA | 2 (6%) | 4 (12%) | NA | NA | NA | 4 (12%) |
| Berghmans et al. [41] | 2005 | 13.3 | 6.6 | NA | NA | 19 | 0 | 12 (19%) | 25 (40%) | 24 (38%) | 59 | NA | 57 (84%) | 2 (3%) | 1 (2%) | NA | NA | 1 (2%) | 2 (3%) | NA | 17 |
| Kalmadi et al. [42] | 2008 | 10 | 3 | NA | 6 | 12 | 1 (2%) | 5 (10%) | 25 (50%) | 19 (38%) | 62 | 12 (24%) | 25 (50%) | 16 (32%) | NA | 2 (4%) | 12 (24%) | 3 (6%) | NA | 1 (2%) | 3 (6%) |
| Dowell et al. [43] | 2012 | 14.8 | NA | NA | 6.9 | 40 | NA | NA | 35% | NA | 35 | 1 (2%) | 6 (11%) | 2 (4%) | NA | 3 (6%) | 4 (8%) | NA | NA | NA | 2 (4%) |
| Kovac et al. [44] | 2012 | 17 | NA | NA | 8 | 50 | 4 (5%) | 35 (45%) | 35 (45%) | 4 (5%) | 95 | 2 (3%) | 18 (23%) | NA | NA | NA | NA | NA | NA | NA | 1 (1%) |
| Kindler et al. [45] | 2012 | 15.6 | 9.1 | 4.8 | 6.9 | 25 | 0 | 13 (25%) | 27 (51%) | 12 (28%) | 75 | 2 (4%) | 22 (42%) | 20 (38%) | 12 (23%) | NA | NA | 5 (10%) | NA | NA | NA |
| Ceresoli et al. [46] | 2013 | 15.3 | 9.5 | 3.9 | 6.9 | 34 | NA | 24 (34%) | 44 (58%) | NA | 92 | 3 (4%) | 6 (8%) | 2 (3%) | 2 (3%) | 2 (3%) | 6 (8%) | NA | 1 (1%) | NA | 2 (3%) |
| O’Brien et al. [47] | 2013 | 13.5 | 7.5 | NA | 5 | 27 | 2 (2%) | 21 (29%) | 39 (49%) | 16 (20%) | 80 | 1 (1%) | 1 (1%) | 9 (11%) | 5 (6%) | 2 (2%) | 15 (18%) | 5 (6%) | NA | 1 (1%) | 3 (3%) |
| Hassan et al. [48] | 2014 | 14.8 | NA | NA | 6.1 | 33 | 0 | 33% | 42% | 8% | 75 | 10 (11%) | 15 (17%) | 0% | 2 (3%) | 2 (3%) | 9 (10%) | 0 | 3 (4%) | 0% | 4 (5%) |
| Krug et al. [16] | 2014 | 13.3 | NA | NA | 5.1 | 31 | 0 | 12 (31%) | 15 (38%) | NA | 69 | 3 (8%) | 2 (6%) | NA | 1 (3%) | 1 (3%) | 7 (18%) | NA | NA | NA | 3 (8%) |
| Buikhuisen et al. [17] | 2016 | 18.9 | NA | NA | 5.8 | 36 | NA | 8 (36%) | 9 (43%) | NA | 79 | 1 (5%) | 9 (45%) | 1 (5%) | 1 (5%) | 3 (15%) | 0 | NA | 1 (5%) | NA | 2 (10%) |
| Tsao et al. [18] | 2019 | 10 | NA | NA | 7.2 | 50 | NA | NA | NA | NA | NA | 1 (2%) | 6 (13%) | 4 (9%) | 10 (22%) | 2 (4%) | 6 (13%) | NA | NA | NA | 4 (9%) |
| Scagliotti et al. [19] | 2019 | 14.4 | NA | NA | 6.8 | 45 | NA | 103 (45%) | NA | NA | 91 | 17 (7%) | 73 (32%) | NA | NA | 6 (3%) | 24 (11%) | 14 (6%) | NA | 1 (1%) | 12 (5%) |
References
- Robinson, B.W.; Musk, A.W.; Lake, R.A. Malignant mesothelioma. Lancet 2005, 366, 397–408. [Google Scholar] [CrossRef]
- Delgermaa, V.; Takahashi, K.; Park, E.-K.; Le, G.V.; Hara, T.; Sorahan, T. Global mesothelioma deaths reported to the World Health Organization between 1994 and 2008. Bull. World Health Organ. 2011, 89, 716–724. [Google Scholar] [CrossRef]
- Kindler, H.L.; Ismaila, N.; Armato, S.G.; Bueno, R.; Hesdorffer, M.; Jahan, T.; Jones, C.M.; Miettinen, M.; Pass, H.; Rimner, A.; et al. Treatment of Malignant Pleural Mesothelioma: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2018, 36, 1343–1373. [Google Scholar] [CrossRef]
- Baas, P.; Scherpereel, A.; Nowak, A.K.; Fujimoto, N.; Peters, S.; Tsao, A.S.; Mansfield, A.S.; Popat, S.; Jahan, T.; Antonia, S.; et al. First-line nivolumab plus ipilimumab in unresectable malignant pleural mesothelioma (CheckMate 743): A multicentre, randomised, open-label, phase 3 trial. Lancet 2021, 397, 375–386. [Google Scholar] [CrossRef]
- Scagliotti, G.V.; Shin, D.-M.; Kindler, H.L.; Vasconcelles, M.J.; Keppler, U.; Manegold, C.; Burris, H.; Gatzemeier, U.; Blatter, J.; Symanowski, J.T.; et al. Phase II Study of Pemetrexed With and Without Folic Acid and Vitamin B 12 as Front-Line Therapy in Malignant Pleural Mesothelioma. J. Clin. Oncol. 2003, 21, 1556–1561. [Google Scholar] [CrossRef]
- Vogelzang, N.J.; Rusthoven, J.J.; Symanowski, J.; Denham, C.; Kaukel, E.; Ruffie, P.; Gatzemeier, U.; Boyer, M.; Emri, S.; Manegold, C.; et al. Phase III Study of Pemetrexed in Combination with Cisplatin Versus Cisplatin Alone in Patients with Malignant Pleural Mesothelioma. J. Clin. Oncol. 2003, 21, 2636–2644. [Google Scholar] [CrossRef] [PubMed]
- Ceresoli, G.L.; Zucali, P.A.; Favaretto, A.G.; Grossi, F.; Bidoli, P.; Del Conte, G.; Ceribelli, A.; Bearz, A.; Morenghi, E.; Cavina, R.; et al. Phase II Study of Pemetrexed Plus Carboplatin in Malignant Pleural Mesothelioma. J. Clin. Oncol. 2006, 24, 1443–1448. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Zang, J.; Xu, J.; Xiang, C.; He, J.; Zou, S. Multi-level Model Synthesis of Median Survival Time in Meta-analysis. Epidemiology 2015, 26, e2–e3. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Ceresoli, G.L.; Aerts, J.G.; Dziadziuszko, R.; Ramlau, R.; Cedres, S.; van Meerbeeck, J.P.; Mencoboni, M.; Planchard, D.; Chella, A.; Crinò, L.; et al. Tumour Treating Fields in combination with pemetrexed and cisplatin or carboplatin as first-line treatment for unresectable malignant pleural mesothelioma (STELLAR): A multicentre, single-arm phase 2 trial. Lancet Oncol. 2019, 20, 1702–1709. [Google Scholar] [CrossRef]
- Zalcman, G.; Mazieres, J.; Margery, J.; Greillier, L.; Audigier-Valette, C.; Moro-Sibilot, D.; Molinier, O.; Corre, R.; Monnet, I.; Gounant, V.; et al. Bevacizumab for newly diagnosed pleural mesothelioma in the Mesothelioma Avastin Cisplatin Pemetrexed Study (MAPS): A randomised, controlled, open-label, phase 3 trial. Lancet 2016, 387, 1405–1414. [Google Scholar] [CrossRef]
- Castagneto, B.; Botta, M.; Aitini, E.; Spigno, F.; Degiovanni, D.; Alabiso, O.; Serra, M.; Muzio, A.; Carbone, R.; Buosi, R.; et al. Phase II study of pemetrexed in combination with carboplatin in patients with malignant pleural mesothelioma (MPM). Ann. Oncol. 2008, 19, 370–373. [Google Scholar] [CrossRef] [PubMed]
- Katirtzoglou, N.; Gkiozos, I.; Makrilia, N.; Tsaroucha, E.; Rapti, A.; Stratakos, G.; Fountzilas, G.; Syrigos, K.N. Carboplatin plus pemetrexed as first-line treatment of patients with malignant pleural mesothelioma: A phase II study. Clin. Lung Cancer 2010, 11, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Krug, L.M.; Wozniak, A.J.; Kindler, H.L.; Feld, R.; Koczywas, M.; Morero, J.L.; Rodriguez, C.P.; Ross, H.J.; Bauman, J.E.; Orlov, S.V.; et al. Randomized phase II trial of pemetrexed/cisplatin with or without CBP501 in patients with advanced malignant pleural mesothelioma. Lung Cancer 2014, 85, 429–434. [Google Scholar] [CrossRef]
- Buikhuisen, W.A.; Scharpfenecker, M.; Griffioen, A.W.; Korse, C.M.; Van Tinteren, H.; Baas, P. A randomized phase II study adding axitinib to pemetrexed-cisplatin in patients with malignant pleural mesothelioma: A single-center trial combining clinical and translational outcomes. J. Thorac. Oncol. 2016, 11, 758–768. [Google Scholar] [CrossRef]
- Tsao, A.S.; Miao, J.; Wistuba, I.I.; Vogelzang, N.J.; Heymach, J.V.; Fossella, F.V.; Lu, C.; Velasco, M.R.; Box-Noriega, B.; Hueftle, J.G.; et al. Phase II trial of cediranib in combination with cisplatin and pemetrexed in chemotherapy-naïve patients with unresectable malignant pleural mesothelioma (SWOG S0905). J. Clin. Oncol. 2019, 37, 2537–2547. [Google Scholar] [CrossRef]
- Scagliotti, G.V.; Gaafar, R.; Nowak, A.K.; Nakano, T.; van Meerbeeck, J.; Popat, S.; Vogelzang, N.J.; Grosso, F.; Aboelhassan, R.; Jakopovic, M.; et al. Nintedanib in combination with pemetrexed and cisplatin for chemotherapy-naive patients with advanced malignant pleural mesothelioma (LUME-Meso): A double-blind, randomised, placebo-controlled phase 3 trial. Lancet Respir. Med. 2019, 7, 569–580. [Google Scholar] [CrossRef]
- Krug, L.M.; Pass, H.I.; Rusch, V.W.; Kindler, H.L.; Sugarbaker, D.J.; Rosenzweig, K.E.; Flores, R.; Friedberg, J.S.; Pisters, K.; Monberg, M.; et al. Multicenter phase II trial of neoadjuvant pemetrexed plus cisplatin followed by extrapleural pneumonectomy and radiation for malignant pleural mesothelioma. J. Clin. Oncol. 2009, 27, 3007–3013. [Google Scholar] [CrossRef]
- Stephenson, J.; Imrie, J. Why do we need randomised controlled trials to assess behavioural interventions? BMJ 1998, 316, 611–613. [Google Scholar] [CrossRef]
- Tang, H.; Foster, N.R.; Grothey, A.; Ansell, S.M.; Goldberg, R.M.; Sargent, D.J. Comparison of error rates in single-arm versus randomized phase II cancer clinical trials. J. Clin. Oncol. 2010, 28, 1936–1941. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.R.; Stadler, W.M.; Ratain, M.J. Randomized phase II trials: A long-term investment with promising returns. J. Natl. Cancer Inst. 2011, 103, 1093–1100. [Google Scholar] [CrossRef]
- Zhao, W. A better alternative to stratified permuted block design for subject randomization in clinical trials. Stat. Med. 2014, 33, 5239–5248. [Google Scholar] [CrossRef] [PubMed]
- Berger, V.W.; Ivanova, A.; Deloria Knoll, M. Minimizing predictability while retaining balance through the use of less restrictive randomization procedures. Stat. Med. 2003, 22, 3017–3028. [Google Scholar] [CrossRef]
- Zhao, W.; Weng, Y. Block urn design—A new randomization algorithm for sequential trials with two or more treatments and balanced or unbalanced allocation. Contemp. Clin. Trials 2011, 32, 953–961. [Google Scholar] [CrossRef]
- Kuznetsova, O.M.; Tymofyeyev, Y. Brick tunnel randomization for unequal allocation to two or more treatment groups. Stat. Med. 2011, 30, 812–824. [Google Scholar] [CrossRef]
- Sharma, M.R.; Karrison, T.G.; Jin, Y.; Bies, R.R.; Maitland, M.L.; Stadler, W.M.; Ratain, M.J. Resampling phase III data to assess phase II trial designs and endpoints. Clin. Cancer Res. 2012, 18, 2309–2315. [Google Scholar] [CrossRef] [PubMed]
- Wason, J.M.S.; Trippa, L. A comparison of Bayesian adaptive randomization and multi-stage designs for multi-arm clinical trials. Stat. Med. 2014, 33, 2206–2221. [Google Scholar] [CrossRef]
- Pond, G.R.; Abbasi, S. Quantitative evaluation of single-arm versus randomized phase II cancer clinical trials. Clin. Trials 2011, 8, 260–269. [Google Scholar] [CrossRef]
- Lambert, P.C.; Sutton, A.J.; Abrams, K.R.; Jones, D.R. A comparison of summary patient-level covariates in meta-regression with individual patient data meta-analysis. J. Clin. Epidemiol. 2002, 55, 86–94. [Google Scholar] [CrossRef]
- Tomblyn, M.R.; Rizzo, J.D. Are there circumstances in which phase 2 study results should be practice-changing? Hematol. Am. Soc. Hematol. Educ. Progr. 2007, 489–492. [Google Scholar] [CrossRef]
- Brims, F.J.H.; Meniawy, T.M.; Duffus, I.; de Fonseka, D.; Segal, A.; Creaney, J.; Maskell, N.; Lake, R.A.; de Klerk, N.; Nowak, A.K. A Novel Clinical Prediction Model for Prognosis in Malignant Pleural Mesothelioma Using Decision Tree Analysis. J. Thorac. Oncol. 2016, 11, 573–582. [Google Scholar] [CrossRef]
- Nowak, A.K.; Byrne, M.J.; Williamson, R.; Ryan, G.; Segal, A.; Fielding, D.; Mitchell, P.; Musk, A.W.; Robinson, B.W.S. A multicentre phase II study of cisplatin and gemcitabine for malignant mesothelioma. Br. J. Cancer 2002, 87, 491–496. [Google Scholar] [CrossRef]
- Van Haarst, J.M.W.; Baas, P.; Manegold, C.; Schouwink, J.H.; Burgers, J.A.; De Bruin, H.G.; Mooi, W.J.; Van Klaveren, R.J.; De Jonge, M.J.A.; Van Meerbeeck, J.P. Multicentre phase II study of gemcitabine and cisplatin in malignant pleural mesothelioma. Br. J. Cancer 2002, 86, 342–345. [Google Scholar] [CrossRef][Green Version]
- Favaretto, A.G.; Aversa, S.M.L.; Paccagnella, A.; Manzini, V.D.P.; Palmisano, V.; Oniga, F.; Stefani, M.; Rea, F.; Bortolotti, L.; Loreggian, L.; et al. Gemcitabine combined with carboplatin in patients with malignant pleural mesothelioma: A multicentric phase II study. Cancer 2003, 97, 2791–2797. [Google Scholar] [CrossRef] [PubMed]
- Schuette, W.; Blankenburg, T.; Lauerwald, K.; Schreiber, J.; Bork, I.; Wollschlaeger, B.; Treutler, D.; Schneider, C.P.; Bonnet, R. A multicenter phase II study of gemcitabine and oxaliplatin for malignant pleural mesothelioma. Clin. Lung Cancer 2003, 4, 294–297. [Google Scholar] [CrossRef] [PubMed]
- Van Meerbeeck, J.P.; Gaafar, R.; Manegold, C.; Van Klaveren, R.J.; Van Marck, E.A.; Vincent, M.; Legrand, C.; Bottomley, A.; Debruyne, C.; Giaccone, G. Randomized phase III study of cisplatin with or without raltitrexed in patients with malignant pleural mesothelioma: An intergroup study of the European organisation for research and treatment of cancer lung cancer group and the National Cancer Institute. J. Clin. Oncol. 2005, 23, 6881–6889. [Google Scholar] [CrossRef]
- Castagneto, B.; Zai, S.; Dongiovanni, D.; Muzio, A.; Bretti, S.; Numico, G.; Botta, M. Cisplatin and gemcitabine in malignant pleural mesothelioma: A phase II study. Am. J. Clin. Oncol. Cancer Clin. Trials 2005, 28, 223–226. [Google Scholar] [CrossRef] [PubMed]
- Fennell, D.A.; Steele, J.P.C.; Shamash, J.; Sheaff, M.T.; Evans, M.T.; Goonewardene, T.I.; Nystrom, M.L.; Gower, N.H.; Rudd, R.M. Phase II trial of vinorelbine and oxaliplatin as first-line therapy in malignant pleural mesothelioma. Lung Cancer 2005, 47, 277–281. [Google Scholar] [CrossRef]
- Berghmans, T.; Lafitte, J.J.; Paesmans, M.; Stach, B.; Berchier, M.C.; Wackenier, P.; Lecomte, J.; Collon, T.; Mommen, P.; Sculier, J.P. A phase II study evaluating the cisplatin and epirubicin combination in patients with unresectable malignant pleural mesothelioma. Lung Cancer 2005, 50, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Kalmadi, S.R.; Rankin, C.; Kraut, M.J.; Jacobs, A.D.; Petrylak, D.P.; Adelstein, D.J.; Keohan, M.L.; Taub, R.N.; Borden, E.C. Gemcitabine and cisplatin in unresectable malignant mesothelioma of the pleura: A phase II study of the Southwest Oncology Group (SWOG 9810). Lung Cancer 2008, 60, 259–263. [Google Scholar] [CrossRef]
- Dowell, J.E.; Dunphy, F.R.; Taub, R.N.; Gerber, D.E.; Ngov, L.; Yan, J.; Xie, Y.; Kindler, H.L. A multicenter phase II study of cisplatin, pemetrexed, and bevacizumab in patients with advanced malignant mesothelioma. Lung Cancer 2012, 77, 567–571. [Google Scholar] [CrossRef] [PubMed]
- Kovac, V.; Zwitter, M.; Rajer, M.; Marin, A.; Debeljak, A.; Smrdel, U.; Vrankar, M. A phase II trial of low-dose gemcitabine in a prolonged infusion and cisplatin for malignant pleural mesothelioma. Anticancer Drugs 2012, 23, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Kindler, H.L.; Karrison, T.G.; Gandara, D.R.; Lu, C.; Krug, L.M.; Stevenson, J.P.; Jänne, P.A.; Quinn, D.I.; Koczywas, M.N.; Brahmer, J.R.; et al. Multicenter, double-blind, placebo-controlled, randomized phase II trial of gemcitabine/cisplatin plus bevacizumab or placebo in patients with malignant mesothelioma. J. Clin. Oncol. 2012, 30, 2509–2515. [Google Scholar] [CrossRef] [PubMed]
- Ceresoli, G.L.; Zucali, P.A.; Mencoboni, M.; Botta, M.; Grossi, F.; Cortinovis, D.; Zilembo, N.; Ripa, C.; Tiseo, M.; Favaretto, A.G.; et al. Phase II study of pemetrexed and carboplatin plus bevacizumab as first-line therapy in malignant pleural mesothelioma. Br. J. Cancer 2013, 109, 552–558. [Google Scholar] [CrossRef]
- O’Brien, M.E.R.; Gaafar, R.M.; Popat, S.; Grossi, F.; Price, A.; Talbot, D.C.; Cufer, T.; Ottensmeier, C.; Danson, S.; Pallis, A.; et al. Phase II study of first-line bortezomib and cisplatin in malignant pleural mesothelioma and prospective validation of progression free survival rate as a primary end-point for mesothelioma clinical trials (European Organisation for Research and Treatment. Eur. J. Cancer 2013, 49, 2815–2822. [Google Scholar] [CrossRef] [PubMed]
- Hassan, R.; Kindler, H.L.; Jahan, T.; Bazhenova, L.; Reck, M.; Thomas, A.; Pastan, I.; Parno, J.; O’Shannessy, D.J.; Fatato, P.; et al. Phase II clinical trial of amatuximab, a chimeric antimesothelin antibody with pemetrexed and cisplatin in advanced unresectable pleural mesothelioma. Clin. Cancer Res. 2014, 20, 5927–5936. [Google Scholar] [CrossRef] [PubMed]




| Author | Year | Acronymous | Duration | Type of Study | Treatment | Primary End Point | Secondary Endpoint | N | Median Age | Sex [No.(%)] | ECOG Performance Status [No.(%)] | Tumour Stage | Tumour Pathology | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | 0 | 1 | 2 | Loco-Regional (Stage I–III) | Metastatic(Stage IV) | Epithelioid | Biphasic | Sarcomatoid | ||||||||||
| Vogelzang et al. [6] | 2003 | NA | 1999–2001 | III | Cisplatin + Pemetrexed | OS | PFS, RR, duration of response | 226 | 61 | 184 (81%) | 42 (19%) | NA | NA | NA | 73 (32%) | 102 (45%) | 154 (68%) | 37 (16%) | 18 (8%) |
| Ceresoli et al. [7] | 2006 | NA | 2002–2005 | II | Carboplatin + Pemetrexed | ORR | toxicity, TTP, and OS | 102 | 65 | 76 (75%) | 26 (25%) | 33 (32%) | 61 (60%) | 8 (8%) | 34 (33%) | 49 (48%) | 80 (78%) | 8 (8%) | 7 (7%) |
| Castagneto et al. [14] | 2008 | NA | 2003–2005 | II | Carboplatin + Pemetrexed | RR | OS, TTP, Toxicity | 76 | 65 | 54 (71%) | 22 (29%) | NA | NA | NA | 27 (36%) | 36 (48%) | 57 (75%) | 13 (17%) | 3 (4%) |
| Katirtzoglou et al. [15] | 2010 | NA | 2004–2007 | II | Carboplatin + Pemetrexed | RR | OS, TTP | 62 | 66 | 53 (86%) | 9 (14%) | 25 (40%) | 37 (60%) | 0 | 23 (37%) | 17 (27%) | 47 (76%) | NA | 15 (24%) |
| Krug et al. [16] | 2014 | NA | NA | II | Cisplatin + Pemetrexed | PFS | OS, DCR, and safety/toxicity | 23 | 66 | 20 (87%) | 3 (13%) | 7 (30%) | 16 (70%) | 0 | NA | NA | 16 (70%) | 2 (9%) | 11 (18%) |
| Buikhuisen et al. [17] | 2016 | NA | 2009–2012 | II | Cisplatin + Pemetrexed | RR | OS, PFS | 11 | 59 | 10 (89%) | 1 (11%) | NA | NA | NA | NA | NA | 10 (89%) | 1 (11%) | 0 |
| Zalcman et al. [13] | 2016 | MAPS | NA | III | Cisplatin + Pemetrexed | OS | PFS, QoL and safety | 225 | 66 | 170 (76%) | 55 (25%) | NA | NA | NA | NA | NA | 182 (81%) | NA | NA |
| Tsao et al. [18] | 2019 | SWOG S0905 | 2011–2016 | II | Cisplatin + Pemetrexed | PFS | OS, DCR, and safety/toxicity | 47 | 72 | 40 (85%) | 7 (15%) | NA | NA | NA | NA | NA | 35 (74%) | 12 (26%) | NA |
| Scagliotti et al. [19] | 2019 | LUME-Meso | 2016–2018 | III | Cisplatin + Pemetrexed | PFS | OS, ORR, DCR, QoL | 229 | 66 | 169 (74%) | 60 (26%) | 98 (43%) | 131 (57%) | NA | 90 (39%) | 105 (46%) | 223 (97%) | 6 (3%) | NA |
| Baas et al. [4] | 2021 | CheckMate 743 | 2016–2018 | III | Cisplatin/Carboplatin + Pemetrexed | OS | PFS, ORR, DCR | 302 | 69 | 233 (77%) | 69 (23%) | 124 (42%) | 173 (57%) | NA | 106 (35%) | 149 (49%) | 227 (75%) | 39 (13%) | 36 (12%) |
| Author | Year | N | OS (Months) | 1 Yr. Survival Rates | 2 Yr. Survival Rates | PFS (Months) | Objective Response Rate (ORR) | Radiological Response Rate [N (%)] | Toxicity Summary (Grade 3 and 4) N (%) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Complete Response | Partial Response | Stable Disease | Progressive Disease | Disease Control Rate (%) | Blood and Lymphatic System Disorders | Cardiac Disorders | Gastrointestinal Disorders | Fatigue | Infections | Respiratory Disorders | Skin Disorders | Nausea and Vomiting | ||||||||||
| Anemia | Neutropenia | Thrombocytopenia | ||||||||||||||||||||
| Vogelzang et al. [6] | 2003 | 226 | 12.1 | 6 | NA | 5.7 | 41.3 | NA | NA | NA | NA | NA | 11 (5%) | NA | NA | NA | NA | NA | 11 (5%) | NA | 3 (1%) | 33 (15%) |
| Ceresoli et al. [7] | 2006 | 102 | 12.7 | 6.5 | NA | 6.5 | 19 | 2 (2%) | 17 (17%) | 48 (47%) | 33 (33%) | 67 | 12 (12%) | 20 (20%) | 8 (8%) | NA | 3 (3%) | 1 (1%) | NA | NA | NA | 1 (1%) |
| Castagneto et al. [14] | 2008 | 76 | 14 | NA | NA | 6 | 25 | 3 (4%) | 16 (21%) | 29 (38%) | 28 (37%) | 63 | 6 (8%) | 25 (33%) | 10 (13%) | NA | 9 (12%) | NA | 4 (5%) | NA | NA | NA |
| Katirtzoglou et al. [15] | 2010 | 62 | 14 | NA | NA | 7 | 29 | 0 | 18 (29%) | 34 (56%) | 10 (16%) | 85 | 6 (10%) | 15 (24%) | 5 (8%) | NA | 2 (3%) | 8 (13%) | 1 (1%) | NA | 3 (5%) | 9 (15%) |
| Krug et al. [16] | 2014 | 23 | 12.8 | NA | NA | 3.4 | 10 | 0 | 2 (10%) | 10 (50%) | 8 (40%) | 60 | 1 (4%) | 1 (4%) | NA | 1 (4%) | 1 (4%) | 3 (13%) | NA | NA | NA | 2 (9%) |
| Buikhuisen et al. [17] | 2016 | 11 | 18.5 | NA | NA | 8.3 | 18 | NA | 2 (18%) | 8 (73%) | NA | 91 | 0 | 1 (5%) | 0 | 0 | 0 | 0 | NA | 0 | NA | 0 |
| Zalcman et al. [13] | 2016 | 225 | 16.1 | NA | NA | 7.3 | NA | NA | NA | NA | NA | NA | 30 (13%) | 100 (44%) | 21 (9%) | 2 (1%) | 3 (1%) | 28 (13%) | 7 (3%) | NA | NA | 18 (8%) |
| Tsao et al. [18] | 2019 | 47 | 8.5 | NA | NA | 5.6 | 20 | NA | NA | NA | NA | NA | 7 (15%) | 9 (20%) | 2 (4%) | 0 | 0 | 6 (13%) | NAA | NA | NA | 0 |
| Scagliotti et al. [19] | 2019 | 229 | 16.1 | NA | NA | 7 | 43 | NA | 98 (43%) | NA | NA | 93 | 33 (14%) | 54 (24%) | NA | NA | 10 (4%) | 17 (7%) | 14 (6%) | NA | 1 (1%) | 15 (7%) |
| Baas et al. [4] | 2021 | 302 | 14.1 | 8.1 | 3.8 | 7.2 | 43 | 0 | 129 (43%) | 125 (41%) | 14 (5%) | 85 | 32 (11%) | 43 (15%) | 10 (3%) | NA | 3 (2%) | 5 (2%) | NA | NA | 0 | 13 (4%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kotecha, R.; Tonse, R.; Rubens, M.; Appel, H.; Albrecht, F.; Kaywin, P.; Alley, E.W.; Tom, M.C.; Mehta, M.P. Meta-Analysis of Survival and Development of a Prognostic Nomogram for Malignant Pleural Mesothelioma Treated with Systemic Chemotherapy. Cancers 2021, 13, 2186. https://doi.org/10.3390/cancers13092186
Kotecha R, Tonse R, Rubens M, Appel H, Albrecht F, Kaywin P, Alley EW, Tom MC, Mehta MP. Meta-Analysis of Survival and Development of a Prognostic Nomogram for Malignant Pleural Mesothelioma Treated with Systemic Chemotherapy. Cancers. 2021; 13(9):2186. https://doi.org/10.3390/cancers13092186
Chicago/Turabian StyleKotecha, Rupesh, Raees Tonse, Muni Rubens, Haley Appel, Federico Albrecht, Paul Kaywin, Evan W. Alley, Martin C. Tom, and Minesh P. Mehta. 2021. "Meta-Analysis of Survival and Development of a Prognostic Nomogram for Malignant Pleural Mesothelioma Treated with Systemic Chemotherapy" Cancers 13, no. 9: 2186. https://doi.org/10.3390/cancers13092186
APA StyleKotecha, R., Tonse, R., Rubens, M., Appel, H., Albrecht, F., Kaywin, P., Alley, E. W., Tom, M. C., & Mehta, M. P. (2021). Meta-Analysis of Survival and Development of a Prognostic Nomogram for Malignant Pleural Mesothelioma Treated with Systemic Chemotherapy. Cancers, 13(9), 2186. https://doi.org/10.3390/cancers13092186