
Implementation of Double Immune Checkpoint Blockade Increases Response Rate to Induction Chemotherapy in Head and Neck Cancer

 , , ,
, , ,  , ,
, ,  ,
,  ,
,  ,
,  ,
,  add
Show full author list
add
Show full author list
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Treatments
2.2. Clinical and Pathologic Response Assessment
2.3. Trial Oversight
2.4. Statistical Analysis
3. Results
3.1. Patients
3.2. Correlation of CR Rate with Patient, Tumor, and Treatment Characteristics in the Overall Sample
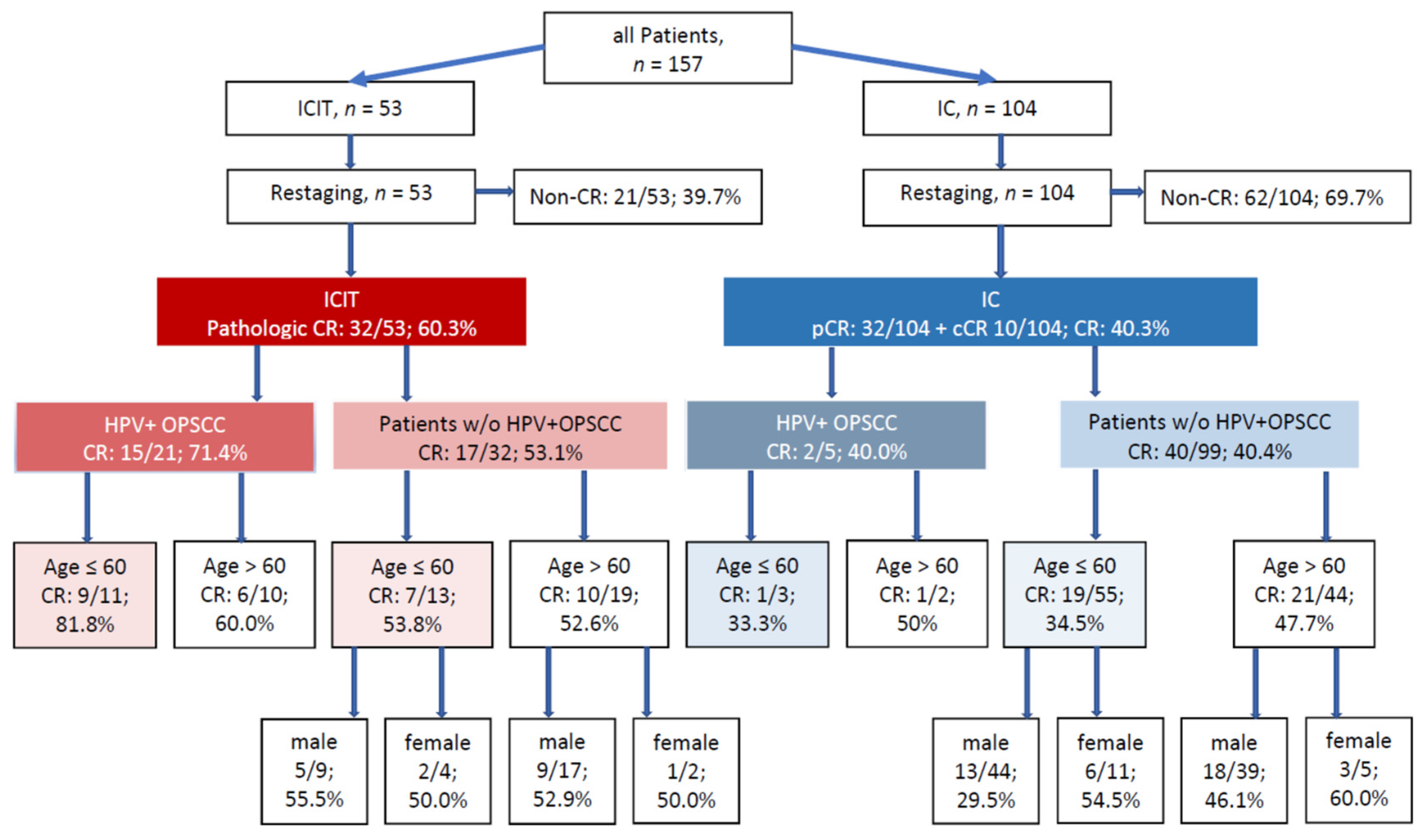
3.3. Response to ICIT vs. IC
3.4. IC vs. ICIT: CR Rates by Individual Patient, Tumor, and Treatment Characteristics
3.5. CR Rates for IC vs. ICIT in Patient Subgroups with Identical Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Forastiere, A.A.; Goepfert, H.; Maor, M.; Pajak, T.F.; Weber, R.; Morrison, W.; Glisson, B.; Trotti, A.; Ridge, J.A.; Chao, C.; et al. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N. Engl. J. Med. 2003, 349, 2091–2098. [Google Scholar] [CrossRef]
- Lefebvre, J.L.; Andry, G.; Chevalier, D.; Luboinski, B.; Collette, L.; Traissac, L.; de Raucourt, D.; Langendijk, J.A.; EORTC Head and Neck Cancer Group. Laryngeal preservation with induction chemotherapy for hypopharyngeal squamous cell carcinoma: 10-year results of EORTC trial 24891. Ann. Oncol. 2012, 23, 2708–2714. [Google Scholar] [CrossRef] [PubMed]
- Geoffrois, L.; Martin, L.; De Raucourt, D.; Sun, X.S.; Tao, Y.; Maingon, P.; Buffet, J.; Pointreau, Y.; Sire, C.; Tuchais, C.; et al. Induction Chemotherapy Followed by Cetuximab Radiotherapy Is not Superior to Concurrent Chemoradiotherapy for Head and Neck Carcinomas: Results of the GORTEC 2007-02 Phase III Randomized Trial. J. Clin. Oncol. 2018, 36, 3077–3083. [Google Scholar] [CrossRef]
- Haddad, R.; O’Neill, A.; Rabinowits, G.; Tishler, R.; Khuri, F.; Adkins, D.; Clark, J.; Sarlis, N.; Lorch, J.; Beitler, J.J.; et al. Induction chemotherapy followed by concurrent chemoradiotherapy (sequential chemoradiotherapy) versus concurrent chemoradiotherapy alone in locally advanced head and neck cancer (PARADIGM): A randomised phase 3 trial. Lancet Oncol. 2013, 14, 257–264. [Google Scholar] [CrossRef]
- Semrau, S.; Waldfahrer, F.; Lell, M.; Linke, R.; Klautke, G.; Kuwert, T.; Uder, M.; Iro, H.; Fietkau, R. Feasibility, toxicity, and efficacy of short induction chemotherapy of docetaxel plus cisplatin or carboplatin (TP) followed by concurrent chemoradio-therapy for organ preservation in advanced cancer of the hypopharynx, larynx, and base of tongue. Early results. Strahlenther. Onkol. 2011, 187, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Breheret, M.; Lubgan, D.; Haderlein, M.; Hecht, M.; Traxdorf, M.; Schmidt, D.; Müller, S.; Kitzsteiner, C.; Kuwert, T.; Iro, H.; et al. Single-cycle induction chemotherapy before chemoradiotherapy or surgery in functionally inoperable head and neck squamous cell carcinoma: 10-year results. Eur. Arch. Otorhinolaryngol. 2020, 277, 245–254. [Google Scholar] [CrossRef]
- Urba, S.; Wolf, G.; Eisbruch, A.; Worden, F.; Lee, J.; Bradford, C.; Teknos, T.; Chepeha, D.; Prince, M.; Hogikyan, N.; et al. Single-cycle induction chemotherapy selects patients with advanced laryngeal cancer for combined chemoradiation: A new treatment paradigm. J. Clin. Oncol. 2006, 24, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Haderlein, M.; Semrau, S.; Ott, O.; Speer, S.; Bohr, C.; Fietkau, R. Dose-dependent deterioration of swallowing function after induction chemotherapy and definitive chemoradiotherapy for laryngopharyngeal cancer. Strahlenther. Onkol. 2014, 190, 192–198. [Google Scholar] [CrossRef]
- Mogadas, S.; Busch, C.J.; Pflug, C.; Hanken, H.; Krüll, A.; Petersen, C.; Tribius, S. Influence of radiation dose to pharyngeal constrictor muscles on late dysphagia and quality of life in patients with locally advanced oropharyngeal carcinoma. Strahlenther. Onkol. 2020, 196, 522–529. [Google Scholar] [CrossRef]
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Rutkowski, P.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Wagstaff, J.; Schadendorf, D.; Ferrucci, P.F.; et al. Overall Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2017, 377, 1345–1356. [Google Scholar] [CrossRef]
- Rotte, A. Combination of CTLA-4 and PD-1 blockers for treatment of cancer. J. Exp. Clin. Cancer Res. 2019, 38, 55. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.C.; Levine, J.H.; Cogdill, A.P.; Zhao, Y.; Anang, N.A.S.; Andrews, M.C.; Sharma, P.; Wang, J.; Wargo, J.A.; Pe’er, D.; et al. Distinct Cellular Mechanisms Underlie Anti-CTLA-4 and Anti-PD-1 Checkpoint Blockade. Cell 2017, 170, 1120–1133.e17. [Google Scholar] [CrossRef] [PubMed]
- Hecht, M.; Gostian, A.O.; Eckstein, M.; Rutzner, S.; von der Grün, J.; Illmer, T.; Hautmann, M.G.; Klautke, G.; Laban, S.; Brunner, T.; et al. Safety and efficacy of single cycle induction treatment with cisplatin/docetaxel/ durvalumab/tremelimumab in locally advanced HNSCC: First results of CheckRad-CD8. J. Immunother. Cancer 2020, 8, e001378. [Google Scholar] [CrossRef] [PubMed]
- Ferris, R.L.; Blumenschein, G., Jr.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab for Recurrent Squamous-Cell Carcinoma of the Head and Neck. N. Engl. J. Med. 2016, 375, 1856–1867. [Google Scholar] [CrossRef]
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulières, D.; Tahara, M.; de Castro, G., Jr.; Psyrri, A.; Basté, N.; Neupane, P.; Bratland, Å.; et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): A randomised, open-label, phase 3 study. Lancet 2019, 394, 1915–1928. [Google Scholar] [CrossRef]
- Hitt, R.; López-Pousa, A.; Martínez-Trufero, J.; Escrig, V.; Carles, J.; Rizo, A.; Isla, D.; Vega, M.E.; Martí, J.L.; Lobo, F.; et al. Phase III study comparing cisplatin plus fluorouracil to paclitaxel, cisplatin, and fluorouracil induction chemotherapy followed by chemoradiotherapy in locally advanced head and neck cancer. J. Clin. Oncol. 2005, 23, 8636–8845. [Google Scholar] [CrossRef]
- Pointreau, Y.; Garaud, P.; Chapet, S.; Sire, C.; Tuchais, C.; Tortochaux, J.; Faivre, S.; Guerrif, S.; Alfonsi, M.; Calais, G. Randomized trial of induction chemotherapy with cisplatin and 5-fluorouracil with or without docetaxel for larynx preservation. J. Natl. Cancer Inst. 2009, 101, 498–506. [Google Scholar] [CrossRef]
- Inhestern, J.; Schmalenberg, H.; Dietz, A.; Rotter, N.; Maschmeyer, G.; Jungehülsing, M.; Grosse-Thie, C.; Kuhnt, T.; Görner, M.; Sudhoff, H.; et al. A two-arm multicenter phase II trial of one cycle chemoselection split-dose docetaxel, cisplatin and 5-fluorouracil (TPF) induction chemotherapy before two cycles of split TPF followed by curative surgery combined with postoperative radiotherapy in patients with locally advanced oral and oropharyngeal squamous cell cancer (TISOC-1). Ann. Oncol. 2017, 28, 1917–1922. [Google Scholar] [CrossRef]
- Ghi, M.G.; Paccagnella, A.; Ferrari, D.; Foa, P.; Alterio, D.; Codecà, C.; Nolè, F.; Verri, E.; Orecchia, R.; Morelli, F.; et al. Induction TPF followed by concomitant treatment versus concomitant treatment alone in locally advanced head and neck cancer. A phase II-III trial. Ann. Oncol. 2017, 28, 2206–2212. [Google Scholar] [CrossRef]
- Posner, M.R.; Hershock, D.M.; Blajman, C.R.; Mickiewicz, E.; Winquist, E.; Gorbounova, V.; Tjulandin, S.; Shin, D.M.; Cullen, K.; Ervin, T.J.; et al. Cisplatin and fluorouracil alone or with docetaxel in head and neck cancer. N. Engl. J. Med. 2007, 357, 1705–1715. [Google Scholar] [CrossRef]
- Vermorken, J.B.; Remenar, E.; van Herpen, C.; Gorlia, T.; Mesia, R.; Degardin, M.; Stewart, J.S.; Jelic, S.; Betka, J.; Preiss, J.H.; et al. Cisplatin, fluorouracil, and docetaxel in unresectable head and neck cancer. N. Engl. J. Med. 2007, 357, 1695–1704. [Google Scholar] [CrossRef]
- Ferris, R.L.; Haddad, R.; Even, C.; Tahara, M.; Dvorkin, M.; Ciuleanu, T.E.; Clement, P.M.; Mesia, R.; Kutukova, S.; Zholudeva, L.; et al. Durvalumab with or without tremelimumab in patients with recurrent or metastatic head and neck squamous cell carcinoma: EAGLE, a randomized, open-label phase III study. Ann. Oncol. 2020, 31, 942–950. [Google Scholar] [CrossRef] [PubMed]
- Siu, L.L.; Even, C.; Mesía, R.; Remenar, E.; Daste, A.; Delord, J.P.; Krauss, J.; Saba, N.F.; Nabell, L.; Ready, N.E.; et al. Safety and Efficacy of Durvalumab With or Without Tremelimumab in Patients With PD-L1-Low/Negative Recurrent or Metastatic HNSCC: The Phase 2 CONDOR Randomized Clinical Trial. JAMA Oncol. 2019, 5, 195–203. [Google Scholar] [CrossRef]
- Zuur, C.L.; Elbers, J.B.W.; Vos, J.L.; van der Leun, A.; Qiao, X.; Karakullukcu, B.; van den Brekel, M.W.M.; Tan, B.; Jasperse, B.; Vogel, W.V.; et al. Feasibility and toxicity of neoadjuvant nivolumab with or without ipilimumab prior to extensive (salvage) surgery in patients with advanced head and neck cancer (the IMCISION trial, NCT03003637). J. Clin. Oncol. 2019, 37 (Suppl. 2575). [Google Scholar] [CrossRef]
- Wise-Draper, T.M.; Old, M.O.; Worden, F.P.; O’Brien, P.E.; Cohen, E.E.W.; Dunlap, N.; Mierzwa, M.L.; Casper, K.; Palackdharry, S.; Hinrichs, B.; et al. Phase II multi-site investigation of neoadjuvant pembrolizumab and adjuvant concurrent radiation and pembrolizumab with or without cisplatin in resected head and neck squamous cell carcinoma. J. Clin. Oncol. 2018, 36 (Suppl. 6017). [Google Scholar] [CrossRef]
- Ferrarotto, R.; Bell, D.; Rubin, M.L.; Hutcheson, K.A.; Johnson, J.M.; Goepfert, R.P.; Phan, J.; Elamin, Y.Y.; Torman, D.K.; Warneke, C.L.; et al. Impact of Neoadjuvant Durvalumab with or without Tremelimumab on CD8+ Tumor Lymphocyte Density, Safety, and Efficacy in Patients with Oropharynx Cancer: CIAO Trial Results. Clin. Cancer Res. 2020, 26, 3211–3219. [Google Scholar] [CrossRef]
- Guigay, J.; Fayette, J.; Mesia, R.; Lafond, C.; Saada-Bouzid, E.; Geoffrois, L.; Martin, L.; Cupissol, D.; Capitain, O.; Castanie, H.; et al. TPEx versus Extreme regimen in 1st line recurrent/metastatic head and neck squamous cell carcinoma (R/M HNSCC). J. Clin. Oncol. 2019, 37, 6002. [Google Scholar] [CrossRef]
- Ferris, R.L.; Blumenschein, G., Jr.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.J.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab vs investigator’s choice in recurrent or metastatic squamous cell carcinoma of the head and neck: 2-year long-term survival update of CheckMate 141 with analyses by tumor PD-L1 expression. Oral Oncol. 2018, 81, 45–51. [Google Scholar] [CrossRef]
- Zandberg, D.P.; Algazi, A.P.; Jimeno, A.; Good, J.S.; Fayette, J.; Bouganim, N.; Ready, N.E.; Clement, P.M.; Even, C.; Jang, R.W.; et al. Durvalumab for recurrent or metastatic head and neck squamous cell carcinoma: Results from a single-arm, phase II study in patients with ≥25% tumour cell PD-L1 expression who have progressed on platinum-based chemotherapy. Eur. J. Cancer 2019, 107, 142–152. [Google Scholar] [CrossRef]
- Worden, F.P.; Kumar, B.; Lee, J.S.; Wolf, G.T.; Cordell, K.G.; Taylor, J.M.; Urba, S.G.; Eisbruch, A.; Teknos, T.N.; Chepeha, D.B.; et al. Chemoselection as a strategy for organ preservation in advanced oropharynx cancer: Response and survival positively associated with HPV16 copy number. J. Clin. Oncol. 2008, 26, 3138–3146. [Google Scholar] [CrossRef]
- Marur, S.; Li, S.; Cmelak, A.J.; Gillison, M.L.; Zhao, W.J.; Ferris, R.L.; Westra, W.H.; Gilbert, J.; Bauman, J.E.; Wagner, L.I.; et al. E1308: Phase II Trial of Induction Chemotherapy Followed by Reduced-Dose Radiation and Weekly Cetuximab in Patients With HPV-Associated Resectable Squamous Cell Carcinoma of the Oropharynx—ECOG-ACRIN Cancer Research Group. J. Clin. Oncol. 2017, 35, 490–497. [Google Scholar] [CrossRef]
- Wondergem, N.E.; Nauta, I.H.; Muijlwijk, T.; Leemans, C.R.; van de Ven, R. The Immune Microenvironment in Head and Neck Squamous Cell Carcinoma: On Subsets and Subsites. Curr. Oncol. Rep. 2020, 22, 81. [Google Scholar] [CrossRef] [PubMed]
- Chakravarthy, A.; Henderson, S.; Thirdborough, S.M.; Ottensmeier, C.H.; Su, X.; Lechner, M.; Feber, A.; Thomas, G.J.; Fenton, T.R. Human Papillomavirus Drives Tumor Development Throughout the Head and Neck: Improved Prognosis Is Associated With an Immune Response Largely Restricted to the Oropharynx. J. Clin. Oncol. 2016, 34, 4132–4141. [Google Scholar] [CrossRef] [PubMed]
- Donaubauer, A.J.; Becker, I.; Rühle, P.F.; Fietkau, R.; Gaipl, U.S.; Frey, B. Analysis of the immune status from peripheral whole blood with a single-tube multicolor flow cytometry assay. Methods Enzymol. 2020, 632, 389–415. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameter | IC | ICIT | p-Value | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Number | 104 | 53 | |||
| Gender | |||||
| Male | 84 | 80.8 | 45 | 84.9 | p = 0.522 |
| Female | 20 | 19.2 | 8 | 15.1 | |
| Median age (range) | 58 (35–78) | 61(38–78) | p = 0.27 ** | ||
| T stage | p = 0.00001 | ||||
| 1 | 1 | 0.9 | 2 | 3.8 | |
| 2 | 35 | 33.7 | 7 | 13.2 | |
| 3 | 42 | 40.4 | 10 | 18.9 | |
| 4 | 26 | 25.0 | 34 | 64.2 | |
| N stage | p = 0.803 | ||||
| 0 | 32 | 30.7 | 14 | 26.4 | |
| 1 | 17 | 16.3 | 10 | 18.9 | |
| 2a | 1 | 1.0 | 2 | 3.8 | |
| 2b | 26 | 25.0 | 13 | 24.5 | |
| 2c | 27 | 26.0 | 14 | 26.4 | |
| 3 | 1 | 1.0 | 0 | 0 | |
| UICC stage (7th Edition) | p = 0.045 | ||||
| 2 | 12 | 11.5 | 0 | 0 | |
| 3 | 23 | 22.1 | 10 | 18.9 | |
| 4 | 69 | 66.4 | 43 | 81.1 | |
| Grading | p = 0.016 | ||||
| 1 | 4 | 3.8 | 0 | 0 | |
| 2 | 49 | 47.2 | 8 | 15.1 | |
| 3 | 46 | 44.2 | 24 | 45.3 | |
| HPV-associated OPSCC | p = 0.000 * | ||||
| No | 99 | 95.2 | 32 | 60.4 | |
| Yes | 5 | 4.8 | 21 | 39.6 | |
| Tumor location | p = 0.000 | ||||
| Oral cavity/oropharynx | 18 | 17.3 | 33 | 62.3 | |
| Hypopharynx | 42 | 40.4 | 11 | 20.8 | |
| Larynx | 44 | 42.3 | 9 | 17.0 | |
| Prognostic Factor | Univariable | Multivariable | ||||||
|---|---|---|---|---|---|---|---|---|
| n | CR | % | p-Value | OR | CI | p-Value | ||
| Gender | Male | 129 | 61 | 47 | 0.93 | |||
| Female | 28 | 13 | 46 | |||||
| Age | <60 years | 82 | 36 | 44 | 0.39 | |||
| ≥60 years | 75 | 38 | 51 | |||||
| T stage | 1/2 | 45 | 26 | 58 | 0.09 | 1.48 | 1.02 | 2.150.037 |
| 3/4 | 48 | 112 | 43 | |||||
| UICC stage | II/III | 45 | 23 | 51 | 0.52 | |||
| IV | 112 | 51 | 46 | |||||
| Grading | 1 | 4 | 2 | 50 | 0.23 | |||
| 2 | 57 | 20 | 35 | |||||
| 3 | 70 | 35 | 50 | |||||
| HPV-associated OPSCC | yes | 26 | 17 | 65 | 0.041 | 0.368 | ||
| no | 131 | 57 | 43 | |||||
| Tumor location | OCOP | 51 | 26 | 51 | 0.741 | |||
| HP | 53 | 23 | 43 | |||||
| L | 53 | 25 | 47 | |||||
| Therapy | ICIT | 53 | 32 | 60 | 0.018 | 2.28 | 1.04–4.98 | 0.038 |
| IC | 104 | 42 | 40 | |||||
| Parameter | Complete Response Rate | p-Value | |
|---|---|---|---|
| ICIT | IC | ||
| HPV-associated OPSCC | |||
| Yes | 71.4% (15/21) | 40.0% (2/5) | 0.145 * |
| No | 53.1% (17/32) | 40.9% (40/99) | 0.208 * |
| Tumor location | |||
| - Oral cavity, oropharynx | 50.0% (6/12) | 23.1% (3/13) | 0.163 * |
| - Hypopharynx | 63.6% (7/11) | 38.1% (16/42) | 0.119 * |
| - Larynx | 44.4% (4/9) | 47.7% (21/44) | 0.575 * |
| Gender | |||
| Male | 62.2% (28/45) | 39.2% (33/84) | 0.013 |
| Female | 50.0% (4/8) | 45.0% (9/20) | 0.569 * |
| Age | |||
| ≤60 years | 66.6% (16/24) | 34.4% (20/58) | 0.008 |
| >60 years | 55.1% (16/29) | 47.8% (22/46) | 0.351 |
| T stage | |||
| T1/2 | 77.7% (7/9) | 52.7% (19/36) | 0.164 * |
| T3/4 | 56.8% (25/44) | 33.8% (23/68) | 0.016 |
| N stage | |||
| N0–N2a | 65.4% (17/26) | 50.0% (25/50) | 0.201 |
| N2b/N3 | 55.5% (15/27) | 31.5% (17/54) | 0.037 |
| UICC stage | |||
| UICC Stage 2/3 | 70.0% (7/10) | 45.7% (16/35) | 0.160 * |
| UICC Stage 4 | 58.1% (25/43) | 37.6% (26/69) | 0.034 |
| Grade | |||
| G1 | 50.0% (2/4) | ||
| G2 | 62.5% (5/8) | 30.6% (15/49) | 0.090 |
| G3 | 50.0% (12/24) | 50.0% (23/46) | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Semrau, S.; Gostian, A.-O.; Traxdorf, M.; Eckstein, M.; Rutzner, S.; von der Grün, J.; Illmer, T.; Hautmann, M.; Klautke, G.; Laban, S.; et al. Implementation of Double Immune Checkpoint Blockade Increases Response Rate to Induction Chemotherapy in Head and Neck Cancer. Cancers 2021, 13, 1959. https://doi.org/10.3390/cancers13081959
Semrau S, Gostian A-O, Traxdorf M, Eckstein M, Rutzner S, von der Grün J, Illmer T, Hautmann M, Klautke G, Laban S, et al. Implementation of Double Immune Checkpoint Blockade Increases Response Rate to Induction Chemotherapy in Head and Neck Cancer. Cancers. 2021; 13(8):1959. https://doi.org/10.3390/cancers13081959
Chicago/Turabian StyleSemrau, Sabine, Antoniu-Oreste Gostian, Maximilian Traxdorf, Markus Eckstein, Sandra Rutzner, Jens von der Grün, Thomas Illmer, Matthias Hautmann, Gunther Klautke, Simon Laban, and et al. 2021. "Implementation of Double Immune Checkpoint Blockade Increases Response Rate to Induction Chemotherapy in Head and Neck Cancer" Cancers 13, no. 8: 1959. https://doi.org/10.3390/cancers13081959
APA StyleSemrau, S., Gostian, A.-O., Traxdorf, M., Eckstein, M., Rutzner, S., von der Grün, J., Illmer, T., Hautmann, M., Klautke, G., Laban, S., Brunner, T., Tamaskovics, B., Frey, B., Zhou, J.-G., Geppert, C.-I., Hartmann, A., Balermpas, P., Budach, W., Gaipl, U., ... Hecht, M. (2021). Implementation of Double Immune Checkpoint Blockade Increases Response Rate to Induction Chemotherapy in Head and Neck Cancer. Cancers, 13(8), 1959. https://doi.org/10.3390/cancers13081959