
Quality of Life with Vulvar Carcinoma Treated with Palliative Electrochemotherapy: The ELECHTRA (ELEctroCHemoTherapy vulvaR cAncer) Study

 ,
,  ,
, 
 ,
,  and
and 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Inclusion Criteria and Data Collection
2.2. Statistical Analysis
3. Results
3.1. Characteristics of Patients
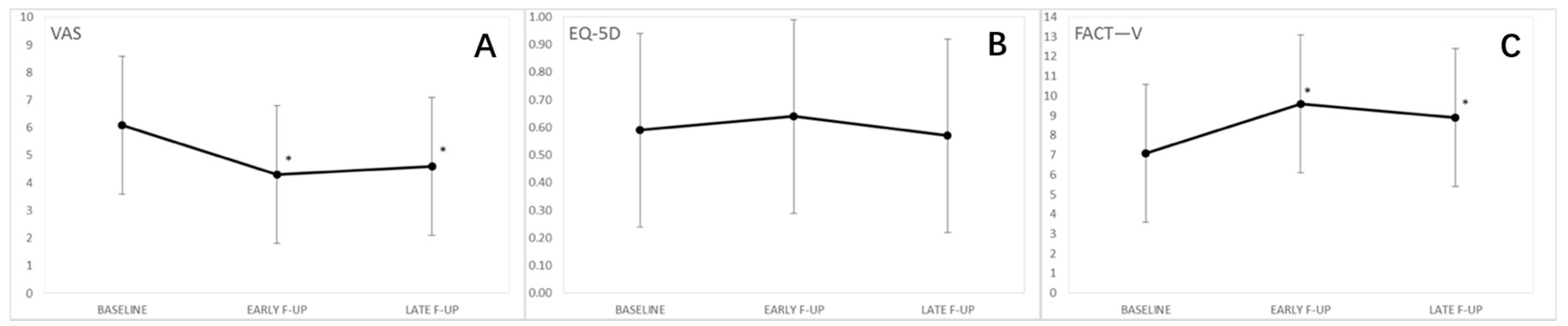
3.2. Quality of Life
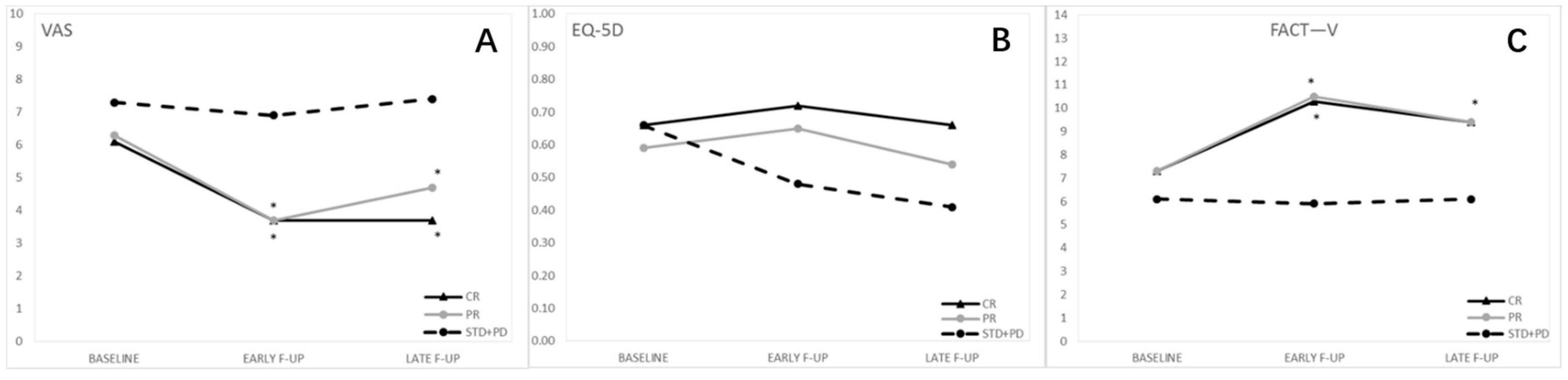
3.3. Subgroup Analyses, Response to Therapy
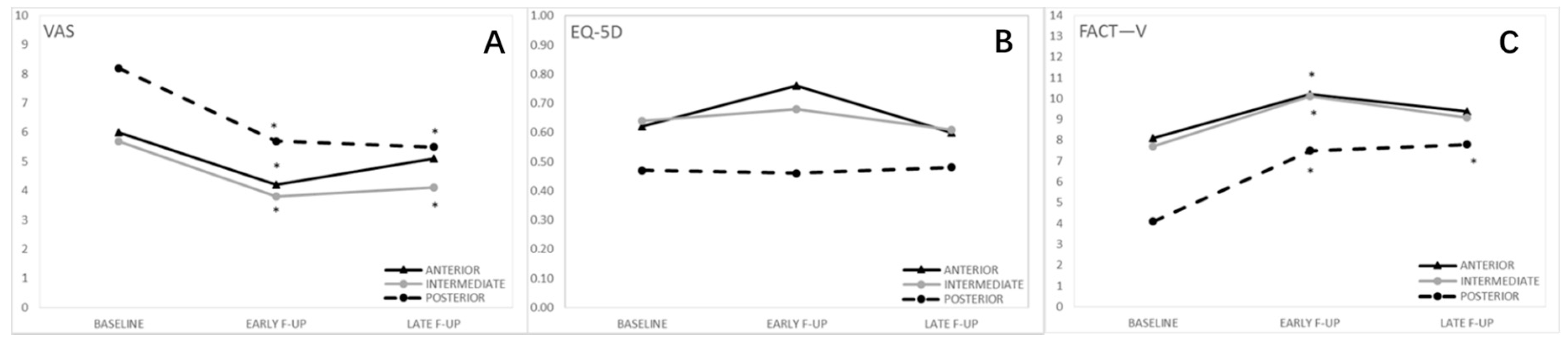
3.4. Subgroup Analyses, Anatomical Site of the Lesions
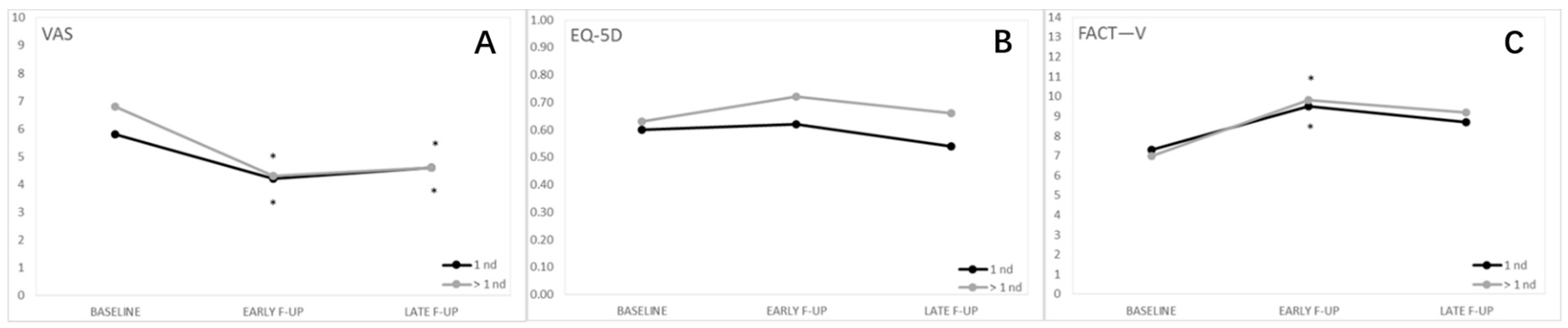
3.5. Subgroup Analyses, Number of Lesions
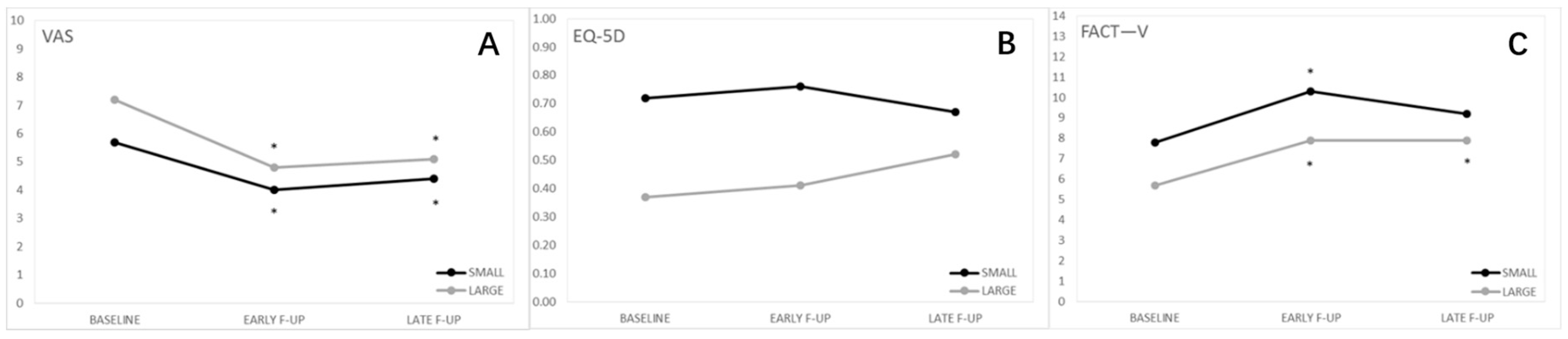
3.6. Subgroup Analyses, Size of Lesions
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tabbaa, Z.M.; Gonzalez, J.; Sznurkowski, J.J.; Weaver, A.L.; Mariani, A.; Cliby, W.A. Impact of the new FIGO 2009 staging classification for vulvar cancer on prognosis and stage distribution. Gynecol. Oncol. 2012, 127, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, D.; Gomez-Martinez, R.A. Vulvar Cancer. Obstet. Gynecol. Clin. N. Am. 2019, 46, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Zapardiel, I.; Iacoponi, S.; Coronado, P.J.; Zalewski, K.; Chen, F.; Fotopoulou, C.; Dursun, P.; Kotsopoulos, I.C.; Jach, R.; Buda, A.; et al. Prognostic factors in patients with vulvar cancer: The VULCAN study. Int. J. Gynecol. Cancer 2020, 30, 1285–1291. [Google Scholar] [CrossRef] [PubMed]
- Alkatout, I.; Schubert, M.; Garbrecht, N.; Weigel, M.T.; Jonat, W.; Mundhenke, C.; Günther, V. Vulvar cancer: Epidemiology, clinical presentation, and management options. Int. J. Womens Health 2015, 7, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Salom, E.M.; Penalver, M. Recurrent vulvar cancer. Curr. Treat. Options Oncol. 2002, 3, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Tranoulis, A.; Georgiou, D.; Founta, C.; Mehra, G.; Sayasneh, A.; Nath, R. Use of electrochemotherapy in women with vulvar cancer to improve quality-of-life in the palliative setting: A meta-analysis. Int. J. Gynecol. Cancer 2020, 30, 107–114. [Google Scholar] [CrossRef]
- Hami, L.T.; Lampe, B.; Mallmann, P.; Forner, D.M. The Impact of Age on the Prognosis of Vulvar Cancer. Oncol. Res. Treat. 2018, 41, 520–524. [Google Scholar] [CrossRef]
- Chan, Y.M.; Ngan, H.Y.S.; Li, B.Y.G.; Yip, A.M.W.; Ng, T.Y.; Lee, P.W.H.; Yip, P.S.F.; Wong, L.C. A longitudinal study on quality of life after gynecologic cancer treatment. Gynecol. Oncol. 2001, 83, 10–19. [Google Scholar] [CrossRef]
- Perrone, A.M.; Galuppi, A.; Cima, S.; Pozzati, F.; Arcelli, A.; Cortesi, A.; Procaccini, M.; Pellegrini, A.; Zamagni, C.; De Iaco, P. Electrochemotherapy can be used as palliative treatment in patients with repeated loco-regional recurrence of squamous vulvar cancer: A preliminary study. Gynecol. Oncol. 2013, 130, 550–553. [Google Scholar] [CrossRef] [PubMed]
- Corrado, G.; Cutillo, G.; Fragomeni, S.M.; Bruno, V.; Tagliaferri, L.; Mancini, E.; Certelli, C.; Paris, I.; Vizza, E.; Scambia, G.; et al. Palliative electrochemotherapy in primary or recurrent vulvar cancer. Int. J. Gynecol. Cancer 2020, 30, 927–931. [Google Scholar] [CrossRef]
- Mir, L.M.; Orlowski, S.; Belehradek, J.; Paoletti, C. Electrochemotherapy potentiation of antitumour effect of bleomycin by local electric pulses. Eur. J. Cancer Clin. Oncol. 1991, 27, 68–72. [Google Scholar] [CrossRef]
- Sersa, G.; Miklavcic, D.; Cemazar, M.; Rudolf, Z.; Pucihar, G.; Snoj, M. Electrochemotherapy in treatment of tumours. Eur. J. Surg. Oncol. 2008, 34, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Ferioli, M.; Perrone, A.M.; Buwenge, M.; Arcelli, A.; Zamagni, A.; Macchia, G.; Deodato, F.; Cilla, S.; Tagliaferri, L.; De Terlizzi, F.; et al. Electrochemotherapy of skin metastases from breast cancer: A systematic review. Clin. Exp. Metastasis 2020, 38, 1–10. [Google Scholar] [CrossRef]
- Campana, L.G.; Edhemovic, I.; Soden, D.; Perrone, A.M.; Scarpa, M.; Campanacci, L.; Cemazar, M.; Valpione, S.; Miklavčič, D.; Mocellin, S.; et al. Electrochemotherapy—Emerging applications technical advances, new indications, combined approaches, and multi-institutional collaboration. Eur. J. Surg. Oncol. 2019, 45, 92–102. [Google Scholar] [CrossRef]
- Perrone, A.M.; Galuppi, A.; Pirovano, C.; Borghese, G.; Covarelli, P.; De Terlizzi, F.; Ferioli, M.; Cara, S.; Morganti, A.G.; De Iaco, P. Palliative electrochemotherapy in vulvar carcinoma: Preliminary results of the ELECHTRA (electrochemotherapy vulvar cancer) multicenter study. Cancers 2019, 11, 657. [Google Scholar] [CrossRef]
- Perrone, A.M.; Ferioli, M.; Galuppi, A.; Coe, M.; de Terlizzi, F.; Tesei, M.; Dondi, G.; de Palma, A.; Morganti, A.G.; de Iaco, P. Palliative treatment with electrochemotherapy in recurrent or metastatic vaginal cancer. Int. J. Gynecol. Cancer 2020, 30, 939–946. [Google Scholar] [CrossRef]
- Perrone, A.M.; Cima, S.; Pozzati, F.; Frakulli, R.; Cammelli, S.; Tesei, M.; Gasparre, G.; Galuppi, A.; Morganti, A.G.; De Iaco, P. Palliative electro-chemotherapy in elderly patients with vulvar cancer: A phase II trial. J. Surg. Oncol. 2015, 112, 529–532. [Google Scholar] [CrossRef]
- Perrone, A.M.; Galuppi, A.; Borghese, G.; Corti, B.; Ferioli, M.; Della Gatta, A.N.; Bovicelli, A.; Morganti, A.G.; De Iaco, P. Electrochemotherapy pre-treatment in primary squamous vulvar cancer. Our preliminary experience. J. Surg. Oncol. 2018, 117, 1813–1817. [Google Scholar] [CrossRef]
- Marty, M.; Sersa, G.; Garbay, J.R.; Gehl, J.; Collins, C.G.; Snoj, M.; Billard, V.; Geertsen, P.F.; Larkin, J.O.; Miklavcic, D.; et al. Electrochemotherapy—An easy, highly effective and safe treatment of cutaneous and subcutaneous metastases: Results of ESOPE (European Standard Operating Procedures of Electrochemotherapy) study. Eur. J. Cancer Suppl. 2006, 4, 3–13. [Google Scholar] [CrossRef]
- Eaton, A.A.; Baser, R.E.; Seidel, B.; Stabile, C.; Canty, J.P.; Goldfrank, D.J.; Carter, J. Validation of Clinical Tools for Vaginal and Vulvar Symptom Assessment in Cancer Patients and Survivors. J. Sex. Med. 2017, 14, 144–151. [Google Scholar] [CrossRef]
- Rabin, R.; De Charro, F. EQ-5D: A measure of health status from the EuroQol Group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.S.; Kohlmann, T.; Janssen, M.F.; Buchholz, I. Psychometric properties of the EQ-5D-5L: A systematic review of the literature. Qual. Life Res. 2020, 30, 647–673. [Google Scholar] [CrossRef] [PubMed]
- Janda, M.; Obermair, A.; Cella, D.; Perrin, L.C.; Nicklin, J.L.; Ward, B.G.; Crandon, A.J.; Trimmel, M. The functional assessment of cancer-vulvar: Reliability and validity. Gynecol. Oncol. 2005, 97, 568–575. [Google Scholar] [CrossRef]
- Senn, B.; Gafner, D.; Happ, M.B.; Eicher, M.; Mueller, M.D.; Engberg, S.; Spirig, R. The unspoken disease: Symptom experience in women with vulval neoplasia and surgical treatment: A qualitative study. Eur. J. Cancer Care 2011, 20, 747–758. [Google Scholar] [CrossRef]
- Alimena, S.; Sullivan, M.W.; Philp, L.; Dorney, K.; Hubbell, H.; del Carmen, M.G.; Goodman, A.; Bregar, A.; Growdon, W.B.; Eisenhauer, E.L.; et al. Patient reported outcome measures among patients with vulvar cancer at various stages of treatment, recurrence, and survivorship. Gynecol. Oncol. 2020, 160, 252–259. [Google Scholar] [CrossRef]
- Novackova, M.; Halaska, M.J.; Robova, H.; Mala, I.; Pluta, M.; Chmel, R.; Rob, L. A prospective study in the evaluation of quality of life after vulvar cancer surgery. Int. J. Gynecol. Cancer 2015, 25, 166–173. [Google Scholar] [CrossRef]
- Janda, M.; Obermair, A.; Cella, D.; Crandon, A.J.; Trimmel, M. Vulvar cancer patients’ quality of life: A qualitative assessment. Int. J. Gynecol. Cancer 2004, 14, 875–881. [Google Scholar] [CrossRef] [PubMed]
- De Melo Ferreira, A.P.; De Figueiredo, E.M.; Lima, R.A.; Cândido, E.B.; De Castro Monteiro, M.V.; De Figueiredo Franco, T.M.R.; Traiman, P.; Da Silva-Filho, A.L. Quality of life in women with vulvar cancer submitted to surgical treatment: A comparative study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 165, 91–95. [Google Scholar] [CrossRef]
- De Hullu, J.A.; van der Zee, A.G.J. Surgery and radiotherapy in vulvar cancer. Crit. Rev. Oncol. Hematol. 2006, 60, 38–58. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group (n) | Baseline | Early Follow-Up | Late Follow-Up | ||
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | p-Value vs. Baseline | Mean ± SD | p-Value vs. Baseline | |
| Type of response | |||||
| CR (29) | 6.1 ± 1.9 | 3.7 ± 2.3 | <0.0001 | 3.7 ± 2.9 | 0.0017 |
| PR (17) | 6.3 ± 2.3 | 3.7 ± 2.0 | <0.0001 | 4.7 ± 2.2 | 0.0060 |
| STD + PD (9) | 7.3 ± 0.9 | 6.9 ± 2.4 | 0.6235 | 7.4 ± 1.9 | 0.7882 |
| Type of anatomical site of the Lesion(s) | |||||
| A (11) | 6.0 ± 1.9 | 4.2 ± 2.1 | 0.0145 | 5.1 ± 2.4 | 0.2471 |
| M (34) | 5.7 ± 2.1 | 3.8 ± 2.4 | <0.0001 | 4.1 ± 3.0 | 0.0051 |
| P (10) | 8.2 ± 1.4 | 5.7 ± 2.9 | 0.0128 | 5.5 ± 2.2 | 0.0054 |
| Number of lesion(s) | |||||
| Single (34) | 5.8 ± 2.4 | 4.2 ± 2.5 | <0.0001 | 4.6 ± 2.9 | 0.0065 |
| Multiple (21) | 6.8 ± 1.6 | 4.3 ± 2.5 | 0.0002 | 4.6 ± 2.6 | 0.0039 |
| Size of lesion(s) | |||||
| ≤30 mm (37) | 5.7 ± 1.9 | 4.0 ± 2.5 | <0.0001 | 4.4 ± 2.9 | 0.0052 |
| >30 mm (18) | 7.2 ± 2.2 | 4.8 ± 2.3 | 0.0002 | 5.1 ± 2.6 | 0.0070 |
| Whole study population | |||||
| 55 | 6.1 ± 2.1 | 4.3 ± 2.5 | <0.0001 | 4.6 ± 2.8 | <0.0001 |
| Group (n) | Baseline | Early Follow-Up | Late Follow-Up | ||
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | p-Value vs. Baseline | Mean ± SD | p-Value vs. Baseline | |
| Type of response | |||||
| CR (29) | 7.3 ± 3.8 | 10.3 ± 3.6 | 0.0008 | 9.4 ± 4.3 | 0.1533 |
| PR (17) | 7.3 ± 4.0 | 10.5 ± 4.1 | 0.0054 | 9.4 ± 3.9 | 0.0092 |
| STD + PD (9) | 6.1 ± 3.0 | 5.9 ± 3.6 | 0.6767 | 6.1 ± 3.4 | 0.6914 |
| Type of anatomical site of the lesion(s) | |||||
| A (11) | 8.1 ± 3.9 | 10.2 ± 2.7 | 0.0474 | 9.4 ± 3.2 | 0.2818 |
| M (34) | 7.7 ± 3.3 | 10.1 ± 3.7 | 0.0070 | 9.1 ± 4.2 | 0.3227 |
| P (10) | 4.1 ± 3.3 | 7.5 ± 5.8 | 0.0057 | 7.8 ± 5.2 | 0.0045 |
| Number of lesion(s) | |||||
| Single (34) | 7.3 ± 3.9 | 9.5 ± 4.3 | 0.0008 | 8.7 ± 4.9 | 0.0836 |
| Multiple (21) | 7.0 ± 3.3 | 9.8 ± 3.7 | 0.0073 | 9.2 ± 3.2 | 0.0681 |
| Size of lesion(s) | |||||
| ≤30 mm (37) | 7.8 ± 3.5 | 10.3 ± 4.0 | 0.0022 | 9.2 ± 4.1 | 0.1613 |
| >30 mm (18) | 5.7 ± 3.6 | 7.9 ± 3.7 | 0.0067 | 7.9 ± 4.0 | 0.0241 |
| Whole study population | |||||
| 55 | 7.1 ± 3.6 | 9.6 ± 4.9 | <0.0001 | 8.9 ± 4.1 | <0.0054 |
| Group (n) | Baseline | Early Follow-Up | Late Follow-Up | ||
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | p-Value vs. Baseline | Mean ± SD | p-Value vs. Baseline | |
| Type of response | |||||
| CR (29) | 0.66 ± 0.28 | 0.72 ± 0.19 | 0.2398 | 0.66 ± 0.29 | 0.9107 |
| PR (17) | 0.59 ± 0.47 | 0.65 ± 0.44 | 0.5698 | 0.54 ± 0.45 | 0.4787 |
| STD + PD (9) | 0.66 ± 0.31 | 0.48 ± 0.51 | 0.5778 | 0.41 ± 0.53 | 0.3925 |
| Type of anatomical site of the lesion(s) | |||||
| A (11) | 0.62 ± 0.42 | 0.76 ± 0.18 | 0.4315 | 0.60 ± 0.35 | 0.3131 |
| M (34) | 0.64 ± 0.28 | 0.68 ± 0.30 | 0.8223 | 0.61 ± 0.34 | 0.4138 |
| P (10) | 0.47 ± 0.59 | 0.46 ± 0.56 | 0.1490 | 0.48 ± 0.58 | 0.0788 |
| Number of lesion(s) | |||||
| Single (34) | 0.60 ± 0.38 | 0.62 ± 0.40 | 0.6509 | 0.54 ± 0.42 | 0.3992 |
| Multiple (21) | 0.63 ± 0.37 | 0.72 ± 0.24 | 0.3572 | 0.66 ± 0.33 | 0.8301 |
| Size of lesion(s) | |||||
| ≤30 mm (37) | 0.72 ± 0.20 | 0.76 ± 0.24 | 0.6743 | 0.67 ± 0.33 | 0.1916 |
| >30 mm (18) | 0.37 ± 0.54 | 0.41 ± 0.44 | 0.5154 | 0.38 ± 0.45 | 0.6699 |
| Whole study population | |||||
| 55 | 0.59 ± 0.38 | 0.64 ± 0.37 | 0.4269 | 0.57 ± 0.40 | 0.4279 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perrone, A.M.; Ferioli, M.; Argnani, L.; De Terlizzi, F.; Pirovano, C.; Covarelli, P.; Dondi, G.; Tesei, M.; De Crescenzo, E.; Ravegnini, G.; et al. Quality of Life with Vulvar Carcinoma Treated with Palliative Electrochemotherapy: The ELECHTRA (ELEctroCHemoTherapy vulvaR cAncer) Study. Cancers 2021, 13, 1622. https://doi.org/10.3390/cancers13071622
Perrone AM, Ferioli M, Argnani L, De Terlizzi F, Pirovano C, Covarelli P, Dondi G, Tesei M, De Crescenzo E, Ravegnini G, et al. Quality of Life with Vulvar Carcinoma Treated with Palliative Electrochemotherapy: The ELECHTRA (ELEctroCHemoTherapy vulvaR cAncer) Study. Cancers. 2021; 13(7):1622. https://doi.org/10.3390/cancers13071622
Chicago/Turabian StylePerrone, Anna Myriam, Martina Ferioli, Lisa Argnani, Francesca De Terlizzi, Cecilia Pirovano, Piero Covarelli, Giulia Dondi, Marco Tesei, Eugenia De Crescenzo, Gloria Ravegnini, and et al. 2021. "Quality of Life with Vulvar Carcinoma Treated with Palliative Electrochemotherapy: The ELECHTRA (ELEctroCHemoTherapy vulvaR cAncer) Study" Cancers 13, no. 7: 1622. https://doi.org/10.3390/cancers13071622
APA StylePerrone, A. M., Ferioli, M., Argnani, L., De Terlizzi, F., Pirovano, C., Covarelli, P., Dondi, G., Tesei, M., De Crescenzo, E., Ravegnini, G., Galuppi, A., Morganti, A. G., & De Iaco, P. (2021). Quality of Life with Vulvar Carcinoma Treated with Palliative Electrochemotherapy: The ELECHTRA (ELEctroCHemoTherapy vulvaR cAncer) Study. Cancers, 13(7), 1622. https://doi.org/10.3390/cancers13071622