
Impact of Local Liver Irradiation Concurrent Versus Sequential with Lenvatinib on Pharmacokinetics and Biodistribution




Simple Summary
Abstract
1. Introduction
2. Materials and methods
2.1. Chemicals and Reagents
2.2. High-Performance Liquid Chromatography-Ultraviolet (HPLC-UV)
2.3. Method Validation: Calibration Curve
2.4. Method Validation: Precision, Accuracy, and Recovery
2.5. Experimental Animals and Drug Administration
2.5.1. Animals and Sample Preparation
2.5.2. Irradiation Technique
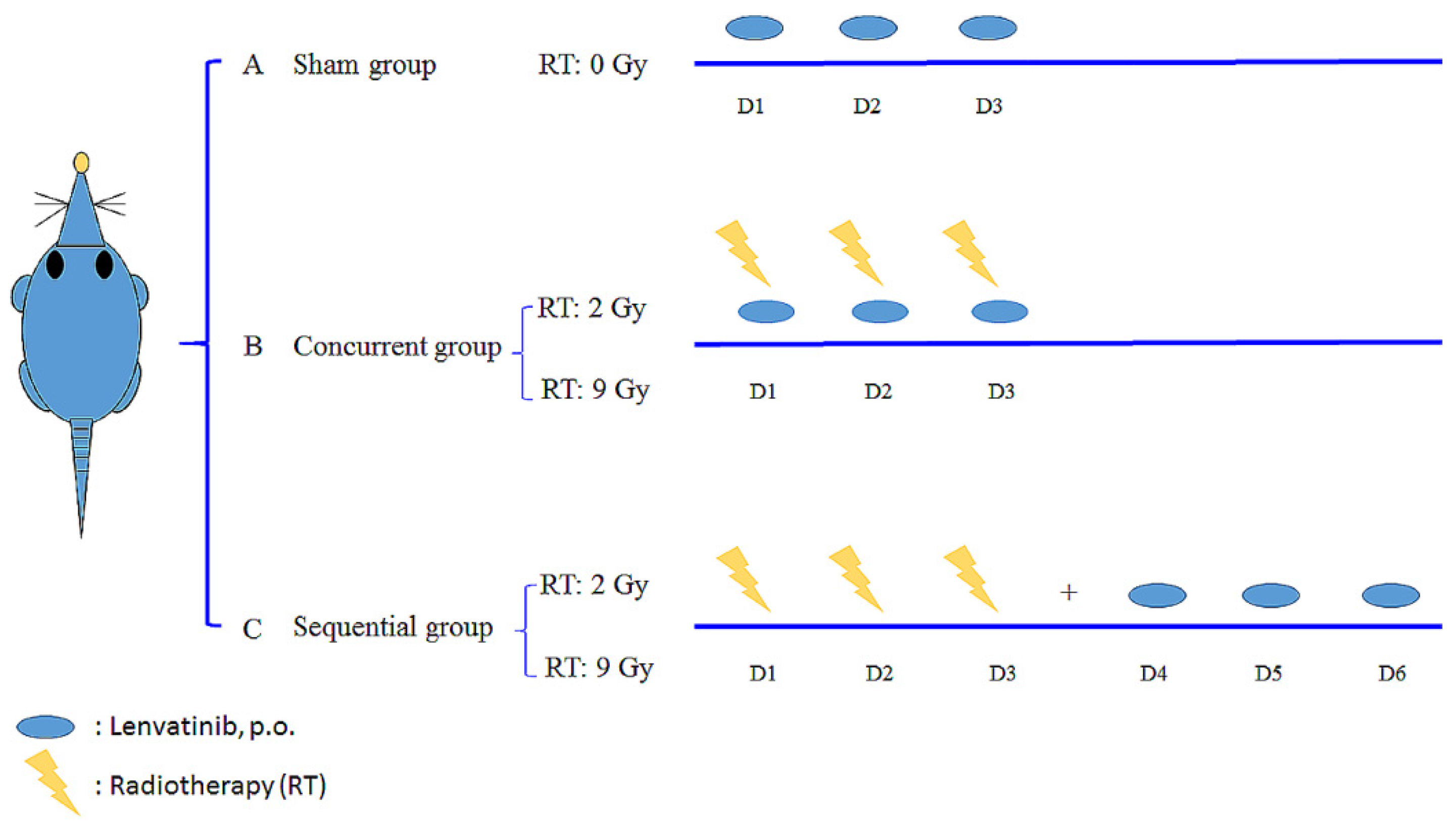
2.5.3. Drug Delivery with Different Schedules and Doses of RT
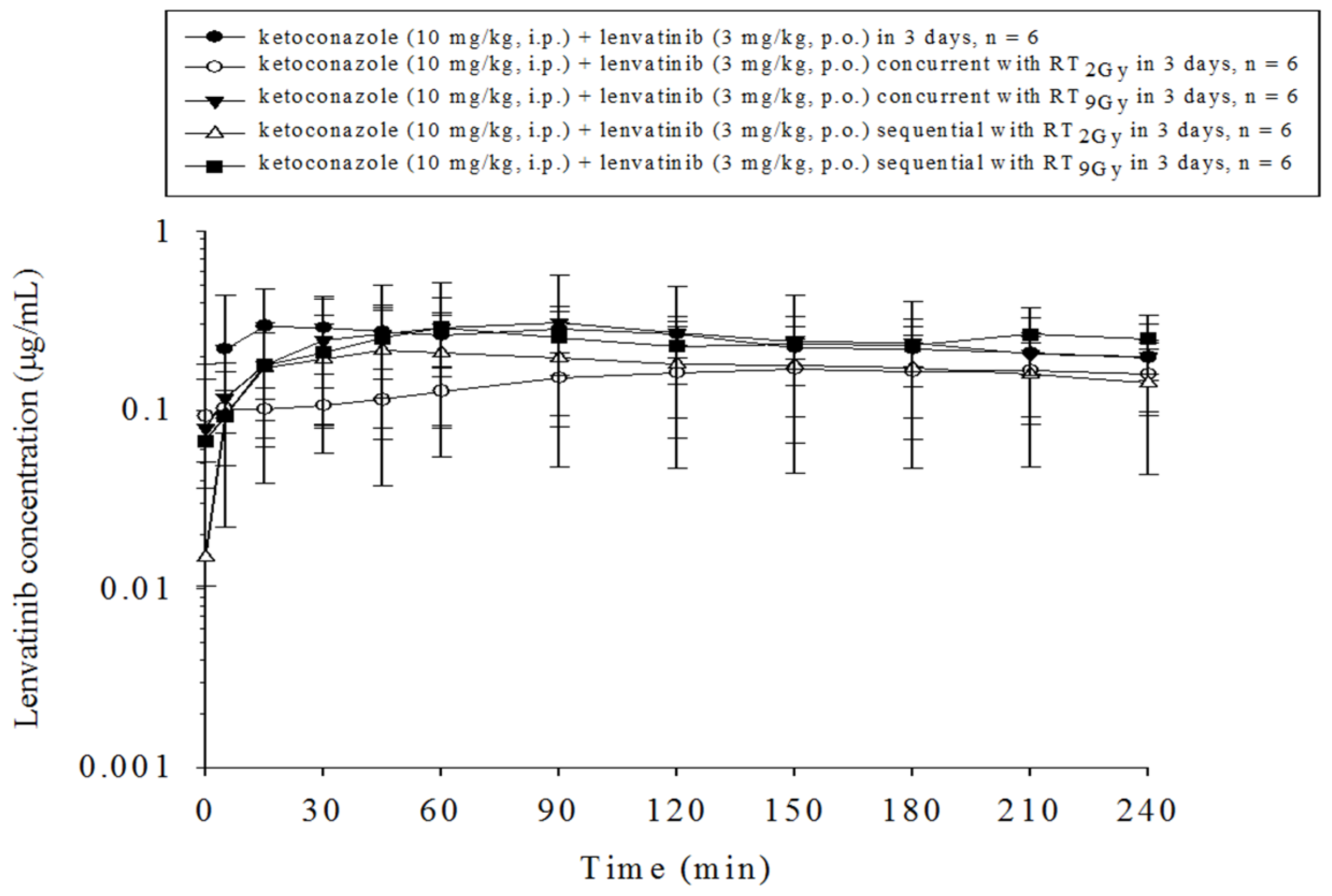
2.5.4. Pretreatment with Ketoconazole for Drug Delivery with RT under Different Time Schedules and Doses
2.5.5. Sample Preparation
2.5.6. Organ Distribution
2.5.7. Organ Samples
2.5.8. Hepatic and Renal Functions
2.6. Pharmacokinetics and Data Analysis
2.7. Calculations and Data Analysis
3. Results
3.1. Method of Validation for Linearity, Recovery, Precision, Accuracy, and Stability
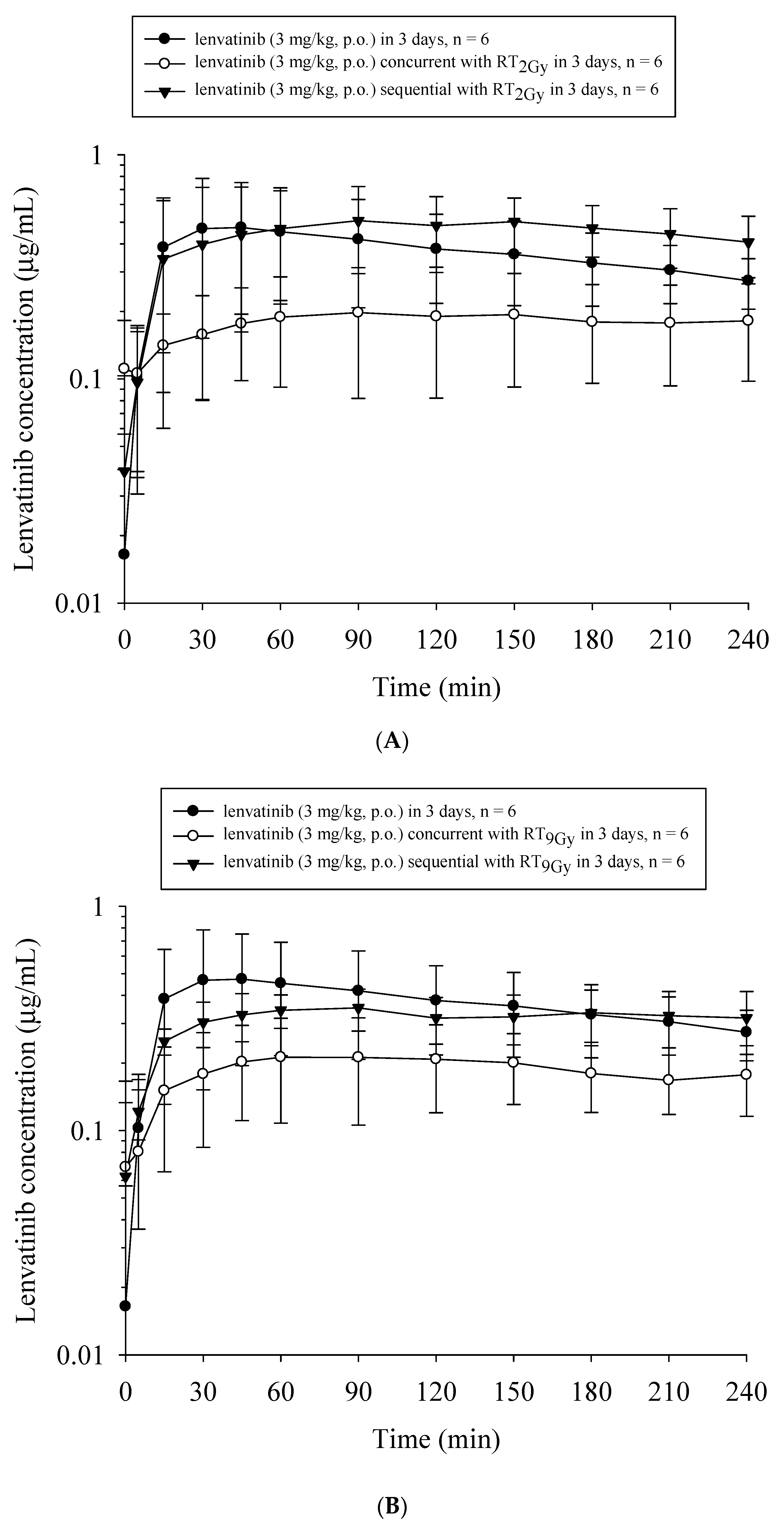
3.2. Both RT2Gy and RT9Gy Modulated the AUC of Lenvatinib in the Plasma of Freely Moving Rats
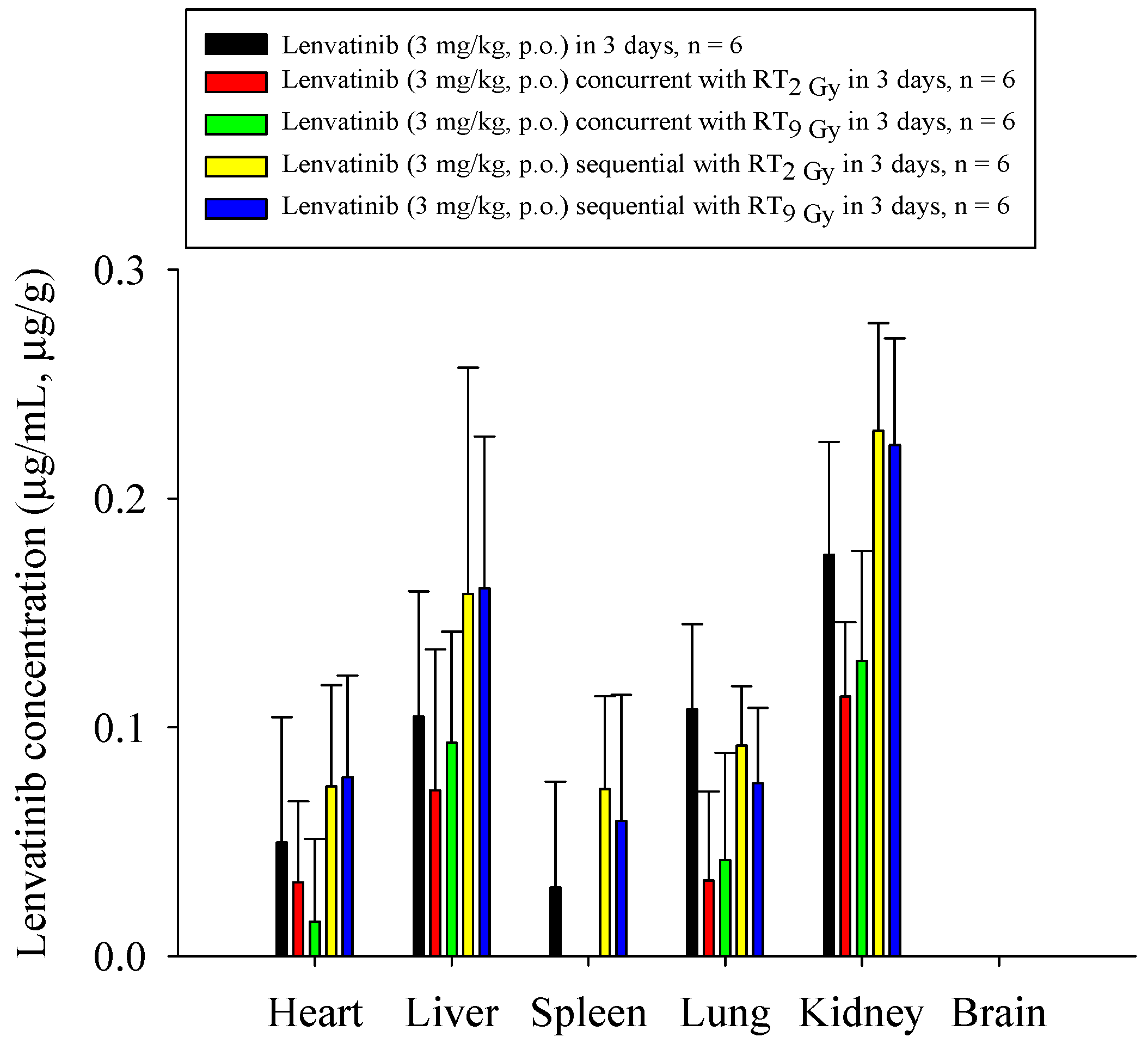
3.3. Organ Distribution under Different RT and Lenvatinib Regimens
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kulik, L.; El-Serag, H.B. Epidemiology and Management of Hepatocellular Carcinoma. Gastroenterology 2019, 156, 477–491. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef]
- Cheng, A.L.; Kang, Y.K.; Chen, Z.; Tsao, C.J.; Qin, S.; Kim, J.S.; Luo, R.; Feng, J.; Ye, S.; Yang, T.S.; et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009, 10, 25–34. [Google Scholar] [CrossRef]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef]
- Munoz-Schuffenegger, P.; Barry, A.; Atenafu, E.G.; Kim, J.; Brierley, J.; Ringash, J.; Brade, A.; Dinniwell, R.; Wong, R.K.S.; Cho, C.; et al. Stereotactic body radiation therapy for hepatocellular carcinoma with Macrovascular invasion. Radiother. Oncol. 2020, 156, 120–126. [Google Scholar] [CrossRef]
- Wahl, D.R.; Stenmark, M.H.; Tao, Y.; Pollom, E.L.; Caoili, E.M.; Lawrence, T.S.; Schipper, M.J.; Feng, M. Outcomes After Stereotactic Body Radiotherapy or Radiofrequency Ablation for Hepatocellular Carcinoma. J. Clin. Oncol. 2016, 34, 452–459. [Google Scholar] [CrossRef]
- Chen, S.W.; Lin, L.C.; Kuo, Y.C.; Liang, J.A.; Kuo, C.C.; Chiou, J.F. Phase 2 study of combined sorafenib and radiation therapy in patients with advanced hepatocellular carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 1041–1047. [Google Scholar] [CrossRef]
- Hsieh, C.H.; Chen, Y.J.; Tsai, T.H.; Wang, L.Y.; Tai, H.C.; Huang, H.L.; Huang, Y.C. Robust combination of liver stereotactic body radiotherapy modulates pharmacokinetics of sorafenib toward preferable parameters. Sci. Rep. 2020, 10, 9575. [Google Scholar] [CrossRef]
- Brade, A.M.; Ng, S.; Brierley, J.; Kim, J.; Dinniwell, R.; Ringash, J.; Wong, R.R.; Cho, C.; Knox, J.; Dawson, L.A. Phase 1 Trial of Sorafenib and Stereotactic Body Radiation Therapy for Hepatocellular Carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2016, 94, 580–587. [Google Scholar] [CrossRef]
- Goody, R.B.; Brade, A.M.; Wang, L.; Craig, T.; Brierley, J.; Dinniwell, R.; Wong, R.K.S.; Cho, C.; Kim, J.; Kassam, Z.; et al. Phase I trial of radiation therapy and sorafenib in unresectable liver metastases. Radiother. Oncol. 2017, 123, 234–239. [Google Scholar] [CrossRef]
- Kuo, M.T.; Liu, Z.; Wei, Y.; Lin-Lee, Y.C.; Tatebe, S.; Mills, G.B.; Unate, H. Induction of human MDR1 gene expression by 2-acetylaminofluorene is mediated by effectors of the phosphoinositide 3-kinase pathway that activate NF-kappaB signaling. Oncogene 2002, 21, 1945–1954. [Google Scholar] [CrossRef]
- Eyries, M.; Collins, T.; Khachigian, L.M. Modulation of growth factor gene expression in vascular cells by oxidative stress. Endothel. J. Endothel. Cell Res. 2004, 11, 133–139. [Google Scholar] [CrossRef]
- Sukhatme, V.P.; Cao, X.M.; Chang, L.C.; Tsai-Morris, C.H.; Stamenkovich, D.; Ferreira, P.C.; Cohen, D.R.; Edwards, S.A.; Shows, T.B.; Curran, T.; et al. A zinc finger-encoding gene coregulated with c-fos during growth and differentiation, and after cellular depolarization. Cell 1988, 53, 37–43. [Google Scholar] [CrossRef]
- Matsui, J.; Funahashi, Y.; Uenaka, T.; Watanabe, T.; Tsuruoka, A.; Asada, M. Multi-kinase inhibitor E7080 suppresses lymph node and lung metastases of human mammary breast tumor MDA-MB-231 via inhibition of vascular endothelial growth factor-receptor (VEGF-R) 2 and VEGF-R3 kinase. Clin. Cancer Res. 2008, 14, 5459–5465. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, Y.; Matsui, J.; Matsushima, T.; Obaishi, H.; Miyazaki, K.; Nakamura, K.; Tohyama, O.; Semba, T.; Yamaguchi, A.; Hoshi, S.S.; et al. Lenvatinib, an angiogenesis inhibitor targeting VEGFR/FGFR, shows broad antitumor activity in human tumor xenograft models associated with microvessel density and pericyte coverage. Vasc. Cell 2014, 6, 18. [Google Scholar] [CrossRef] [PubMed]
- Shumaker, R.C.; Aluri, J.; Fan, J.; Martinez, G.; Thompson, G.A.; Ren, M. Effect of rifampicin on the pharmacokinetics of lenvatinib in healthy adults. Clin. Investig. 2014, 34, 651–659. [Google Scholar] [CrossRef][Green Version]
- Achira, M.; Suzuki, H.; Ito, K.; Sugiyama, Y. Comparative studies to determine the selective inhibitors for P-glycoprotein and cytochrome P4503A4. AAPS PharmSci 1999, 1, E18. [Google Scholar] [CrossRef][Green Version]
- Thummel, K.E.; Wilkinson, G.R. In vitro and in vivo drug interactions involving human CYP3A. Annu. Rev. Pharmacol. Toxicol. 1998, 38, 389–430. [Google Scholar] [CrossRef]
- Liu, L.; Cao, Y.; Chen, C.; Zhang, X.; McNabola, A.; Wilkie, D.; Wilhelm, S.; Lynch, M.; Carter, C. Sorafenib blocks the RAF/MEK/ERK pathway, inhibits tumor angiogenesis, and induces tumor cell apoptosis in hepatocellular carcinoma model PLC/PRF/5. Cancer Res. 2006, 66, 11851–11858. [Google Scholar] [CrossRef] [PubMed]
- Wilhelm, S.; Carter, C.; Lynch, M.; Lowinger, T.; Dumas, J.; Smith, R.A.; Schwartz, B.; Simantov, R.; Kelley, S. Discovery and development of sorafenib: A multikinase inhibitor for treating cancer. Nat. Rev. Drug Discov. 2006, 5, 835–844. [Google Scholar] [CrossRef]
- Wild, A.T.; Gandhi, N.; Chettiar, S.T.; Aziz, K.; Gajula, R.P.; Williams, R.D.; Kumar, R.; Taparra, K.; Zeng, J.; Cades, J.A.; et al. Concurrent versus sequential sorafenib therapy in combination with radiation for hepatocellular carcinoma. PLoS ONE 2013, 8, e65726. [Google Scholar] [CrossRef] [PubMed]
- Yu, W.; Gu, K.; Yu, Z.; Yuan, D.; He, M.; Ma, N.; Lai, S.; Zhao, J.; Ren, Z.; Zhang, X.; et al. Sorafenib potentiates irradiation effect in hepatocellular carcinoma in vitro and in vivo. Cancer Lett 2013, 329, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Schlumberger, M.; Tahara, M.; Wirth, L.J.; Robinson, B.; Brose, M.S.; Elisei, R.; Habra, M.A.; Newbold, K.; Shah, M.H.; Hoff, A.O.; et al. Lenvatinib versus placebo in radioiodine-refractory thyroid cancer. N. Engl. J. Med. 2015, 372, 621–630. [Google Scholar] [CrossRef]
- Motzer, R.J.; Hutson, T.E.; Glen, H.; Michaelson, M.D.; Molina, A.; Eisen, T.; Jassem, J.; Zolnierek, J.; Maroto, J.P.; Mellado, B.; et al. Lenvatinib, everolimus, and the combination in patients with metastatic renal cell carcinoma: A randomised, phase 2, open-label, multicentre trial. Lancet Oncol. 2015, 16, 1473–1482. [Google Scholar] [CrossRef]
- Stetler-Stevenson, W.G. Matrix metalloproteinases in angiogenesis: A moving target for therapeutic intervention. J. Clin. Investig. 1999, 103, 1237–1241. [Google Scholar] [CrossRef] [PubMed]
- Zeng, H.; Dvorak, H.F.; Mukhopadhyay, D. Vascular permeability factor (VPF)/vascular endothelial growth factor (VEGF) peceptor-1 down-modulates VPF/VEGF receptor-2-mediated endothelial cell proliferation, but not migration, through phosphatidylinositol 3-kinase-dependent pathways. J. Biol. Chem. 2001, 276, 26969–26979. [Google Scholar] [CrossRef]
- Wachsberger, P.; Burd, R.; Dicker, A.P. Tumor response to ionizing radiation combined with antiangiogenesis or vascular targeting agents: Exploring mechanisms of interaction. Clin. Cancer Res. 2003, 9, 1957–1971. [Google Scholar]
- Abdollahi, A.; Lipson, K.E.; Han, X.; Krempien, R.; Trinh, T.; Weber, K.J.; Hahnfeldt, P.; Hlatky, L.; Debus, J.; Howlett, A.R.; et al. SU5416 and SU6668 attenuate the angiogenic effects of radiation-induced tumor cell growth factor production and amplify the direct anti-endothelial action of radiation in vitro. Cancer Res. 2003, 63, 3755–3763. [Google Scholar]
- Timke, C.; Zieher, H.; Roth, A.; Hauser, K.; Lipson, K.E.; Weber, K.J.; Debus, J.; Abdollahi, A.; Huber, P.E. Combination of vascular endothelial growth factor receptor/platelet-derived growth factor receptor inhibition markedly improves radiation tumor therapy. Clin. Cancer Res. 2008, 14, 2210–2219. [Google Scholar] [CrossRef]
- Li, M.; Ping, G.; Plathow, C.; Trinh, T.; Lipson, K.E.; Hauser, K.; Krempien, R.; Debus, J.; Abdollahi, A.; Huber, P.E. Small molecule receptor tyrosine kinase inhibitor of platelet-derived growth factor signaling (SU9518) modifies radiation response in fibroblasts and endothelial cells. BMC Cancer 2006, 6, 79. [Google Scholar] [CrossRef]
- Li, N.; Karin, M. Ionizing radiation and short wavelength UV activate NF-kappaB through two distinct mechanisms. Proc. Natl. Acad. Sci. USA 1998, 95, 13012–13017. [Google Scholar] [CrossRef]
- Jain, R.K.; Duda, D.G.; Clark, J.W.; Loeffler, J.S. Lessons from phase III clinical trials on anti-VEGF therapy for cancer. Nat. Clin. Pract. Oncol. 2006, 3, 24–40. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, M.S. Radiation combined with antiangiogenic and antivascular agents. Semin. Radiat. Oncol. 2006, 16, 45–50. [Google Scholar] [CrossRef]
- Harada, H.; Inoue, M.; Itasaka, S.; Hirota, K.; Morinibu, A.; Shinomiya, K.; Zeng, L.; Ou, G.; Zhu, Y.; Yoshimura, M.; et al. Cancer cells that survive radiation therapy acquire HIF-1 activity and translocate towards tumour blood vessels. Nat. Commun. 2012, 3, 783. [Google Scholar] [CrossRef]
- Kolesnick, R.; Fuks, Z. Radiation and ceramide-induced apoptosis. Oncogene 2003, 22, 5897–5906. [Google Scholar] [CrossRef]
- Garnett, C.T.; Palena, C.; Chakraborty, M.; Tsang, K.Y.; Schlom, J.; Hodge, J.W. Sublethal irradiation of human tumor cells modulates phenotype resulting in enhanced killing by cytotoxic T lymphocytes. Cancer Res. 2004, 64, 7985–7994. [Google Scholar] [CrossRef] [PubMed]
- Van Lint, P.; Libert, C. Matrix metalloproteinase-8: Cleavage can be decisive. Cytokine Growth Factor Rev. 2006, 17, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, R.E.; Dejonckheere, E.; Van Lint, P.; Demeestere, D.; Van Wonterghem, E.; Vanlaere, I.; Puimege, L.; Van Hauwermeiren, F.; De Rycke, R.; Mc Guire, C.; et al. Matrix metalloprotease 8-dependent extracellular matrix cleavage at the blood-CSF barrier contributes to lethality during systemic inflammatory diseases. J. Neurosci. Off. J. Soc. Neurosci. 2012, 32, 9805–9816. [Google Scholar] [CrossRef]
- Weiss, S.J.; Peppin, G.; Ortiz, X.; Ragsdale, C.; Test, S.T. Oxidative autoactivation of latent collagenase by human neutrophils. Science 1985, 227, 747–749. [Google Scholar] [CrossRef]
- Quintero-Fabian, S.; Arreola, R.; Becerril-Villanueva, E.; Torres-Romero, J.C.; Arana-Argaez, V.; Lara-Riegos, J.; Ramirez-Camacho, M.A.; Alvarez-Sanchez, M.E. Role of Matrix Metalloproteinases in Angiogenesis and Cancer. Front. Oncol. 2019, 9, 1370. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Yin, Y.; Wang, X.; Wu, Z.; Liu, Y.; Zhang, F.; Lin, J.; Huang, Z.; Zhou, L. Sublethal irradiation promotes the metastatic potential of hepatocellular carcinoma cells. Cancer Sci. 2021, 112, 265–274. [Google Scholar] [CrossRef]
- Hsieh, C.H.; Liu, C.Y.; Hsieh, Y.J.; Tai, H.C.; Wang, L.Y.; Tsai, T.H.; Chen, Y.J. Matrix metalloproteinase-8 mediates the unfavorable systemic impact of local irradiation on pharmacokinetics of anti-cancer drug 5-Fluorouracil. PLoS ONE 2011, 6, e21000. [Google Scholar] [CrossRef]
- Mehta, M.; Griffith, J.; Panneerselvam, J.; Babu, A.; Mani, J.; Herman, T.; Ramesh, R.; Munshi, A. Regorafenib sensitizes human breast cancer cells to radiation by inhibiting multiple kinases and inducing DNA damage. Int. J. Radiat. Biol. 2020, 1–12. [Google Scholar] [CrossRef]
- Suzuki, K.; Iwai, H.; Utsunomiya, K.; Kono, Y.; Kobayashi, Y.; Van Bui, D.; Sawada, S.; Yun, Y.; Mitani, A.; Kondo, N.; et al. Combination therapy with lenvatinib and radiation significantly inhibits thyroid cancer growth by uptake of tyrosine kinase inhibitor. Exp. Cell Res. 2021, 398, 112390. [Google Scholar] [CrossRef]
- Plastaras, J.P.; Kim, S.H.; Liu, Y.Y.; Dicker, D.T.; Dorsey, J.F.; McDonough, J.; Cerniglia, G.; Rajendran, R.R.; Gupta, A.; Rustgi, A.K.; et al. Cell cycle dependent and schedule-dependent antitumor effects of sorafenib combined with radiation. Cancer Res. 2007, 67, 9443–9454. [Google Scholar] [CrossRef]
- Tsai, T.H.; Chen, Y.J.; Wang, L.Y.; Hsieh, C.H. Effect of Synchronous Versus Sequential Regimens on the Pharmacokinetics and Biodistribution of Regorafenib with Irradiation. Pharmaceutics 2021, 13, 386. [Google Scholar] [CrossRef]
- Liu, J.H.; Tsai, T.H.; Chen, Y.J.; Wang, L.Y.; Liu, H.Y.; Hsieh, C.H. Local Irradiation Modulates the Pharmacokinetics of Metabolites in 5-Fluorouracil-Radiotherapy-Pharmacokinetics Phenomenon. Front. Pharmacol. 2020, 11, 141. [Google Scholar] [CrossRef]
- Chen, Y.J.; Tsai, T.H.; Wang, L.Y.; Hsieh, C.H. Local Radiotherapy Affects Drug Pharmacokinetics-Exploration of a Neglected but Significant Uncertainty of Cancer Therapy. Technol. Cancer Res. Treat. 2017, 16, 705–716. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.H.; Hou, M.L.; Chiang, M.H.; Tai, H.C.; Tien, H.J.; Wang, L.Y.; Tsai, T.H.; Chen, Y.J. Head and neck irradiation modulates pharmacokinetics of 5-fluorouracil and cisplatin. J. Transl. Med. 2013, 11, 231. [Google Scholar] [CrossRef] [PubMed]
- Tsai, T.H.; Chen, Y.J.; Hou, M.L.; Wang, L.Y.; Tai, H.C.; Hsieh, C.H. Pelvic irradiation modulates the pharmacokinetics of cisplatin in the plasma and lymphatic system. Am. J. Transl. Res. 2015, 7, 375–384. [Google Scholar]
- Zhang, X.; Li, Y.; Huang, Q.; Wang, H.; Yan, B.; Dewhirst, M.W.; Li, C.Y. Increased resistance of tumor cells to hyperthermia mediated by integrin-linked kinase. Clin. Cancer Res. 2003, 9, 1155–1160. [Google Scholar]
- Shumaker, R.; Aluri, J.; Fan, J.; Martinez, G.; Thompson, G.A.; Ren, M. Effects of Ketoconazole on the Pharmacokinetics of Lenvatinib (E7080) in Healthy Participants. Clin. Pharmacol. Drug Dev. 2015, 4, 155–160. [Google Scholar] [CrossRef]
- Purdy, J.A. Dose to normal tissues outside the radiation therapy patient’s treated volume: A review of different radiation therapy techniques. Health Phys. 2008, 95, 666–676. [Google Scholar] [CrossRef]
- Blettner, M.; Boice, J.D., Jr. Radiation dose and leukaemia risk: General relative risk techniques for dose-response models in a matched case-control study. Stat. Med. 1991, 10, 1511–1526. [Google Scholar] [CrossRef] [PubMed]
- Coppes, R.P.; Muijs, C.T.; Faber, H.; Gross, S.; Schippers, J.M.; Brandenburg, S.; Langendijk, J.A.; van Luijk, P. Volume-dependent expression of in-field and out-of-field effects in the proton-irradiated rat lung. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Cabanillas, M.E.; Takahashi, S. Managing the adverse events associated with lenvatinib therapy in radioiodine-refractory differentiated thyroid cancer. Semin. Oncol. 2019, 46, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Wirth, L.J.; Tahara, M.; Robinson, B.; Francis, S.; Brose, M.S.; Habra, M.A.; Newbold, K.; Kiyota, N.; Dutcus, C.E.; Mathias, E.; et al. Treatment-emergent hypertension and efficacy in the phase 3 Study of (E7080) lenvatinib in differentiated cancer of the thyroid (SELECT). Cancer 2018, 124, 2365–2372. [Google Scholar] [CrossRef]
- Launay-Vacher, V.; Deray, G. Hypertension and proteinuria: A class-effect of antiangiogenic therapies. Anticancer Drugs 2009, 20, 81–82. [Google Scholar] [CrossRef]
- Gupta, A.; Jarzab, B.; Capdevila, J.; Shumaker, R.; Hussein, Z. Population pharmacokinetic analysis of lenvatinib in healthy subjects and patients with cancer. Br. J. Clin. Pharmacol. 2016, 81, 1124–1133. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pharmacokinetics (PK) | Radiotherapy (RT) | CYP3A4 Modulation | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| RT2Gy | RT9Gy | RT2Gy | RT9Gy | ||||||||
| PK Parameters | Unit | Lenvatinib Only 3 mg/kg (n = 6) | RT Concurrent with Lenvatinib 3 mg/kg (n = 6) | RT Followed by Lenvatinib 3 mg/kg (n = 6) | RT Concurrent with Lenvatinib 3 mg/kg (n = 6) | RT Followed by Lenvatinib 3 mg/kg (n = 6) | KTZ Pretreatment + Lenvatinib 3 mg/kg (n = 6) | KTZ Pretreatment + RT Concurrent with Lenvatinib 3 mg/kg (n = 6) | KTZ Pretreatment + RT Followed by Lenvatinib 3 mg/kg (n = 6) | KTZ Pretreatment + RT Concurrent with Lenvatinib 3 mg/kg (n = 6) | KTZ Pretreatment + RT Followed by Lenvatinib 3 mg/kg (n = 6) |
| AUC0-T | min·µg/mL | 87.85 ± 38.2 | 42.96 ± 20.7 a | 106.5 ± 41.8 * | 44.83 ± 18.0 a | 75.70 ± 15.1 ** | 58.53 ± 11.1 | 35.06 ± 13.5 # | 42.18 ± 23.1 b | 58.19 ± 42.8 | 56.53 ± 22.6 |
| Tmax | min | 67.50 ± 55.1 | 152.5 ± 87.2 | 105.0 ± 52.8 | 110.0 ± 64.1 | 112.5 ± 79.2 | 123.3 ± 101 | 135.0 ± 86.4 | 90.00 ± 74.1 | 72.50 ± 30.6 | 112.5 ± 87.8 |
| Cmax | µg/mL | 0.531 ± 0.29 | 0.221 ± 0.1 | 0.561 ± 0.23 | 0.233 ± 0.1 | 0.393 ± 0.08 | 0.363 ± 0.13 | 0.183 ± 0.07 | 0.280 ± 0.13 | 0.318 ± 0.26 | 0.308 ± 0.11 |
| T1/2 | min | 621.3 ± 507 | 304.9 ± 149 | 444.5 ± 469 | 1998 ± 2989 | 575.2 ± 404 | 222.5 ± 178 | 864.2 ± 879 | 192.4 ± 127 | 845.8 ± 889 | 888.9 ± 692 |
| Organ (µg/mL) | Lenvatinib Only 3 mg/kg (n = 6) | RT2Gy | RT9 Gy | ||
|---|---|---|---|---|---|
| RT Concurrent with Lenvatinib 3 mg/kg (n = 6) | RT Followed by Lenvatinib 3 mg/kg (n = 6) | RT Concurrent with Lenvatinib 3 mg/kg (n = 6) | RT Followed by Lenvatinib 3 mg/kg (n = 6) | ||
| Heart | 0.05 ± 0.05 | 0.032 ± 0.04 (↓ 36.0%) | 0.074 ± 0.04 (↑ 48.0%) | 0.015 ± 0.04 (↓ 70.0%) | 0.078 ± 0.04 (↑ 56.0%) |
| Liver | 0.104 ± 0.05 | 0.072 ± 0.06 (↓ 30.8%) | 0.158 ± 0.09 (↑ 51.9%) | 0.093 ± 0.05 (↓ 10.6%) | 0.161 ± 0.07 (↑ 54.8%) |
| Spleen | 0.03 ± 0.05 | 0 (↓ 100.0%) | 0.073 ± 0.04 (↑ 143.3%) | 0 (↓ 100%) | 0.06 ± 0.06 (↑ 100%) |
| Lung | 0.108 ± 0.04 | 0.033 ± 0.04 ** (↓ 69.4%) | 0.092 ± 0.03 (↓ 14.8%) | 0.042 ± 0.05 * (↓ 61.1%) | 0.075 ± 0.03 (↓ 30.6%) |
| Kidney | 0.175 ± 0.05 | 0.113 ± 0.03 * (↓ 35.4%) | 0.23 ± 0.05 (↑ 31.4%) | 0.129 ± 0.05 (↓ 26.2%) | 0.223 ± 0.05 (↑ 27.4%) |
| Brain | 0 | 0 | 0 | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, T.-H.; Chen, Y.-J.; Wang, L.-Y.; Hsieh, C.-H. Impact of Local Liver Irradiation Concurrent Versus Sequential with Lenvatinib on Pharmacokinetics and Biodistribution. Cancers 2021, 13, 1598. https://doi.org/10.3390/cancers13071598
Tsai T-H, Chen Y-J, Wang L-Y, Hsieh C-H. Impact of Local Liver Irradiation Concurrent Versus Sequential with Lenvatinib on Pharmacokinetics and Biodistribution. Cancers. 2021; 13(7):1598. https://doi.org/10.3390/cancers13071598
Chicago/Turabian StyleTsai, Tung-Hu, Yu-Jen Chen, Li-Ying Wang, and Chen-Hsi Hsieh. 2021. "Impact of Local Liver Irradiation Concurrent Versus Sequential with Lenvatinib on Pharmacokinetics and Biodistribution" Cancers 13, no. 7: 1598. https://doi.org/10.3390/cancers13071598
APA StyleTsai, T.-H., Chen, Y.-J., Wang, L.-Y., & Hsieh, C.-H. (2021). Impact of Local Liver Irradiation Concurrent Versus Sequential with Lenvatinib on Pharmacokinetics and Biodistribution. Cancers, 13(7), 1598. https://doi.org/10.3390/cancers13071598