
Dietary Fats, Serum Cholesterol and Liver Cancer Risk: A Systematic Review and Meta-Analysis of Prospective Studies

Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection and Inclusion Criteria
2.3. Data Extraction and Quality Assessment
2.4. Patient Involvement
2.5. Statistical Methods
2.5.1. Statistical Synthesis
2.5.2. Heterogeneity
2.5.3. Sensitivity Analyses and Publication Bias
2.5.4. Software Used
3. Results
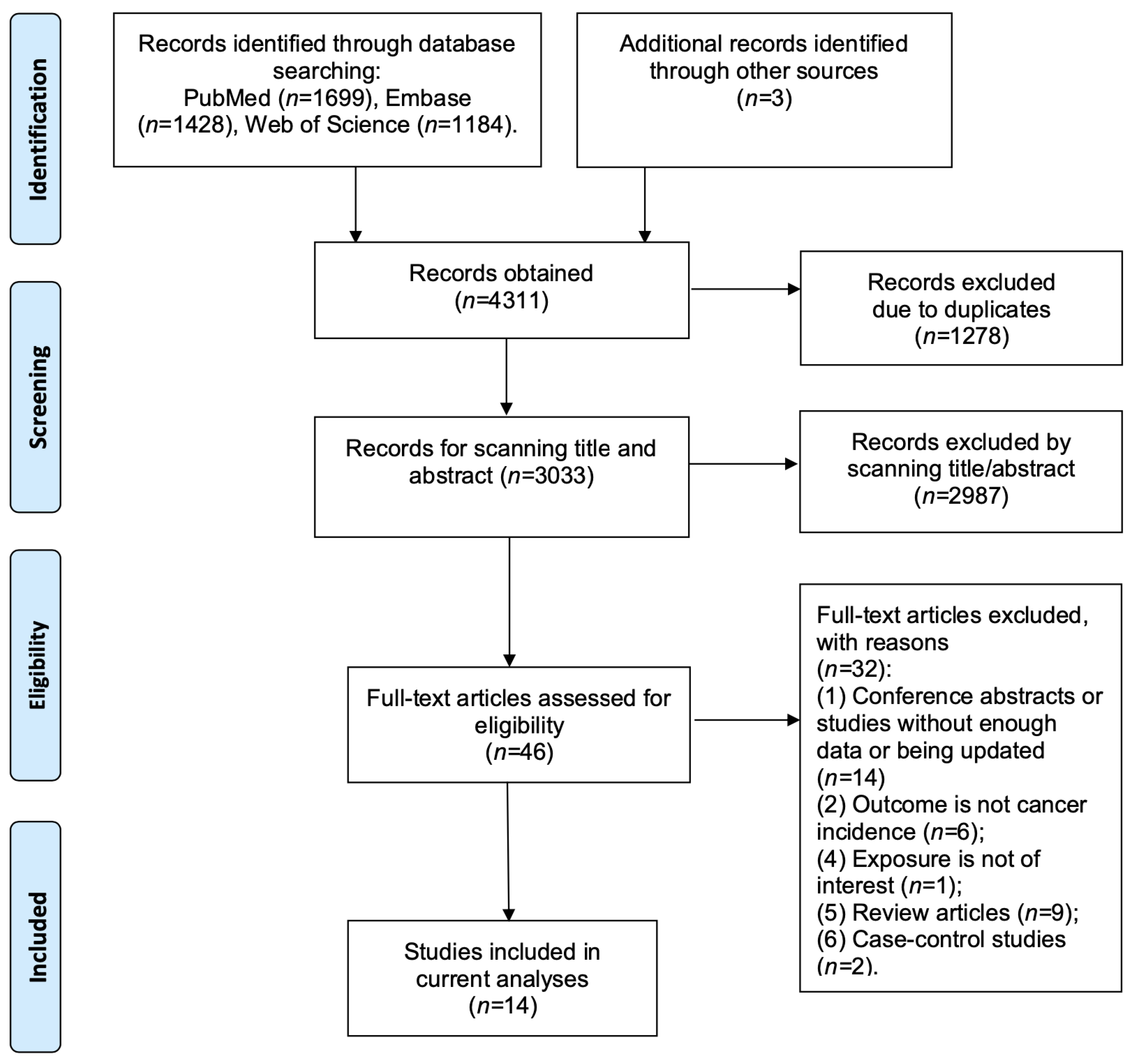
3.1. Literature Research and Data Abstraction
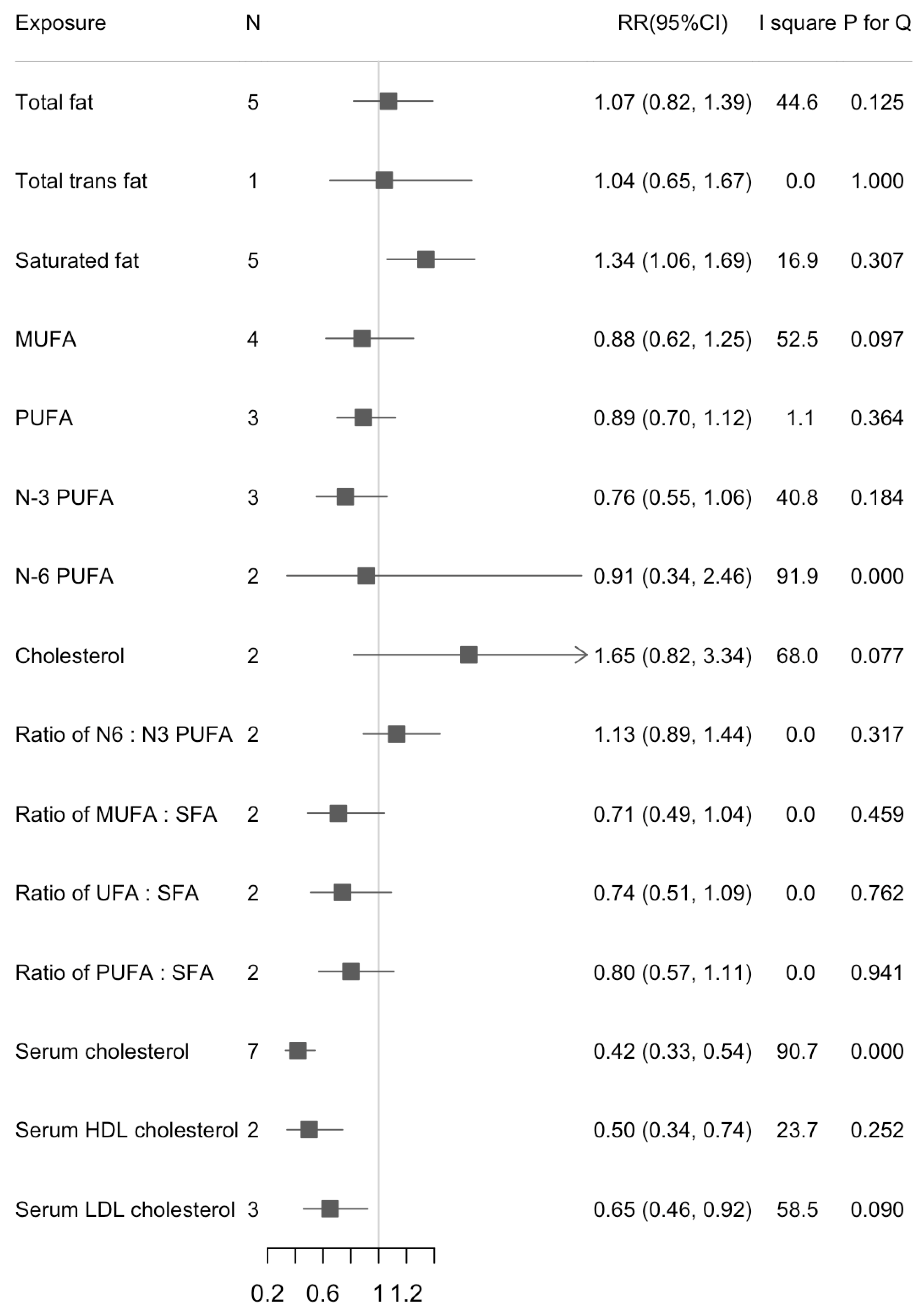
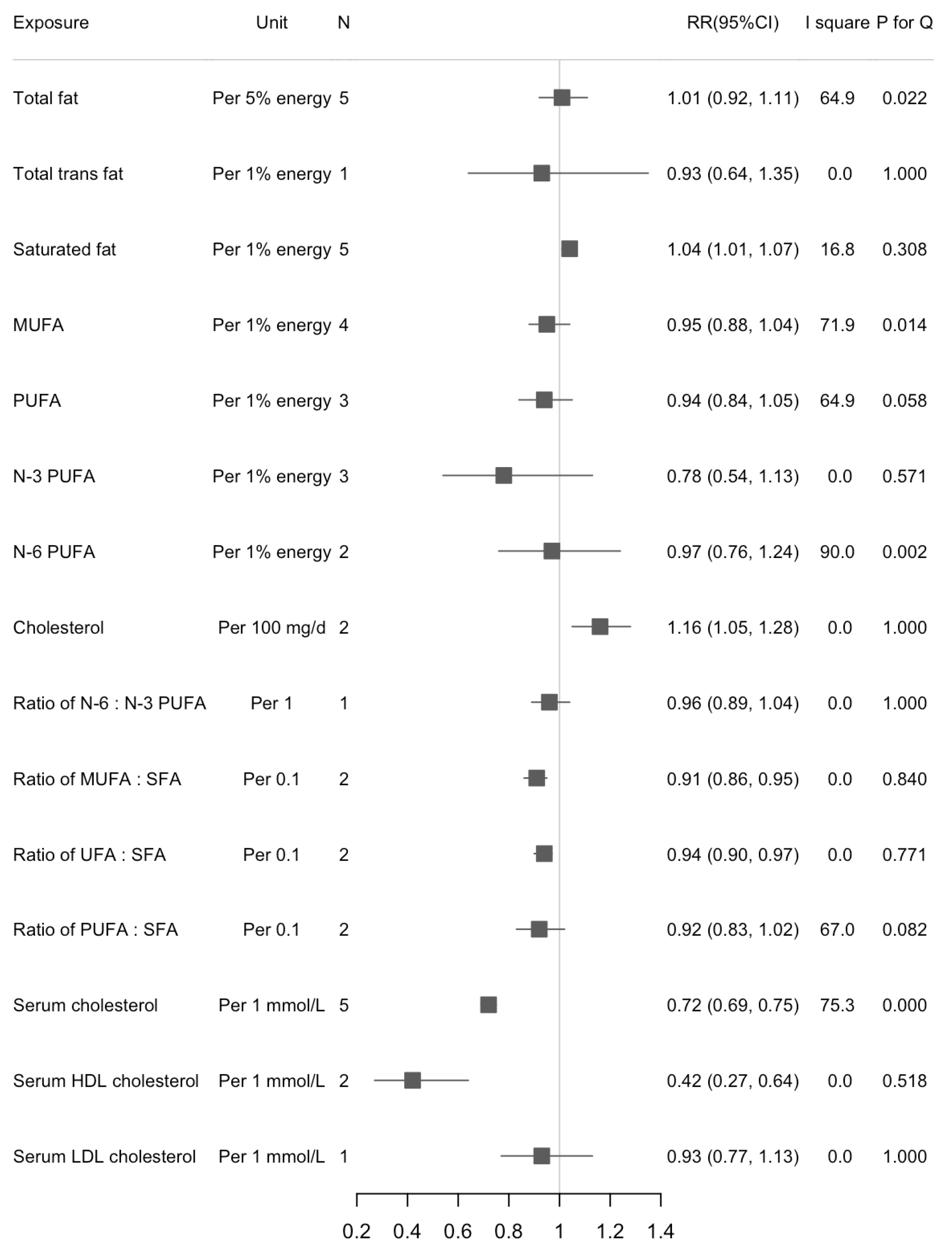
3.2. Dietary Fats and Liver Cancer Risk
3.3. Serum Cholesterol and Liver Cancer Risk
3.4. Publication Bias
4. Discussion
4.1. Principal Findings
4.2. Implications
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.D.; Hainaut, P.; Gores, G.J.; Amadou, A.; Plymoth, A.; Roberts, L.R. A global view of hepatocellular carcinoma: Trends, risk, prevention and management. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 589–604. [Google Scholar] [CrossRef] [PubMed]
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [PubMed]
- Makarova-Rusher, O.V.; Altekruse, S.F.; McNeel, T.S.; Ulahannan, S.; Duffy, A.G.; Graubard, B.I.; Greten, T.F.; McGlynn, K.A. Population attributable fractions of risk factors for hepatocellular carcinoma in the United States. Cancer 2016, 122, 1757–1765. [Google Scholar] [CrossRef] [PubMed]
- Savard, C.; Tartaglione, E.V.; Kuver, R.; Haigh, W.G.; Farrell, G.C.; Subramanian, S.; Chait, A.; Yeh, M.M.; Quinn, L.S.; Ioannou, G.N. Synergistic interaction of dietary cholesterol and dietary fat in inducing experimental steatohepatitis. Hepatology 2013, 57, 81–92. [Google Scholar] [CrossRef] [PubMed]
- Duarte-Salles, T.; Fedirko, V.; Stepien, M.; Aleksandrova, K.; Bamia, C.; Lagiou, P.; Laursen, A.S.; Hansen, L.; Overvad, K.; Tjonneland, A.; et al. Dietary fat, fat subtypes and hepatocellular carcinoma in a large European cohort. Int. J. Cancer 2015, 137, 2715–2728. [Google Scholar] [CrossRef] [PubMed]
- Koh, W.P.; Dan, Y.Y.; Goh, G.B.; Jin, A.; Wang, R.; Yuan, J.M. Dietary fatty acids and risk of hepatocellular carcinoma in the Singapore Chinese health study. Liver Int. 2016, 36, 893–901. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Sui, J.; Ma, Y.; Simon, T.G.; Petrick, J.L.; Lai, M.; McGlynn, K.A.; Campbell, P.T.; Giovannucci, E.L.; Chan, A.T.; et al. High dietary intake of vegetable or polyunsaturated fats is associated with reduced risk of hepatocellular carcinoma. Clin. Gastroenterol. Hepatol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Peters, S.A.; Singhateh, Y.; Mackay, D.; Huxley, R.R.; Woodward, M. Total cholesterol as a risk factor for coronary heart disease and stroke in women compared with men: A systematic review and meta-analysis. Atherosclerosis 2016, 248, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Silvente-Poirot, S.; Poirot, M. Cholesterol and cancer, in the balance. Science 2014, 343, 1445–1446. [Google Scholar] [CrossRef] [PubMed]
- Kitahara, C.M.; Berrington de Gonzalez, A.; Freedman, N.D.; Huxley, R.; Mok, Y.; Jee, S.H.; Samet, J.M. Total cholesterol and cancer risk in a large prospective study in Korea. J. Clin. Oncol. 2011, 29, 1592–1598. [Google Scholar] [CrossRef]
- Li, M.; Lu, J.; Fu, J.; Wan, Q.; Wang, T.; Huo, Y.; Xu, Y.; Xu, M.; Zhao, Z.; Chen, Y.; et al. The association and joint effect of serum cholesterol, glycemic status with the risk of incident cancer among middle-aged and elderly population in china cardiometabolic disease and cancer cohort (4C)-study. Am. J. Cancer Res. 2020, 10, 975–986. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 25 March 2021).
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Greenland, S.; Longnecker, M.P. Methods for trend estimation from summarized dose-response data, with applications to meta-analysis. Am. J. Epidemiol. 1992, 135, 1301–1309. [Google Scholar] [CrossRef] [PubMed]
- Orsini, N.; Li, R.; Wolk, A.; Khudyakov, P.; Spiegelman, D. Meta-analysis for linear and nonlinear dose-response relations: Examples, an evaluation of approximations, and software. Am. J. Epidemiol. 2012, 175, 66–73. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.; Lim, U.; Weinstein, S.J.; Schatzkin, A.; Hayes, R.B.; Virtamo, J.; Albanes, D. Prediagnostic total and high-density lipoprotein cholesterol and risk of cancer. Cancer Epidemiol. Biomarkers Prev. 2009, 18, 2814–2821. [Google Scholar] [CrossRef] [PubMed]
- Borena, W.; Strohmaier, S.; Lukanova, A.; Bjorge, T.; Lindkvist, B.; Hallmans, G.; Edlinger, M.; Stocks, T.; Nagel, G.; Manjer, J.; et al. Metabolic risk factors and primary liver cancer in a prospective study of 578,700 adults. Int. J. Cancer 2012, 131, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Freedman, N.D.; Cross, A.J.; McGlynn, K.A.; Abnet, C.C.; Park, Y.; Hollenbeck, A.R.; Schatzkin, A.; Everhart, J.E.; Sinha, R. Association of meat and fat intake with liver disease and hepatocellular carcinoma in the NIH-AARP cohort. J. Natl. Cancer Inst. 2010, 102, 1354–1365. [Google Scholar] [CrossRef]
- Guan, X.M.; Wu, S.L.; Yang, X.L.; Han, X.; Yang, Y.H.; Li, X.T.; Bin Waleed, K.; Yue, D.; Zhan, S.Y.; Liu, Y.; et al. Association of total cholesterol, low-density lipoprotein cholesterol, and non-high-density lipoprotein cholesterol with atherosclerotic cardiovascular disease and cancer in a Chinese male population. Int. J. Cancer 2018, 142, 1209–1217. [Google Scholar] [CrossRef]
- Ioannou, G.N.; Morrow, O.B.; Connole, M.L.; Lee, S.P. Association between dietary nutrient composition and the incidence of cirrhosis or liver cancer in the United States population. Hepatology 2009, 50, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Iso, H.; Ikeda, A.; Inoue, M.; Sato, S.; Tsugane, S.; Group, J.S. Serum cholesterol levels in relation to the incidence of cancer: The JPHC study cohorts. Int. J. Cancer 2009, 125, 2679–2686. [Google Scholar] [CrossRef] [PubMed]
- Nderitu, P.; Bosco, C.; Garmo, H.; Holmberg, L.; Malmstrom, H.; Hammar, N.; Walldius, G.; Jungner, I.; Ross, P.; Van Hemelrijck, M. The association between individual metabolic syndrome components, primary liver cancer and cirrhosis: A study in the Swedish AMORIS cohort. Int. J. Cancer 2017, 141, 1148–1160. [Google Scholar] [CrossRef] [PubMed]
- Sawada, N.; Inoue, M.; Iwasaki, M.; Sasazuki, S.; Shimazu, T.; Yamaji, T.; Takachi, R.; Tanaka, Y.; Mizokami, M.; Tsugane, S.; et al. Consumption of n-3 fatty acids and fish reduces risk of hepatocellular carcinoma. Gastroenterology 2012, 142, 1468–1475. [Google Scholar] [CrossRef] [PubMed]
- Strasak, A.M.; Pfeiffer, R.M.; Brant, L.J.; Rapp, K.; Hilbe, W.; Oberaigner, W.; Lang, S.; Borena, W.; Concin, H.; Diem, G.; et al. Time-dependent association of total serum cholesterol and cancer incidence in a cohort of 172,210 men and women: A prospective 19-year follow-up study. Ann. Oncol. 2009, 20, 1113–1120. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, D.S.; Willett, W.C.; Volek, J.S.; Neuhouser, M.L. Dietary fat: From foe to friend? Science 2018, 362, 764–770. [Google Scholar] [CrossRef] [PubMed]
- Thiebaut, A.C.; Kipnis, V.; Chang, S.C.; Subar, A.F.; Thompson, F.E.; Rosenberg, P.S.; Hollenbeck, A.R.; Leitzmann, M.; Schatzkin, A. Dietary fat and postmenopausal invasive breast cancer in the National Institutes of Health-AARP Diet and Health Study cohort. J. Natl. Cancer Inst. 2007, 99, 451–462. [Google Scholar] [CrossRef] [PubMed]
- Thiebaut, A.C.; Jiao, L.; Silverman, D.T.; Cross, A.J.; Thompson, F.E.; Subar, A.F.; Hollenbeck, A.R.; Schatzkin, A.; Stolzenberg-Solomon, R.Z. Dietary fatty acids and pancreatic cancer in the NIH-AARP diet and health study. J. Natl. Cancer Inst. 2009, 101, 1001–1011. [Google Scholar] [CrossRef] [PubMed]
- Liss, M.A.; Al-Bayati, O.; Gelfond, J.; Goros, M.; Ullevig, S.; DiGiovanni, J.; Hamilton-Reeves, J.; O’Keefe, D.; Bacich, D.; Weaver, B.; et al. Higher baseline dietary fat and fatty acid intake is associated with increased risk of incident prostate cancer in the SABOR study. Prostate Cancer Prostatic Dis. 2019, 22, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.J.; Yu, D.; Takata, Y.; Smith-Warner, S.A.; Blot, W.; White, E.; Robien, K.; Park, Y.; Xiang, Y.B.; Sinha, R.; et al. Dietary fat intake and lung cancer risk: A pooled analysis. J. Clin. Oncol. 2017, 35, 3055–3064. [Google Scholar] [CrossRef] [PubMed]
- Chapkin, R.S.; Navarro, S.L.; Hullar, M.A.J.; Lampe, J.W. Diet and Gut Microbes Act Coordinately to Enhance Programmed Cell Death and Reduce Colorectal Cancer Risk. Dig. Dis. Sci. 2020, 65, 840–851. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, S.; Li, H.; Yu, D.; Cai, H.; Gao, J.; Gao, Y.; Luu, H.; Tran, H.; Xiang, Y.B.; Zheng, W.; et al. Dietary Fatty Acids and Colorectal Cancer Risk in Men: A Report from the Shanghai Men’s Health Study and a Meta-Analysis. Int. J. Cancer 2020. [Google Scholar] [CrossRef]
- Hernandez, E.A.; Kahl, S.; Seelig, A.; Begovatz, P.; Irmler, M.; Kupriyanova, Y.; Nowotny, B.; Nowotny, P.; Herder, C.; Barosa, C.; et al. Acute dietary fat intake initiates alterations in energy metabolism and insulin resistance. J. Clin. Investig. 2017, 127, 695–708. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Otgonsuren, M.; Henry, L.; Venkatesan, C.; Mishra, A.; Erario, M.; Hunt, S. Association of nonalcoholic fatty liver disease (NAFLD) with hepatocellular carcinoma (HCC) in the United States from 2004 to 2009. Hepatology 2015, 62, 1723–1730. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, K.L.; Smith, C.I.; Schwarzenberg, S.J.; Jessurun, J.; Boldt, M.D.; Parks, E.J. Sources of fatty acids stored in liver and secreted via lipoproteins in patients with nonalcoholic fatty liver disease. J. Clin. Investig. 2005, 115, 1343–1351. [Google Scholar] [CrossRef] [PubMed]
- Phillips, C.M.; Kesse-Guyot, E.; McManus, R.; Hercberg, S.; Lairon, D.; Planells, R.; Roche, H.M. High dietary saturated fat intake accentuates obesity risk associated with the fat mass and obesity-associated gene in adults. J. Nutr. 2012, 142, 824–831. [Google Scholar] [CrossRef] [PubMed]
- Van Dam, R.M.; Willett, W.C.; Rimm, E.B.; Stampfer, M.J.; Hu, F.B. Dietary fat and meat intake in relation to risk of type 2 diabetes in men. Diabetes Care 2002, 25, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Mensink, R.P. Effects of Saturated Fatty Acids on Serum Lipids and Lipoproteins: A Systematic Review and Regression Analysis; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Li, T.T.; Li, T.H.; Peng, J.; He, B.; Liu, L.S.; Wei, D.H.; Jiang, Z.S.; Zheng, X.L.; Tang, Z.H. TM6SF2: A novel target for plasma lipid regulation. Atherosclerosis 2018, 268, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.; Zhang, J.; Mei, T.T.; Guo, H.Q.; Wei, X.H.; Zhang, W.Y.; Liu, Y.L.; Liang, S.; Fan, Z.P.; Ma, L.X.; et al. Association of TM6SF2 rs58542926 T/C gene polymorphism with hepatocellular carcinoma: A meta-analysis. BMC Cancer 2019, 19, 1128. [Google Scholar] [CrossRef]
- Chen, V.L.; Chen, Y.; Du, X.; Handelman, S.K.; Speliotes, E.K. Genetic variants that associate with cirrhosis have pleiotropic effects on human traits. Liver Int. 2020, 40, 405–415. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Keech, A.; Collins, R.; Slavin, B.; Chen, J.; Campbell, T.C.; Peto, R. Prolonged infection with hepatitis B virus and association between low blood cholesterol concentration and liver cancer. BMJ 1993, 306, 890–894. [Google Scholar] [CrossRef][Green Version]
- Welzel, T.M.; Graubard, B.I.; Zeuzem, S.; El-Serag, H.B.; Davila, J.A.; McGlynn, K.A. Metabolic syndrome increases the risk of primary liver cancer in the United States: A study in the SEER-Medicare database. Hepatology 2011, 54, 463–471. [Google Scholar] [CrossRef] [PubMed]
- Russo, M.W.; Hoofnagle, J.H.; Gu, J.; Fontana, R.J.; Barnhart, H.; Kleiner, D.E.; Chalasani, N.; Bonkovsky, H.L. Spectrum of statin hepatotoxicity: Experience of the drug-induced liver injury network. Hepatology 2014, 60, 679–686. [Google Scholar] [CrossRef]
- Islam, M.M.; Poly, T.N.; Walther, B.A.; Yang, H.C.; Jack Li, Y.C. Statin Use and the Risk of Hepatocellular Carcinoma: A Meta-Analysis of Observational Studies. Cancers 2020, 12, 671. [Google Scholar] [CrossRef] [PubMed]
- Kantor, E.D.; Rehm, C.D.; Haas, J.S.; Chan, A.T.; Giovannucci, E.L. Trends in Prescription Drug Use Among Adults in the United States From 1999–2012. JAMA 2015, 314, 1818–1831. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Zhang, X. Comments on “one-carbon metabolism-related micronutrients intake and risk for hepatocellular carcinoma: A prospective cohort study”. Int. J. Cancer 2021, 148, 252–253. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author, Year (Reference) | Country, Study Design | Baseline Years | Median Follow-Up (Years) | Age (Mean/Median, Years) | Sex | Population Exclusion | Cohort Size | Cases | Exposure | Exposure Assessment | Outcome | Outcome Assessment | Adjustment for Confounding Variables | NOS Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Li, 2020 [12] | China, 4C Cohort | 2010–2014 | 3.8 | 56.9 | Both | Participants diagnosed as cancer within 6 months from baseline were excluded. | 137,884 | 156 | LDL cholesterol | Serum level | Liver cancer | Medical records | Age, sex, BMI, family history of cancer, smoking, drinking, education status, physical activity, consumption of vegetables and fruit, insulin therapy, lipid-lowering medication, and systolic blood pressure. | 8 |
| Yang, 2020 [8] | U.S., NHS/HPFS | 1980 | 26.6 | Median = 64–68 | Both | Cancer diagnosed before baseline except for non-melanoma skin cancer were excluded. | 138,483 | 160 | Total fat, SFA, MUFA, PUFA, Trans fat, cholesterol, N3 PUFA, N6 PUFA, N6/N3 ratio, P:S ratio, M:S ratio, (M + P):S ratio | Validated FFQ | HCC | Biennial questionnaires, medical records and pathological reports confirmed by a study physician, state cancer registries, the National Death Index, death certificate | Age, sex, race, physical activity, BMI, smoking status, aspirin use, type 2 diabetes, alcohol intake, total coffee intake, and total energy intake. | 8 |
| Nderitu, 2017 [26] | Sweden, Swedish AMORIS | 1985 | 20.03 | 44 | Both | Participants with benign liver tumors, primary liver cancer or cirrhosis at baseline were excluded. | 509,436 | 766 | Cholesterol, HDL cholesterol, LDL cholesterol | Serum level | Liver cancer | Linkage with Swedish national registries | Age, sex, SES, triglycerides, cholesterol, raised glucose, diabetic status and history of liver disease (Cholesterol not adjusted for total cholesterol; HDL-C, LDL-C not adjusted for triglycerides). | 7 |
| Guan, 2017 [23] | China, Kailuan Cohort Study | 2006 | approximately 8 years | 51.05 | Male | Participants with history of cancer and cardiovascular disease were excluded. | 68,759 | 205 | Cholesterol, LDL cholesterol | Serum level | Liver cancer | Medical insurance, hospital records/death confirmed by death certificates | Age, cigarette smoking, alcohol consumption, physical activity, hypertension, diabetes mellitus, BMI. | 7 |
| Koh, 2016 [7] | Singapore, SCHS | 1993 | 14 | 56.4 | Both | Individuals who had history of invasive cancer at baseline (except non-melanoma skin cancer) were excluded. | 60,298 | 488 | Total fat, SFA, MUFA, N3 PUFA, N6 PUFA, N6/N3 ratio | Validated FFQ | HCC | Record linkage analysis of the cohort database with databases of the population-based Singapore Cancer Registry and Singapore Registry of Births and Deaths | Age, sex, dialect, year of interview, educational level, BMI, smoking status, alcohol use, coffee drinking status, baseline history of self-reported diabetes, total energy and dietary protein. Fat subtype intakes are mutually adjusted. | 9 |
| Duarte-Salles, 2015 [6] | Europe, EPIC | 1992 | 11.4 | 51.2 | Both | Generally healthy population across centers. | 477,206 | 191 | Total fat, SFA, MUFA, PUFA, P:S ratio, M:S ratio, (P + M):S ratio | Validated FFQ and 24-h dietary recall | HCC | Record linkage with cancer registries/a combination of methods. | Baseline alcohol intake and non-alcohol total energy intake, sex-specific physical activity level, BMI, smoking status, lifetime alcohol intake pattern, coffee intake, and intake of dietary fiber. Fat subtype intakes are mutually adjusted. | 9 |
| Sawada, 2012 [27] | Japan, JPHC | 1990 | 11.2 | 40–69 | Both | Subjects who had been diagnosed with cancer before the starting point were excluded. | 90,296 | 398 | N3 PUFA | Validated FFQ | HCC | Data linkage of major local hospitals with cancer registries/death certificate | Age, area, sex, smoking status, alcohol frequency, BMI, past history of diabetes mellitus, intake of coffee, soy foods, vegetables, vegetable oil, protein, and iron. | 9 |
| Borena, 2011 [21] | Europe, Me-Can cohort | 2006 | 12 | 44 | Both | Malignant cancer before the health examination were excluded. | 578,700 | 266 | Cholesterol | Serum level | Liver Cancer | National cancer registries | Age, smoking status, cohort, birth year and sex, BMI. | 8 |
| Kitahara, 2011 [11] | Korea, KCPS | 1992–1995 | 12.7 | 44.9 (men), 49.3 (women) | Both | Participants who reported having cardiovascular disease, cancer, liver disease, or a respiratory disease at or before the initial visit, or who had extremely low levels of BMI, with missing or implausibly high or low total cholesterol levels were excluded. | 1,189,719 | 10,161 | Cholesterol | Serum level | Liver cancer | Medical records | Cigarette smoking, alcohol drinking, BMI, fasting serum glucose, hypertension, and physical activity. | 9 |
| Freedman, 2010 [22] | U.S., NIH-AARP | 1995 | NR | Median = 62.6 | Both | Participants who developed cancer or died before their questionnaires were scanned were excluded. | 495,006 | 338 | Total fat, SFA, MUFA, PUFA | Validated FFQ | HCC | State cancer registries | Age, sex, alcohol, BMI, cigarette smoking, diabetes, education, fruit intake, vegetable intake, marital status, race and/or ethnicity, total energy from nonalcohol sources, usual physical activity throughout the day, and vigorous physical activity. | 7 |
| Ahn, 2009 [20] | U.S., ATBC | 1985 | 14.9 | 50–69 | Male | Participants with history of cancer other than nonmelanoma skin cancer or carcinoma in situ, severe angina pectoris, chronic renal insufficiency, liver cirrhosis, chronic alcoholism, anticoagulant therapy, other medical problems that might have limited long-term participation were excluded. | 29,093 | 191 | Cholesterol, HDL cholesterol | Serum level | Liver cancer | Medical records | Age, intervention, level of education, systolic blood pressure, BMI, physical activity, duration of smoking, number of cigarettes smoked per day, saturates fat intake, polyunsaturated fat intake, total calorie, alcohol consumption, and serum HDL cholesterol. | 9 |
| Ioannou, 2009 [24] | U.S., NHANES | 1971 | 13.3 | 48.8 | Both | Participants who reported at baseline ever being told by a physician that they had jaundice, hepatitis, or a malignant tumor, who had hepatomegaly or splenomegaly at baseline examination, or whose level of serum albumin was less than 3 g/dL were excluded. | 9221 | 123 | Total fat, SFA, cholesterol | 24-h dietary recall questionnaire | Cirrhosis and liver cancer | Hospitalization records death certificates | Energy from other macronutrients, daily alcohol consumption, coffee or tea, gender, race, age, education, region, diabetes, BMI, and subscapular-to-triceps skinfold ratio. | 6 |
| Iso, 2009 [25] | Japan, JPHC | 1990 | 12.4 | 40–69 | Both | Participants with history of cardiovascular disease were excluded. | 33,368 | 125 | Cholesterol | Serum level | Liver cancer | Medical records and/or cancer registries | Age, BMI, pack years of smoking, ethanol intake, hypertension, diabetes, hyperlipidemia medication use, total vegetable intake, coffee intake and public health center. | 9 |
| Strasak, 2009 [28] | Australia, VHM and PP | 1985 | 11.6 | 41.6 | Both | Healthy participants, free of cancer at baseline. | 172,210 | 2322 | Cholesterol | Fasting blood sample | Malignant neoplasms of digestive organs | Vorarlberg Cancer Registry | Age, BMI, smoking status, occupational status, and year of entry into the cohort. | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, L.; Deng, C.; Lin, Z.; Giovannucci, E.; Zhang, X. Dietary Fats, Serum Cholesterol and Liver Cancer Risk: A Systematic Review and Meta-Analysis of Prospective Studies. Cancers 2021, 13, 1580. https://doi.org/10.3390/cancers13071580
Zhao L, Deng C, Lin Z, Giovannucci E, Zhang X. Dietary Fats, Serum Cholesterol and Liver Cancer Risk: A Systematic Review and Meta-Analysis of Prospective Studies. Cancers. 2021; 13(7):1580. https://doi.org/10.3390/cancers13071580
Chicago/Turabian StyleZhao, Longgang, Chuanjie Deng, Zijin Lin, Edward Giovannucci, and Xuehong Zhang. 2021. "Dietary Fats, Serum Cholesterol and Liver Cancer Risk: A Systematic Review and Meta-Analysis of Prospective Studies" Cancers 13, no. 7: 1580. https://doi.org/10.3390/cancers13071580
APA StyleZhao, L., Deng, C., Lin, Z., Giovannucci, E., & Zhang, X. (2021). Dietary Fats, Serum Cholesterol and Liver Cancer Risk: A Systematic Review and Meta-Analysis of Prospective Studies. Cancers, 13(7), 1580. https://doi.org/10.3390/cancers13071580