
Predictors of Survival in Subtotally Resected WHO Grade I Skull Base Meningiomas




Abstract
Simple Summary
Abstract
1. Introduction
2. Results
2.1. Overall Characteristics
2.2. Clinical Outcomes
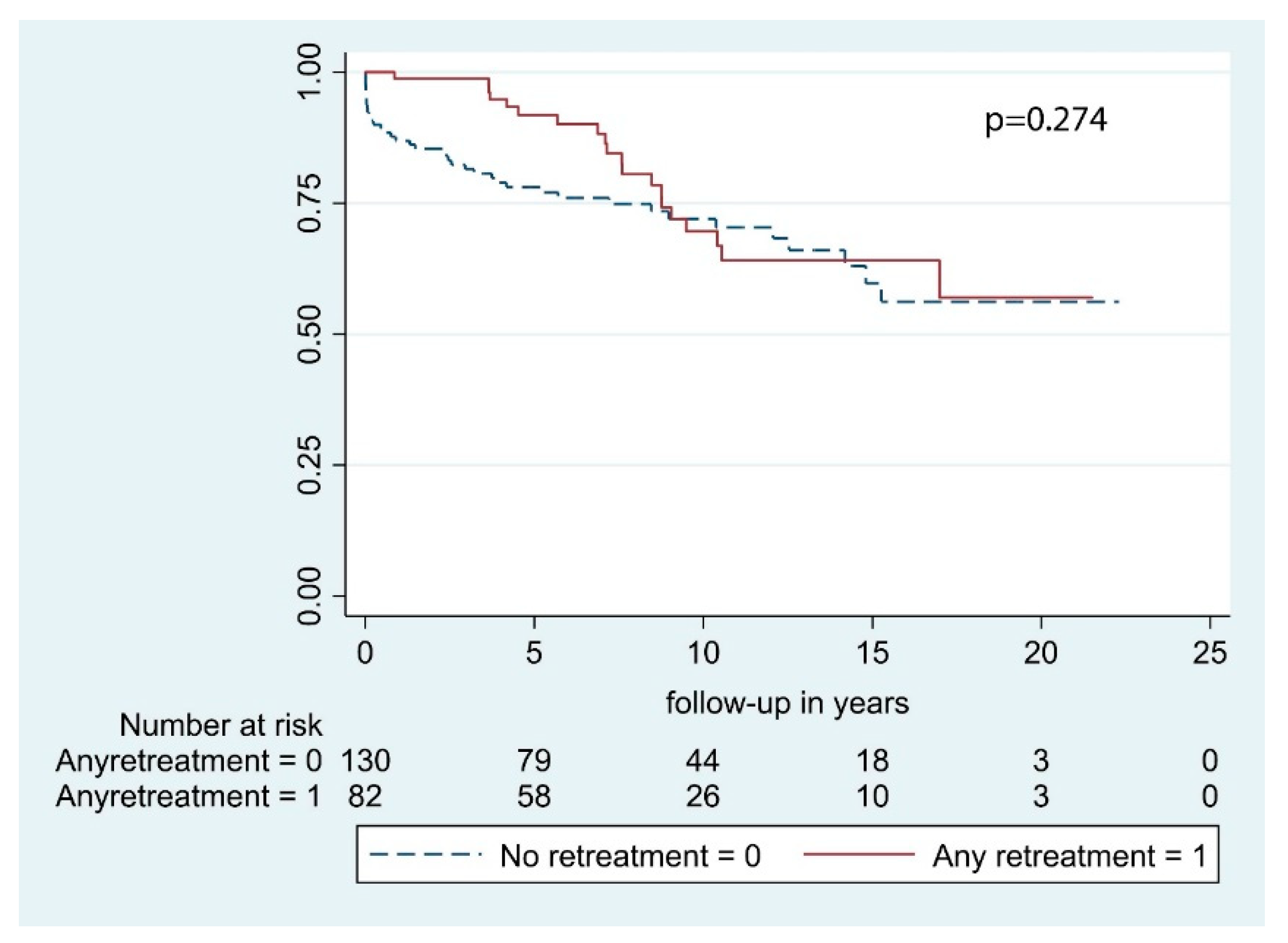
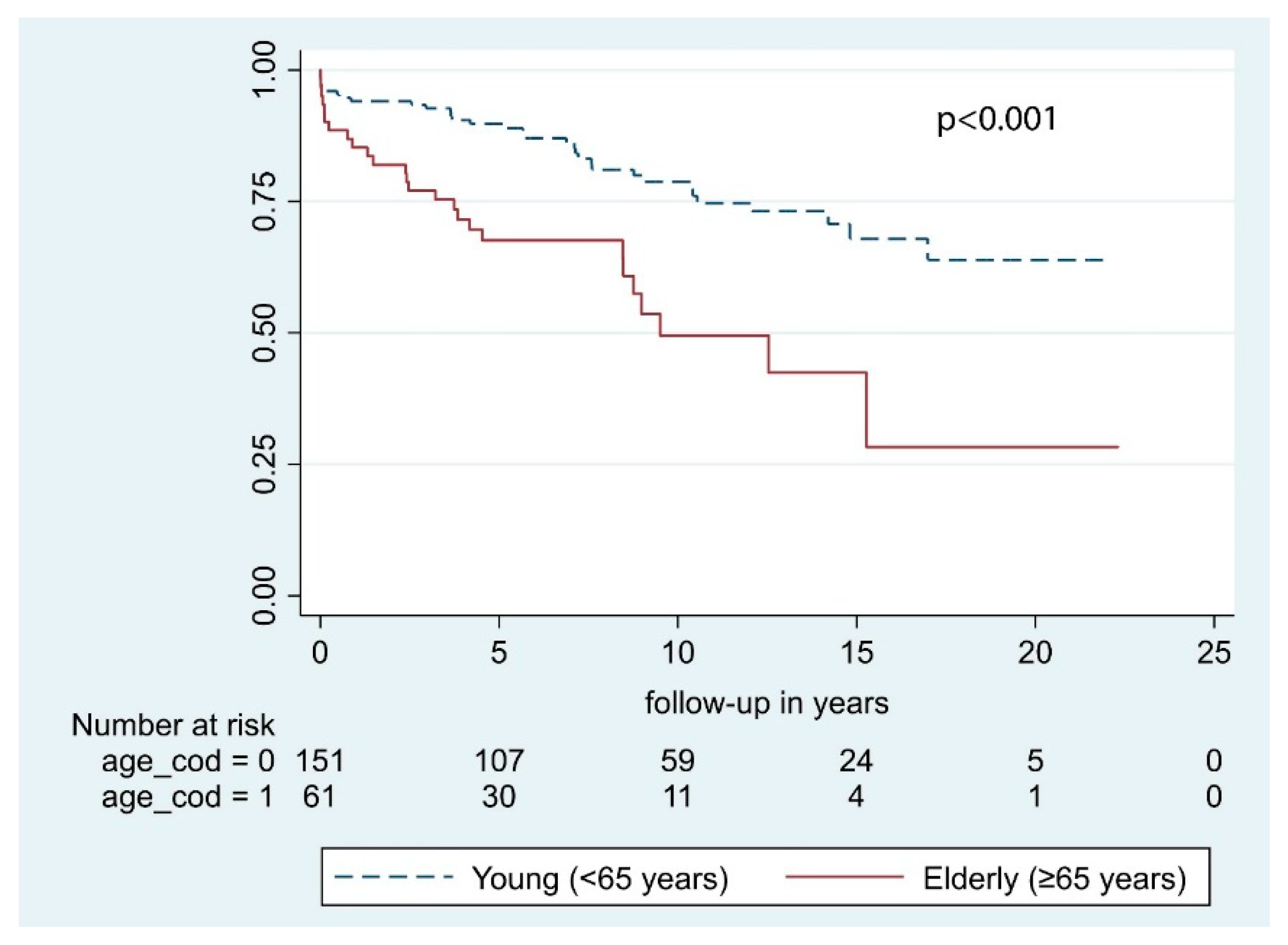
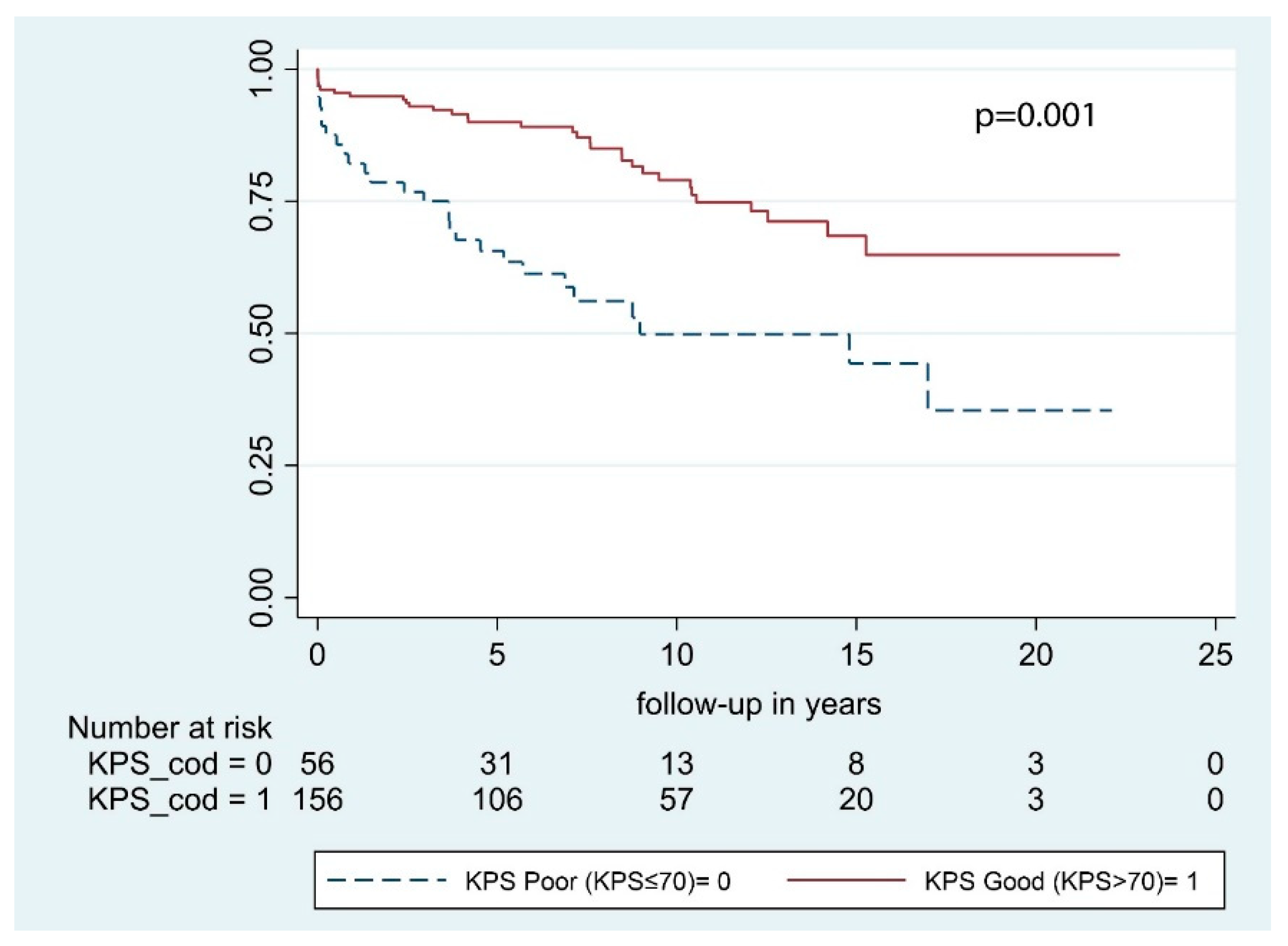
2.3. Predictors of Overall Survival
3. Discussion
3.1. Clinical Predictors of Survival
3.2. Clinical Outcomes
3.3. Tumor Location
3.4. Retreatment and Radiation Therapy
4. Materials and Methods
4.1. Patient Cohort
4.2. Ethics
4.3. Statistics
5. Conclusions
Strengths and Limitations of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Meling, T.R.; Da Broi, M.; Scheie, D.; Helseth, E. Meningiomas: Skull base versus non-skull base. Neurosurg. Rev. 2019, 42, 163–173. [Google Scholar] [CrossRef]
- Simpson, D. The recurrence of intracranial meningiomas after surgical treatment. J. Neurol. Neurosurg. Psychiatry 1957, 20, 22–39. [Google Scholar] [CrossRef] [PubMed]
- Hasseleid, B.F.; Meling, T.R.; Ronning, P.; Scheie, D.; Helseth, E. Surgery for convexity meningioma: Simpson Grade I resection as the goal: Clinical article. J. Neurosurg. 2012, 117, 999–1006. [Google Scholar] [CrossRef] [PubMed]
- Corniola, M.V.; Lemee, J.M.; Da Broi, M.; Joswig, H.; Schaller, K.; Helseth, E.; Meling, T.R. Posterior fossa meningiomas: Perioperative predictors of extent of resection, overall survival and progression-free survival. Acta Neurochir. 2019, 161, 1003–1011. [Google Scholar] [CrossRef]
- Goldbrunner, R.; Minniti, G.; Preusser, M.; Jenkinson, M.D.; Sallabanda, K.; Houdart, E.; von Deimling, A.; Stavrinou, P.; Lefranc, F.; Lund-Johansen, M.; et al. EANO guidelines for the diagnosis and treatment of meningiomas. Lancet Oncol. 2016, 17, e383–e391. [Google Scholar] [CrossRef]
- Konglund, A.; Rogne, S.G.; Lund-Johansen, M.; Scheie, D.; Helseth, E.; Meling, T.R. Outcome following surgery for intracranial meningiomas in the aging. Acta Neurol. Scand. 2012, 127, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Lemee, J.M.; Corniola, M.V.; Da Broi, M.; Joswig, H.; Scheie, D.; Schaller, K.; Helseth, E.; Meling, T.R. Extent of Resection in Meningioma: Predictive Factors and Clinical Implications. Sci. Rep. 2019, 9, 5944. [Google Scholar] [CrossRef] [PubMed]
- Meling, T.R.; Da Broi, M.; Scheie, D.; Helseth, E.; Smoll, N.R. Meningioma Surgery-Are We Making Progress? World Neurosurg. 2019, 125, e205–e213. [Google Scholar] [CrossRef]
- Odegaard, K.M.; Helseth, E.; Meling, T.R. Intraventricular meningiomas: A consecutive series of 22 patients and literature review. Neurosurg. Rev. 2013, 36, 57–64, discussion 64. [Google Scholar] [CrossRef]
- Konglund, A.; Rogne, S.G.; Helseth, E.; Meling, T.R. Meningioma surgery in the very old-validating prognostic scoring systems. Acta Neurochir. 2013, 155, 2263–2271, discussion 2271. [Google Scholar] [CrossRef]
- Meling, T.R.; Da Broi, M.; Scheie, D.; Helseth, E. Skull base versus non-skull base meningioma surgery in the elderly. Neurosurg. Rev. 2019, 42, 961–972. [Google Scholar] [CrossRef]
- Combs, S.E.; Ganswindt, U.; Foote, R.L.; Kondziolka, D.; Tonn, J.C. State-of-the-art treatment alternatives for base of skull meningiomas: Complementing and controversial indications for neurosurgery, stereotactic and robotic based radiosurgery or modern fractionated radiation techniques. Radiat. Oncol. 2013, 7, 226. [Google Scholar] [CrossRef] [PubMed]
- Faramand, A.; Kano, H.; Niranjan, A.; Johnson, S.A.; Hassib, M.; Park, K.J.; Arai, Y.; Flickinger, J.C.; Lunsford, L.D. Cranial nerve outcomes after primary stereotactic radiosurgery for symptomatic skull base meningiomas. J. Neurooncol. 2018, 139, 341–348. [Google Scholar] [CrossRef]
- Komotar, R.J.; Starke, R.M.; Raper, D.M.; Anand, V.K.; Schwartz, T.H. Endoscopic endonasal versus open transcranial resection of anterior midline skull base meningiomas. World Neurosurg. 2012, 77, 713–724. [Google Scholar] [CrossRef] [PubMed]
- Schneider, M.; Schuss, P.; Guresir, A.; Borger, V.; Vatter, H.; Guresir, E. Surgery for posterior fossa meningioma: Elevated postoperative cranial nerve morbidity discards aggressive tumor resection policy. Neurosurg. Rev. 2020. [Google Scholar] [CrossRef] [PubMed]
- Schneider, M.; Schuss, P.; Guresir, A.; Wach, J.; Hamed, M.; Vatter, H.; Guresir, E. Cranial Nerve Outcomes After Surgery for Frontal Skull Base Meningiomas: The Eternal Quest of the Maximum-Safe Resection with the Lowest Morbidity. World Neurosurg. 2019, 125, e790–e796. [Google Scholar] [CrossRef] [PubMed]
- Goldsmith, B.J.; Wara, W.M.; Wilson, C.B.; Larson, D.A. Postoperative irradiation for subtotally resected meningiomas. A retrospective analysis of 140 patients treated from 1967 to 1990. J. Neurosurg. 1994, 80, 195–201. [Google Scholar] [CrossRef]
- Mathiesen, T.; Lindquist, C.; Kihlstrom, L.; Karlsson, B. Recurrence of cranial base meningiomas. Neurosurgery 1996, 39, 2–7, discussion 8–9. [Google Scholar] [CrossRef]
- Materi, J.; Mampre, D.; Ehresman, J.; Rincon-Torroella, J.; Chaichana, K.L. Predictors of recurrence and high growth rate of residual meningiomas after subtotal resection. J. Neurosurg. 2020, 1–7. [Google Scholar] [CrossRef]
- Worldometer.info Worldometer. Available online: www.worldometer.info (accessed on 20 March 2020).
- Brokinkel, B.; Holling, M.; Spille, D.C.; Hess, K.; Sauerland, C.; Bleimuller, C.; Paulus, W.; Wolfer, J.; Stummer, W. Surgery for meningioma in the elderly and long-term survival: Comparison with an age- and sex-matched general population and with younger patients. J. Neurosurg. 2016, 126, 1201–1211. [Google Scholar] [CrossRef]
- Cahill, K.S.; Claus, E.B. Treatment and survival of patients with nonmalignant intracranial meningioma: Results from the Surveillance, Epidemiology, and End Results Program of the National Cancer Institute. Clinical article. J. Neurosurg. 2011, 115, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Park, J.S.; Sade, B.; Oya, S.; Kim, C.G.; Lee, J.H. The influence of age on the histological grading of meningiomas. Neurosurg. Rev. 2014, 37, 425–429, discussion 429. [Google Scholar] [CrossRef] [PubMed]
- Kallio, M.; Sankila, R.; Hakulinen, T.; Jaaskelainen, J. Factors affecting operative and excess long-term mortality in 935 patients with intracranial meningioma. Neurosurgery 1992, 31, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Gerlach, R.; Raabe, A.; Scharrer, I.; Meixensberger, J.; Seifert, V. Post-operative hematoma after surgery for intracranial meningiomas: Causes, avoidable risk factors and clinical outcome. Neurol. Res. 2014, 26, 61–66. [Google Scholar] [CrossRef]
- Lassen, B.; Helseth, E.; Ronning, P.; Scheie, D.; Johannesen, T.B.; Maehlen, J.; Langmoen, I.A.; Meling, T.R. Surgical mortality at 30 days and complications leading to recraniotomy in 2630 consecutive craniotomies for intracranial tumors. Neurosurgery 2011, 68, 1259–1268, discussion 1259–1268. [Google Scholar] [CrossRef]
- Roser, F.; Ebner, F.H.; Ritz, R.; Samii, M.; Tatagiba, M.S.; Nakamura, M. Management of skull based meningiomas in the elderly patient. J. Clin. Neurosci. 2007, 14, 224–228. [Google Scholar] [CrossRef]
- Kressner, M.; Arlt, F.; Riepl, W.; Meixensberger, J. Prognostic factors of microsurgical treatment of intracranial meningiomas-A multivariate analysis. PLoS ONE 2018, 13, e0202520. [Google Scholar] [CrossRef]
- Van Alkemade, H.; de Leau, M.; Dieleman, E.M.; Kardaun, J.W.; van Os, R.; Vandertop, W.P.; van Furth, W.R.; Stalpers, L.J. Impaired survival and long-term neurological problems in benign meningioma. Neuro Oncol. 2012, 14, 658–666. [Google Scholar] [CrossRef] [PubMed]
- Caroli, M.; Locatelli, M.; Prada, F.; Beretta, F.; Martinelli-Boneschi, F.; Campanella, R.; Arienta, C. Surgery for intracranial meningiomas in the elderly: A clinical-radiological grading system as a predictor of outcome. J. Neurosurg. 2005, 102, 290–294. [Google Scholar] [CrossRef]
- Cohen-Inbar, O.; Soustiel, J.F.; Zaaroor, M. Meningiomas in the elderly, the surgical benefit and a new scoring system. Acta Neurochir. 2009, 152, 87–97, discussion 97. [Google Scholar] [CrossRef]
- Cohen-Inbar, O.; Sviri, G.E.; Soustiel, J.F.; Zaaroor, M. The Geriatric Scoring System (GSS) in meningioma patients--validation. Acta Neurochir. 2011, 153, 1501–1508, discussion 1508. [Google Scholar] [CrossRef]
- Samii, M.; Klekamp, J.; Carvalho, G. Surgical results for meningiomas of the craniocervical junction. Neurosurgery 1996, 39, 1086–1094, discussion 1085–1094. [Google Scholar] [CrossRef]
- Levine, Z.T.; Buchanan, R.I.; Sekhar, L.N.; Rosen, C.L.; Wright, D.C. Proposed grading system to predict the extent of resection and outcomes for cranial base meningiomas. Neurosurgery 1999, 45, 221–230. [Google Scholar] [CrossRef]
- Mansouri, A.; Klironomos, G.; Taslimi, S.; Kilian, A.; Gentili, F.; Khan, O.H.; Aldape, K.; Zadeh, G. Surgically resected skull base meningiomas demonstrate a divergent postoperative recurrence pattern compared with non-skull base meningiomas. J. Neurosurg. 2016, 125, 431–440. [Google Scholar] [CrossRef] [PubMed]
- Roberti F, Sekhar LN, Kalavakonda C, Wright DC Posterior fossa meningiomas-surgical experience in 161 cases. Surg. Neurol. 2011, 56, 8–20, discussion 20–21.
- Gallagher, M.J.; Jenkinson, M.D.; Brodbelt, A.R.; Mills, S.J.; Chavredakis, E. WHO grade 1 meningioma recurrence: Are location and Simpson grade still relevant? Clin. Neurol. Neurosurg. 2016, 141, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Ildan, F.; Erman, T.; Gocer, A.I.; Tuna, M.; Bagdatoglu, H.; Cetinalp, E.; Burgut, R. Predicting the probability of meningioma recurrence in the preoperative and early postoperative period: A multivariate analysis in the midterm follow-up. Skull Base 2007, 17, 157–171. [Google Scholar] [CrossRef] [PubMed]
- Kollová, A.; Liscák, R.; Novotný, J.; Vladyka, V., Jr.; Simonová, G.; Janousková, L. Gamma Knife surgery for benign meningioma. J. Neurosurg. 2007, 107, 325–336. [Google Scholar] [CrossRef] [PubMed]
- Kondziolka, D.; Mathieu, D.; Lunsford, L.D.; Martin, J.J.; Madhok, R.; Niranjan, A.; Flickinger, J.C. Radiosurgery as definitive management of intracranial meningiomas. Neurosurgery 2008, 62, 53–58, discussion 58–60. [Google Scholar] [CrossRef]
- Stafford, S.L.; Pollock, B.E.; Foote, R.L.; Link, M.J.; Gorman, D.A.; Schomberg, P.J.; Leavitt, J.A. Meningioma radiosurgery: Tumor control, outcomes, and complications among 190 consecutive patients. Neurosurgery 2001, 49, 1029–1037, discussion 1028–1037. [Google Scholar] [CrossRef]
- Ostrom, Q.T.; Gittleman, H.; Xu, J.; Kromer, C.; Wolinsky, Y.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2009-2013. Neuro Oncol. 2016, 18, v1–v75. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [PubMed]
- Landriel Ibanez, F.A.; Hem, S.; Ajler, P.; Vecchi, E.; Ciraolo, C.; Baccanelli, M.; Tramontano, R.; Knezevich, F.; Carrizo, A. A new classification of complications in neurosurgery. World Neurosurg. 2011, 75, 709–715, discussion 604–711. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | n | % | |
|---|---|---|---|
| 212 | 100 | ||
| Sex | |||
| Male | 46 | 21.7 | |
| Female | 166 | 78.3 | |
| Age at primary surgery | |||
| <40 years | 24 | 11.3 | |
| 40–50 years | 35 | 16.5 | |
| 50–60 years | 64 | 30.2 | |
| 60–70 years | 51 | 24.1 | |
| ≥70 years | 38 | 17.9 | |
| Preoperative KPS | |||
| 100 | 4 | 1.9 | |
| 90 | 72 | 34.0 | |
| 80 | 80 | 37.7 | |
| ≤70 | 56 | 26.4 | |
| Presenting symptoms | |||
| Seizure | 28 | 13.2 | |
| Raised ICP | 66 | 31.1 | |
| Neurological deficits | 154 | 72.6 | |
| Asymptomatic | 3 | 1.4 | |
| Location | |||
| Supratentorial | 3 | 1.4 | |
| Infratentorial | 21 | 9.9 | |
| Tuberculum sellae/suprasellar | 30 | 14.2 | |
| Cavernous sinus | 14 | 6.6 | |
| Petroclival | 27 | 12.7 | |
| Intraorbital | 13 | 6.1 | |
| Olfactory groove | 10 | 4.7 | |
| Middle fossa/Cavum Meckeli | 7 | 3.3 | |
| Medial sphenoid wing | 50 | 23.6 | |
| Lateral sphenoid wing | 10 | 4.7 | |
| Craniocervical junction/Foramen magnum | 6 | 2.8 | |
| CP angle | 21 | 9.9 | |
| Clinical outcome | n | % | |
|---|---|---|---|
| Surgical outcome | |||
| Postop hematomas | 9/259 | 3.5 | |
| Postop infections | 2/259 | 0.8 | |
| 30-day mortality | 10/212 | 4.7 | |
| Neurological outcome at final visit | |||
| Improved-unchanged | 122 | 70.1 | |
| Worsened | 52 | 29.9 | |
| Retreatment rate | |||
| 1-year | 34 | 16.0 | |
| 2-year | 49 | 23.1 | |
| 3-year | 57 | 26.9 | |
| 5-year | 71 | 33.5 | |
| 10-year | 80 | 37.7 | |
| 15-year | 81 | 38.2 | |
| Variable | Univariate Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| HR (95%CI) | p Value | HR (95%CI) | p Value | |
| Sex M vs. F | 1.70 (0.99–2.93) | 0.052 | 1.24 (0.71–2.17) | 0.446 |
| Age at primary surgery years | 1.05 (1.03–1.08) | <0.001 | 1.05 (1.02–1.07) | <0.001 |
| Preoperative KPS Good vs. Poor | 0.35 (0.21–0.59) | <0.001 | 0.42 (0.24–0.71) | 0.001 |
| Neurological deficits Yes vs. No | 1.49 (0.80–2.77) | 0.199 | - | - |
| Location Posterior fossa vs. fronto-basal | 0.89 (0.52–1.53) | 0.692 | - | - |
| Bony invasion Yes vs. No | 0.61 (0.31–1.18) | 0.143 | - | - |
| Retreatment Any retreatment vs. No retreatment | 0.74 (0.43–1.26) | 0.274 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Da Broi, M.; Borrelli, P.; Meling, T.R. Predictors of Survival in Subtotally Resected WHO Grade I Skull Base Meningiomas. Cancers 2021, 13, 1451. https://doi.org/10.3390/cancers13061451
Da Broi M, Borrelli P, Meling TR. Predictors of Survival in Subtotally Resected WHO Grade I Skull Base Meningiomas. Cancers. 2021; 13(6):1451. https://doi.org/10.3390/cancers13061451
Chicago/Turabian StyleDa Broi, Michele, Paola Borrelli, and Torstein R. Meling. 2021. "Predictors of Survival in Subtotally Resected WHO Grade I Skull Base Meningiomas" Cancers 13, no. 6: 1451. https://doi.org/10.3390/cancers13061451
APA StyleDa Broi, M., Borrelli, P., & Meling, T. R. (2021). Predictors of Survival in Subtotally Resected WHO Grade I Skull Base Meningiomas. Cancers, 13(6), 1451. https://doi.org/10.3390/cancers13061451