
The Prognostic Role of LRIG Proteins in Endometrial Cancer

 , , and
, , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Study Population and Analytic Cohort
4.2. Endometrial Cancer Biopsies and Other Biologic Samples
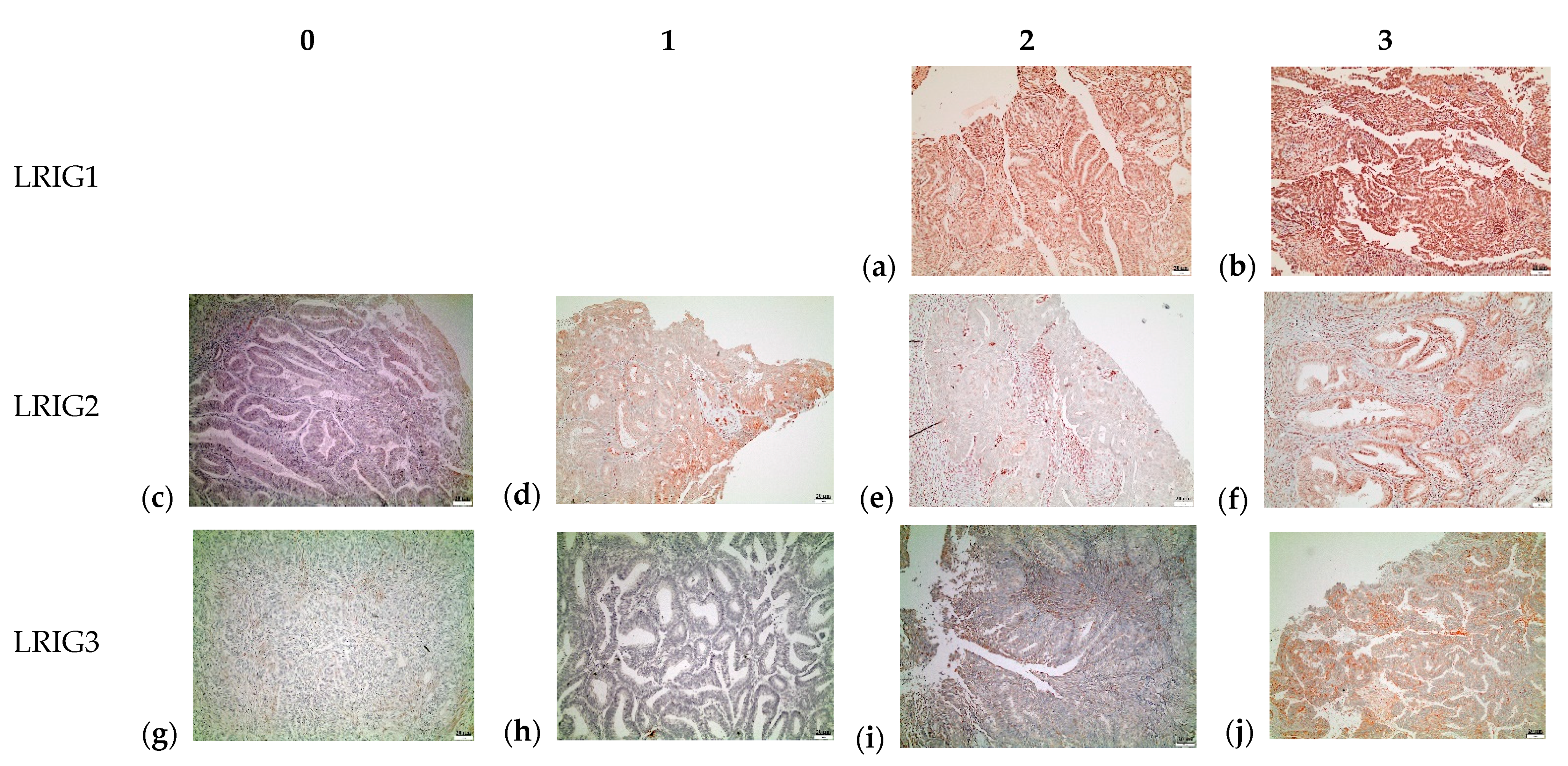
4.3. Immunohistochemistry
4.4. Evaluation and Classification of Immunostaining
4.5. Medical Records
4.6. Ethics Statement
4.7. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Bergman, O.F.L.; Hont, G.; Johansson, E.; Ljungman, P.; Munck-Wikland, E.; Nahi, H.; Zedenius, J. Cancer i Siffror 2018—Populärvetenskapliga Fakta om Cancer; Socialstyrelsen och Cancerfonden: Stockholm, Sweden, 2018; p. 70. [Google Scholar]
- Kurman, R.J.; Carcangiu, M.L.; Herrington, C.S.; Young, R.H. WHO Classification of Tumours of Female Reproductive Organs, 4th ed.; International Agency for Research on Cancer: Lyon, France, 2014; Volume 6. [Google Scholar]
- Felix, A.S.; Weissfeld, J.L.; Stone, R.A.; Bowser, R.; Chivukula, M.; Edwards, R.P.; Linkov, F. Factors associated with Type I and Type II endometrial cancer. Cancer Causes Control 2010, 21, 1851–1856. [Google Scholar] [CrossRef]
- Bhatla, N.; Denny, L. FIGO Cancer Report 2018. Int. J. Gynaecol. Obstet. 2018, 143 (Suppl. S2), 2–3. [Google Scholar] [CrossRef]
- Colombo, N.; Creutzberg, C.; Amant, F.; Bosse, T.; Gonzalez-Martin, A.; Ledermann, J.; Marth, C.; Nout, R.; Querleu, D.; Mirza, M.R.; et al. ESMO-ESGO-ESTRO Consensus Conference on Endometrial Cancer: Diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, 16–41. [Google Scholar] [CrossRef]
- Regionala Cancercentrum i Samverkan. Nationellt Vårdprogram Livmoderkroppscancer. Available online: https://www.cancercentrum.se/samverkan/cancerdiagnoser/gynekologi/livmoderkropp/vardprogram/ (accessed on 20 August 2020).
- Nastic, D.; Shanwell, E.; Wallin, K.L.; Valla, M.; Masback, A.; Mateoiu, C.; Lidang, M.; Liakka, A.; Lappi-Blanco, E.; Grove, A.; et al. A Selective Biomarker Panel Increases the Reproducibility and the Accuracy in Endometrial Biopsy Diagnosis. Int. J. Gynecol. Pathol. 2017. [Google Scholar] [CrossRef] [PubMed]
- May, K.; Bryant, A.; Dickinson, H.O.; Kehoe, S.; Morrison, J. Lymphadenectomy for the management of endometrial cancer. Cochrane Database Syst. Rev. 2010, CD007585. [Google Scholar] [CrossRef]
- Matias-Guiu, X.; Prat, J. Molecular pathology of endometrial carcinoma. Histopathology 2013, 62, 111–123. [Google Scholar] [CrossRef] [PubMed]
- Hedman, H.; Henriksson, R. LRIG inhibitors of growth factor signalling—Double-edged swords in human cancer? Eur. J. Cancer 2007, 43, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Human Protein Atlas. Available online: https://www.proteinatlas.org/ (accessed on 20 August 2020).
- Nilsson, J.; Vallbo, C.; Guo, D.; Golovleva, I.; Hallberg, B.; Henriksson, R.; Hedman, H. Cloning, characterization, and expression of human LIG1. Biochem. Biophys. Res. Commun. 2001, 284, 1155–1161. [Google Scholar] [CrossRef] [PubMed]
- Holmlund, C.; Nilsson, J.; Guo, D.; Starefeldt, A.; Golovleva, I.; Henriksson, R.; Hedman, H. Characterization and tissue-specific expression of human LRIG2. Gene 2004, 332, 35–43. [Google Scholar] [CrossRef]
- Guo, D.; Holmlund, C.; Henriksson, R.; Hedman, H. The LRIG gene family has three vertebrate paralogs widely expressed in human and mouse tissues and a homolog in Ascidiacea. Genomics 2004, 84, 157–165. [Google Scholar] [CrossRef]
- Nilsson, J.; Starefeldt, A.; Henriksson, R.; Hedman, H. LRIG1 protein in human cells and tissues. Cell Tissue Res. 2003, 312, 65–71. [Google Scholar] [CrossRef]
- Knuutila, S.; Aalto, Y.; Autio, K.; Bjorkqvist, A.M.; El-Rifai, W.; Hemmer, S.; Huhta, T.; Kettunen, E.; Kiuru-Kuhlefelt, S.; Larramendy, M.L.; et al. DNA copy number losses in human neoplasms. Am. J. Pathol. 1999, 155, 683–694. [Google Scholar] [CrossRef]
- Gur, G.; Rubin, C.; Katz, M.; Amit, I.; Citri, A.; Nilsson, J.; Amariglio, N.; Henriksson, R.; Rechavi, G.; Hedman, H.; et al. LRIG1 restricts growth factor signaling by enhancing receptor ubiquitylation and degradation. EMBO J. 2004, 23, 3270–3281. [Google Scholar] [CrossRef]
- Laederich, M.B.; Funes-Duran, M.; Yen, L.; Ingalla, E.; Wu, X.; Carraway, K.L., 3rd; Sweeney, C. The leucine-rich repeat protein LRIG1 is a negative regulator of ErbB family receptor tyrosine kinases. J. Biol. Chem. 2004, 279, 47050–47056. [Google Scholar] [CrossRef]
- Hedman, H.; Lindstrom, A.K.; Tot, T.; Stendahl, U.; Henriksson, R.; Hellberg, D. LRIG2 in contrast to LRIG1 predicts poor survival in early-stage squamous cell carcinoma of the uterine cervix. Acta Oncol. 2010, 49, 812–815. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.K.; Chen, H.; Mao, F.; Xiao, Q.G.; Xie, R.F.; Lei, T. Downregulation of LRIG2 expression inhibits angiogenesis of glioma via EGFR/VEGF-A pathway. Oncol. Lett. 2017, 14, 4021–4028. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Wu, J.; Song, H. LRIG2 expression and prognosis in non-small cell lung cancer. Oncol. Lett. 2014, 8, 667–672. [Google Scholar] [CrossRef]
- Lindstrom, A.K.; Ekman, K.; Stendahl, U.; Tot, T.; Henriksson, R.; Hedman, H.; Hellberg, D. LRIG1 and squamous epithelial uterine cervical cancer: Correlation to prognosis, other tumor markers, sex steroid hormones, and smoking. Int. J. Gynecol. Cancer 2008, 18, 312–317. [Google Scholar] [CrossRef] [PubMed]
- Zeng, K.; Chen, X.; Xu, M.; Liu, X.; Li, C.; Xu, X.; Pan, B.; Qin, J.; He, B.; Pan, Y.; et al. LRIG3 represses cell motility by inhibiting slug via inactivating ERK signaling in human colorectal cancer. IUBMB Life 2020. [Google Scholar] [CrossRef] [PubMed]
- Lindstrom, A.K.; Hellberg, D. Immunohistochemical LRIG3 expression in cervical intraepithelial neoplasia and invasive squamous cell cervical cancer: Association with expression of tumor markers, hormones, high-risk HPV-infection, smoking and patient outcome. Eur. J. Histochem. 2014, 58, 2227. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Muller, S.; Lindquist, D.; Kanter, L.; Flores-Staino, C.; Henriksson, R.; Hedman, H.; Andersson, S. Expression of LRIG1 and LRIG3 correlates with human papillomavirus status and patient survival in cervical adenocarcinoma. Int. J. Oncol. 2013, 42, 247–252. [Google Scholar] [CrossRef]
- Ranhem, C.; Lillsunde Larsson, G.; Hedman, H.; Lindquist, D.; Karlsson, M.G.; Hellstrom, A.C.; Ostensson, E.; Sorbe, B.; Hellman, K.; Andersson, S. Expression of LRIG proteins as possible prognostic factors in primary vaginal carcinoma. PLoS ONE 2017, 12, e0183816. [Google Scholar] [CrossRef] [PubMed]
- Stefansson, K.; Oda, H.; Öfverman, C.; Lundin, E.; Hedman, H.; Lindquist, D. LRIG1-2 and LMO7 immunoreactivity in vulvar squamous cell carcinoma: Association with prognosis in relation to HPV-DNA and p16INK4a status. Oncol. Rep. 2019, 42, 142–150. [Google Scholar] [CrossRef]
- Suh, D.S.; Park, S.E.; Jin, H.; Lee, K.; Bae, J. LRIG2 is a growth suppressor of Hec-1A and Ishikawa endometrial adenocarcinoma cells by regulating PI3K/AKT- and EGFR-mediated apoptosis and cell-cycle. Oncogenesis 2018, 7, 3. [Google Scholar] [CrossRef] [PubMed]
- Qi, Y.; Chang, L.; Li, H.; Yu, G.; Xiao, W.; Xia, D.; Guan, W.; Yang, Y.; Lang, B.; Deng, K.L.; et al. Over-expression of LRIG3 suppresses growth and invasion of bladder cancer cells. J. Huazhong Univ. Sci. Technol. Med. Sci. 2013, 33, 111–116. [Google Scholar] [CrossRef]
- Yuan, X.; Bao, S.; Yang, W.; Ye, Z. Effect of silencing LRIG3 gene on the proliferation and apoptosis of bladder cancer T24 cells. J. Huazhong Univ. Sci Technol. Med. Sci. 2011, 31, 220. [Google Scholar] [CrossRef] [PubMed]
- Kohno, M.; Pouyssegur, J. Targeting the ERK signaling pathway in cancer therapy. Ann. Med. 2006, 38, 200–211. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Wang, Q.; Wang, M.; Li, M. Overexpressed LRIG3 gene ameliorates prostate cancer through suppression of cell invasion and migration. Int. J. Biol. Macromol. 2018. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Range | Cohort (n = 75) | Type 1 (n = 51) | Type 2 (n = 24) |
|---|---|---|---|---|
| Age at EC diagnosis (years) | - | 66.9 (42–92) | 66.3 (42–87) | 68.1 (44–92) |
| Body mass index (kg/m2) | - | 28.4 (18.4–47.3) | 28.3 (20.5–47.3) | 28.6 (18.4–36.5) |
| Parity (%) | None | 13.3 | 13.7 | 12.5 |
| 1–2 | 61.3 | 66.7 | 50 | |
| ≥3 | 24 | 19.6 | 33.3 | |
| Diabetes (%) | n/a | 10.7 | 12 | 9 |
| Hormone replacement therapy—ever use (%) | n/a | 52 | 51 | 59 |
| Type of EC (%) | Endometrioid adenocarcinoma | 37.8 | n/a | n/a |
| Serous carcinoma | 0 | n/a | n/a | |
| Clear cell carcinoma | 8.1 | n/a | n/a | |
| Sarcoma or myosarcoma | 8.1 | n/a | n/a | |
| Mixed cell type | 45.9 | n/a | n/a | |
| Grade of EC (%) | G1 (high) | 29.3 | 43.1 | 0 |
| G2 (moderate) | 32.0 | 47.1 | 0 | |
| G3 (poor) | 38.7 | 9.8 | 100.0 | |
| Stage of EC (%) | IA | 65.3 | 88.2 | 16.7 |
| IB | 18.7 | 11.8 | 33.3 | |
| II | 4 | 0 | 12.5 | |
| IIIA | 5.3 | 0 | 16.7 | |
| IIIB | 1.3 | 0 | 4.2 | |
| IIIC (IIIC1 or IIIC2) | 1.3 | 0 | 4.2 | |
| IVA | 0 | 0 | 0 | |
| IVB | 4 | 0 | 12.5 | |
| Depth of invasion (%) | None | 9.3 | 11.8 | 4.2 |
| <50% | 65.3 | 76.5 | 41.7 | |
| ≥50% | 25.3 | 11.8 | 54.2 | |
| Ploidy (%) | Diploid | 62.7 | 88.2 | 8.3 |
| Aneuploid | 36 | 11.8 | 87.5 | |
| p53 | % | 24 | 10 | 57 |
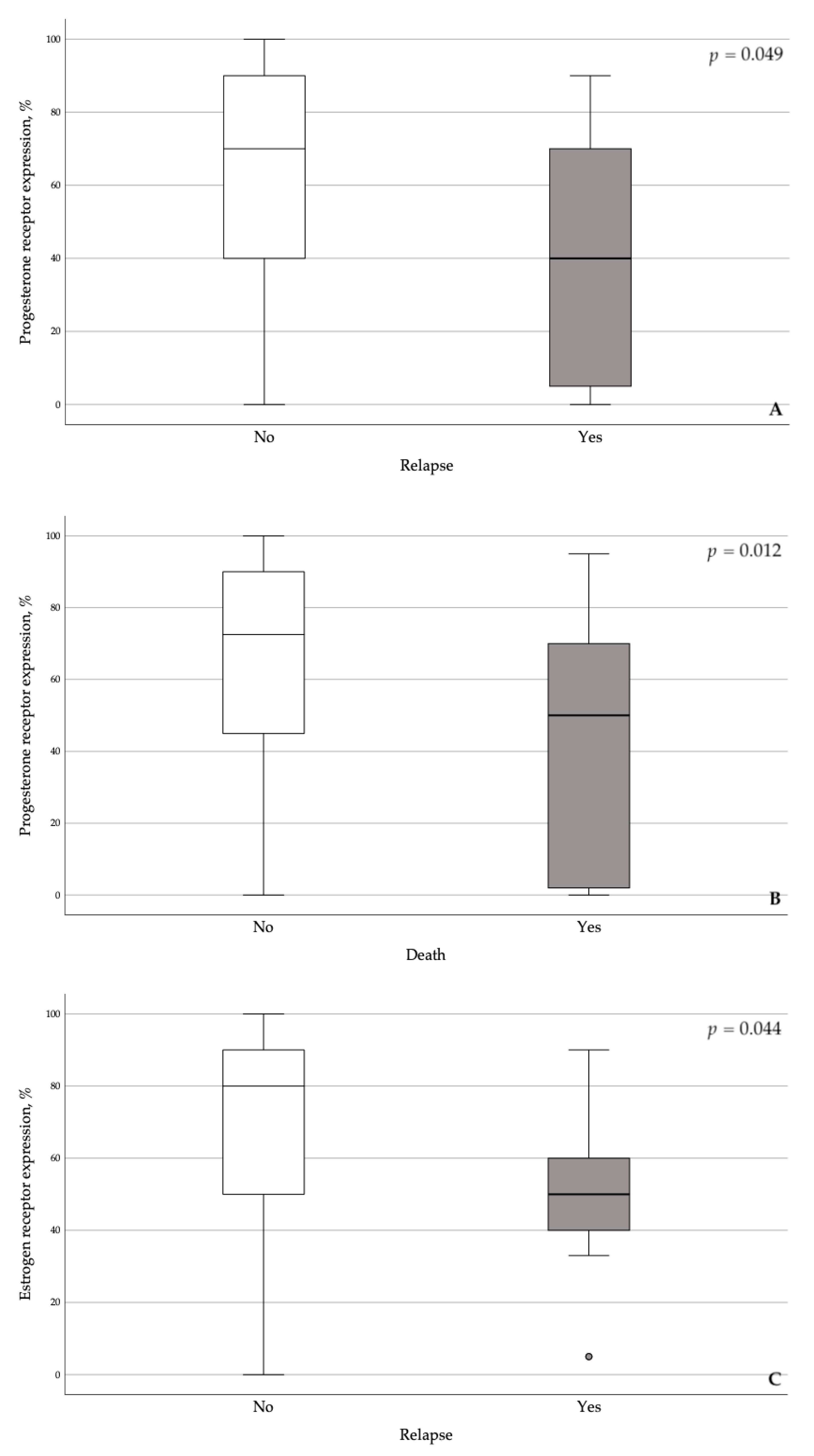
| Progesterone receptor expression | % | 57 | 71.3 | 27.3 |
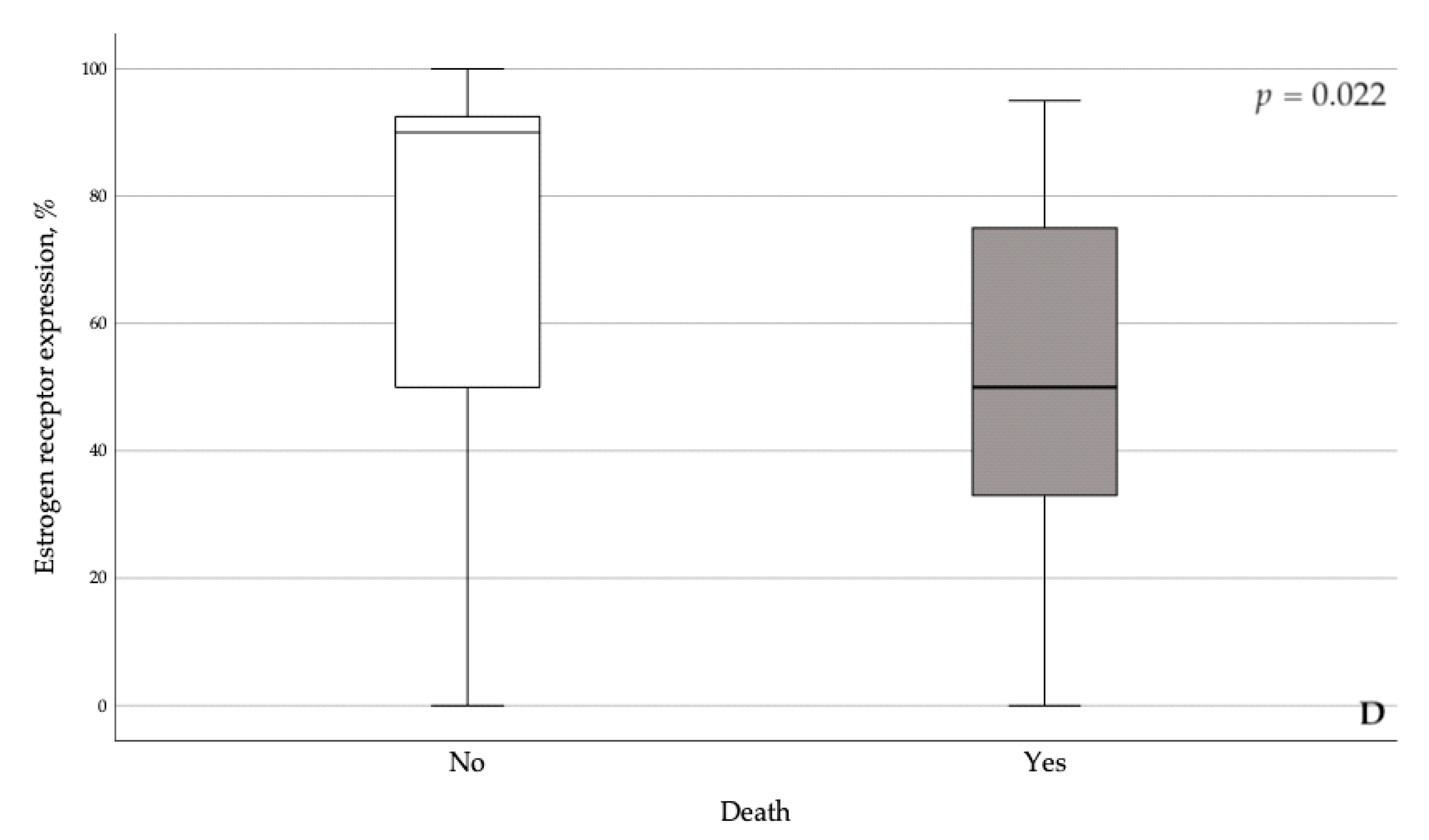
| Estrogen receptor expression | % | 64.5 | 77.9 | 36.5 |
| Protein | Protein Score * | N (%) | Type 1 | Type 2 |
|---|---|---|---|---|
| LRIG1 | 0 | 0 | 0 | 0 |
| 1 | 0 | 0 | 0 | |
| 2 | 2 (2.7) | 1 (2) | 1 (4.2) | |
| 3 | 73 (97.3) | 50 (98) | 23 (95.8) | |
| LRIG2 | 0 | 1 (1.3) | 1 (2) | 0 |
| 1 | 34 (45.3) | 24 (47.1) | 10 (41.7) | |
| 2 | 22 (29.3) | 13 (25.5) | 9 (37.5) | |
| 3 | 18 (24.0) | 13 (25.5) | 5 (20.8) | |
| LRIG3 | 0 | 4 (5.3) | 1 (2) | 3 (12.5) |
| 1 | 29 (38.7) | 16 (31.4) | 13 (54.2) | |
| 2 | 25 (33.3) | 18 (35.3) | 7 (29.2) | |
| 3 | 17 (22.7) | 16 (31.4) | 1 (4.2) |
| Type | Grade | ||||
|---|---|---|---|---|---|
| 1 | 2 | 1 | 2 | 3 | |
| LRIG1 | 90.00 (80.00–95.00) | 90.00 (80.00–95.00) | 90.00 (85.00–95.00) | 90.00 (80.00–95.00) | 90.00 (80.00–95.00) |
| p = 0.755 | p = 0.795 | ||||
| LRIG2 | 30.00 (10.00–55.00) | 30.00 (15.00–50.00) | 15.00 (5.00–50.00) | 30.00 (15.00–45.00) | 35.00 (10.00–65.00) |
| p = 0.657 | p = 0.293 | ||||
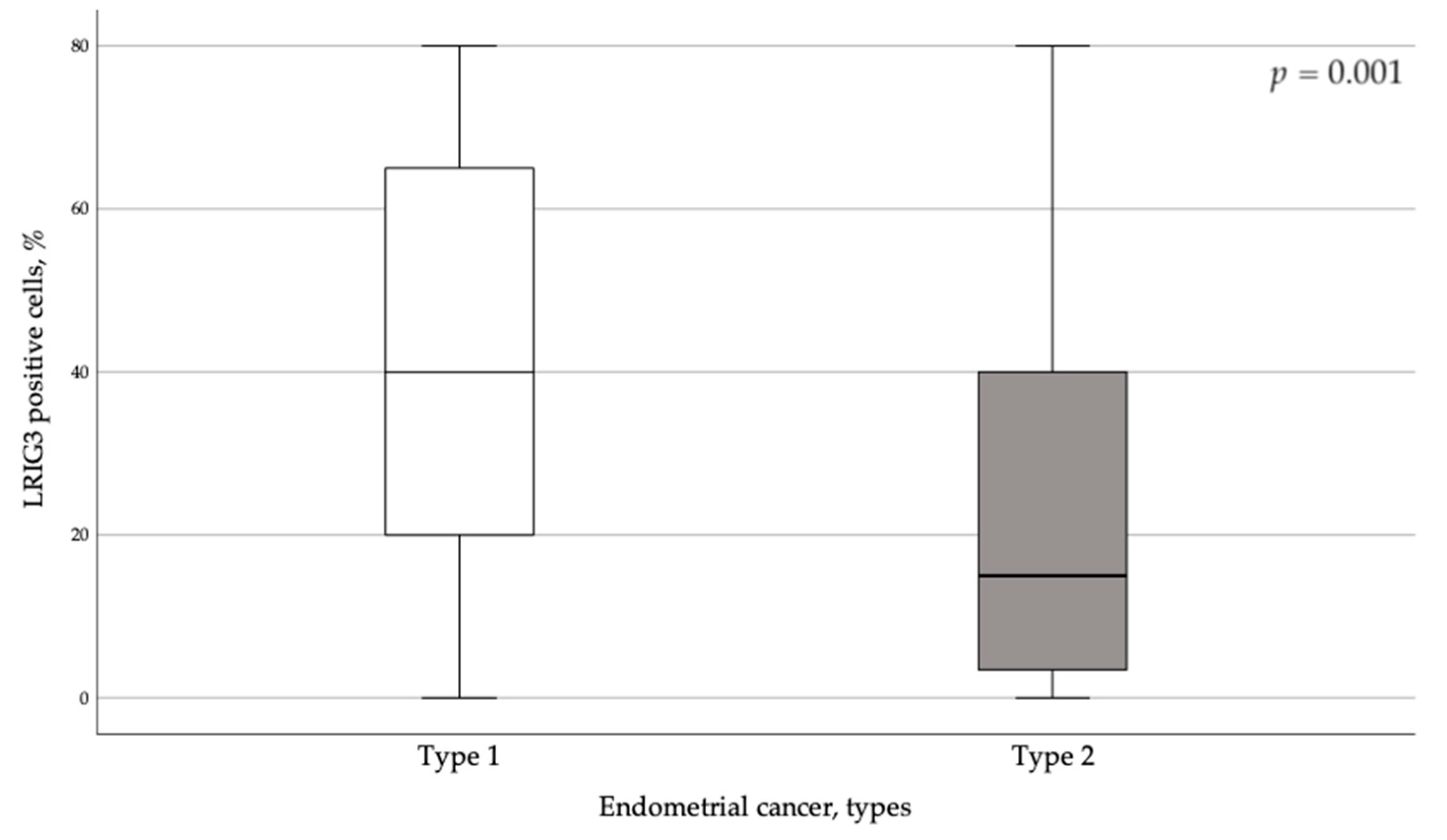
| LRIG3 | 40.00 (20.00–65.00) | 15.00 (2.75–40.00) | 45.00 (20.00–65.00) | 35.00 (17.50–55.00) | 10.00 (1.00–40.00) |
| p = 0.001 | p = 0.001 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Razumova, Z.; Oda, H.; Govorov, I.; Lundin, E.; Östensson, E.; Lindquist, D.; Mints, M. The Prognostic Role of LRIG Proteins in Endometrial Cancer. Cancers 2021, 13, 1361. https://doi.org/10.3390/cancers13061361
Razumova Z, Oda H, Govorov I, Lundin E, Östensson E, Lindquist D, Mints M. The Prognostic Role of LRIG Proteins in Endometrial Cancer. Cancers. 2021; 13(6):1361. https://doi.org/10.3390/cancers13061361
Chicago/Turabian StyleRazumova, Zoia, Husam Oda, Igor Govorov, Eva Lundin, Ellinor Östensson, David Lindquist, and Miriam Mints. 2021. "The Prognostic Role of LRIG Proteins in Endometrial Cancer" Cancers 13, no. 6: 1361. https://doi.org/10.3390/cancers13061361
APA StyleRazumova, Z., Oda, H., Govorov, I., Lundin, E., Östensson, E., Lindquist, D., & Mints, M. (2021). The Prognostic Role of LRIG Proteins in Endometrial Cancer. Cancers, 13(6), 1361. https://doi.org/10.3390/cancers13061361