
Combined Systemic and Hepatic Artery Infusion Pump Chemo-Therapy as a Liver-Directed Therapy for Colorectal Liver Metastasis-Review of Literature and Case Discussion


{kind=link}
Abstract
Simple Summary
Abstract
1. Introduction
2. Management of Resectable Liver Metastasis
3. Management of Unresectable Liver Metastasis
4. Hepatic Artery Infusion Pump (HAIP) Chemotherapy
5. Two Cases Demonstrating the Benefit of HAIP Chemotherapy
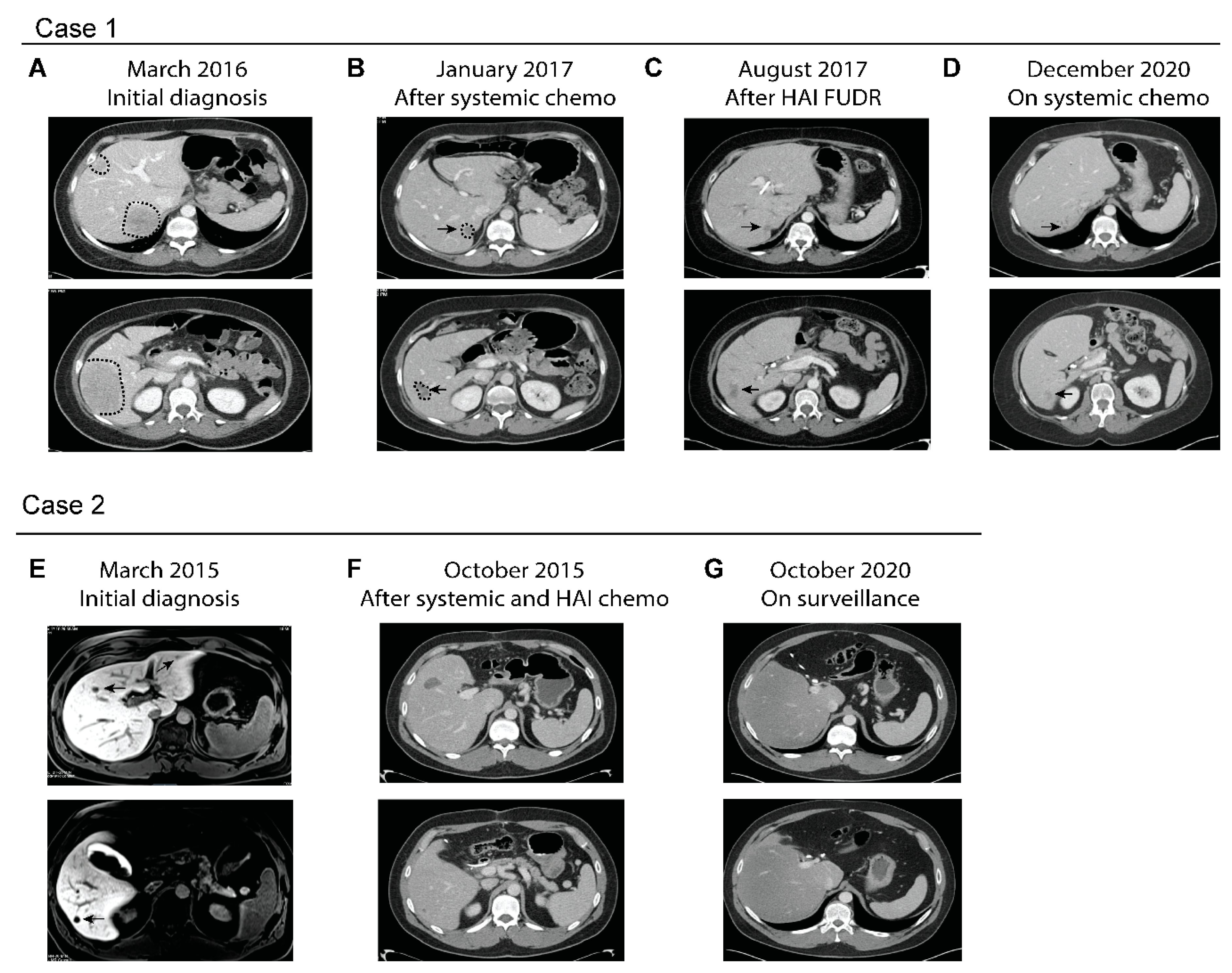
5.1. Case 1
5.2. Case 2
6. Limitations with the Use of HAIP
7. Potential Role of HAIP in the Modern Era of Systemic Treatment
8. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA A Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Manfredi, S.; Lepage, C.; Hatem, C.; Coatmeur, O.; Faivre, J.; Bouvier, A.-M. Epidemiology and Management of Liver Metastases From Colorectal Cancer. Ann. Surg. 2006, 244, 254–259. [Google Scholar] [CrossRef]
- Qiu, M.; Hu, J.; Yang, D.; Cosgrove, D.P.; Xu, R. Pattern of distant metastases in colorectal cancer: A SEER based study. Oncotarget 2015, 6, 38658–38666. [Google Scholar] [CrossRef]
- Riihimäki, M.; Hemminki, A.; Sundquist, J.; Hemminki, K. Patterns of metastasis in colon and rectal cancer. Sci. Rep. 2016, 6, 29765. [Google Scholar] [CrossRef] [PubMed]
- Abdalla, E.K.; Vauthey, J.-N.; Ellis, L.M.; Ellis, V.; Pollock, R.; Broglio, K.R.; Hess, K.; Curley, S.A. Recurrence and Outcomes Following Hepatic Resection, Radiofrequency Ablation, and Combined Resection/Ablation for Colorectal Liver Metastases. Ann. Surg. 2004, 239, 818–827. [Google Scholar] [CrossRef]
- Zacharias, A.J.; Jayakrishnan, T.T.; Rajeev, R.; Rilling, W.S.; Thomas, J.P.; George, B.; Johnston, F.M.; Gamblin, T.C.; Turaga, K.K. Comparative Effectiveness of Hepatic Artery Based Therapies for Unresectable Colorectal Liver Metastases: A Meta-Analysis. PLoS ONE 2015, 10, e0139940. [Google Scholar] [CrossRef] [PubMed]
- Sigurdson, E.R.; Ridge, A.J.; Kemeny, N.; Daly, J.M. Tumor and liver drug uptake following hepatic artery and portal vein infusion. J. Clin. Oncol. 1987, 5, 1836–1840. [Google Scholar] [CrossRef]
- Garden, O.J. Guidelines for resection of colorectal cancer liver metastases. Gut 2006, 55, iii1–iii8. [Google Scholar] [CrossRef]
- Tomlinson, J.S.; Jarnagin, W.R.; DeMatteo, R.P.; Fong, Y.; Kornprat, P.; Gonen, M.; Kemeny, N.; Brennan, M.F.; Blumgart, L.H.; D’Angelica, M. Actual 10-Year Survival After Resection of Colorectal Liver Metastases Defines Cure. J. Clin. Oncol. 2007, 25, 4575–4580. [Google Scholar] [CrossRef]
- Ekberg, H.; Tranberg, K.G.; Andersson, R.; Jeppsson, B.; Bengmark, S. Major liver resection: Perioperative course and man-agement. Surgery 1986, 100, 1–8. [Google Scholar]
- Boudjema, K.; Locher, C.; Sabbagh, C.; Ortega-Deballon, P.; Heyd, B.; Bachellier, P.; Métairie, S.; Paye, F.; Bourlier, P.; Adam, R.; et al. Simultaneous Versus Delayed Resection for Initially Resectable Synchronous Colorectal Cancer Liver Metastases. Ann. Surg. 2021, 273, 49–56. [Google Scholar] [CrossRef]
- House, M.G.; Ito, H.; Gönen, M.; Fong, Y.; Allen, P.J.; DeMatteo, R.P.; Brennan, M.F.; Blumgart, L.H.; Jarnagin, W.R.; D’Angelica, M.I. Survival after Hepatic Resection for Metastatic Colorectal Cancer: Trends in Outcomes for 1,600 Patients during Two Decades at a Single Institution. J. Am. Coll. Surg. 2010, 210, 744–752. [Google Scholar] [CrossRef] [PubMed]
- Gold, J.S.; Are, C.; Kornprat, P.; Jarnagin, W.R.; Gönen, M.; Fong, Y.; DeMatteo, R.P.; Blumgart, L.H.; D’Angelica, M. Increased Use of Parenchymal-Sparing Surgery for Bilateral Liver Metastases from Colorectal Cancer Is Associated With Improved Mortality Without Change in Oncologic Outcome. Ann. Surg. 2008, 247, 109–117. [Google Scholar] [CrossRef]
- Kingham, T.P.; Correa-Gallego, C.; D’Angelica, M.I.; Gönen, M.; DeMatteo, R.P.; Fong, Y.; Allen, P.J.; Blumgart, L.H.; Jarnagin, W.R. Hepatic Parenchymal Preservation Surgery: Decreasing Morbidity and Mortality Rates in 4,152 Resections for Malignancy. J. Am. Coll. Surg. 2015, 220, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Fong, Y.; Cohen, A.M.; Fortner, J.G.; Enker, W.; Turnbull, A.D.; Coit, D.G.; Marrero, A.M.; Prasad, M.; Blumgart, L.H.; Brennan, M.F. Liver resection for colorectal metastases. J. Clin. Oncol. 1997, 15, 938–946. [Google Scholar] [CrossRef] [PubMed]
- Nordlinger, B.; Quilichini, M.A.; Parc, R.; Hannoun, L.; Delva, E.; Huguet, C. Surgical resection of liver metastases from co-lo-rectal cancers. Int. Surg. 1987, 72, 70–72. [Google Scholar]
- Fong, Y.; Fortner, J.; Sun, R.L.; Brennan, M.F.; Blumgart, L.H. Clinical Score for Predicting Recurrence After Hepatic Resection for Metastatic Colorectal Cancer. Ann. Surg. 1999, 230, 309. [Google Scholar] [CrossRef] [PubMed]
- Choti, M.A.; Sitzmann, J.V.; Tiburi, M.F.; Sumetchotimetha, W.; Rangsin, R.; Schulick, R.D.; Lillemoe, K.D.; Yeo, C.J.; Cameron, J.L. Trends in Long-Term Survival Following Liver Resection for Hepatic Colorectal Metastases. Ann. Surg. 2002, 235, 759–766. [Google Scholar] [CrossRef] [PubMed]
- Pawlik, T.M.; Scoggins, C.R.; Zorzi, D.; Abdalla, E.K.; Andres, A.; Eng, C.; Curley, S.A.; Loyer, E.M.; Muratore, A.; Mentha, G.; et al. Effect of Surgical Margin Status on Survival and Site of Recurrence After Hepatic Resection for Colorectal Metastases. Ann. Surg. 2005, 241, 715–724. [Google Scholar] [CrossRef]
- Charnsangavej, C.; Clary, B.; Fong, Y.; Grothey, A.; Pawlik, T.M.; Choti, M.A. Selection of Patients for Resection of Hepatic Colorectal Metastases: Expert Consensus Statement. Ann. Surg. Oncol. 2006, 13, 1261–1268. [Google Scholar] [CrossRef] [PubMed]
- Nordlinger, B.; Guiguet, M.; Vaillant, J.; Balladur, P.; Boudjema, K.; Bachellier, P.; Jaeck, D. Surgical resection of colorectal carcinoma metastases to the liver: A prognostic scoring system to improve case selection, based on 1568 patients. Cancer 1996, 77, 1254–1262. [Google Scholar] [CrossRef]
- Carpizo, D.R.; Are, C.; Jarnagin, W.; DeMatteo, R.; Fong, Y.; Gonen, M.; Blumgart, L.; D’Angelica, M. Liver Resection for Metastatic Colorectal Cancer in Patients with Concurrent Extrahepatic Disease: Results in 127 Patients Treated at a Single Center. Ann. Surg. Oncol. 2009, 16, 2138–2146. [Google Scholar] [CrossRef] [PubMed]
- Covey, A.M.; Brown, K.T.; Jarnagin, W.R.; Brody, L.A.; Schwartz, L.; Tuorto, S.; Sofocleous, C.T.; D’Angelica, M.; Getrajdman, G.I.; DeMatteo, R.; et al. Combined Portal Vein Embolization and Neoadjuvant Chemotherapy as a Treatment Strategy for Resectable Hepatic Colorectal Metastases. Ann. Surg. 2008, 247, 451–455. [Google Scholar] [CrossRef] [PubMed]
- Adam, R.; Miller, R.; Pitombo, M.; Wicherts, D.A.; de Haas, R.J.; Bitsakou, G.; Aloia, T. Two-stage Hepatectomy Approach for Initially Unresectable Colorectal Hepatic Metastases. Surg. Oncol. Clin. North Am. 2007, 16, 525–536. [Google Scholar] [CrossRef]
- Teo, J.-Y.; Allen, J.C.; Foong-Khoon, C.; Choo, S.-P.; Tai, D.W.; Chang, J.P.; Cheah, F.-K.; Chow, P.K.; Goh, B.K. A systematic review of contralateral liver lobe hypertrophy after unilobar selective internal radiation therapy with Y90. HPB 2016, 18, 7–12. [Google Scholar] [CrossRef]
- Bartlett, D.L.; Berlin, J.; Lauwers, G.Y.; Messersmith, W.A.; Petrelli, N.J.; Venook, A.P. Chemotherapy and Regional Therapy of Hepatic Colorectal Metastases: Expert Consensus Statement. Ann. Surg. Oncol. 2006, 13, 1284–1292. [Google Scholar] [CrossRef]
- Hagness, M.; Foss, A.; Egge, T.S.; Dueland, S. Patterns of Recurrence after Liver Transplantation for Nonresectable Liver Metastases from Colorectal Cancer. Ann. Surg. Oncol. 2014, 21, 1323–1329. [Google Scholar] [CrossRef]
- Simoneau, E.; D’Angelica, M.; Halazun, K.J. Liver transplantation for colorectal liver metastasis. Curr. Opin. Organ Transplant. 2019, 24, 175–181. [Google Scholar] [CrossRef]
- Ensminger, W.D.; Gyves, J.W. Clinical pharmacology of hepatic arterial chemotherapy. Semin. Oncol. 1983, 10, 176–182. [Google Scholar]
- Dzodic, R.; Gomez-Abuin, G.; Rougier, P.; Bonnay, M.; Ardouin, P.; Gouyette, A.; Rixe, O.; Ducreux, M.; Munck, J.-N. Pharmacokinetic advantage of intra-arterial hepatic oxaliplatin administration: Comparative results with cisplatin using a rabbit VX2 tumor model. Anti-Cancer Drugs 2004, 15, 647–650. [Google Scholar] [CrossRef]
- Blackshear, P.J.; Dorman, F.D.; Varco, R.L.; Buchwald, H. The design and initial testing of an implantable infusion pump. Surg. Gynecol. Obstet. 1972, 134, 51–56. [Google Scholar] [PubMed]
- Thiels, C.A.; D’Angelica, M.I. Hepatic artery infusion pumps. J. Surg. Oncol. 2020, 122, 70–77. [Google Scholar] [CrossRef]
- Barone, R.M.; Byfield, J.E.; Goldfarb, P.B.; Frankel, S.; Ginn, C.; Greer, S. Intra-arterial chemotherapy using an implantable infusion pump and liver irradiation for the treatment of hepatic metastases. Cancer 1982, 50, 850–862. [Google Scholar] [CrossRef]
- Buchwald, H.; Grage, T.B.; Vassilopoulos, P.P.; Rohde, T.D.; Varco, R.L.; Blackshear, P.J. Intraarterial infusion chemotherapy for hepatic carcinoma using a totally implantable infusion pump. Cancer 1980, 45, 866–869. [Google Scholar] [CrossRef]
- Doussot, A.; Kemeny, N.E.; D’Angelica, M.I. Hepatic arterial infusional chemotherapy in the management of colorectal cancer liver metastases. Hepatic Oncol. 2015, 2, 275–290. [Google Scholar] [CrossRef]
- Chang, A.E.; Schneider, P.D.; Sugarbaker, P.H.; Simpson, C.; Culnane, M.; Steinberg, S.M. A Prospective Randomized Trial of Regional Versus Systemic Continuous 5-Fluorodeoxyuridine Chemotherapy in the Treatment of Colorectal Liver Metastases. Ann. Surg. 1987, 206, 685–693. [Google Scholar] [CrossRef]
- Kemeny, N.; Daly, J.; Reichman, B.; Geller, N.; Botet, J.; Oderman, P. Intrahepatic or Systemic Infusion of Fluorodeoxyuridine in Patients with Liver Metastases from Colorectal Carcinoma. Ann. Intern. Med. 1987, 107, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Kemeny, N.E.; Niedzwiecki, D.; Hollis, D.R.; Lenz, H.-J.; Warren, R.S.; Naughton, M.J.; Weeks, J.C.; Sigurdson, E.R.; Ii, J.E.H.; Zhang, C.; et al. Hepatic Arterial Infusion Versus Systemic Therapy for Hepatic Metastases from Colorectal Cancer: A Randomized Trial of Efficacy, Quality of Life, and Molecular Markers (CALGB 9481). J. Clin. Oncol. 2006, 24, 1395–1403. [Google Scholar] [CrossRef] [PubMed]
- Mocellin, S.; Pasquali, S.; Nitti, D. Fluoropyrimidine-HAI (hepatic arterial infusion) versus systemic chemotherapy (SCT) for unresectable liver metastases from colorectal cancer. Cochrane Database Syst. Rev. 2009, CD007823. [Google Scholar] [CrossRef]
- De Gramont, A.; Figer, A.; Seymour, M.; Homerin, M.; Hmissi, A.; Cassidy, J.; Boni, C.; Cortes-Funes, H.; Cervantes, A.; Freyer, G.; et al. Leucovorin and Fluorouracil with or Without Oxaliplatin as First-Line Treatment in Advanced Colorectal Cancer. J. Clin. Oncol. 2000, 18, 2938–2947. [Google Scholar] [CrossRef]
- Kemeny, N.; Jarnagin, W.; Paty, P.; Gonen, M.; Schwartz, L.; Morse, M.; Leonard, G.; D’Angelica, M.; DeMatteo, R.; Blumgart, L.; et al. Phase I Trial of Systemic Oxaliplatin Combination Chemotherapy with Hepatic Arterial Infusion in Patients With Unresectable Liver Metastases From Colorectal Cancer. J. Clin. Oncol. 2005, 23, 4888–4896. [Google Scholar] [CrossRef] [PubMed]
- Kemeny, N.; Gonen, M.; Sullivan, D.; Schwartz, L.; Benedetti, F.; Saltz, L.; Stockman, J.; Fong, Y.; Jarnagin, W.; Bertino, J.; et al. Phase I Study of Hepatic Arterial Infusion of Floxuridine and Dexamethasone with Systemic Irinotecan for Unresectable Hepatic Metastases From Colorectal Cancer. J. Clin. Oncol. 2001, 19, 2687–2695. [Google Scholar] [CrossRef]
- Kemeny, N.E.; Melendez, F.D.H.; Capanu, M.; Paty, P.B.; Fong, Y.; Schwartz, L.H.; Jarnagin, W.R.; Patel, D.; D’Angelica, M. Conversion to Resectability Using Hepatic Artery Infusion Plus Systemic Chemotherapy for the Treatment of Unresectable Liver Metastases from Colorectal Carcinoma. J. Clin. Oncol. 2009, 27, 3465–3471. [Google Scholar] [CrossRef]
- D’Angelica, M.I.; Correa-Gallego, C.; Paty, P.B.; Cercek, A.; Gewirtz, A.N.; Chou, J.F.; Capanu, M.; Kingham, T.P.; Fong, Y.; DeMatteo, R.P.; et al. Phase II Trial of Hepatic Artery Infusional and Systemic Chemotherapy for Patients with Unresectable Hepatic Metastases From Colorectal Cancer. Ann. Surg. 2015, 261, 353–360. [Google Scholar] [CrossRef]
- Chan, D.L.; Alzahrani, N.A.; Morris, D.L.; Chua, T.C. Systematic review and meta-analysis of hepatic arterial infusion chemotherapy as bridging therapy for colorectal liver metastases. Surg. Oncol. 2015, 24, 162–171. [Google Scholar] [CrossRef]
- De Jong, M.C.; Pulitano, C.; Ribero, D.; Strub, J.; Mentha, G.; Schulick, R.D.; Choti, M.A.; Aldrighetti, L.; Capussotti, L.; Pawlik, T.M. Rates and Patterns of Recurrence Following Curative Intent Surgery for Colorectal Liver Metastasis. Ann. Surg. 2009, 250, 440–448. [Google Scholar] [CrossRef]
- D’Angelica, M.; Kornprat, P.; Gonen, M.; DeMatteo, R.P.; Fong, Y.; Blumgart, L.H.; Jarnagin, W.R. Effect on Outcome of Recurrence Patterns After Hepatectomy for Colorectal Metastases. Ann. Surg. Oncol. 2010, 18, 1096–1103. [Google Scholar] [CrossRef] [PubMed]
- Kemeny, N.E.; Chou, J.F.; Ba, T.M.B.; Capanu, M.; DeMatteo, R.P.; Jarnagin, W.R.; Allen, P.J.; Fong, Y.C.; Cercek, A.; D’Angelica, M.I. Updated long-term survival for patients with metastatic colorectal cancer treated with liver resection followed by hepatic arterial infusion and systemic chemotherapy. J. Surg. Oncol. 2016, 113, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Buisman, F.E.; Galjart, B.; Van Der Stok, E.P.; Kemeny, N.E.; Balachandran, V.P.; Boerner, T.; Cercek, A.; Grünhagen, D.J.; Jarnagin, W.R.; Kingham, T.P.; et al. The impact of hepatic arterial infusion pump chemotherapy on hepatic recurrences and survival in patients with resected colorectal liver metastases. HPB 2020, 22, 1271–1279. [Google Scholar] [CrossRef]
- Allen, P.J.; Nissan, A.; Picon, A.I.; Kemeny, N.; Dudrick, P.; Ben-Porat, L.; Espat, J.; Stojadinovic, A.; Cohen, A.M.; Fong, Y.; et al. Technical Complications and Durability of Hepatic Artery Infusion Pumps for Unresectable Colorectal Liver Metastases: An Institutional Experience of 544 Consecutive Cases. J. Am. Coll. Surg. 2005, 201, 57–65. [Google Scholar] [CrossRef]
- Mocellin, S.; Pilati, P.; Lise, M.; Nitti, D. Meta-Analysis of Hepatic Arterial Infusion for Unresectable Liver Metastases From Colorectal Cancer: The End of an Era? J. Clin. Oncol. 2007, 25, 5649–5654. [Google Scholar] [CrossRef] [PubMed]
- Bloom, A.I.; Gordon, R.L.; Ahl, K.H.; Kerlan, R.K.; Laberge, J.M.; Wilson, M.W.; Venook, A.P.; Warren, R. Transcatheter Embolization for the Treatment of Misperfusion After Hepatic Artery Chemoinfusion Pump Implantation. Ann. Surg. Oncol. 1999, 6, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Ito, K.; Ito, H.; Kemeny, N.E.; Gonen, M.; Allen, P.J.; Paty, P.B.; Fong, Y.; DeMatteo, R.P.; Blumgart, L.H.; Jarnagin, W.R.; et al. Biliary Sclerosis after Hepatic Arterial Infusion Pump Chemotherapy for Patients with Colorectal Cancer Liver Metastasis: Incidence, Clinical Features, and Risk Factors. Ann. Surg. Oncol. 2011, 19, 1609–1617. [Google Scholar] [CrossRef]
- Loupakis, F.; Cremolini, C.; Masi, G.; Lonardi, S.; Zagonel, V.; Salvatore, L.; Cortesi, E.; Tomasello, G.; Ronzoni, M.; Spadi, R.; et al. Initial Therapy with FOLFOXIRI and Bevacizumab for Metastatic Colorectal Cancer. N. Engl. J. Med. 2014, 371, 1609–1618. [Google Scholar] [CrossRef]
- Cremolini, C.; Loupakis, F.; Antoniotti, C.; Lupi, C.; Sensi, E.; Lonardi, S.; Mezi, S.; Tomasello, G.; Ronzoni, M.; Zaniboni, A.; et al. FOLFOXIRI plus bevacizumab versus FOLFIRI plus bevacizumab as first-line treatment of patients with metastatic colorectal cancer: Updated overall survival and molecular subgroup analyses of the open-label, phase 3 TRIBE study. Lancet Oncol. 2015, 16, 1306–1315. [Google Scholar] [CrossRef]
- Gruenberger, T.; Bridgewater, J.; Chau, I.; Alfonso, P.G.; Rivoire, M.; Mudan, S.; Lasserre, S.; Hermann, F.; Waterkamp, D.; Adam, R. Bevacizumab plus mFOLFOX-6 or FOLFOXIRI in patients with initially unresectable liver metastases from colorectal cancer: The OLIVIA multinational randomised phase II trial. Ann. Oncol. 2015, 26, 702–708. [Google Scholar] [CrossRef] [PubMed]
- Modest, D.P.; Martens, U.M.; Riera-Knorrenschild, J.; Greeve, J.; Florschütz, A.; Wessendorf, S.; Ettrich, T.; Kanzler, S.; Nörenberg, D.; Ricke, J.; et al. FOLFOXIRI Plus Panitumumab As First-Line Treatment of RAS Wild-Type Metastatic Colorectal Cancer: The Randomized, Open-Label, Phase II VOLFI Study (AIO KRK0109). J. Clin. Oncol. 2019, 37, 3401–3411. [Google Scholar] [CrossRef]
- Boland, C.R.; Goel, A. Microsatellite instability in colorectal cancer. Gastroenterology 2010, 138, 2073–2087. [Google Scholar] [CrossRef]
- André, T.; Shiu, K.-K.; Kim, T.W.; Jensen, B.V.; Jensen, L.H.; Punt, C.; Smith, D.; Garcia-Carbonero, R.; Benavides, M.; Gibbs, P.; et al. Pembrolizumab in Microsatellite-Instability–High Advanced Colorectal Cancer. N Engl. J. Med. 2020, 383, 2207–2218. [Google Scholar] [CrossRef]
- Le, D.T.; Uram, J.N.; Wang, H.; Bartlett, B.R.; Kemberling, H.; Eyring, A.D.; Skora, A.D.; Luber, B.S.; Azad, N.S.; Laheru, D.; et al. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N. Engl. J. Med. 2015, 372, 2509–2520. [Google Scholar] [CrossRef]
- Overman, M.J.; McDermott, R.; Leach, J.L.; Lonardi, S.; Lenz, H.-J.; Morse, M.; Desai, J.; Hill, A.; Axelson, M.; Moss, R.; et al. Nivolumab in patients with metastatic DNA mismatch repair-deficient or microsatellite instability-high colorectal cancer (CheckMate 142): An open-label, multicentre, phase 2 study. Lancet Oncol. 2017, 18, 1182–1191. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chaudhry, S.; Fields, R.C.; Grierson, P.M.; Lim, K.-H. Combined Systemic and Hepatic Artery Infusion Pump Chemo-Therapy as a Liver-Directed Therapy for Colorectal Liver Metastasis-Review of Literature and Case Discussion. Cancers 2021, 13, 1283. https://doi.org/10.3390/cancers13061283
Chaudhry S, Fields RC, Grierson PM, Lim K-H. Combined Systemic and Hepatic Artery Infusion Pump Chemo-Therapy as a Liver-Directed Therapy for Colorectal Liver Metastasis-Review of Literature and Case Discussion. Cancers. 2021; 13(6):1283. https://doi.org/10.3390/cancers13061283
Chicago/Turabian StyleChaudhry, Salman, Ryan C. Fields, Patrick M. Grierson, and Kian-Huat Lim. 2021. "Combined Systemic and Hepatic Artery Infusion Pump Chemo-Therapy as a Liver-Directed Therapy for Colorectal Liver Metastasis-Review of Literature and Case Discussion" Cancers 13, no. 6: 1283. https://doi.org/10.3390/cancers13061283
APA StyleChaudhry, S., Fields, R. C., Grierson, P. M., & Lim, K.-H. (2021). Combined Systemic and Hepatic Artery Infusion Pump Chemo-Therapy as a Liver-Directed Therapy for Colorectal Liver Metastasis-Review of Literature and Case Discussion. Cancers, 13(6), 1283. https://doi.org/10.3390/cancers13061283