
Lymphopenia as a Biological Predictor of Outcomes in COVID-19 Patients: A Nationwide Cohort Study

 , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Results
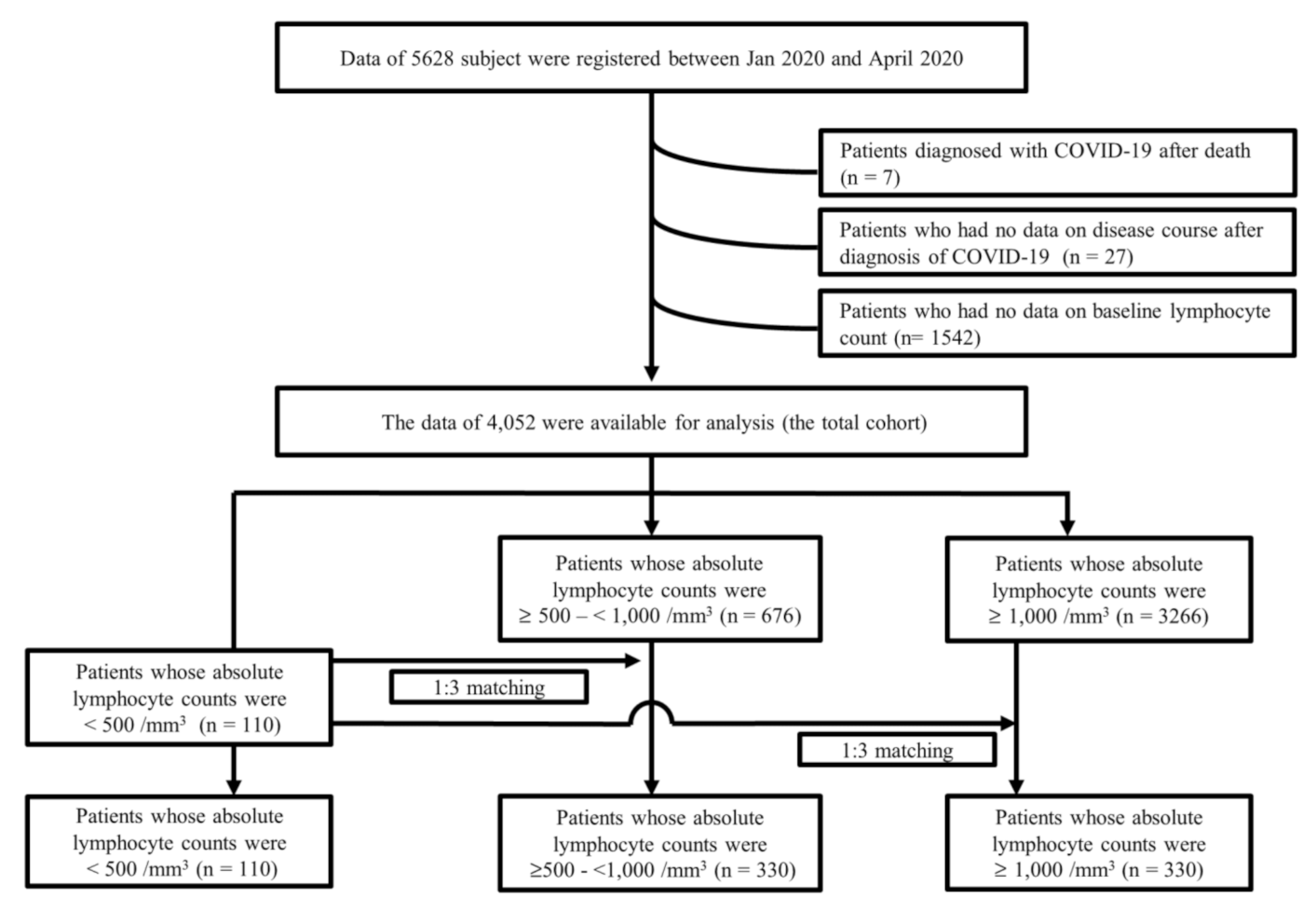
2.1. Characteristics of the Total Cohort
2.2. Baseline Characteristics among Propensity Matched Cohorts
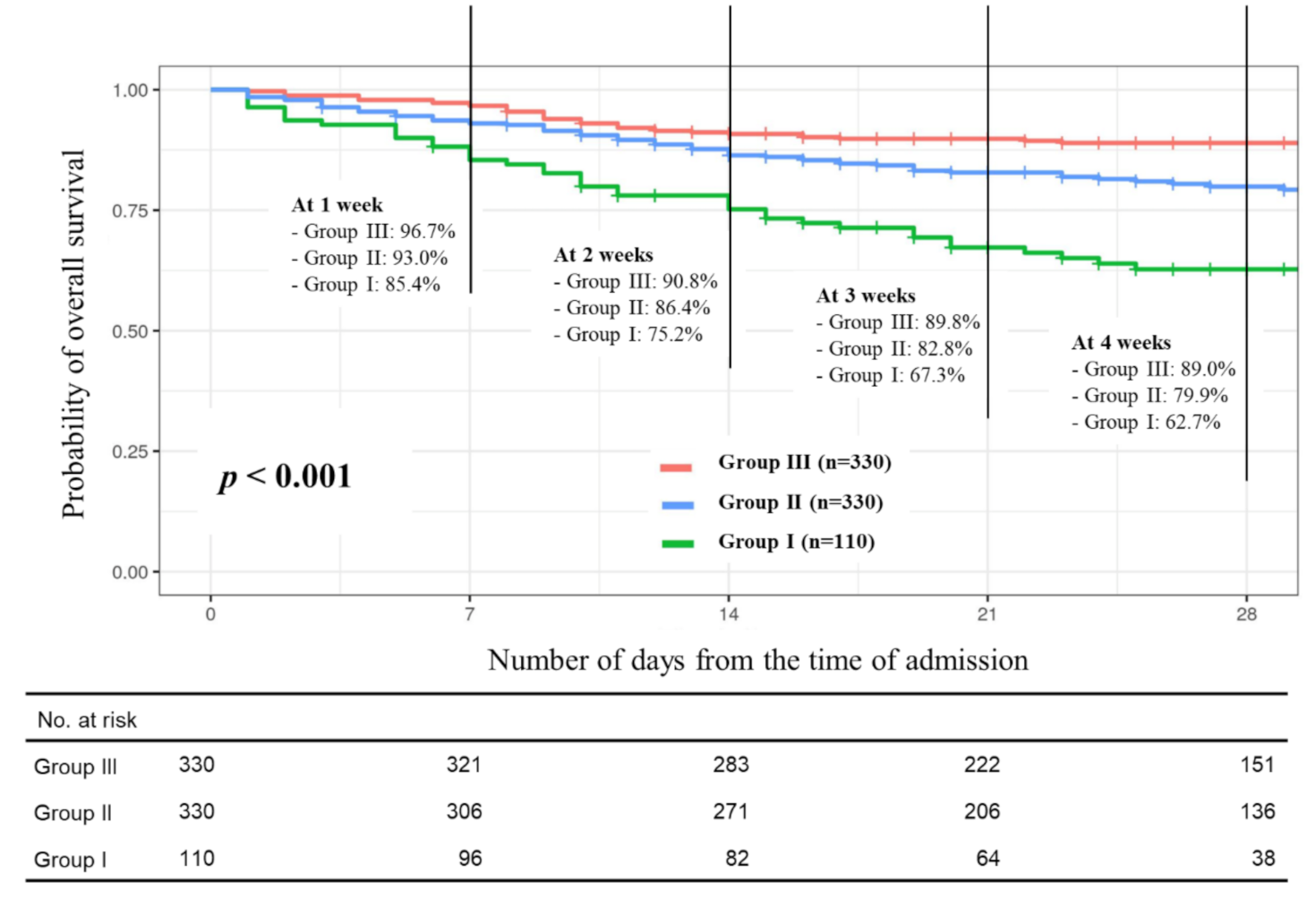
2.3. Primary and Secondary Endpoints
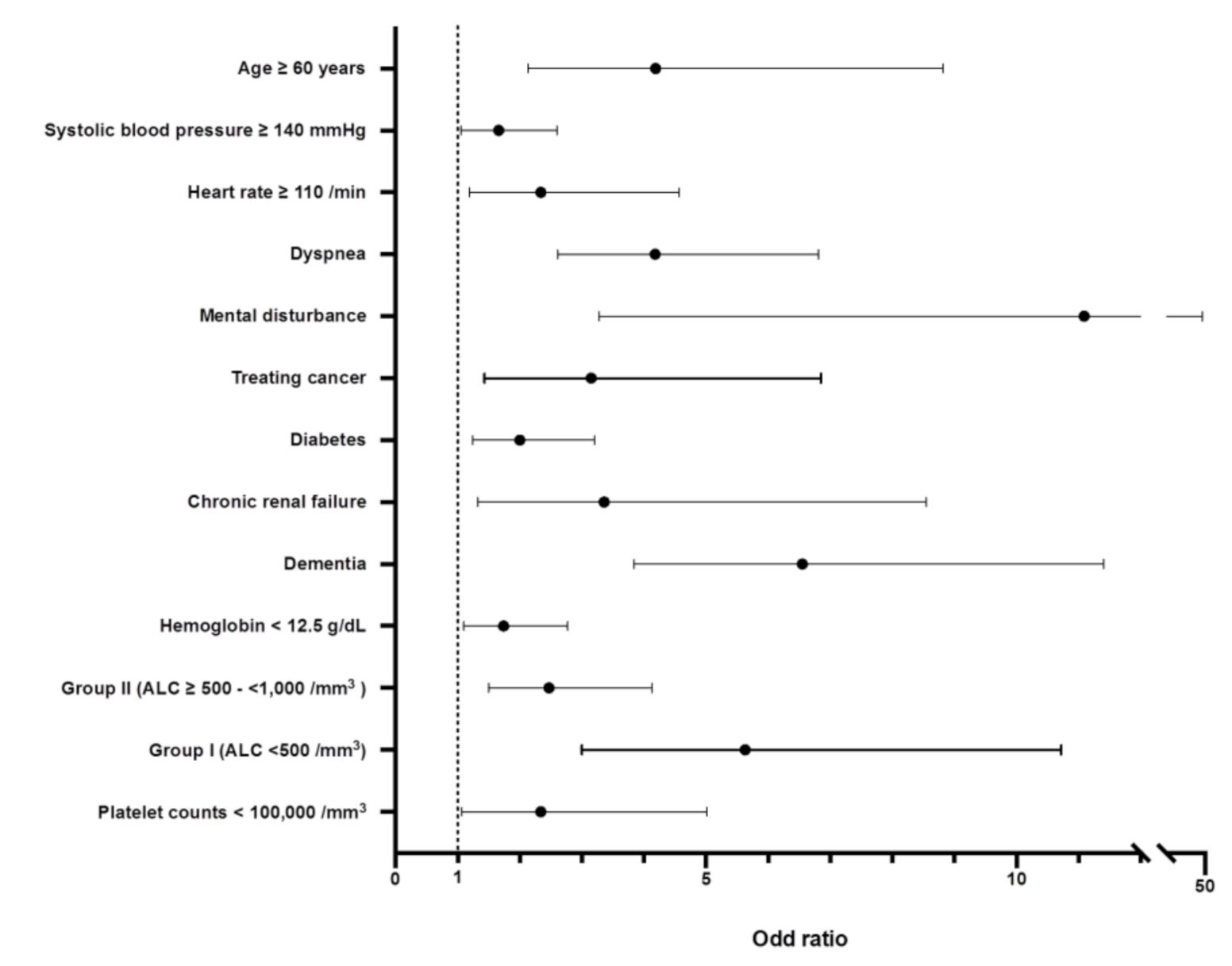
2.4. Prognostic Parameters for Mortality of COVID-19
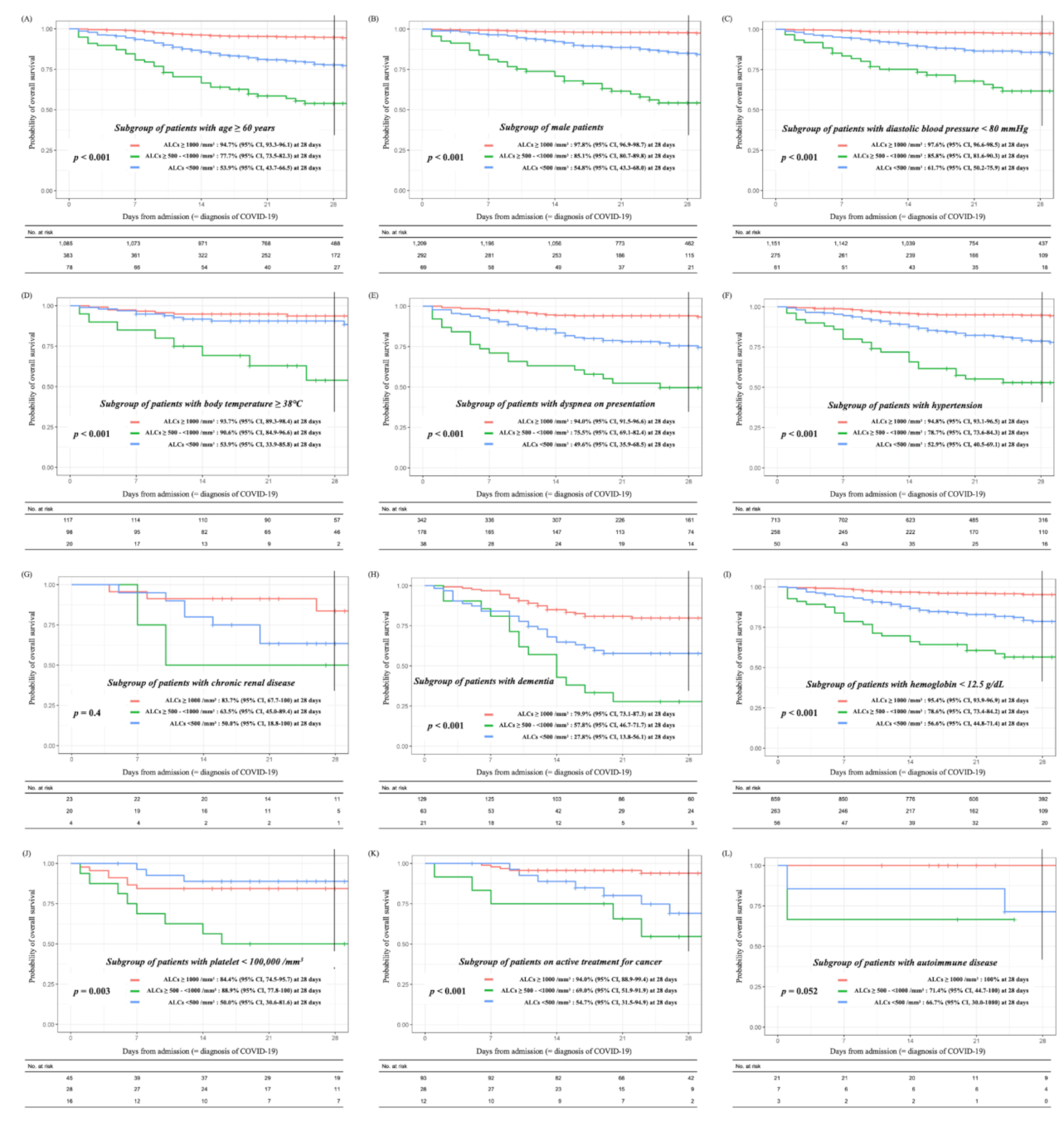
2.5. Subgroup Analysis
3. Discussion
4. Materials and Methods
4.1. Data Source
4.2. Outcome Measurements
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- WHO, Coronavirus disease 2019 (COVID-19) Situation Report—70. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200330-sitrep-70-covid-19.pdf?sfvrsn=7e0fe3f8_2 (accessed on 30 March 2020).
- Cascella, M.; Rajnik, M.; Cuomo, A.; Dulebohn, S.C.; Di Napoli, R. Features, Evaluation, and Treatment of Coronavirus (COVID-19); StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Emanuel, E.J.; Persad, G.; Upshur, R.; Thome, B.; Parker, M.; Glickman, A.; Zhang, C.; Boyle, C.; Smith, M.; Phillips, J.P. Fair Allocation of Scarce Medical Resources in the Time of Covid-19. N. Engl. J. Med. 2020, 382, 2049–2055. [Google Scholar] [CrossRef]
- Kang, S.J.; Jung, S.I. Age-Related Morbidity and Mortality among Patients with COVID-19. Infect. Chemother. 2020, 52, 154–164. [Google Scholar] [CrossRef]
- Jang, J.G.; Hur, J.; Choi, E.Y.; Hong, K.S.; Lee, W.; Ahn, J.H. Prognostic Factors for Severe Coronavirus Disease 2019 in Daegu, Korea. J. Korean Med. Sci. 2020, 35, e209. [Google Scholar] [CrossRef]
- Li, X.; Xu, S.; Yu, M.; Wang, K.; Tao, Y.; Zhou, Y.; Shi, J.; Zhou, M.; Wu, B.; Yang, Z.; et al. Risk factors for severity and mortality in adult COVID-19 inpatients in Wuhan. J. Allergy Clin. Immunol. 2020, 146, 110–118. [Google Scholar] [CrossRef]
- Weiss, S.R. Forty years with coronaviruses. J. Exp. Med. 2020, 217. [Google Scholar] [CrossRef]
- Meo, S.A.; Alhowikan, A.M.; Al-Khlaiwi, T.; Meo, I.M.; Halepoto, D.M.; Iqbal, M.; Usmani, A.M.; Hajjar, W.; Ahmed, N. Novel coronavirus 2019-nCoV: Prevalence, biological and clinical characteristics comparison with SARS-CoV and MERS-CoV. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 2012–2019. [Google Scholar] [CrossRef]
- Fathi, N.; Rezaei, N. Lymphopenia in COVID-19: Therapeutic opportunities. Cell Biol. Int. 2020, 44, 1792–1797. [Google Scholar] [CrossRef]
- de Wit, E.; van Doremalen, N.; Falzarano, D.; Munster, V.J. SARS and MERS: Recent insights into emerging coronaviruses. Nat. Rev. Microbiol. 2016, 14, 523–534. [Google Scholar] [CrossRef]
- Chien, J.Y.; Hsueh, P.R.; Cheng, W.C.; Yu, C.J.; Yang, P.C. Temporal changes in cytokine/chemokine profiles and pulmonary involvement in severe acute respiratory syndrome. Respirology 2006, 11, 715–722. [Google Scholar] [CrossRef]
- Tan, L.; Wang, Q.; Zhang, D.; Ding, J.; Huang, Q.; Tang, Y.Q.; Wang, Q.; Miao, H. Lymphopenia predicts disease severity of COVID-19: A descriptive and predictive study. Signal. Transduct. Target. Ther. 2020, 5, 33. [Google Scholar] [CrossRef]
- Fan, B.E.; Chong, V.C.L.; Chan, S.S.W.; Lim, G.H.; Lim, K.G.E.; Tan, G.B.; Mucheli, S.S.; Kuperan, P.; Ong, K.H. Hematologic parameters in patients with COVID-19 infection. Am. J. Hematol. 2020, 95, e131–e134. [Google Scholar] [CrossRef]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of Immune Response in Patients with Coronavirus 2019 (COVID-19) in Wuhan, China. Clin. Infect. Dis. 2020, 71, 762–768. [Google Scholar] [CrossRef]
- Moon, S.-S.; Lee, K.; Park, J.; Yun, S.; Lee, Y.S.; Lee, D.S. Clinical Characteristics and Mortality Predictors of COVID-19 Patients Hospitalized at Nationally-Designated Treatment Hospitals. J. Korean Med. Sci. 2020, 35, e328. [Google Scholar] [CrossRef]
- Wan, S.; Xiang, Y.; Fang, W.; Zheng, Y.; Li, B.; Hu, Y.; Lang, C.; Huang, D.; Sun, Q.; Xiong, Y.; et al. Clinical features and treatment of COVID-19 patients in northeast Chongqing. J. Med. Virol. 2020, 92, 797–806. [Google Scholar] [CrossRef]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.a.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated with Acute Respiratory Distress Syndrome and Death in Patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef]
- Zhang, J.J.; Dong, X.; Cao, Y.Y.; Yuan, Y.D.; Yang, Y.B.; Yan, Y.Q.; Akdis, C.A.; Gao, Y.D. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy 2020, 75, 1730–1741. [Google Scholar] [CrossRef]
- Qian, G.Q.; Yang, N.B.; Ding, F.; Ma, A.H.Y.; Wang, Z.Y.; Shen, Y.F.; Shi, C.W.; Lian, X.; Chu, J.G.; Chen, L.; et al. Epidemiologic and clinical characteristics of 91 hospitalized patients with COVID-19 in Zhejiang, China: A retrospective, multi-centre case series. QJM 2020, 113, 474–481. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- U.S. National Cancer Institue. Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0. 2017. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_5x7.pdf (accessed on 30 March 2020).
- Cheung, C.K.M.; Law, M.F.; Lui, G.C.Y.; Wong, S.H.; Wong, R.S.M. Coronavirus Disease 2019 (COVID-19): A Haematologist’s Perspective. Acta Haematol. 2020, 10, 1–14. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; the Northwell, C.-R.C.; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- Park, P.G.; Kim, C.H.; Heo, Y.; Kim, T.S.; Park, C.W.; Kim, C.H. Out-of-Hospital Cohort Treatment of Coronavirus Disease 2019 Patients with Mild Symptoms in Korea: An Experience from a Single Community Treatment Center. J. Korean Med. Sci. 2020, 35, e140. [Google Scholar] [CrossRef]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef]
- Acharya, D.; Lee, K.; Lee, D.S.; Lee, Y.S.; Moon, S.-S. Mortality Rate and Predictors of Mortality in Hospitalized COVID-19 Patients with Diabetes. Healthcare 2020, 13, 338. [Google Scholar] [CrossRef]
- Zhang, C.; Wang, X.M.; Li, S.R.; Twelkmeyer, T.; Wang, W.H.; Zhang, S.Y.; Wang, S.F.; Chen, J.Z.; Jin, X.; Wu, Y.Z.; et al. NKG2A is a NK cell exhaustion checkpoint for HCV persistence. Nat. Commun. 2019, 10, 1507. [Google Scholar] [CrossRef]
- Zheng, H.Y.; Zhang, M.; Yang, C.X.; Zhang, N.; Wang, X.C.; Yang, X.P.; Dong, X.Q.; Zheng, Y.T. Elevated exhaustion levels and reduced functional diversity of T cells in peripheral blood may predict severe progression in COVID-19 patients. Cell Mol. Immunol. 2020, 17, 541–543. [Google Scholar] [CrossRef]
- Liao, Y.C.; Liang, W.G.; Chen, F.W.; Hsu, J.H.; Yang, J.J.; Chang, M.S. IL-19 induces production of IL-6 and TNF-alpha and results in cell apoptosis through TNF-alpha. J. Immunol. 2002, 169, 4288–4297. [Google Scholar] [CrossRef]
- Yang, P.; Ding, Y.; Xu, Z.; Pu, R.; Li, P.; Yan, J.; Liu, J.; Meng, F.; Huang, L.; Shi, L.; et al. Epidemiological and clinical features of COVID-19 patients with and without pneumonia in Beijing, China. MedRxiv 2020. [Google Scholar] [CrossRef]
- Fischer, K.; Hoffmann, P.; Voelkl, S.; Meidenbauer, N.; Ammer, J.; Edinger, M.; Gottfried, E.; Schwarz, S.; Rothe, G.; Hoves, S.; et al. Inhibitory effect of tumor cell-derived lactic acid on human T cells. Blood 2007, 109, 3812–3819. [Google Scholar] [CrossRef]
- Bermejo-Martin, J.F.; Almansa, R.; Menéndez, R.; Mendez, R.; Kelvin, D.J.; Torres, A. Lymphopenic community acquired pneumonia as signature of severe COVID-19 infection. J. Infect. 2020, 80, e23–e24. [Google Scholar] [CrossRef]
- Diao, B.; Wang, C.; Tan, Y.; Chen, X.; Liu, Y.; Ning, L.; Chen, L.; Li, M.; Liu, Y.; Wang, G.; et al. Reduction and Functional Exhaustion of T Cells in Patients with Coronavirus Disease 2019 (COVID-19). Front. Immunol. 2020, 11, 827. [Google Scholar] [CrossRef]
- WHO COVID-19 Case Definition. Updated in Public Health Surveillance for COVID-19. 2020. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Surveillance_Case_Definition-2020.1 (accessed on 10 November 2020).
- Korea Disease Control and Prevention Agency. Case Definition and People Subject to Testing. 2020. Available online: http://ncov.mohw.go.kr/en/baroView.do?brdId=11&brdGubun=112&dataGubun=&ncvContSeq=&contSeq=&board_id=&gubunn= (accessed on 10 November 2020).
- Kim, E.S.; Chin, B.S.; Kang, C.K.; Kim, N.J.; Kang, Y.M.; Choi, J.P.; Oh, D.H.; Kim, J.H.; Koh, B.; Kim, S.E.; et al. Clinical Course and Outcomes of Patients with Severe Acute Respiratory Syndrome Coronavirus 2 Infection: A Preliminary Report of the First 28 Patients from the Korean Cohort Study on COVID-19. J. Korean Med. Sci. 2020, 35, e142. [Google Scholar] [CrossRef]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Cho, S.Y.; Park, S.S.; Lee, J.Y.; Kim, H.J.; Kim, Y.J.; Min, C.K.; Cho, B.; Lee, D.G.; Kim, D.W. Successful prevention and screening strategies for COVID-19: Focus on patients with haematologic diseases. Br. J. Haematol. 2020, 190, e33–e37. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables (Total, n = 4052) | Univariable Analysis | Multivariable Analysis | |||
|---|---|---|---|---|---|
| ALCs < 1000/mm3 (n = 786) | ALCs ≥ 1000/mm3 (n = 3266) | p-Value | Odds Ratio (95% CI) | p-Value | |
| Age | <0.001 | <0.001 | |||
| <60 years | 325 (41.3%) | 2181 (66.8%) | 1 | ||
| ≥60 years | 461 (58.7%) | 1085 (33.2%) | 1.75 (1.44–2.13) | ||
| Sex | <0.001 | <0.001 | |||
| Female | 425 (54.1%) | 2057 (63.0%) | 1 | ||
| Male | 361 (45.9%) | 1209 (37.0%) | 1.56 (1.3–1.87) | ||
| Systolic blood pressure, baseline (missing, n = 82) | 0.143 | - | |||
| <140 mmHg, no (%) | 474 (61.2%) | 2045 (64.1%) | - | ||
| ≥140 mmHg, no (%) | 301 (38.8%) | 1147 (35.9%) | - | ||
| Diastolic blood pressure, baseline (missing, n = 175) | <0.001 | <0.001 | |||
| <80 mmHg, no (%) | 336 (43.4%) | 1151 (36.1%) | 1 | ||
| ≥80 mmHg, no (%) | 349 (56.6%) | 2041 (63.9%) | 0.75 (0.63–0.9) | ||
| Heart rate, baseline (missing, n = 71) | 0.007 | 0.393 | |||
| <110/min | 701 (90.2%) | 2984 (93.1%) | 1 | ||
| ≥110/min | 76 (9.8%) | 220 (6.9%) | 1.15 (0.83–1.57) | ||
| Body temperature, baseline (missing, n= 13) | <0.001 | <0.001 | |||
| <38 °C | 666 (84.9%) | 3138 (96.4%) | 1 | ||
| ≥8 °C | 118 (15.1%) | 117 (3.6%) | 3.73 (2.77–5.02) | ||
| Presentation of sputum, baseline | 0.797 | - | |||
| Yes | 227 (28.9%) | 961 (29.4%) | - | ||
| No | 559 (71.1%) | 2305 (70.6%) | - | ||
| Presentation of fatigue, baseline | <0.001 | 0.061 | |||
| Yes | 52 (6.6%) | 118 (3.6%) | 1 | ||
| No | 734 (93.4%) | 3148 (96.4%) | 0.69 (0.48–1.02) | ||
| Presentation of dyspnea, baseline | <0.001 | <0.001 | |||
| Yes | 216 (27.5%) | 342 (10.5%) | 1 | ||
| No | 570 (72.5%) | 2924 (89.5%) | 0.42 (0.34–0.53) | ||
| Presentation of mental disturbance, baseline | <0.001 | 0.623 | |||
| Yes | 15 (1.9%) | 14 (0.4%) | 1 | ||
| No | 771 (98.1%) | 3252 (99.6%) | 0.81 (0.35–1.89) | ||
| Presentation of nausea/vomiting, baseline | 0.002 | 0.136 | |||
| Yes | 58 (7.4%) | 151 (4.6%) | 1 | ||
| No | 728 (92.6%) | 3115 (95.4%) | 0.76 (0.54–1.1) | ||
| Presentation of diarrhea, baseline | 0.327 | - | |||
| Yes | 81 (10.3%) | 297 (9.1%) | - | ||
| No | 705 (89.7%) | 2969 (90.9%) | - | ||
| Comorbidity of cancer with active treatment # | 0.002 | 0.084 | |||
| Yes | 40 (5.1%) | 93 (2.8%) | 1 | ||
| No | 746 (94.9%) | 3173 (97.2%) | 0.69 (0.45–1.06) | ||
| Comorbidity of diabetes | <0.001 | 0.381 | |||
| Yes | 181 (23.0%) | 421 (12.9%) | 1 | ||
| No | 605 (77.0%) | 2845 (87.1%) | 0.9 (0.72–1.13) | ||
| Comorbidity of hypertension | <0.001 | 0.01 | |||
| Yes | 308 (39.2%) | 713 (21.8%) | 1 | ||
| No | 478 (60.8%) | 2553 (78.2%) | 0.76 (0.63–0.94) | ||
| Comorbidity of chronic cardiac disease | <0.001 | 0.956 | |||
| Yes | 62 (7.9%) | 130 (4.0%) | 1 | ||
| No | 724 (92.1%) | 3136 (96.0%) | 1.01 (0.45–1.45) | ||
| Comorbidity of pulmonary disease $ | 0.035 | 0.962 | |||
| Yes | 36 (4.6%) | 98 (3.0%) | 1 | ||
| No | 750 (95.4%) | 3168 (97.0%) | 0.99 (0.65–1.56) | ||
| Comorbidity of chronic renal disease | <0.001 | 0.019 | |||
| Yes | 24 (3.1%) | 23 (0.7%) | 1 | ||
| No | 762 (96.9%) | 3243 (98.6%) | 0.46 (0.24–0.88) | ||
| Comorbidity of hepatic disease † | 0.019 | 0.485 | |||
| Yes | 21 (2.7%) | 46 (1.4%) | 1 | ||
| No | 765 (97.3%) | 3220 (98.6%) | 0.81 (0.45–1.49) | ||
| Comorbidity of autoimmune disease | 0.112 | - | |||
| Yes | 10 (1.3%) | 21 (0.6%) | - | ||
| No | 776 (98.7%) | 3245 (99.4%) | - | ||
| Comorbidity of dementia | <0.001 | <0.001 | |||
| Yes | 84 (10.7%) | 129 (3.9%) | 1 | ||
| No | 702 (89.3%) | 3137 (96.1%) | 0.55 (0.4–0.76) | ||
| Hemoglobin (missing, n = 7) | <0.001 | <0.001 | |||
| <12.5 g/dL | 319 (40.6%) | 859 (26.4%) | 1 | ||
| ≥12.5 g/dL | 467 (59.4%) | 2400 (73.6%) | 0.67 (0.55–0.81) | ||
| Platelet counts (missing, n = 1) | <0.001 | 0.001 | |||
| <100,000/mm3 | 44 (5.6%) | 45 (1.4%) | 1 | ||
| ≥100,000/mm3 | 742 (94.4%) | 3220 (98.6%) | 0.43 (0.26–0.7) | ||
| Variables | Absolute Lymphocyte Counts (Total, n = 770) | p-Value | ||
|---|---|---|---|---|
| Group I, <500/mm3 (n = 110) | Group II, ≥500–<1000/mm3 (n = 330) | Group III, ≥1000/mm3 (n = 330) | ||
| Age | ||||
| <40 years, no (%) | 7 (25.4%) | 25 (7.6%) | 28 (8.5%) | 0.808 |
| 40–59 years, no (%) | 25 (25.4%) | 89 (27.0%) | 81 (24.5%) | |
| ≥60 years, no (%) | 78 (70.9%) | 216 (65.5%) | 221 (67.0%) | |
| Gender | 0.669 | |||
| Female, no (%) | 41 (37.3%) | 138 (41.8%) | 138 (41.8%) | |
| Male, no (%) | 69 (62.7%) | 192 (58.2%) | 192 (58.2%) | |
| Systolic blood pressure, baseline | ||||
| <140 mmHg, no (%) | 68 (61.8%) | 198 (60.0%) | 206 (62.4%) | 0.475 |
| ≥140 mmHg, no (%) | 40 (36.4%) | 131 (39.7%) | 122 (58.2%) | |
| Missing, no (%) | 2 (1.8%) | 1 (0.3%) | 2 (0.6%) | |
| Diastolic blood pressure, baseline | ||||
| <80 mmHg, no (%) | 61 (55.5%) | 164 (49.7%) | 186 (56.4%) | 0.168 |
| ≥80 mmHg, no (%) | 47 (42.7%) | 165 (50.0%) | 142 (43.0%) | |
| Missing, no (%) | 2 (1.8%) | 1 (0.3%) | 2 (0.6%) | |
| Heart rate, baseline | ||||
| <110/min, no (%) | 93 (87.5%) | 291 (88.2%) | 295 (89.1%) | 0.443 |
| ≥110/min, no (%) | 17 (15.5%) | 39 (11.8%) | 36 (10.9%) | |
| Missing, no (%) | 2 (1.8%) | 1 (0.3%) | 2 (0.6%) | |
| Body temperature, baseline, °C, mean ± SD | 37.1 ± 0.8 | 37.1 ± 0.5 | 37.1 ± 0.8 | 0.855 |
| <38 °C | 90 (81.8%) | 275 (83.3%) | 294 (89.1%) | 0.895 |
| ≥38 °C | 20 (18.2%) | 55 (16.7%) | 36 (10.9%) | |
| Baseline presentation | ||||
| Sputum (+), no (%) | 38 (34.5%) | 105 (31.8%) | 109 (33.0%) | 0.860 |
| Fatigue (+), no (%) | 7 (6.4%) | 17 (5.2%) | 17 (5.2%) | 0.872 |
| Dyspnea (+), no (%) | 38 (34.5%) | 105 (31.8%) | 109 (33.0%) | 0.252 |
| Mental disturbance (+), no (%) | 3 (2.7%) | 9 (2.7%) | 8 (2.4%) | 0.966 |
| Nausea/vomiting (+), no (%) | 9 (8.2%) | 22 (6.7%) | 28 (8.5%) | 0.664 |
| Diarrhea (+), no (%) | 16 (4.5%) | 46 (13.9%) | 52 (15.8%) | 0.803 |
| Comorbidity | ||||
| Cancer with active treatment # (+), no (%) | 12 (10.9%) | 23 (7.0%) | 20 (6.1%) | 0.860 |
| Diabetes (+), no (%) | 31 (28.2%) | 88 (26.7%) | 90 (27.3%) | 0.951 |
| Hypertension (+), no (%) | 50 (45.5%) | 148 (44.8%) | 139 (42.1%) | 0.724 |
| Chronic cardiac disease (+), no (%) | 12 (10.9%) | 32 (9.7%) | 34 (10.3%) | 0.927 |
| Chronic pulmonary disease $ (+), no (%) | 4 (3.6%) | 13 (3.9%) | 12 (3.6%) | 0.976 |
| Chronic renal disease (+), no (%) | 4 (3.6%) | 13 (3.9%) | 12 (3.6%) | 0.976 |
| Chronic hepatic disease † (+), no (%), | 7 (6.4%) | 13 (3.9%) | 14 (4.2%) | 0.552 |
| Autoimmune disease (+), no (%) | 3 (2.7%) | 6 (1.8%) | 4 (1.2%) | 0.549 |
| Dementia (+), no (%) | 21 (19.1%) | 53 (16.1%) | 59 (17.9%) | 0.712 |
| Baseline hemogram | ||||
| Hemoglobin, g/dL ± SD | 12.1 ± 2.4 | 12.5 ± 2.0 | 12.5 ± 2.1 | 0.266 |
| Absolute lymphocyte counts, /mm3, mean ± SD | 376.0 ± 106.4 | 787.3 ± 136.7 | 1627.6 ± 742.5 | <0.001 |
| White blood cell counts, /mm3, mean ± SD | 5995 ± 3990 | 5846 ± 3211 | 6322 ± 3876 | 0.232 |
| Platelet, /mm3, mean ± SD | 184,946 ± 98,719 | 186,860 ± 70,172 | 199,632 ± 74,163 | 0.058 |
| Outcomes | Absolute Lymphocyte Counts (Total n = 770) | p-Value | ||
|---|---|---|---|---|
| Group I, <500/mm3 (n = 110) | Group II,≥500–<1000/mm3 (n = 330) | Group III ≥1000/mm3 (n = 330) | ||
| Death, no (%) | 44 (40%) | 75 (22.7%) | 45 (13.0%) | <0.001 |
| Requirement of invasive ventilation, no (%) | 45 (40.9%) | 80 (24.5%) | 49 (14.8%) | <0.001 |
| Requirement of intensive oxygen supplements #, no (%) | 52 (47.3%) | 105 (31.8%) | 60 (18.2%) | <0.001 |
| Requirement of oxygen supplements, no (%) | 80 (72.7%) | 183 (55.5%) | 113 (34.2%) | <0.001 |
| Total hospitalized period, days, mean ± SD | 23.4 ± 13.9 | 25.5 ± 13.4 | 26.3 ± 11.8 | 0.120 |
| Survival periods since admission for patients who died, days, mean ± SD | 14.5 ± 13.3 | 16.4 ± 13.6 | 15.6 ± 14.4 | 0.764 |
| Hospitalized periods for alive patient, days, mean ± SD | 29.4 ± 10.8 | 28.2 ± 12.1 | 28.0 ± 10.5 | 0.631 |
| Variable | Odds Ratio (95% CI) | p-Value |
|---|---|---|
| Age | ||
| <60 years | 1 | |
| ≥60 years | 4.19 (2.14 -8.82) | <0.001 |
| Systolic blood pressure, baseline | ||
| <140 mmHg, no (%) | 1 | |
| ≥140 mmHg, no (%) | 1.66 (1.06 -2.6) | 0.028 |
| Heart rate, baseline | ||
| <110/min | 1 | |
| ≥110/min | 2.34 (1.19–4.57) | 0.013 |
| Dyspnea at presentation | ||
| Not present | 1 | |
| Present | 4.18 (2.61 -6.81) | <0.001 |
| Mental disturbance at presentation | ||
| Not present | 1 | |
| Present | 11.09 (3.28–47.25) | <0.001 |
| Diarrhea at presentation | ||
| Not present | 1 | |
| Present | 0.60 (0.28–1.21) | 0.171 |
| Comorbidity | ||
| Treating cancer, no | 1 | |
| Treating cancer, yes | 3.15 (1.43 -6.85) | 0.004 |
| Diabetes, no | 1 | |
| Diabetes, yes | 2.00 (1.24–3.21) | 0.004 |
| Hypertension, no | 1 | |
| Hypertension, yes | 1.12 (0.69–1.8) | 0.647 |
| Chronic cardiac disease#, no | 1 | |
| Chronic cardiac disease#, yes | 1.10 (0.57–2.08) | 0.773 |
| Chronic pulmonary disease#, no | 1 | |
| Chronic pulmonary disease#, yes | 1.84 (0.68–4.74) | 0.214 |
| Chronic renal disease, no | 1 | |
| Chronic renal disease, yes | 3.36 (1.32–8.54) | 0.010 |
| Dementia, no | 1 | |
| Dementia, yes | 6.55 (3.84–11.40) | <0.001 |
| Hemoglobin | ||
| ≥12.5 g/dL | 1 | |
| <12.5 g/dL | 1.74 (1.10–2.77) | 0.019 |
| Absolute lymphocyte counts | ||
| Group III, ≥1000/mm3 | 1 | |
| Group II, ≥500–<1000/mm3 | 2.47 (1.50–4.13) | <0.001 |
| Group I, <500/mm3 | 5.63 (3.0–10.72) | <0.001 |
| Platelet counts | ||
| ≥100,000/mm3 | 1 | |
| <100,000/mm3 | 2.34 (1.07–5.01) | 0.031 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.; Park, S.-S.; Kim, T.Y.; Lee, D.-G.; Kim, D.-W. Lymphopenia as a Biological Predictor of Outcomes in COVID-19 Patients: A Nationwide Cohort Study. Cancers 2021, 13, 471. https://doi.org/10.3390/cancers13030471
Lee J, Park S-S, Kim TY, Lee D-G, Kim D-W. Lymphopenia as a Biological Predictor of Outcomes in COVID-19 Patients: A Nationwide Cohort Study. Cancers. 2021; 13(3):471. https://doi.org/10.3390/cancers13030471
Chicago/Turabian StyleLee, Jongmin, Sung-Soo Park, Tong Yoon Kim, Dong-Gun Lee, and Dong-Wook Kim. 2021. "Lymphopenia as a Biological Predictor of Outcomes in COVID-19 Patients: A Nationwide Cohort Study" Cancers 13, no. 3: 471. https://doi.org/10.3390/cancers13030471
APA StyleLee, J., Park, S.-S., Kim, T. Y., Lee, D.-G., & Kim, D.-W. (2021). Lymphopenia as a Biological Predictor of Outcomes in COVID-19 Patients: A Nationwide Cohort Study. Cancers, 13(3), 471. https://doi.org/10.3390/cancers13030471