
Postoperative Radiotherapy for Endometrial Cancer in Elderly (≥80 Years) Patients: Oncologic Outcomes, Toxicity, and Validation of Prognostic Scores

 ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient and Treatment Characteristics
2.2. Radiotherapy and Oncological Treatment
2.3. Toxicity, Oncologic Follow-Up, and Prognostic Factors
2.4. Statistical Analysis
3. Results
3.1. Patient and Tumor Characteristics
3.2. Treatment Characteristics
3.3. Toxicity
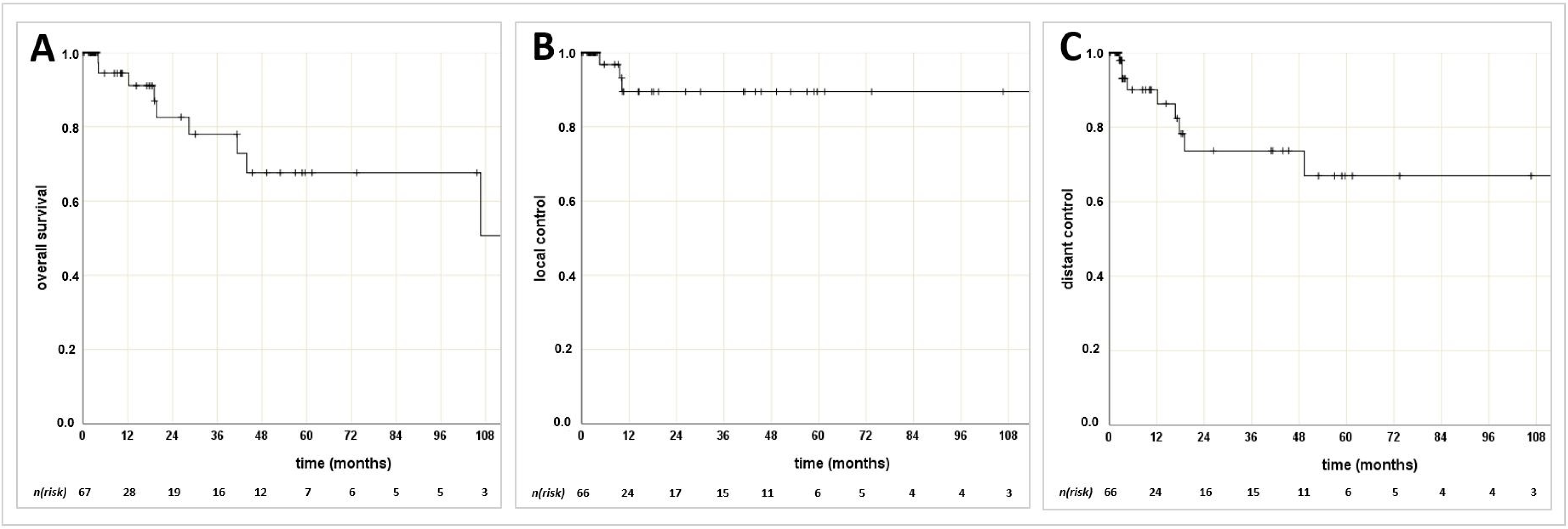
3.4. Oncologic Outcomes
3.5. Prognostic Factor Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Henley, S.J.; Ward, E.M.; Scott, S.; Ma, J.; Anderson, R.N.; Firth, A.U.; Thomas, C.C.; Islami, F.; Weir, H.K.; Lewis, D.R.; et al. Annual report to the nation on the status of cancer, part I: National cancer statistics. Cancer 2020, 126, 2225–2249. [Google Scholar] [CrossRef]
- Robert Koch Institut. Krebsregisterdaten (ZfKD) des Robert Koch-Instituts (RKI) und der Gesellschaft der Epidemiologischen Krebsregister in Deutschland: Krebs in Deutschland für 2013/2014; RKI: Berlin, Germany, 2017. [Google Scholar]
- Onstad, M.A.; Schmandt, R.E.; Lu, K.H. Addressing the Role of Obesity in Endometrial Cancer Risk, Prevention, and Treatment. J. Clin. Oncol. 2016, 34, 4225–4230. [Google Scholar] [CrossRef]
- Pike, M.C.; Peters, R.K.; Cozen, W.; Probst-Hensch, N.M.; Felix, J.C.; Wan, P.C.; Mack, T.M. Estrogen-progestin replacement therapy and endometrial cancer. J. Natl. Cancer Inst. 1997, 89, 1110–1116. [Google Scholar] [CrossRef] [Green Version]
- Zeleniuch-Jacquotte, A.; Akhmedkhanov, A.; Kato, I.; Koenig, K.L.; Shore, R.E.; Kim, M.Y.; Levitz, M.; Mittal, K.R.; Raju, U.; Banerjee, S.; et al. Postmenopausal endogenous oestrogens and risk of endometrial cancer: Results of a prospective study. Br. J. Cancer 2001, 84, 975–981. [Google Scholar] [CrossRef] [Green Version]
- American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 426: The role of transvaginal ultrasonography in the evaluation of postmenopausal bleeding. Obstet. Gynecol. 2009, 113, 462–464. [Google Scholar] [CrossRef]
- Clarke, M.A.; Long, B.J.; Del Mar Morillo, A.; Arbyn, M.; Bakkum-Gamez, J.N.; Wentzensen, N. Association of Endometrial Cancer Risk with Postmenopausal Bleeding in Women: A Systematic Review and Meta-analysis. JAMA Intern. Med. 2018, 178, 1210–1222. [Google Scholar] [CrossRef] [Green Version]
- Bokhman, J.V. Two pathogenetic types of endometrial carcinoma. Gynecol. Oncol. 1983, 15, 10–17. [Google Scholar] [CrossRef]
- Murali, R.; Davidson, B.; Fadare, O.; Carlson, J.A.; Crum, C.P.; Gilks, C.B.; Irving, J.A.; Malpica, A.; Matias-Guiu, X.; McCluggage, W.G.; et al. High-grade Endometrial Carcinomas: Morphologic and Immunohistochemical Features, Diagnostic Challenges and Recommendations. Int. J. Gynecol. Pathol. 2019, 38 (Suppl. 1), S40–S63. [Google Scholar] [CrossRef]
- Lax, S.F. Molecular genetic pathways in various types of endometrial carcinoma: From a phenotypical to a molecular-based classification. Virchows Arch. 2004, 444, 213–223. [Google Scholar] [CrossRef]
- FIGO; Amant, F.; Mirza, M.R.; Koskas, M.; Creutzberg, C.L. Cancer of the corpus uteri. Int. J. Gynaecol. Obstet. 2018, 143 (Suppl. 2), 37–50. [Google Scholar] [CrossRef] [Green Version]
- Frost, J.A.; Webster, K.E.; Bryant, A. Lymphadenectomy for the management of endometrial cancer. Cochrane Database Syst. Rev. 2015, 2015, CD007585. [Google Scholar]
- Holloway, R.W.; Abu-Rustum, N.R.; Backes, F.J.; Boggess, J.F.; Gotlieb, W.H.; Jeffrey Lowery, W.; Rossi, E.C.; Tanner, E.J.; Wolsky, R.J. Sentinel lymph node mapping and staging in endometrial cancer: A Society of Gynecologic Oncology literature review with consensus recommendations. Gynecol. Oncol. 2017, 146, 405–415. [Google Scholar] [CrossRef]
- Levine, D.; The Cancer Genome Atlas Research Network. Integrated genomic characterization of endometrial carcinoma. Nature 2013, 497, 67–73, Erratum in 2013, 500, 242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colombo, N.; Creutzberg, C.; Amant, F.; Bosse, T.; González-Martín, A.; Ledermann, J.; Marth, C.; Nout, R.; Querleu, D.; Mirza, M.R.; et al. ESMO-ESGO-ESTRO Consensus Conference on Endometrial Cancer: Diagnosis, Treatment and Follow-up. Int. J. Gynecol. Cancer 2016, 26, 2–30. [Google Scholar] [CrossRef] [Green Version]
- Creutzberg, C.L.; Nout, R.A.; Lybeert, M.L.; Wárlám-Rodenhuis, C.C.; Jobsen, J.J.; Mens, J.W.; Lutgens, L.C.; Pras, E.; van de Poll-Franse, L.V.; PORTEC Study Group; et al. Fifteen-year radiotherapy outcomes of the randomized PORTEC-1 trial for endometrial carcinoma. Int. J. Radiat Oncol. Biol. Phys. 2011, 81, e631–e638. [Google Scholar] [CrossRef] [Green Version]
- Nout, R.A.; Smit, V.T.; Putter, H.; Jürgenliemk-Schulz, I.M.; Jobsen, J.J.; Lutgens, L.C.; van der Steen-Banasik, E.M.; Mens, J.W.; Slot, A.; Kroese, M.C.; et al. Vaginal brachytherapy versus pelvic external beam radiotherapy for patients with endometrial cancer of high-intermediate risk (PORTEC-2): An open-label, non-inferiority, randomised trial. Lancet 2010, 375, 816–823. [Google Scholar] [CrossRef]
- Poulsen, H.; Jacobsen, M.; Bertelsen, K.; Andersen, J.; Ahrons, S.; Bock, J.; Bostofte, E.; Engelholm, S.; Hølund, B.; Jakobsen, A.; et al. Adjuvant radiation therapy is not necessary in the management of endometrial carcinoma stage I, low risk cases. Int. J. Gynecol. Cancer 1996, 6, 38–43. [Google Scholar] [CrossRef]
- Keys, H.M.; Roberts, J.A.; Brunetto, V.L.; Zaino, R.J.; Spirtos, N.M.; Bloss, J.D.; Pearlman, A.; Maiman, M.A.; Bell, J.G.; Gynecologic Oncology Group. A phase III trial of surgery with or without adjunctive external pelvic radiation therapy in intermediate risk endometrial adenocarcinoma: A Gynecologic Oncology Group study. Gynecol. Oncol. 2004, 92, 744–751, Erratum in 2004, 94, 241–242. [Google Scholar] [CrossRef] [PubMed]
- Bourgin, C.; Saidani, M.; Poupon, C.; Cauchois, A.; Foucher, F.; Leveque, J.; Lavoue, V. Endometrial cancer in elderly women: Which disease, which surgical management? A systematic review of the literature. Eur. J. Surg. Oncol. 2016, 42, 166–175. [Google Scholar] [CrossRef]
- Duska, L.; Shahrokni, A.; Powell, M. Treatment of Older Women with Endometrial Cancer: Improving Outcomes with Personalized Care. Am. Soc. Clin. Oncol. Educ. Book 2016, 35, 164–174. [Google Scholar] [CrossRef] [PubMed]
- Benito, V.; Lubrano, A.; Andújar, M.; Mori, M.; Federico, M. Management of endometrial cancer in patients aged 80 years and older: Identifying patients who may benefit from a curative treatment. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 242, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Kallogjeri, D.; Gaynor, S.M.; Piccirillo, M.L.; Jean, R.A.; Spitznagel, E.L., Jr.; Piccirillo, J.F. Comparison of comorbidity collection methods. J. Am. Coll Surg. 2014, 219, 245–255. [Google Scholar] [CrossRef] [Green Version]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Bellera, C.A.; Rainfray, M.; Mathoulin-Pélissier, S.; Mertens, C.; Delva, F.; Fonck, M.; Soubeyran, P.L. Screening older cancer patients: First evaluation of the G-8 geriatric screening tool. Ann. Oncol. 2012, 23, 2166–2172. [Google Scholar] [CrossRef] [PubMed]
- Racin, A.; Raimond, E.; Bendifallah, S.; Nyangoh Timoh, K.; Ouldamer, L.; Canlorbe, G.; Hudry, N.; Coutant, C.; Graesslin, O.; Touboul, C.; et al. Lymphadenectomy in elderly patients with high-intermediate-risk, high-risk or advanced endometrial cancer: Time to move from personalized cancer medicine to personalized patient medicine! Eur. J. Surg. Oncol. 2019, 45, 1388–1395. [Google Scholar] [CrossRef] [Green Version]
- Small, W., Jr.; Mell, L.K.; Anderson, P.; Creutzberg, C.; De Los Santos, J.; Gaffney, D.; Jhingran, A.; Portelance, L.; Schefter, T.; Iyer, R.; et al. Consensus guidelines for delineation of clinical target volume for intensity-modulated pelvic radiotherapy in postoperative treatment of endometrial and cervical cancer. Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 428–434. [Google Scholar] [CrossRef] [Green Version]
- Small, W., Jr.; Bosch, W.R.; Harkenrider, M.M.; Strauss, J.B.; Abu-Rustum, N.; Albuquerque, K.V.; Beriwal, S.; Creutzberg, C.L.; Eifel, P.J.; Erickson, B.A.; et al. NRG Oncology/RTOG Consensus Guidelines for Delineation of Clinical Target Volume for Intensity Modulated Pelvic Radiation Therapy in Postoperative Treatment of Endometrial and Cervical Cancer: An Update. Int. J. Radiat. Oncol. Biol. Phys. 2021, 109, 413–424. [Google Scholar] [CrossRef]
- Bentzen, S.M.; Constine, L.S.; Deasy, J.O.; Eisbruch, A.; Jackson, A.; Marks, L.B.; Ten Haken, R.K.; Yorke, E.D. Quantitative Analyses of Normal Tissue Effects in the Clinic (QUANTEC): An introduction to the scientific issues. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, S3–S9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Small, W., Jr.; Beriwal, S.; Demanes, D.J.; Dusenbery, K.E.; Eifel, P.; Erickson, B.; Jones, E.; Rownd, J.J.; De Los Santos, J.F.; Viswanathan, A.N.; et al. American Brachytherapy Society consensus guidelines for adjuvant vaginal cuff brachytherapy after hysterectomy. Brachytherapy 2012, 11, 58–67. [Google Scholar] [CrossRef]
- Kenis, C.; Bron, D.; Libert, Y.; Decoster, L.; Van Puyvelde, K.; Scalliet, P.; Cornette, P.; Pepersack, T.; Luce, S.; Langenaeken, C.; et al. Relevance of a systematic geriatric screening and assessment in older patients with cancer: Results of a prospective multicentric study. Ann. Oncol. 2013, 24, 1306–1312. [Google Scholar] [CrossRef]
- Scher, K.S.; Hurria, A. Under-representation of older adults in cancer registration trials: Known problem, little progress. J. Clin. Oncol. 2012, 30, 2036–2038. [Google Scholar] [CrossRef]
- Zaino, R.J.; Kurman, R.J.; Diana, K.L.; Morrow, C.P. Pathologic models to predict outcome for women with endometrial adenocarcinoma: The importance of the distinction between surgical stage and clinical stage—A Gynecologic Oncology Group study. Cancer 1996, 77, 1115–1121, Erratum in 1997, 79, 422. [Google Scholar] [CrossRef]
- Alektiar, K.M.; Venkatraman, E.; Abu-Rustum, N.; Barakat, R.R. Is endometrial carcinoma intrinsically more aggressive in elderly patients? Cancer 2003, 98, 2368–2377. [Google Scholar] [CrossRef]
- Fiorica, F.; Zini, G.; Cartei, F.; Candela, M.V.; Pascale, G.; Berretta, M.; Lleshi, A.; Falco Abramo, M.R.; Del Pup, L.; Fisichella, R.; et al. Postoperative radiotherapy and comorbidity assessment in older and oldest elderly endometrial cancer patients: A retrospective analysis. WCRJ 2014, 1, e55. [Google Scholar]
- Truong, P.T.; Kader, H.A.; Lacy, B.; Lesperance, M.; MacNeil, M.V.; Berthelet, E.; McMurtrie, E.; Alexander, S. The effects of age and comorbidity on treatment and outcomes in women with endometrial cancer. Am. J. Clin. Oncol. 2005, 28, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Montemaggi, P.; Guerrieri, P. Brachytherapy in the elderly. Crit. Rev. Oncol. Hematol. 2001, 37, 159–167. [Google Scholar] [CrossRef]
- Hurria, A.; Togawa, K.; Mohile, S.G.; Owusu, C.; Klepin, H.D.; Gross, C.P.; Lichtman, S.M.; Gajra, A.; Bhatia, S.; Katheria, V.; et al. Predicting chemotherapy toxicity in older adults with cancer: A prospective multicenter study. J. Clin. Oncol. 2011, 29, 3457–3465. [Google Scholar] [CrossRef] [Green Version]
- Manzano, J.G.; Luo, R.; Elting, L.S.; George, M.; Suarez-Almazor, M.E. Patterns and predictors of unplanned hospitalization in a population-based cohort of elderly patients with GI cancer. J. Clin. Oncol. 2014, 32, 3527–3533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, A.W.; Reeve, B.B.; Bellizzi, K.M.; Harlan, L.C.; Klabunde, C.N.; Amsellem, M.; Bierman, A.S.; Hays, R.D. Cancer, comorbidities, and health-related quality of life of older adults. Health Care Financ. Rev. 2008, 29, 41–56. [Google Scholar] [PubMed]
- Giacalone, A.; Quitadamo, D.; Zanet, E.; Berretta, M.; Spina, M.; Tirelli, U. Cancer-related fatigue in the elderly. Support. Care Cancer 2013, 21, 2899–2911. [Google Scholar] [CrossRef]
- Mundt, A.J.; Lujan, A.E.; Rotmensch, J.; Waggoner, S.E.; Yamada, S.D.; Fleming, G.; Roeske, J.C. Intensity-modulated whole pelvic radiotherapy in women with gynecologic malignancies. Int. J. Radiat. Oncol. Biol. Phys. 2002, 52, 1330–1337. [Google Scholar] [CrossRef]
- Wortman, B.G.; Post, C.C.B.; Powell, M.E.; Khaw, P.; Fyles, A.; D’Amico, R.; Haie-Meder, C.; Jürgenliemk-Schulz, I.M.; McCormack, M.; Do, V.; et al. Radiation Therapy Techniques and Treatment-Related Toxicity in the PORTEC-3 Trial: Comparison of 3-Dimensional Conformal Radiation Therapy Versus Intensity-Modulated Radiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2021. [Google Scholar] [CrossRef] [PubMed]
- de Jong, R.A.; Pras, E.; Boezen, H.M.; van der Zee, A.G.; Mourits, M.J.; Arts, H.J.; Aalders, J.G.; Slot, A.; Timmer, P.R.; Hollema, H.; et al. Less gastrointestinal toxicity after adjuvant radiotherapy on a small pelvic field compared to a standard pelvic field in patients with endometrial carcinoma. Int. J. Gynecol. Cancer 2012, 22, 1177–1186. [Google Scholar] [CrossRef]
- Poorvu, P.D.; Sadow, C.A.; Townamchai, K.; Damato, A.L.; Viswanathan, A.N. Duodenal and other gastrointestinal toxicity in cervical and endometrial cancer treated with extended-field intensity modulated radiation therapy to paraaortic lymph nodes. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 1262–1268. [Google Scholar] [CrossRef]
- Hamaker, M.E.; Jonker, J.M.; de Rooij, S.E.; Vos, A.G.; Smorenburg, C.H.; van Munster, B.C. Frailty screening methods for predicting outcome of a comprehensive geriatric assessment in elderly patients with cancer: A systematic review. Lancet Oncol. 2012, 13, e437–e444. [Google Scholar] [CrossRef]
- Baitar, A.; Van Fraeyenhove, F.; Vandebroek, A.; De Droogh, E.; Galdermans, D.; Mebis, J.; Schrijvers, D. Evaluation of the Groningen Frailty Indicator and the G8 questionnaire as screening tools for frailty in older patients with cancer. J. Geriatr. Oncol. 2013, 4, 32–38. [Google Scholar] [CrossRef] [Green Version]
- Kaufmann, A.; Schmidt, H.; Ostheimer, C.; Ullrich, J.; Landenberger, M.; Vordermark, D. Quality of life in very elderly radiotherapy patients: A prospective pilot study using the EORTC QLQ-ELD14 module. Support. Care Cancer 2015, 23, 1883–1892. [Google Scholar] [CrossRef] [PubMed]
- Huguenin, P.; Glanzmann, C.; Lütolf, U.M. Acute toxicity of curative radiotherapy in elderly patients. Strahlenther. Onkol. 1996, 172, 658–663. [Google Scholar]


{kind=link}
| Characteristics | Values |
|---|---|
| Median age | 82 (range: 80–95) years |
| Median Karnofsky performance score | 80 (60–100) % |
| Median Charlson Comorbidity Index | 5 (4–9) |
| Median G8 screening score | 13 (6–16) * |
| Median BMI | 26.5 (20.5–45.7) |
| Median hemoglobin level | 11.9 (8.9–14.0) g/dL |
| FIGO stage | |
| 1/2 | 58 (82.9%) |
| 3/4 | 12 (17.1%) |
| Surgical procedure | |
| oncological procedure | 62 (88.6%) |
| non-oncologic excision only | 8 (11.4%) |
| Adjuvant chemotherapy | |
| not indicated | 30 (42.9%) |
| performed | 1 (1.43%) |
| indicated, but not feasible | 39 (55.7%) |
| Lymph node dissection | |
| not indicated | 20 (28.6%) |
| performed | 25 (35.7%) |
| indicated, but not feasible | 25 (35.7%) |
| Postoperative radiotherapy | |
| performed as indicated | 57 (81.4%) |
| EBRT indicated, but not feasible | 13 (18.6%) |
| Histological subtype | |
| endometrioid | 51 (72.9%) |
| serous | 13 (18.6%) |
| carcinosarcoma | 6 (8.6%) |
| Characteristics | Values |
|---|---|
| Median time from surgery to start of RT | 54 (range: 6–219) days |
| Median treatment time | 25 (1–67) days |
| Median days of RT discontinuation | 0 (0–5) days |
| Premature cessation of RT | 4 (5.7%) |
| Median total dose in EQD2 (α/β = 10) | 28.42 (6.25–77.98) Gy |
| RT technique | |
| IMRT (EBRT + BT) | 16 (22.9%) |
| 3D-CRT (EBRT + BT) | 18 (25.7%) |
| BT only | 36 (51.4%) |
| Rates | Overall Survival | Local Control | Distant Control |
|---|---|---|---|
| 1-year | 94.4% | 89.5% | 86.3% |
| 2-year | 82.6% | 89.5% | 73.6% |
| 5-year | 67.6% | 89.5% | 66.9% |
| Characteristics | Overall Survival | Local Control | Distant Control | |||
|---|---|---|---|---|---|---|
| HR 95%CI | p | HR 95%CI | p | HR 95%CI | p | |
| Age | 0.937 (0.732–1.200) | 0.608 | 1.005 (0.734–1.375) | 0.976 | 0.668 (0.440–1.015) | 0.059 |
| Body mass index BMI < 28 vs. ≥28 | 1.102 (0.989–1.228) | 0.033 | 1.112 (0.778–1.589) | 0.208 | 0.936 (0.696–1.259) | 0.137 |
| Charlson Comorbidity Index | 1.197 (0.706–2.030) | 0.505 | 1.401 (0.648–3.026) | 0.391 | 0.657 (0.335–1.288) | 0.221 |
| G8 Screening Score | 0.666 (0.503–0.883) | 0.005 | 1.438 (0.700–2.955) | 0.323 | 0.936 (0.666–1.317) | 0.705 |
| Karnofsky performance score ≤80 vs. ≥90 | 1.215 (0.245–6.030) | 0.811 | 0.034 (0–4223.770) | 0.572 | 3.049 (0.816–11.397) | 0.081 |
| Number of medications | 0.898 (0.690–1.167) | 0.420 | 0.970 (0.547–1.723) | 0.918 | 0.931 (0.710–1.220) | 0.603 |
| Hemoglobin level ≤12 vs. >12 g/dL | 0.155 (0.019–1.267) | 0.046 | 47.435 (0–5,464,301) | 0.516 | 0.522 (0.124–2.195) | 0.375 |
| Histologic grading G1 vs. G2 vs. G3 | 2.412 (0.749–7.767) | 0.140 | 1.274 (0.260–6.256) | 0.765 | 34.098 (0.82–1411.8) | 0.001 |
| FIGO stage 1/2 vs. 3/4 | 0.993 (0.122–8.089) | 0.995 | 0.042 (0–335,213.6) | 0.695 | 1.881 (0.388–9.122) | 0.433 |
| TNM T1/2 vs. T3/4 | 34.49 (2.158–551.6) | 0.012 | 0.031 (0–1604.964) | 0.529 | 8.762 (0.792–96.963) | 0.077 |
| Nodal stage N0 vs. N+ | 0.993 (0.122–8.089) | 0.995 | 0.042 (0–335,213.6) | 0.695 | 2.110 (0.434–10.251) | 0.354 |
| Tumor type endometrioid vs. serous vs. carcinosarcoma | 3.400 (1.427–8.100) | 0.006 | 0.052 (0–294.620) | 0.503 | 1.770 (0.638–4.914) | 0.273 |
| Lymph vascular involvement L1 vs. L0 | 0.470 (0.055–4.033) | 0.491 | 1.149 (0.104–12.68) | 0.910 | 5.581 (0.979–31.829) | 0.031 |
| EQD2 ≥ 60 Gy (α/β = 10) | 33.062 (3.618–302) | 0.002 | 0.038 (0–32,130.29) | 0.639 | 8.969 (1.766–45.543) | 0.008 |
| Omission of indicated therapy | ||||||
| Oncological surgery | 0.043 (0–2466.448) | 0.574 | 0.044 (0–2,913,770) | 0.733 | 0.040 (0–277.695) | 0.476 |
| Lymph node dissection | 1.094 (0.459–2.609) | 0.839 | 0.616 (0.134–2.836) | 0.534 | 1.636 (0.665–4.026) | 0.284 |
| Chemotherapy | 1.122 (0.572–2.202) | 0.738 | 0.733 (0.221–2.435) | 0.613 | 2.236 (0.925–5.405) | <0.0001 |
| EBRT | 1.013 (0.199–5.164) | 0.987 | 0.039 (0–44,883.5) | 0.649 | 0.600 (0.074–4.873) | 0.633 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meixner, E.; Lang, K.; König, L.; Sandrini, E.; Lischalk, J.W.; Debus, J.; Hörner-Rieber, J. Postoperative Radiotherapy for Endometrial Cancer in Elderly (≥80 Years) Patients: Oncologic Outcomes, Toxicity, and Validation of Prognostic Scores. Cancers 2021, 13, 6264. https://doi.org/10.3390/cancers13246264
Meixner E, Lang K, König L, Sandrini E, Lischalk JW, Debus J, Hörner-Rieber J. Postoperative Radiotherapy for Endometrial Cancer in Elderly (≥80 Years) Patients: Oncologic Outcomes, Toxicity, and Validation of Prognostic Scores. Cancers. 2021; 13(24):6264. https://doi.org/10.3390/cancers13246264
Chicago/Turabian StyleMeixner, Eva, Kristin Lang, Laila König, Elisabetta Sandrini, Jonathan W. Lischalk, Jürgen Debus, and Juliane Hörner-Rieber. 2021. "Postoperative Radiotherapy for Endometrial Cancer in Elderly (≥80 Years) Patients: Oncologic Outcomes, Toxicity, and Validation of Prognostic Scores" Cancers 13, no. 24: 6264. https://doi.org/10.3390/cancers13246264
APA StyleMeixner, E., Lang, K., König, L., Sandrini, E., Lischalk, J. W., Debus, J., & Hörner-Rieber, J. (2021). Postoperative Radiotherapy for Endometrial Cancer in Elderly (≥80 Years) Patients: Oncologic Outcomes, Toxicity, and Validation of Prognostic Scores. Cancers, 13(24), 6264. https://doi.org/10.3390/cancers13246264